
Abstract
Objectives
Activated macrophages expressing CD163 (M2) are the most abundant macrophage subtype in renal biopsies from lupus nephritis (LN) patients. We studied the role of proteolytically cleaved soluble CD163 (sCD163) as a biomarker of LN disease activity.
Methods
SLE patients were classified as active LN (AN), inactive disease (ID), and active non-renal disease (ANR). Urine and plasma samples were collected at baseline from all patients and at 3 monthly follow-up from AN patients. sCD163 was measured by ELISA. Urine values were normalized to urinary creatinine excretion and expressed as pg/mg. Urine samples from 25 healthy controls (HC) and 20 rheumatoid arthritis patients served as disease controls (DC).
Results
Among the 122 patients studied (114 females, 57 AN, 42 ID, 23 ANR), baseline median urinary sCD163 in the AN group (114.01 pg/mg) was significantly higher (p < 0.001) as compared with ID (10.34 pg/mg), ANR (3.82 pg/mg), HC (0 pg/mg), and DC (7.56 pg/mg) groups and showed modest correlation with renal SLEDAI (r = 0.47; p < 0.001). Urinary sCD163 performed the best on receiver operating characteristics (ROC) analysis (AUC = 0.76) at baseline to differentiate between AN and ANR as compared with plasma sCD163, anti-ds DNA antibodies, and C3 and C4.
In follow-up study, urinary sCD163 decreased significantly (p < 0.001) in AN patients at 3 (22.07 pg/mg), 6 (12.7 pg/mg), 9 (11.09 pg/mg), and 12 months (7.2 pg/mg). In 4 patients who had either relapse or developed CKD, urinary sCD163 levels correlated with the changing disease activity.
Conclusions
Urinary sCD163 is a good biomarker of LN disease activity.
Key Points • Urinary sCD163 levels are raised in patients with active lupus nephritis and correlate with renal SLEDAI. • Urinary sCD163 levels fall after treatment and may be helpful in monitoring response to therapy in lupus nephritis. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Renal involvement in systemic lupus erythematosus (SLE) is important to recognize early as it is a major predictor of long-term outcome. Furthermore, lupus nephritis (LN) also warrants a more aggressive immunosuppression besides corticosteroids and hydroxychloroquine. Though kidney biopsy is the gold standard for diagnosis and classification of LN, it is invasive and cannot be done repeatedly to assess response. Thus, there is a quest to identify urinary markers that can identify patients with LN among patients with SLE and can also help in assessing response to treatment. Proteinuria and active sediment are traditional biomarkers of renal involvement but have a number of limitations [1]. Proteinuria can be present in patients with renal damage and leucocyturia can be seen with urinary tract infection as well as in interstitial inflammation.
In the pursuit of finding new biomarkers for LN that can overcome the limitations of the existing ones, recent studies have focused on the urinary sediment. Since it can directly reflect the renal immuno-inflammatory milieu, its characterization and pathological correlation would give invaluable information to look for new biomarkers. It has been noticed that macrophages are the most abundant urinary cells in active sediment of LN followed by T cells and B cells [2]. Macrophages are classified into M1 and M2 macrophages based on their phenotype as well as function. Among the various subtypes of macrophages, alternatively activated M2c-like macrophages are the most abundant in renal biopsies as well as in urine of patients with LN [3].
M2 macrophages express CD163 and are predominantly anti-inflammatory in activity as compared with M1 macrophages. Their major function is in resolution of inflammation, tissue remodeling, and promotion of fibrosis. The chief anti-inflammatory cytokines secreted by them are IL-10, arginase-1, and transforming growth factor–β. M2 macrophages have been thought to play key pathogenic role in development of various autoimmune diseases including SLE [4]. Since these macrophages express CD163 which can be proteolytically cleaved from the surface and released in the circulation as a soluble protein, soluble CD163 (sCD163) may correlate with disease activity.
In patients with lupus nephritis, it has been shown that a number of glomerular M2 macrophages correlate with severity of proteinuria. These macrophages have defective expression of heme oxygenase-1 (HO-1). SLE has been associated with type I interferon signature and, interestingly, human M2 macrophages, when exposed to type I interferons in vitro, downregulate the expression of HO-1 which connects the type I interferon signature and macrophages in LN pathogenesis [5].
In patients with ANCA-associated vasculitis and (AAV) crescentic glomerulonephritis, sCD163 has been shown to be elevated in urine in active disease and its levels correlated with treatment response [6]. The same study also included some patients with LN and they also had higher expression of mRNA of CD163 in renal biopsies as compared with healthy renal tissue.
Therefore, it is possible that urinary sCD163 may serve as a biomarker of renal disease activity in LN. We hypothesize that urinary sCD163 may not only be able to differentiate active LN from other groups like active disease without nephritis but may also be able to help in assessing response to therapy. In this study, we aimed to determine the utility of urinary and plasma sCD163 as a biomarker in LN in both cross-sectional as well as in longitudinal manner to address the above questions.
Patients and methods
This observational study was carried out at the Clinical Immunology and Rheumatology department of a tertiary care hospital. The institutional ethics committee approved the study and informed consent was taken from all the enrolled patients and control subjects. Consenting SLE patients who satisfied 1997 modified American College of Rheumatology (ACR) criteria were enrolled in this study [7]. Patients who were either pregnant or having active infection were excluded. Depending upon their organ system involvement, they were classified into one of the three classes: active disease with renal involvement (active nephritis, AN), active disease without any renal involvement (active non-renal disease, ANR), and inactive disease (ID). Disease was characterized as active if their SLE disease activity index (SLEDAI) was > 4 and inactive if SLEDAI was ≤ 4 [8]. Based on renal involvement, patients with active disease were further classified as AN if renal SLEDAI (rSLEDAI) was ≥ 4 and ANR if rSLEDAI was 0. rSLEDAI is the sum value of the 4 components in SLEDAI that refer to urinary examination which include hematuria, leucocyturia, proteinuria, and urinary casts with each having a score of 4 and hence can vary between 0 and 16.
Patients with active renal disease underwent renal biopsy before the initiation of treatment as per ACR guidelines unless contraindicated [9]. If renal biopsy was not done, patient was treated as per the most probable histological class based upon their clinical and laboratory parameters. All patients with AN disease were followed up at least every 3 months or earlier as needed for 1 year. Disease activity was measured using SLEDAI and rSLEDAI and the response to therapy was defined using the ACR criteria [10].
All the patients gave informed consent and, at baseline, blood and urine samples were collected along with clinical details. Follow-up samples at every 3 monthly visits were taken from only AN patients. Urine samples from 25 healthy individuals and 20 rheumatoid arthritis patients with active disease served as healthy controls (HC) and disease control (DC) respectively. Plasma and the cell free urine samples were stored at − 80 °C till analysis and thawed only once for ELISA.
sCD163 was measured by commercially available ELISA kits (R&D systems, Minneapolis, MN, USA). The lowest detection limit of the assay was 62.5 pg/ml and the range was 62.5–4000 pg/ml. The intra-assay variability was less than 7% while inter-assay variability was less than 9%. Urinary sCD163 values were analyzed with and without normalization for urinary creatinine excretion (mg/dl) to control for fall in glomerular filtration rate (GFR) with rising creatinine.
Variables are expressed as median (range, i.e., min–max). For comparison between 2 groups, Mann-Whitney U test and chi-squared tests were used. For comparison among > 2 groups, Kruskal-Wallis test was used. If any difference was found, then the groups were further compared using Mann-Whitney U test. Spearman’s rank correlation was used for studying associations between 2 variables. A p value < 0.05 was considered significant.
A total of one hundred and twenty-two patients (F:M = 114:8) were enrolled in the study. The median age in the three groups was comparable. Among these patients, 57 had active nephritis (AN), 23 had active non-renal (ANR) disease, and 42 had inactive disease (ID) (Table 1). Among the 45 patients who had a renal biopsy done in the AN group, according to the ISN/RPS classification, 5 showed class II nephritis, 16 each had class III and IV nephritis, 7 had class V nephritis, and 1 had class VI nephritis. Biopsy could not be done for various reasons in 12 patients and they were treated as per the most probable histological class decided by clinical and laboratory features (11 as proliferative nephritis and 1 as membranous nephropathy). All the patients with class II nephritis (n = 5) were treated with steroids in combination with azathioprine. Patients with proliferative nephritis (i.e., class III & IV n = 44) were induced with cyclophosphamide (n = 5 for the high dose monthly boluses for 6 months and n = 36 for the 500 mg fortnightly boluses for 6 doses) or mycophenolate (n = 3). Patients with class V nephritis (n = 8) were induced with cyclophosphamide (n = 7 for high dose monthly boluses for 6 months) or mycophenolate (n = 1). One of the patients from proliferative nephritis group who was on low-dose cyclophosphamide regimen did not respond and was given rituximab at 3 months and developed ESRD at 6 months. All the patients who were induced with mycophenolate continued it during maintenance phase. Patients who received cyclophosphamide as inducing agent were given azathioprine during maintenance.
Results
Among the 57 patients of AN group, 51 completed 6-month follow-up whereas 46 completed complete 12-month follow-up visit. Complete response (CR) rates at 3, 6, 9, and 12 months were 26%, 36%, 43%, and 43% respectively.
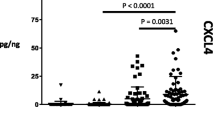
Median (range) urinary sCD163 was significantly higher in AN group [4296.5 (0–127,750)] as compared with all other groups (ID [558.6 (0–24,032.5)]; ANR [290.3 (0–3767)]; HC [158.3 (0–1610.5)]; and RA [530.9 (0–2394.1)] pg/ml) at baseline (p < 0.001 for all comparisons). To control for fall in GFR with rising creatinine, urinary sCD163 values were analyzed after normalization for urinary creatinine excretion and the results were no different. (Table 1, Fig. 1a; normalized median urinary sCD163 levels in HC and DC: 0 (0–110.58) and 7.56 (0–20.76) pg/mg). In contrast, plasma sCD163 levels in patients of AN group were significantly higher as compared with patients in ID group (p < 0.001) but were indifferent from those of ANR group (Table 1, Fig. 1b). Among the patients of AN group, urinary sCD163 values were not different in patients with proliferative LN as compared with membranous nephropathy.

Scatter plot showing baseline (a) normalized urinary sCD163 and (b) plasma sCD163 levels in patients and control groups
Urinary sCD163 showed a modest correlation with proteinuria (ρ = 0.59; p < 0.001) and with SLEDAI (ρ = 0.33; p < 0.001) at baseline (Fig. 2a). Urinary sCD163 and plasma sCD163 did not show any significant correlation with each other at baseline (ρ = 0.23) suggesting that urinary sCD163 was not merely the filtered fraction of the plasma sCD163. Among the patients with AN, urinary sCD163 showed modest correlation with rSLEDAI (ρ = 0.47; p < 0.001) (Fig. 2b). In contrast, plasma sCD163 did not correlate with any of these parameters.

Relationship of baseline normalized urinary sCD163 with (a) SLEDAI in all patients and (b) rSLEDAI in AN group
Receiver operating characteristics (ROC) analysis (area under curve; 95% confidence interval; p value) at baseline to differentiate between AN and ANR showed that urinary sCD163 was the best marker (0.76; 0.65–0.86; p < 0.001) as compared with plasma sCD163 (0.46; 0.32–0.61; p = ns), anti-ds DNA antibodies (0.6; 0.44–0.76; p = ns), C3 (0.65; 0.51–0.8; p = ns), and C4 (0.62; 0.47–0.77; p = ns). Comparison was not done with proteinuria as it was present in all patients with LN and was used to define AN category (Supplementary Fig. 1).
In the follow-up study of AN patients, the level of urinary sCD163 dropped significantly from baseline at all the subsequent visits (Table 2, Fig. 3a). In contrast, plasma sCD163 levels showed a drop at 3 and 6 months, but rose significantly at 9 months and then fell significantly at 12 months (Table 2, Fig. 3b, Supplementary Fig. 2).

Scatter plot showing (a) urinary sCD163 and (b) plasma sCD163 in AN group at different time points
Among the patients in AN group, three patients had relapse of nephritis at 6, 11, and 12 months respectively and one had active disease not responding to cyclophosphamide. She was treated with rituximab at 3 months but developed chronic kidney disease at 6 months. The trends in the levels of urinary sCD163 for these four patients were suggestive of rise in the levels even before clinical deterioration/relapse. (Fig. 4).

Normalized uCD163 levels in patients with relapse (n = 3) and poor renal outcome (n = 1)
Discussion
Through this study, we have demonstrated that sCD163 in urine from patients with active LN is significantly higher as compared with the urinary levels in patients with active disease without nephritis, inactive lupus, healthy individuals, and rheumatoid arthritis patients (inflammatory disease control). It also correlates modestly with disease activity parameters in cross-sectional analysis and, in longitudinally analysis, its levels fall with response to therapy. In limited number of patients, urinary sCD163 rose before clinical relapse/deterioration of LN.
Lupus is a disease associated with increased formation of apoptotic cells and neutrophil extracellular traps releasing a number of autoantigens. Because of the defective phagocytic function of macrophages, these uncleared autoantigens lead to breakdown of immune homeostasis and activate myriad of immune cells like B cells, T cells, and dendritic cells leading to full-blown autoimmune syndrome [11]. Macrophages in SLE develop into both its major subtypes, i.e., classically activated M1 macrophages and alternatively activated M2 macrophages. However, a number of observations have suggested that M2 macrophages play an important role in pathogenesis of various manifestations of SLE. Since M2 macrophages express the proteolytically cleavable marker CD163, its soluble form could therefore serve as a surrogate marker for M2 macrophage presence and activation.
Nakayama et al. showed that M2 macrophages infiltrate the skin in patients with SLE and these patients have elevated plasma levels of sCD163 [12]. Plasma sCD163 levels in this study were higher in active SLE but did not differ between AN and ANR which suggests that plasma levels reflect only systemic inflammation and not renal inflammation. Another study by Nishino et al. also noted significant difference in serum levels of soluble CD163 between patients with LN and healthy controls. Interestingly, this study also did not find any significant difference in the serum sCD163 levels between patients of active SLE with or without LN, which again suggests that the serum levels of sCD163 fail to reflect renal disease activity [13]. Similarly, Zizzo et al. and Zhu et al. have also shown correlation between serum sCD16 and SLEDAI as well as with other soluble markers of M2c macrophages like sMER [14, 15]. Together, these observations about the serum soluble markers of macrophages correlating with disease activity in SLE prove that they reflect only the systemic disease activity. However, none of these studies had evaluated urinary levels of the respective biomarkers.
In the background of the observations made by O’Reilly et al. [6] regarding urinary sCD163 in a few patients of LN, we explored its utility as a potential biomarker of LN. In our study, we observed that urinary sCD163 was significantly higher among patients with AN as compared with all other groups including RA which suggests that sCD163 in urine is not just a marker of systemic inflammation but specifically represents the renal inflammation. Urinary sCD163 correlated with different disease activity parameters in AN group whereas plasma sCD163 did not. These observations imply that as compared with non-renal active disease, in LN, there is local activation of M2 macrophages in the kidneys leading to production of sCD163 by proteolysis that is reflected in the urine.
This may suggest a role for M2 macrophages in LN pathogenesis. Renal biopsy findings from another study on LN patients show infiltration of CD163+ macrophages in tubulointerstitial and glomerular lesions which supports their pathogenic role [16, 17]. Accordingly, one study has shown that urinary sCD163 may serve as a biomarker of LN [17]. However, this study did not include patients with active non-renal disease and inactive disease and, hence, it could not be assessed if it was elevated only in LN or in all patients of SLE to conclude on its utility as a biomarker. Furthermore, another major limitation of the study was that no longitudinal data was included to know the effect of treatment on levels of urinary sCD163 which is essential for it to be used as a biomarker.
In the follow-up part of our study, we showed that urinary sCD163 levels decreased significantly after treatment within 3 months and stayed low for full 1 year suggesting that it can be a potential marker of treatment response. We had earlier shown that another macrophage marker MCP-1 correlates with renal disease activity in LN [18]. This suggests that with response to treatment, macrophage activation is reduced in kidneys and further supports their pathogenic role in LN.
In longitudinal part of this study over 1 year, we could demonstrate though in a limited number of patients, that in cases with relapse of LN or poor response to therapy, urinary sCD163 rises before the clinical relapse/deterioration which may suggest that it could be a potential marker for prediction of poor treatment response. Validation in a larger cohort with relapses may help know its true potential.
Recent data has shown that macrophages constitute the largest number of cells in the urinary sediment which is a valuable information in terms of pathogenesis of LN [3]. In AAV with renal involvement, it has been shown that urinary sCD25 detection complements the urinary sCD163 in detecting active renal disease which may mean that T cells may be helped by macrophages in causing LN [19]. Earlier, we have also looked at the soluble markers of T cell activation and markers of B cell and macrophages and have noted a good correlation of these markers with disease activity in LN [18, 20, 21]. The findings on glomerulonephritis in AAV and our findings in LN converge the concepts of pathogenesis of nephritis in both the diseases and sharing of the biomarker specificities. It could be postulated that macrophages help the cells of adaptive immune system in propagating the disease [22].
Predominance of M2 macrophages which are “anti-inflammatory” and pro-fibrotic in nature on renal biopsies in LN leaves us with the perplexing question about their role in an “inflammatory” active LN [23]. The explanations could be that the pro-inflammatory subtypes of macrophages are the early players (subclinical phase of LN) in LN pathogenesis which set the stage for the adaptive immune system to take over the inflammation and perpetuate the damage and these are later replaced by anti-inflammatory subtypes of macrophages by the time the clinical disease sets in. Another explanation could be that the drugs used for treating LN are known to increase the CD163 expression and thereby M2 phenotype in macrophages [3].
To conclude, we have shown that urinary sCD163 is a potential biomarker of LN disease activity. It can differentiate between lupus patients who have active disease with nephritis from the ones who have active disease without nephritis. Its levels correlate with conventional disease activity parameters and decrease as the disease activity decreases with treatment. Thus, it is a good marker of lupus nephritis activity.
References
Misra R, Gupta R (2009) Biomarkers in lupus nephritis. Int J Rheum Dis 18:219–232
Kopetschke K, Klocke J, Grießbach AS et al (2015) The cellular signature of urinary immune cells in lupus nephritis: new insights into potential biomarkers. Arthritis Res Ther 17:94
Olmes G, Büttner-Herold M, Ferrazzi F, Distel L, Amann K, Daniel C (2016) CD163+ M2c-like macrophages predominate in renal biopsies from patients with lupus nephritis. Arthritis Res Ther 18:–90
Bhattacharya S, Aggarwal A (2019) M2 macrophages and their role in rheumatic diseases. Rheumatol Int 39:769–780
Kishimoto D, Kirino Y, Tamura M et al (2018) Dysregulated heme oxygenase-1low M2-like macrophages augment lupus nephritis via Bach1 induced by type I interferons. Arthritis Res Ther 20:64
O’Reilly VP, Wong L, Kennedy C et al (2016) Urinary soluble CD163 in active renal vasculitis. J Am Soc Nephrol 27:2906–2916
Hochberg MC (1997) Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 40:1725
Gladman DD, Ibañez D, Urowitz MB (2002) Systemic lupus erythematosus disease activity index 2000. J Rheumatol 29:288–291
Hahn BH, McMahon MA, Wilkinson A et al (2012) American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res 64:797–808
The American College of Rheumatology response criteria for proliferative and membranous renal disease in systemic lupus erythematosus clinical trials. Renal Disease Subcommittee of the American College of Rheumatology Ad Hoc Committee on Systemic Lupus Erythematosus Response Criteria. (2006) Arthritis Rheum 54:421–32
Ma C, Xia Y, Yang Q, Zhao Y (2019) The contribution of macrophages to systemic lupus erythematosus. Clin Immunol 207:1–9
Nakayama W, Jinnin M, Makino K et al (2012) CD163 expression is increased in the involved skin and sera of patients with systemic lupus erythematosus. Eur J Dermatol 22:512–517
Nishino A, Katsumata Y, Kawasumi H, Hirahara S, Kawaguchi Y, Yamanaka H (2019) Usefulness of soluble CD163 as a biomarker for macrophage activation syndrome associated with systemic lupus erythematosus. Lupus 986–994
Zizzo G, Guerrieri J, Dittman LM, Merrill JT, Cohen PL (2013) Circulating levels of soluble MER in lupus reflect M2c activation of monocytes/macrophages, autoantibody specificities and disease activity. Arthritis Res Ther 15(6):R212
Zhu H, Sun X, Zhu L, Hu F, Shi L, Li Z, Su Y (2014) The expression and clinical significance of different forms of Mer receptor tyrosine kinase in systemic lupus erythematosus. J Immunol Res 2014:431896
Li J, Liu CH, Xu DL, Gao B (2015) Significance of CD163-positive macrophages in proliferative glomerulonephritis. Am J Med Sci 350:387–392
Endo N, Tsuboi N, Furuhashi K, Shi Y, du Q, Abe T, Hori M, Imaizumi T, Kim H, Katsuno T, Ozaki T, Kosugi T, Matsuo S, Maruyama S (2016) Urinary soluble CD163 level reflects glomerular inflammation in human lupus nephritis. Nephrol Dial Transplant 31:2023–2033
Gupta R, Yadav A, Aggarwal A (2016) Longitudinal assessment of monocyte chemoattractant protein-1 in lupus nephritis as a biomarker of disease activity. Clin Rheumatol 35(11):2707–2714
Dekkema GJ, Abdulahad WH, Bijma T, Moran SM, Ryan L, Little MA, Stegeman CA, Heeringa P, Sanders JSF (2019) Urinary and serum soluble CD25 complements urinary soluble CD163 to detect active renal anti-neutrophil cytoplasmic autoantibody-associated vasculitis: a cohort study. Nephrol Dial Transplant 34:234–242
Gupta R, Yadav A, Misra R, Aggarwal A (2015) Urinary sCD25 as a biomarker of lupus nephritis disease activity. Lupus 24:273–279
Phatak S, Chaurasia S, Mishra SK, Gupta R, Agrawal V, Aggarwal A, Misra R (2017) Urinary B cell activating factor (BAFF) and a proliferation-inducing ligand (APRIL): potential biomarkers of active lupus nephritis. Clin Exp Immunol 187:376–382
Moran SM, Monach PA, Zgaga L et al (2020) Urinary soluble CD163 and monocyte chemoattractant protein-1 in the identification of subtle renal flare in anti-neutrophil cytoplasmic antibody-associated vasculitis. Nephrol Dial Transplant 35(2):283–291
Lu J, Cao Q, Zheng D, Sun Y, Wang C, Yu X, Wang Y, Lee VWS, Zheng G, Tan TK, Wang X, Alexander SI, Harris DCH, Wang Y (2013) Discrete functions of M2a and M2c macrophage subsets determine their relative efficacy in treating chronic kidney disease. Kidney Int 84:745–755
Funding
This project was partially supported by the Dept. of Biotechnology, Government of India research grant (BT/PR15397/MED/30/604/2011) to AA and partially by the India Rheumatology Association (IRA) research grant to RG.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The institutional ethics committee approved the study and informed consent was taken from all the enrolled patients and control subjects.
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(PDF 128 kb)
Rights and permissions
About this article

Cite this article
Gupta, R., Yadav, A. & Aggarwal, A. Urinary soluble CD163 is a good biomarker for renal disease activity in lupus nephritis. Clin Rheumatol 40, 941–948 (2021). https://doi.org/10.1007/s10067-020-05343-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-020-05343-6