
Abstract
Objectives
Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a systemic vasculitis with unknown aetiology. Although biopsies are helpful for diagnosing AAV, whether they improve the outcomes of AAV patients remains unknown. The objective of this study was to elucidate the association between biopsies and prognosis.
Method
This retrospective cohort study analysed health care records that were routinely collected at 190 hospitals in Japan from April 2005 to March 2019. Patients who were 18 years or older and hospitalized for AAV were eligible for inclusion. The primary outcome was the composite outcome of death and renal replacement therapy (RRT) during the first admission. We compared the outcome between the biopsy group and the no-biopsy group. The chi-square test was performed as a univariable analysis, and logistic regression analysis was performed as a multivariable analysis.
Results
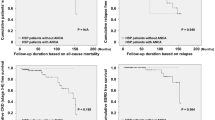
Three hundred and eighty-six patients were assessed in this study. One hundred fifty-four (39.9%) patients underwent biopsy, and 232 (60.1%) patients did not undergo biopsy during the first admission with AAV. In univariable analysis, the composite outcome of death and RRT were observed in 7 (4.5%) patients in the biopsy group and 25 (10.8%) patients in the no-biopsy group (OR 0.39 [95% CI 0.17, 0.94], P = 0.01). The result was consistent in the multivariable analysis (OR 0.31 [95% CI 0.12, 0.79], P = 0.01) after adjusting for potential confounders.
Conclusions
We showed that patients who underwent biopsy had a better prognosis in the composite outcome of mortality and RRT during admission using a Japanese healthcare record database.
Key Points • This is the first study to elucidate the association between undergoing biopsy and prognosis. • Patients undergoing biopsy had a better prognosis in the composite outcome of mortality and RRT. • The proportion of patients who received transfusions was not significantly different between the two groups. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a rare, autoimmune disease that is characterized by a high positive rate of ANCAs and necrotic vasculitis of small vessels [1,2,3,4,5,6]. AAV includes granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA). Although the incidence of AAV was reported to be as low as approximately 1.2 per 100,000 person-years in both Europe and Japan, it leads to high mortality (18–44%) and end-stage renal disease (23–30%) in affected patients [7,8,9,10,11].
Although various types of biopsies are performed on patients with AAV to confirm diagnosis and predict prognosis [12, 13], they have some adverse events. For example, it was reported that haemorrhages requiring transfusions occur in 0.4–1.5% of patients with renal biopsies and pneumothoraxes occur in 20.2% of patients with lung biopsies [14, 15]. They are performed in practice and recommended by the European League Against Rheumatism (EULAR) and European Renal Association-European Dialysis and Transplant Association (ERA-EDTA) [16, 17]; however, these recommendations are based only on studies that revealed the diagnostic sensitivities of each type of biopsy [18,19,20,21,22].
Although biopsies have decent diagnostic performance for AAV, whether biopsies improve the prognosis of AAV patients remains unknown. It is not acceptable to conduct harmful procedures to patients without rationale. Considering the situation, it is crucial to investigate the association between biopsies and prognosis as the first step in developing a rationale for the efficacy of biopsies in the management of AAV. The objective of this study was to elucidate the association between biopsies and prognosis utilizing the Japanese healthcare record database.
Materials and methods
Study design and setting
This retrospective cohort study used the RWD database, which is managed by the Health, Clinic and Education Information Evaluation Institute (HCEI; Kyoto, Japan) [23, 24]. The HCEI is a not-for-profit research service foundation in Japan that is supported by Real World Data Co., Ltd. (Kyoto, Japan) for data collection and standardization. This database consists of the data of 20 million patients from 190 hospitals in Japan. It includes demographic data, diagnoses with the International Statistical Classification of Diseases and Related Health Problems, 10th Revision Codes (ICD-10 code), prescriptions, laboratory results, and procedures of inpatients and outpatients. These data are managed by allocating unique identifiers for each individual. No linkage with other databases was performed for this study.
Data collection and definitions
We included inpatients who were 18 years and older and had codes associated with a diagnostic code representing AAV. Only data about first admissions associated with AAV were utilized for this study. We defined first admissions as the earliest admissions in the database. The data were available only after hospitals implemented electronic medical records, and the median date of admission in the database was July 2013 (interquartile range, July 2009–July 2016). The definition of “admissions associated with AAV” was an admission that had the ICD-10 code (M301, M310, M313, M317, M318, N007, N017, N019, N037, N057, J991) as at least one of the following three definitions: main disease, main trigger of admission, or the disease that was the most resource intensive during admission, which were recorded in the discharge abstract of each patient. These three definitions of ICD-10 codes were assigned by the physicians in charge. We excluded patients who had prior histories of dialysis. Patients who were prescribed prednisolone or immunosuppressive agents such as cyclophosphamide, rituximab, cyclosporine, tacrolimus, and azathioprine until 30 days before admissions were also excluded because they could already have been treated for AAV. We identified biopsies by procedural codes in administrative claims data. In Japan, although lung biopsies and otorhinolaryngological biopsies have some health care fee codes, there was no specific code for renal biopsies at the time when these data were collected. In practice, “percutaneous needle biopsy” and “open abdominal biopsy” are substituted as renal biopsies. Therefore, we extracted “percutaneous needle biopsy” and “open abdominal biopsy” as renal biopsies. We identified the procedural code “tissue sampling” from the ear, nose, oral cavity, pharynx and larynx as otorhinolaryngological biopsies. We also extracted the procedural codes for “tissue sampling” from skin, muscle, and peripheral nerve as other biopsies. The procedural codes for data extractions are shown in the Supplementary Materials.
This study was approved by the Institutional Review Board at Kyoto University and did not need individual consent because the data were anonymized.
Variables
The primary outcome was the composite outcome of death and RRT. Secondary outcomes were death alone, RRT alone [25], use of cyclophosphamide (CPA), use of rituximab (RTX), use of steroid pulse therapy, maximum dose of oral steroids per day, and use of transfusion during admission. We chose the composite outcome of death and RRT as the primary outcome because death and RRT are plausibly competing risks with each other for AAV patients who suffer from severe renal failure, and they would occur sufficiently often [10, 25, 26]. Outcomes were identified by ICD-10 codes, procedural codes, laboratory data, and the Anatomical Therapeutic Chemical code, which is a code for prescriptions.
Statistical analysis
Continuous variables are reported as the mean and standard deviation, and categorical variables are reported as numbers and percentages. First, we described the characteristics of patients who underwent biopsies and those who did not. The characteristics of patients with each type of biopsy were also described. We performed a chi-square test for binary data and a t-test for continuous data as univariable analyses. We also used multivariable linear regression analysis for continuous data and multivariable logistic regression analysis for categorical data. In multivariable analysis, we used age, sex, body mass index (BMI) [27], haemoglobin, serum albumin on admission, type of ANCA, anti-GBM antibody, Charlson comorbidity index (CCI), and disease severity, which is determined by the clinical grading system and indicates the severity of patients with rapidly progressive glomerulonephritis (RPGN), as confounding variables. These variables were indicated as potential confounding factors in previous studies [28,29,30]. The clinical grading system, which includes serum creatinine, C-reactive protein (CRP), and the presence of pulmonary regions, can predict the long-term prognosis of patients with RPGN [2]. We adopted this system because it precisely reflects the Japanese population and can be fulfilled with only laboratory data and the existence of lung involvement, which can be found in this database.
We dealt with treatments such as RTX, CPA, and the maximum dose of oral steroids as outcomes because we hypothesized that treatments would be changed by the results of biopsies. We did not utilize treatments as confounding variables because they are intermediate factors for other prognostic outcomes. We performed multiple imputation analysis with the mice package of R to fill in the missing BMI data and some laboratory data on admission by creating 10 imputed datasets. We reported P-values with a two-sided test and considered P < 0.05 to indicate statistical significance. All statistical analyses were conducted using R ver. 3.5.3.
Post hoc sensitivity analysis
The proportion of ANCA-positive patients was estimated as the baseline characteristics of the patients, and nearly half of the patients were found to be ANCA-negative. The reason why a subset of patients without laboratory confirmation was diagnosed with AAV was likely due to the Japanese-specific guideline [31, 32]. In that guideline, the combination of the following three features may allow physicians in Japan to make a probable diagnosis of AAV, even with ANCA-negative patients. However, since it is not possible to determine how the diagnosis of AAV was actually made from our database, we conducted a post hoc analysis to investigate the impact of the misclassification of AAV patients on the results. In this sensitivity analysis, we made two assumptions: (1) The diagnosis of the patients in the biopsy group was correct. (2) More outcomes occur in patients with AAV than in patients who are misclassified as having AAV because the prognosis of AAV is generally poor [7, 8, 10].
Results
We identified 676 admissions that were assigned codes associated with AAV from April 2005 to March 2019. Of them, 290 admissions were excluded for reasons such as age, number of admissions, RRT before admission, and immunosuppressant prescriptions (Fig. 1). Finally, 386 patients were included in this study. During the first admission, 154 (39.9%) inpatients underwent biopsies, and 232 (60.1%) inpatients did not. Eighty-seven patients underwent renal biopsies, 31 patients underwent lung biopsies, 10 patients underwent otorhinolaryngological biopsies, and 53 patients underwent other biopsies. Twenty-one patients underwent two of four types of biopsies, and 3 patients underwent three of them during the first admission with AAV. The baseline characteristics of each group are shown in Table 1. Younger age and male sex were more frequently observed in the biopsy group. The CCI was significantly different between the two groups; patients with CCI ≥ 5 were observed more frequently in the biopsy group. Other characteristics were not different between the two groups.

Algorithm for selection of AAV patients
We show the baseline characteristics of patients with each type of biopsy in Table 2. The serum creatinine level of patients with renal biopsy tended to be higher than that of patients with other types of biopsies. The CRP levels of patients with otorhinolaryngological biopsies were higher than those of patients with other types of biopsies. Interstitial pneumonia was observed more frequently among patients with lung biopsy.
In Table 3, we show crude and adjusted odds ratios (ORs) for outcomes in both groups. The composite outcomes of death and RRT were observed in 7 (4.5%) patients in the biopsy group and 25 (10.8%) patients in the no-biopsy group (OR 0.39 [95% CI 0.17, 0.94], P = 0.01). Two (1.3%) patients in the biopsy group and 10 (4.3%) in the no-biopsy group (OR 0.33 [95% CI 0.07, 1.53], P = 0.22) died during the first admission. RRT was observed in 6 (3.9%) patients in the biopsy group and 16 (6.9%) patients in the no-biopsy group (OR 0.55 [95% CI 0.21, 1.43], P = 0.28). The mean maximum dose of oral steroids was 32.2 mg in the biopsy group and 20.1 mg in the no-biopsy group (mean difference 10.8 mg [95% CI 7.9, 16.4], P < 0.01). There was no significant difference in transfusion between the groups (OR 1.23 [95% CI 0.76, 1.99], P = 0.39). In the multivariable analysis, the adjusted OR of the composite outcome of death and haemodialysis remained lower in the biopsy group than in the no-biopsy group (OR 0.31 [95% CI 0.12, 0.79], P = 0.01). The maximum dose of oral steroids also remained significantly higher in the biopsy group (mean difference 10.8 mg [95% CI 6.4, 15.2], P < 0.01).
A post hoc sensitivity analysis to examine the impact of misclassification showed that the results did not differ depending on the presence of misclassification. The details of this analysis are shown in the Supplementary Material.
Discussion
In this study, we found that biopsies in inpatients with AAV were associated with composite outcomes of death and RRT. Notably, composite outcomes were observed more frequently in the no-biopsy group. This result was consistent between the univariable analysis and multivariable analysis. Additionally, the maximum dose of oral steroids was significantly higher in the biopsy group than in the no-biopsy group. As one of the surrogate outcomes of haemorrhage, transfusion was not significantly different between the biopsy group and the no-biopsy group. Our results showed that AAV patients with biopsies received more intensive treatments and had a better prognosis during admission.
To our knowledge, this is the first study to compare the short-term prognosis of AAV patients who underwent biopsies with those who did not. Previous studies focused only on patients who underwent biopsies and whose histopathologic patterns and prognosis were assessed [26, 27]. Although previous studies revealed the diagnostic performance of biopsies for AAV patients, there were no published data to indicate the association between biopsies and the prognosis of AAV patients. Moreover, in our study, we utilized laboratory data from the database to adjust the difference between the biopsy group and the no-biopsy group. Our study offered new findings in the management of AAV patients, which implies the benefit of performing biopsies.
The finding that the frequency of transfusion was not significantly different between the two groups was also noteworthy. Although the risk of haemorrhage as an adverse effect of biopsy discourages physicians from performing biopsies, our results may support performing biopsies in terms of safety. However, we must admit that the sample size may not be large enough to detect a difference in such a rare outcome between the two groups.
There are five limitations in this study. First, the present study was a retrospective study. There would be confounding by indications between the biopsy group and the no-biopsy group, and confounding would widen the gap between the two groups. However, we utilized the laboratory data and adjusted for it as much as possible in multivariable analysis. Second, there was no specific health care fee code for renal biopsy during the target period of this study. We substituted “percutaneous biopsy” and “open abdominal biopsy”, which could include other types of biopsies. However, given that the biopsies were performed during the first admission with AAV, we assume that most of them would be renal biopsies. Moreover, the fact that patients with renal biopsies had higher serum creatinine levels indicated that the substitution of “percutaneous biopsies” and “open abdominal biopsy” for renal biopsy was valid (Table 2). Third, this study did not include admissions before hospitals applied the electronic medical record system. Second and subsequent admissions could have been identified as the first admission just after hospitals implemented electronic medical records. Therefore, we excluded patients who were treated with steroids or other immunosuppressive agents before the first admission with AAV. Thus, there may be some misclassification between the biopsy group and the no-biopsy group. However, we considered this type of misclassification to be nondifferential misclassification in this study because there is no relationship between the timing of admissions with AAV and the timing at which hospitals adopted electronic medical records. Among the situations with nondifferential misclassification, the direction of the bias would close the gap between the two groups [31]. Even in the situation, some outcomes were significantly different between the two groups. We believe the gap would remain significant and wider, even without misclassification, and the results with statistical significance are acceptable. Fourth, ICD-10 codes associated with AAV were not validated in Japan and thus may not completely reflect the actual disease. Regarding this limitation, we believe almost all of the codes reflected the actual disease because they were given by the doctors in charge in Japan. Finally, this study was based on the Japanese healthcare record database. These results may not be applicable to other regions.
In conclusion, we elucidated that AAV patients who underwent biopsies had a better prognosis in terms of the composite outcome of death and RRT in a Japanese healthcare database.
References
Pagnoux C (2016) Updates in ANCA-associated vasculitis. Eur J Rheumatol 3(3):122–133. https://doi.org/10.5152/eurjrheum.2015.0043
Koyama A, Yamagata K, Makino H, Arimura Y, Wada T, Nitta K et al (2009) A nationwide survey of rapidly progressive glomerulonephritis in Japan: etiology, prognosis and treatment diversity. Clin Exp Nephrol 13(6):633–650. https://doi.org/10.1007/s10157-009-0201-7
Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F et al (2013) 2012 Revised International Chapel Hill consensus conference nomenclature of vasculitides. In: Arthritis and rheumatism. Instituto Nacional de Enfermedades Respiratorias 1:1–11. https://doi.org/10.1002/art.37715
La Guillevin L (2012) granulomatose éosinophilique avec polyangéite (syndrome de Churg et Strauss). Vol. 41. Presse Med 41:1004–13. https://doi.org/10.1016/j.lpm.2012.07.008
Comarmond C, Pagnoux C, Khellaf M, Cordier JF, Hamidou M, Viallard JF et al (2013) Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): clinical characteristics and long-term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort. Arthritis Rheum 65(1):270–281. https://doi.org/10.1002/art.37721
Watts RA, Mahr A, Mohammad AJ, Gatenby P, Basu N, Flores-Suárez LF (2015) Classification, epidemiology and clinical subgrouping of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis. Nephrol Dial Transplant 30:i14-22. https://doi.org/10.1093/ndt/gfv022
Fujimoto S, Uezono S, Hisanaga S, Fukudome K, Kobayashi S, Suzuki K et al (2006) Incidence of ANCA-associated primary renal vasculitis in the Miyazaki Prefecture: the first population-based, retrospective, epidemiologic survey in Japan. Clin J Am Soc Nephrol 1(5):1016–1022. https://doi.org/10.2215/CJN.01461005
Mohammad AJ, Weiner M, Sjöwall C, Johansson ME, Bengtsson AA, Ståhl-Hallengren C et al (2015) Incidence and disease severity of anti-neutrophil cytoplasmic antibody-associated nephritis are higher than in lupus nephritis in Sweden. Nephrol Dial Transplant 30:i23-30. https://doi.org/10.1093/ndt/gfu396
Mohammad AJ, Jacobsson LTH, Westman KWA, Sturfelt G, Segelmark M (2009) Incidence and survival rates in Wegener’s granulomatosis, microscopic polyangiitis, Churg-Strauss syndrome and polyarteritis nodosa. Rheumatology 48(12):1560–1565. https://doi.org/10.1093/rheumatology/kep304
Mohammad AJ, Segelmark M (2014) Antineutrophil cytoplasmic antibody (ANCA) a population-based study showing better renal prognosis for proteinase 3. J Rheumatol 41(7):2020. https://doi.org/10.3899/jrheum.131038
Watts RA, Scott DGI, Jayne DRW, Ito-Ihara T, Muso E, Fujimoto S et al (2008) Renal vasculitis in Japan and the UK - are there differences in epidemiology and clinical phenotype? Nephrol Dial Transplant 23(12):3928–3931. https://doi.org/10.1093/ndt/gfn354
Thompson G, Klecka M, Roden AC, Specks U, Cartin-Ceba R (2016) Biopsy-proven pulmonary capillaritis: a retrospective study of aetiologies including an in-depth look at isolated pulmonary capillaritis. Respirology 21(4):734–738. https://doi.org/10.1111/resp.12738
Berden AE, Ferrario F, Hagen EC, Jayne DR, Jennette JC, Joh K et al (2010) Histopathologic classification of ANCA-associated glomerulonephritis. J Am Soc Nephrol 21:1628–1636. https://doi.org/10.1681/ASN.2010050477
Corapi KM, Chen JLT, Balk EM, Gordon CE (2012) Bleeding complications of native kidney biopsy: a systematic review and meta-analysis. Am J Kidney Dis 60(1):62–73. https://doi.org/10.1053/j.ajkd.2012.02.330
Ravaglia C, Bonifazi M, Wells AU, Tomassetti S, Gurioli C, Piciucchi S et al (2016) Safety and diagnostic yield of transbronchial lung cryobiopsy in diffuse parenchymal lung diseases: a comparative study versus video-assisted thoracoscopic lung biopsy and a systematic review of the literature. Respiration 91(3):215–227. https://doi.org/10.1159/000444089
Yates M, Watts RA, Bajema IM, Cid MC, Crestani B, Hauser T et al (2016) EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann Rheum Dis 75(9):1583–1594. https://doi.org/10.1136/annrheumdis-2016-209133
Mukhtyar C, Guillevin L, Cid MC, Dasgupta B, De Groot K, Gross W et al (2009) EULAR recommendations for the management of primary small and medium vessel vasculitis. Ann Rheum Dis 68(3):310–317. https://doi.org/10.1136/ard.2008.088096
Travis WD, Hoffman GS, Leavitt RY, Pass HI, Fauci AS (1991) Surgical pathology of the lung in Wegener’s granulomatosis: review of 87 open lung biopsies from 67 patients. Am J Surg Pathol 15(4):315–33. https://doi.org/10.1097/00000478-199104000-00001
Devaney KO, Ferlito A, Hunter BC, Devaney SL, Rinaldo A (1998) Wegener’s granulomatosis of the head and neck. Ann Otol Rhinol Laryngol. 107(5 I):439–45. https://doi.org/10.1177/000348949810700515
Devaney KO, Travis WD, Hoffman G, Leavitt R, Lebovics R, Fauci AS (1990) Interpretation of head and neck biopsies in Wegener’s granulomatosis. A pathologic study of 126 biopsies in 70 patients. Am J Surg Pathol. 14(6):555–64. https://doi.org/10.1097/00000478-199006000-00006
Schnabel A, Holl-Ulrich K, Dalhoff K, Reuter M, Gross WL (1997) Efficacy of transbronchial biopsy in pulmonary vaculitides. Eur Respir J 10(12):2738–2743. https://doi.org/10.1183/09031936.97.10122738
Aasarød K, Bostad L, Hammerstrøm J, Jørstad S, Iversen BM (2001) Renal histopathology and clinical course in 94 patients with Wegener’s granulomatosis. Nephrol Dial Transplant 16(5):953–960. https://doi.org/10.1093/ndt/16.5.953
Takeuchi M, Ogura M, Minoura T, Inagaki N, Kawakami K (2020) Comparative effectiveness of sodium-glucose cotransporter-2 inhibitors versus other classes of glucose-lowering medications on renal outcome in type 2 diabetes. Mayo Clin Proc 95:265–273. https://doi.org/10.1016/j.mayocp.2019.12.004
Ide K, Fujiwara T, Shimada N, Tokumasu H (2021) Influence of acetaminophen on renal function: a longitudinal descriptive study using a real-world database. Int Urol Nephrol 53(1):129–135. https://doi.org/10.1007/s11255-020-02596-7
Manja V, AlBashir S, Guyatt G (2017) Criteria for use of composite end points for competing risks—a systematic survey of the literature with recommendations. J Clin Epidemiol 82:4–11. https://doi.org/10.1016/j.jclinepi.2016.12.001
Friedman DJ, Piccini JP, Wang T, Zheng J, Malaisrie SC, Holmes DR et al (2018) Association between left atrial appendage occlusion and readmission for thromboembolism among patients with atrial fibrillation undergoing concomitant cardiac surgery. JAMA - J Am Med Assoc 319(4):365–374. https://doi.org/10.1001/jama.2017.20125
Di Angelantonio E (2018) Body mass index as a measure of global adiposity. Arch Cardiovasc Dis 111(3):141–143. https://doi.org/10.1016/j.acvd.2018.02.002
Wang Y, Huang X, Cai J, Xie L, Wang W, Tang S et al (2016) Clinicopathologic characteristics and outcomes of lupus nephritis with antineutrophil cytoplasmic antibody: a retrospective study. Med (United States) 95(4):e2580. https://doi.org/10.1097/MD.0000000000002580
Moon JS, Ahn SS, Park YB, Lee SK, Lee SW (2018) C-reactive protein to serum albumin ratio is an independent predictor of all-cause mortality in patients with ANCA-associated vasculitis. Yonsei Med J 59(7):865–871. https://doi.org/10.3349/ymj.2018.59.7.865
Özçelik G, Hafize &, Sönmez E, Şahin S, Özağarı A, Meral, et al (2019) Clinical and histopathological prognostic factors affecting the renal outcomes in childhood ANCA-associated vasculitis. Pediatr Nephrol 34:847–54. https://doi.org/10.1007/s00467-018-4162-5
Harigai M, Nagasaka K, Amano K, Bando M, Dobashi H, Kawakami T et al (2019) 2017 Clinical practice guidelines of the Japan Research Committee of the Ministry of Health, Labour, and Welfare for intractable vasculitis for the management of ANCA-associated vasculitis. Mod Rheumatol 29(1):20–30. https://doi.org/10.1080/14397595.2018.1500437
Arimura Y, Harigai M, Maruyama S, Homma S (2018) Anca Kanren Kekkanen Gaidorain 2017. Nippon Naika Gakkai Zasshi 107(4):741–745. https://doi.org/10.2169/naika.107.741
Acknowledgements
We acknowledge HCEI, which provided data to us.
Funding
This work was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (grant number 20H03941).
Author information
Authors and Affiliations
Contributions
HH conducted the analysis and wrote the first draft of the manuscript. MT commented on the analysis and redrafted the manuscript. KK advised on the analysis and study design. HH and MT contributed to the study conception and design. HH contributed to the analysis and interpretation of data. The first draft was written by HH, and all authors commented and revised the draft. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Institutional Review Board at Kyoto University. We performed this study in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. This study did not need individual consent because the data were anonymized.
Competing interests
Koji Kawakami has received research funds from Eisai Co. Ltd.; Kyowa Kirin Co. Ltd.; Sumitomo Dainippon Pharma Co. Ltd.; Pfizer Inc.; Stella Pharma Corporation; CMIC Co. Ltd.; Suntory Beverage & Food Ltd.; Mitsubishi Corporation, and Real World Data Co. Ltd.; consulting fees from LEBER Inc.; JMDC Inc.; Shin Nippon Biomedical Laboratories Ltd.; Kaken Pharmaceutical Co. Ltd.; and Advanced Medical Care Inc.; executive compensation from Cancer Intelligence Care Systems; Inc.; honorarium from Mitsubishi Chemical Holdings Corporation, Mitsubishi Corporation, and Pharma Business Academy; and holds stock in Real World Data Co. Ltd. Other authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hashimoto, H., Takeuchi, M. & Kawakami, K. Association between biopsies for anti-neutrophil cytoplasmic antibody-associated vasculitis and prognosis: a retrospective cohort study. Clin Rheumatol 41, 541–548 (2022). https://doi.org/10.1007/s10067-021-05889-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-021-05889-z