
Abstract
This study aimed to quantify whether there is association between music-based movement therapy and motor dysfunction in patients with Parkinson’s disease, and, if so, whether music-based movement therapy can be used as first-line non-pharmacological treatment. To conduct a systematic review and meta-analysis of clinical trials that examined the effect of music-based movement therapy on patient-relevant and disease-specific outcomes. Comprehensive literature was searched of PubMed, EMbase, and the Cochrane Library from inception to November 2016. Randomized controlled trial of patients with Parkinson’s disease was searched to identify trials comparing music-based movement therapy with no music care. A total of 8 studies (11 analyses, 241 subjects) were included; all of them had acceptable quality by PEDro scale score. Studies based on any type of Parkinson’s disease patients were combined and subgroup analyzed. Compared with the control group, the SMD of Berg Balance Scale score was 0.85(0.46 to 1.25), −0.60 (−0.98 to −0.22) in Parkinson Disease Questionnaire-39 summary index, −0.90s (−1.56 to −0.23) in Time Up and Go text, and −0.43 (−1.11 to 0.25) in Unified Parkinson’s Disease Rating Scale Motor Subscale 3 as instrument methods for motor function. Secondary outcomes included cognitive function and quality of life. There was positive evidence to support the use of music-based movement therapy on treatment of motor function; there was neutral evidence to support the use of music for the treatment of cognitive function quality of life.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative movement disorder disease that causes motor disturbances (postural and walking difficulties, rigidity, bradykinesia, and tremor) and non-motor disturbances, such as neuropsychiatric (e.g., depression, anxiety, cognitive impairments), neurovegetative disorders (e.g., decreased control of urinary bladder, sexual dysfunctions) [1], and Health-related quality of life [2], which affects more than 1 million people in the USA, causes falls and hip fractures costing approximately US$192 million annually [3]. Moreover, PD is also a chronic progressive neuropathy disorder accompanied by motor and cognitive dysfunction and alterations in different regulatory mechanisms [4].
Treatment of PD is settled by both pharmacological and non-pharmacological treatments. Currently, pharmacological therapy is essentially symptomatic and does not have a satisfactory impact on symptoms related to neurodegenerative diseases progression. A systematic review [5] of randomized controlled trials had reached the conclusion that physiotherapy has short-term benefits in PD. As a result, several health institutions recommended the development of non-pharmacological complementary interventions as a first-line treatment [6]. However, intensive motor training can improve important motor and cognitive function, in recent years, more attention has been given to the effectiveness of non-pharmacological approaches in dysfunction therapy, including a growing interest in music therapy and music-based stimulation [7].
The power of music and its non-verbal nature make it an effective medium of communication when language is diminished or abolished,7 though the curative effect of music is still uncertain. Music easily elicits movement, stimulating interactions between perception and action systems [8]. Therefore, music therapy has been developed with the aim of improving motor recovery in patients with PD. The definition of music-based movement therapy is not only hearing the music but also singing and playing rhythm and percussion instruments. In studies, we used activity controls and individuals receiving usual care as the comparators. The intriguing sensitivity to music exhibited by persons with dementia has been shown to have therapeutic purposes.
Due to the numerous classifications of music therapy and the small sample sizes, the effects of music-based movement therapy are still inconsistent. To further explore these issues, we performed a meta-analysis of all available clinical trials of motor dysfunction and cognitive dysfunction therapy in PD patients. No previous reviews [9] have provided a comprehensive overview with meta-analyses.
Methods
This review was performed using a prespecified protocol. It was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [10]. The project was prospectively registered with the PROSPERO database of systematic reviews, number CRD 42016045719 [11].
Study selection criteria
Eligible clinical trials were in any language and included patients with Parkinson’s disease undergoing motor dysfunction. We evaluated all studies that compared any form and intervention method of music-based movement therapy with no music care while excluded studies which did not provide comparative or missing outcomes. The patients diagnosed with any type of Parkinson’s disease by each individual study were accepted. We systematically reviewed three electronic databases: PubMed, EMbase, and the Cochrane library, from inception to November 2016. The search strategy included keywords and MeSH terms relating to music-based movement therapy and motor function and cognitive function or other outcomes and diseases. We also reviewed the reference list of relevant publications for additional studies.
Data collection, extraction, and quality assessment
Two investigators (Shuai Zhang and Dong Liu) examined the eligibility of the studies. Both of them independently extracted and compiled data from the studies using a standardized data extraction form, and disagreements were resolved through consensus or referral to a third reviewer (Kai Liu). Discrepancies and unobtainable data were resolved by group discussion between at least three investigators. Randomized controlled trials (RCTs) were eligible for the meta-analysis.
We extracted baseline information from the individual studies, including publication, year, country, study design, participants (n, age, male%), disease type, disease duration, delivery, etc. Moreover, outcome measure scale scores were also extracted at baseline. The design of each individual study was also included in the baseline information, such as the intervention method, frequency and duration, and the outcome assessment time.
We assessed the quality of the included studies with Physiotherapy Evidence Database (PEDro) scale score [12]. The PEDro is an 11-item scale that assesses the quality of RCTs; if the answer to the first item is “NO,” the study is excluded from the meta-analysis. When the PEDro score is greater than 4 (the max score was 10), the study is considered high quality.
Outcome measures
The predefined primary outcome was motor function; the secondary outcomes included cognitive function and quality of life. The outcomes measured before and after the therapy period were extracted by the investigators. We also explored evidence for the presence of method-related effects on outcomes.
Motor function was evaluated by the Unified Parkinson’s Disease Rating Scale Motor Subscale 3(UPDRS) [13], Berg Balance Scale(BBS) [14], and the Timed Up and Go test (TUG) [15]. Quality of life was evaluated by the Parkinson Disease Questionnaire-39 summary index (PDQ-39) [16] and the 12-item short-form health survey (SF-12) [17]. In addition, PDQ-39 sub-scale was considered as measures for other indicators, then combined analysis with other non-sub-scales.
Statistical analysis
We tabulated the characteristics and results of all included studies, performed a meta-analysis of the baseline demographics, comparing music-based movement therapy with a control group for all studies, and presented them as the standardized mean difference (SMD). Statistical heterogeneity was also tested by I 2, with an I 2 < 25% indicating low heterogeneity.
We used random-effects models to assess heterogeneity between studies, based on P value (P < 0.05) and I 2 statistic (I 2 > 50%). All outcomes were continuous variables, and thus we analyzed the SMD in change from baseline and the 95% confidence interval (CI) in the analysis. We defined studies reporting multiple interventions and comparators as sub-studies to avoid double counting and mistreating data. We used Comprehensive Meta-Analysis statistical software (CMA, version 2) for meta-analysis.
Results
Baseline characteristics
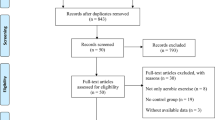
We identified 8 trials [18,19,20,21,22,23,24,25] (11 analyses) for systematic review and meta-analysis, including 241 subjects allocated to music-based movement therapy or control (Fig. 1). The studies were conducted in wide range of counties and continents, the publication data range from 2000 to 2013, and the size of the included studies was between 16 and 61 subjects. Overall, all included studies were designed as RCT. Table 1 summarizes the differences in fundamental characteristics between the music-based movement therapy group and control group. The table showed that two groups had similar results in age, gender, disease period, UPDRS score, and Hoehn and Yahr. In conclusion, baseline characteristics were balanced between music-based movement therapy group and control group. Duration of music training varied between 6 weeks to 2 years. The assessments of study quality were presented in Supplementary Appendix, and result of PEDro scale score showed all of our included studies had acceptable quality.

Flow of studies through review process for systematic review and meta-analysis
Efficacy of music-based movement therapy on primary outcome
The included studies were suitable for meta-analysis of motor function (Fig. 2); these studies contributed to four separate sub-analyses, each with different types of evaluated measures. Three studies [21,22,23] (4 analyses) reported BBS score, and there was no heterogeneity between the trials (P = 0.486, I 2 = 0%). In fixed-effects meta-analysis, the SMD was 0.85 (95%CI 0.46~1.25) suggesting that music-based movement therapy might be beneficial to improve motor function. Two studies evaluated the effect of music-based movement therapy by PDQ39 sub-scale [20, 21]. The result showed significant positive effect of music-based movement therapy (SMD = −0.60, 95%CI −0.98~−0.22) but also little heterogeneity (P = 0.155, I 2 = 42.772%) among included studies. The overall effect of executive function evaluated by TUG(s) score was −0.90(SMD, 95%CI 0.94~2.56) from 4 trials (5 analyses) [18, 21,22,23] and revealed significant differences between the two groups which means music-based movement therapy could improve motor function but with heterogeneity among studies (P = 0.021, I 2 = 65.435%). Motor function can also be reported by UPDRS from five therapy-ending data [19, 22,23,24, 26], and the merged results favor for music-based movement therapy group (SMD = −0.43, 95%CI: -1.11 ~ 0.25) and huge heterogeneity among studies (P = 0.001, I 2 = 74.874%). These results revealed music-based movement therapy has better curative effect than the control group, while publication bias was not detected.

Overall efficacy of music-based training on motor function. #evaluated by follow-up data. BBS Berg Balance Scale, PDQ39 Parkinson Disease Questionnaire-39 summary index, TUG Timed Up and Go test, UPDRS Unified Parkinson’s Disease Rating Scale Motor Subscale 3
Efficacy of music-based movement therapy for secondary outcomes
Three of them (eight analyses) reported cognitive function [18,19,20] and no significant difference between two groups (SMD = −0.33, 95%CI −0.97~0.31) with large heterogeneity (P = 0.001, I 2 = 72.5%). Quality of life was also reported in Parkinson’s disease group (6 analyses [19,20,21, 26]). The summarized results might favor the control group (SMD = 0.54, 95%CI −0.66 ~ 1.73; P = 0.000, I 2 = 90.8%), and no significant difference was found (Fig. 3).

Efficacy of music-based movement therapy for secondary outcomes
Discussion
Our meta-analysis suggests that music-based movement therapy has a positive effect on motor function as evaluated by the following instruments: BBS, PDQ39#, TUG(s), and UPDRS and a positive trend on cognitive function and quality of life. This finding was based on a comprehensive systematic review including 8 studies (11 analyses) and over 200 subjects. Most trials suggested that music-based movement therapy was associated with improvements in motor function. However, one group of these associations did not reach statistical significance and heterogeneity existed in the other two groups (Fig. 2). For secondary outcomes, most trials suggested that music-based movement therapy was associated with improvement in outcomes of cognitive function and quality of life. However, these associations did not reach statistical significance and heterogeneity existed in most of the outcomes. Based on that the factors might affect the results, we conducted meta-regression and subgroup analyses (Fig. 3).
For the primary outcome of motor function (our studies included mainly four methods of evaluation, because of the small number of studies), we did not conduct meta-regression and subgroup analyses for the instrument methods in the primary outcome (Fig. 2). Though we only used 11 instruments for assessment, more indicators in our included fundamental research are reported, such as PLM movement time [18], Exit Questionnaire [22], etc. Although these indicators have not been included in our meta-analysis because of few analyses (less than three), they showed a favorable effect of music-based movement therapy. Although lacking data, the included trials were compliant with a good standard of quality, and we believe that this meta-analysis is the most comprehensive systematic review so far to investigate the use of music-based movement therapy in patients with PD. No adverse effects were reported in our included fundamental studies.
Our conclusion by meta-analysis should be verified. A study made by Craig [26] arrived at a general direction that music relaxation therapy could get a similar efficacy with neuromuscular therapy on motor and non-motor symptoms. Besides, another study [27] gave evidence that specific music can improve the precision of arm and finger movements. Moreover, training accompanied by “walking songs” were evaluated using objective measures of gait score; one study demonstrated that music listening can be safely implemented among PD patients during home exercise [7]. According to the source of the subjects, dividing subjects into those from hospitals and nursing homes—a controlled clinical trial [28] studied on relatively healthy elderly—the results suggested that impoverished environment of long-term-care institutions might contribute to lower cognitive scores.
This review followed guideline for rigorous systematic reviews and meta-analysis [10]. In order to identify as many relevant reports as possible and reduce the risk of bias, a comprehensive search strategy was made. With all these reasons, we observed no evidence of publication bias by statistical assessment. The present meta-analysis has several limitations. We undertook this systematic review with a comprehensive search strategy, and although there were no data and language restrictions, it was impossible to include all published and unpublished literature, especially the unpublished literature. Furthermore, positive results are easy to publish, but negative results are not likely to leave the laboratory. Another limitation was that many of the included studies had very small sample sizes (the average sample size was less than 40), which means that many of our included studies may have lacked tests to detect differences between the intervention group and control group. An additional limitation of many outcomes was their extensive heterogeneity, which indicated substantial variability in the outcomes of included studies, although this was often because of the presence of heterogeneity of baseline outcomes and anticipated differences in trial design, populations, and country. Subgroup analyses generally did not substantially explain and reduce the heterogeneity; we used random effect mode to take heterogeneity into account, and the results showed were explained as reflecting the average result across the group of studies.
The beneficial effects of music-based movement therapy on participants meet expectations and the perception of music. Several possible and potential mechanisms could help to explain effects of music training on neurodegenerative symptoms. Several potential mechanisms could help to explain effects of music-based movement therapy; it may involve rhythmic entrainment mechanisms [29]. However, the mechanisms underlying successful musical neurodegenerative dysfunctions are not well understood. The mechanism through which cadence-matched, salient music improves gait performance and motor symptoms in PD patients is equivocal [7]. The discovery of the clinical effectiveness of rhythmic motor entertainment also brought into focus for the first time that the structural elements of music have enormous potential in clinical applications to retrain the injured brain [30]. The previous meta-analyses based on patients with PD had similar trend of the results we obtained [9], but their analyses were not comprehensive and detailed with less number into study. We believed that this meta-analysis is the most comprehensive systematic review so far for use of music in motor dysfunction therapy. No adverse effects were reported in our included fundamental studies. Further clinical trials of music-based movement therapy should be large size, robust, and random to confirm the effect of music-based movement therapy, particularly on patient-relevant or disease-specific outcomes. Further studies should ensure that the appropriate methods are used for randomization, blinding, and intent-to-treat. Further trials should assess outcomes using standardized or prescribed measures at similar period points. Analyses of individual data would be valuable in exploring further. More normative studies will be used for further meta-analysis.
In summary, there was evidence of a positive effect of music-based movement therapy, supporting its use for the treatment of motor dysfunction. There was neutral effect evidence to support the use of music-based movement therapy for the treatment of cognitive function and quality of life. On a local scale, patients with PD suffering from motor dysfunction could be encouraged to undertake music-based movement therapy.
References
Chaudhuri KR, Schapira AH (2009) Non-motor symptoms of Parkinson’s disease: dopaminergic pathophysiology and treatment. Lancet Neurol 8(5):464–474
Martinez-Martin P, Deuschl G (2007) Effect of medical and surgical interventions on health-related quality of life in Parkinson’s disease. Mov Disord 22(6):757–765
Melton LJ, Leibson CL, Achenbach SJ, Bower JH, Maraganore DM, Oberg AL, Rocca WA (2006) Fracture risk after the diagnosis of Parkinson's disease: influence of concomitant dementia. Mov Disord 21(9):1361–1367
Bruguerolle B, Simon N (2002) Biologic rhythms and Parkinson’s disease: a chronopharmacologic approach to considering fluctuations in function. Clin Neuropharmacol 25(4):194–201
Tomlinson CL, Patel S, Meek C, Herd CP, Clarke CE, Stowe R, Shah L, Sackley C, Deane KH, Wheatley K, Ives N (2012) Physiotherapy intervention in Parkinson’s disease: systematic review and meta-analysis. BMJ 345:e5004
Kadivar Z, Corcos DM, Foto J, Hondzinski JM (2011) Effect of step training and rhythmic auditory stimulation on functional performance in Parkinson patients. Neurorehabil Neural Repair 25(7):626–635
de Bruin N, Doan JB, Turnbull G, Suchowersky O, Bonfield S, Hu B, Brown LA (2010) Walking with music is a safe and viable tool for gait training in Parkinson’s disease: the effect of a 13-week feasibility study on single and dual task walking. Parkinson’s Dis 2010
Zatorre RJ, Chen JL, Penhune VB (2007) When the brain plays music: auditory–motor interactions in music perception and production. Nat Rev Neurosci 8(7):547–558
De Dreu MJ, Van Der Wilk ASD, Poppe E, Kwakkel G, Van Wegen EEH (2012) Rehabilitation, exercise therapy and music in patients with Parkinson's disease: a meta-analysis of the effects of music-based movement therapy on walking ability, balance and quality of life. Parkinsonism Relat Disord 18:S114–S119
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(4):264–269
Centre for Reviews and Dissemination (2009) Systematic reviews: CRD’s guidance for undertaking reviews in health care (Internet). University of York, York
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M (2003) Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther 83(8):713–721
Movement Disorder Society Task Force on Rating Scales for Parkinson's Disease (2003) The Unified Parkinson's disease rating scale (UPDRS): status and recommendations. Mov Dis 18(7):738
Berg K, Wood-Dauphinee S, Williams JI (1995) The balance scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med 27(1):27–36
Morris ME, Huxham F, McGinley J, Dodd K, Iansek R (2001) The biomechanics and motor control of gait in Parkinson disease. Clin Biomech 16(6):459–470
Jenkinson C, Fitzpatrick RAY, Peto VIV, Greenhall R, Hyman N (1997) The Parkinson’s disease Questionnaire (PDQ-39): development and validation of a Parkinson’s disease summary index score. Age Ageing 26(5):353–357
Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, Bullinger M, Kaasa S, Leplege A, Prieto L, Sullivan M (1998) Cross-validation of item selection and scoring for the SF-12 health survey in nine countries: results from the IQOLA project. J Clin Epidemiol 51(11):1171–1178
Pohl P, Dizdar N, Hallert E (2013) The Ronnie Gardiner rhythm and music method—a feasibility study in Parkinson’s disease. Disabil Rehabil 35(26):2197–2204
Modugno N, Iaconelli S, Fiorlli M, Lena F, Kusch I, Mirabella G (2010) Active theater as a complementary therapy for Parkinson’s disease rehabilitation: a pilot study. Sci World J 10:2301–2313
Hackney ME, Earhart GM (2009) Health-related quality of life and alternative forms of exercise in Parkinson disease. Parkinsonism Relat Disord 15(9):644–648
Hackney ME, Earhart GM (2009) Effects of dance on movement control in Parkinson's disease: a comparison of Argentine tango and American ballroom. J Rehabil Med 41(6):475–481
Hackney ME, Earhart GM (2008) Tai chi improves balance and mobility in people with Parkinson disease. Gait Posture 28(3):456–460
Hackney ME, Kantorovich S, Levin R, Earhart GM (2007) Effects of tango on functional mobility in Parkinson's disease: a preliminary study. J Neurol Phys Ther 31(4):173
Hackney ME, Kantorovich S, Earhart GM (2007) A study on the effects of Argentine tango as a form of partnered dance for those with Parkinson disease and the healthy elderly. Am J Dance Ther 29(2):109–127
Pacchetti C, Mancini F, Aglieri R, Fundarò C, Martignoni E, Nappi G (2000) Active music therapy in Parkinson’s disease: an integrative method for motor and emotional rehabilitation. Psychosom Med 62(3):386–393
Craig LH, Svircev A, Haber M, Juncos JL (2006) Controlled pilot study of the effects of neuromuscular therapy in patients with Parkinson’s disease. Mov Disord 21(12):2127–2133
Bernatzky G, Bernatzky P, Hesse HP, Staffen W, Ladurner G (2004) Stimulating music increases motor coordination in patients afflicted with Morbus Parkinson. Neurosci Lett 361(1):4–8
Galdino De TC (2014) Beneficial effects of multisensory and cognitive stimulation on age-related cognitive decline in long-term-care institutions. Clin Interv Aging 9:309–321
Morris ME, Iansek R, Matyas TA, Summers JJ (1996) Stride length regulation in Parkinson’s disease. Brain 119(2):551–568
Thaut MH (2015) The discovery of human auditory–motor entrainment and its role in the development of neurologic music therapy. Prog Brain Res 217:253–266
Acknowledgments
We thank the authors of primary studies for providing data and other critical information. And, the authors would like to thank all researchers and participants for their valuable contributions to this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Funding
None.
Electronic supplementary material
ESM 1
(DOC 27 kb)
Rights and permissions
About this article

Cite this article
Zhang, S., Liu, D., Ye, D. et al. Can music-based movement therapy improve motor dysfunction in patients with Parkinson’s disease? Systematic review and meta-analysis. Neurol Sci 38, 1629–1636 (2017). https://doi.org/10.1007/s10072-017-3020-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-017-3020-8