
Abstract
The international classification criteria for definite antiphospholipid syndrome (APS) include three laboratory measurements: lupus anticoagulant (LA), IgG and IgM isotypes of anti-cardiolipin (aCL) and anti-β2glycoprotein I antibodies (anti-β2GPI). When persistently elevated, they are specific for APS; however, many patients that fulfil clinical criteria may exhibit negative serological results. These “seronegative” APS (SN-APS) are exposed to an increased thrombotic risk. The aims of our cross-sectional, retrospective study of consecutive autoimmune patients’ samples were to evaluate the association of non-criteria antiphospholipid antibodies (aPL) with thrombosis and obstetric events, to calculate the risk score for adverse events and to assess the specific contribution of single aPL positivity in SN-APS. LA, aCL, anti-β2GPI and anti-phosphatidylserine/prothrombin antibodies (aPS/PT) of IgG, IgM, and IgA isotypes were determined in sera of 323 patients with autoimmune disorders. Medical records of all patients were carefully analyzed. aCL, anti-β2GPI and aPS/PT of IgG and IgA isotypes were significantly associated with thrombosis while none of the IgM aPL showed such association. aPS/PT of all isotypes, aCL and anti-β2GPI of IgG and IgA isotype showed significant correlation to obstetric events. When considering results of aPS/PT ELISA, we could additionally identify 3% of thrombotic patients and 2% of obstetric patients. Thrombotic and obstetric risk scores were calculated showing significantly higher association to clinical events, as compared to evaluating individual risk factors. aPS/PT could represent an additional biomarker in SN-APS patients. IgA aPL are associated with thrombosis and obstetric complications. Risk scores accounting different aPL and conventional risk factors, better assesses risk for adverse event, as compared to evaluating individual factors alone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Antiphospholipid syndrome (APS) is an autoimmune disease characterized by recurrent thrombosis or pregnancy complications, along with persistently present antiphospholipid antibodies (aPL) [1]. Lupus anticoagulant (LA), anti-cardiolipin (aCL) and anti-β2-glycoprotein I antibodies (anti-β2GPI), of IgG and/or IgM isotype are the laboratory biomarkers included in the 2006 revised APS classification criteria. However, it is well known that aPL antibodies are heterogeneous in function and specificity, comprising of IgG, IgM and IgA isotypes, and individual tests may recognize various subtypes of antibodies. Furthermore, there are patients strongly suspected of having APS by their clinical phenotype, but persistently negative for any currently tested aPL [2]. Recently, the concept of “seronegative APS” (SN-APS) has been coined to describe a particular group of patients with clinical manifestation highly suggestive of APS and “non-criteria” aPL, i.e. autoantibodies targeting other plasma proteins or phospholipid-bound proteins complexes [3, 4]. Several authors have suggested that testing for new aPL specificities, may help to identify the syndrome in patients with thrombosis or pregnancy loss.
Antibodies against prothrombin emerged as a potential marker for APS and many reports have confirmed the association between antibodies against phosphatidylserine/prothrombin complexes (aPS/PT) and clinical manifestations of APS. Our group developed an in-house aPS/PT ELISA [5] and reported that these antibodies are detected in some of the SN-APS patients and are advantageous in distinguishing patients at greater risk for thrombosis [6,7,8]. Moreover, we found these antibodies to be the strongest independent risk factor for the aPL-related obstetric complications [8].
The issue of the value of IgA aPL antibodies and their inclusion in the diagnostic algorithm of APS has been a subject of debate since 2006, when the international consensus report concluded that available data for establishing IgA, as an independent risk factor for APS is inadequate. The following literature on IgA aPL is quite diverse, reporting a high variability in its prevalence, as well as clinical significance. However, several experimental data published in recent years showed the potential pathogenic role of IgA aCL and IgA anti-β2GPI [9,10,11,12,13,14]. These antibodies have been reported in up to 70% of patients with systemic lupus erythematosus (SLE) and in those with primary APS [15].
Recently, two research groups proposed a quantitative index in an attempt to quantify the probability of thrombosis in APS. The aPL score (aPL-S), comprising aPL profile [16] and the global APS score (GAPSS), comprising both aPL profile and conventional prothrombotic risk factors [17]. Both groups included LA, aCL, anti-β2GPI of IgG and IgM isotype as well as IgG/M aPS/PT; however, none included IgA aPL measurements in their calculations. Two validation studies have previously been published in order to support clinical assessment of GAPSS [18, 19].
In order to evaluate the advantage of detection of non-criteria aPL, including IgA aCL, IgA anti-β2GPI and IgG/M/A aPS/PT for patients with chronic rheumatic diseases, their added value for diagnostic and risk purposes was determined. Our aims in this study were first, to systematically record conventional risk factors for thrombotic events, together with aPL positivity and evaluate their association to thrombosis in patients with different systemic autoimmune diseases. Secondly, to analyze the value of non-criteria aPL in the APS risk calculations, separately for thrombosis and obstetric manifestations and thirdly, to assess the specific contribution of single aPL positivity in SN-APS.
Materials and methods
Participants
This retrospective, cross-sectional study included all patients who were tested for aPL at the Immunology laboratory between January 2014 and November 2014. The laboratory is part of the Department of Rheumatology, University Medical Centre Ljubljana. The study was approved by the National Medical Ethics Committee, Ljubljana, Slovenia (#99/04/15), and all patients provided informed consent.
Among 804 consecutive patient samples tested for aPL, clinical data was obtained for 323 patients (230 females, 93 males) (Table 1). Of these, 106 patients had APS, specifically, 91 primary APS and 15 APS associated to other autoimmune disease. Non-APS patients (n = 217) had the following diagnoses: cerebrovascular insult (18), SLE (53), rheumatoid arthritis (14), Sjögren’s syndrome (34), systemic sclerosis (7), spondyloarthritis (34), giant cell arteritis (26), other vasculitis (25) and polymyalgia rheumatica (6).
Data collection
Patient medical records were analyzed and the following was recorded at the time of obtaining sera: age, gender, obesity (body mass index > 25 kg/m2), smoking status, ascertain by self-report (smokers, ex-smokers and non-smokers), arterial hypertension (systolic pressure ≥ 140 mmHg, or diastolic pressure ≥ 95 mmHg, on at least two occasions, or use of oral anti-hypertensive drugs), treatment status including oral contraception (current or at the event), diabetes (fasting glucose value ≥ 7.0 mmol/L on at least two occasions or use of insulin or oral hypoglycaemic medication), history of venous or arterial thrombosis and history of obstetric complications, included in the APS classification criteria [1].
Serological parameters
At the time of the visit, patient sera were measured for aPL profile including LA, aCL, anti-β2GPI, aPS/PT of IgG, IgM and IgA isotype. Lipid levels and platelet count were regularly recorded. Hyperlipidaemia was defined as serum total cholesterol > 5.2 mmol/L or LDL > 3.5 mmol/L, or use of cholesterol-lowering medications and thrombocytopenia was defined as platelet count < 140 × 109/L.
Anti-phospholipid antibody measurements
In-house aPS/PT ELISA
In-house aPS/PT ELISA was performed as previously described [20]. Briefly, medium-binding microtitre plates were coated with phosphatidylserine in chloroform/methanol 1:4 and blocked with 1% bovine serum albumin (BSA) in Tris-buffered saline (TBS) containing 5 mM CaCl2 (1% BSA/TBS-Ca). Human prothrombin (Enzyme Research Laboratories, Ltd., Swansea, UK) [10 mg/L] and patients’ sera diluted 1:100 in 1% BSA/TBS-Ca were applied to wells immediately one after the other and incubated for 1 h. After washing with 5 mM CaCl2-TBS-0.05% Tween 20, alkaline phosphatase-conjugated goat anti-human IgG/IgM/IgA (ACSC, Westbury, USA) were applied in 1% BSA/TBS-Ca and incubated for 30 min. Binding of antibodies was detected with para-nitrophenylphosphate (Sigma Chemical Company, St. Louis, USA) in diethanolamine buffer (pH 9.8) and OD405 was kinetically measured by a spectrometer (Tecan Sunrise Remote, Grödig, Austria).
In-house aCL ELISA
IgG, IgM and IgA aCL were determined according to the previously described method [21]. Briefly, medium-binding microtitre plates were coated with cardiolipin and blocked with 10% fetal bovine serum (FBS) in phosphate-buffered saline (PBS). After washing with PBS, diluted samples in 10% FBS-PBS were applied and incubated at room temperature (RT) for 2.5 h. The detection system was the same as in aPS/PT ELISA.
In-house anti-β2GPI ELISA
In-house anti-β2GPI ELISA was performed as previously described [22] and evaluated through the European forum for aPL [23]. Briefly, high-binding polystyrene microtitre plates coated with 50 μl/well of β2GPI (10 mg/L) in PBS were incubated for 2 h at RT. The plates were then washed with PBS containing 0.05% Tween-20 (PBS-Tween) and incubated with samples diluted in PBS-Tween for 30 min at RT. The detection system was the same, as in aPS/PT ELISA.
Lupus anticoagulant
The assay was performed in blood samples collected in tubes containing 0.109 M sodium citrate. Platelet-poor plasma was obtained by centrifugation at 2400g for 20 min at 4 °C. After filtration, aliquots were stored at − 80 °C until use. Clotting tests were performed using coagulation analyzer BCS Siemens, according to the previous guidelines of the International Society on Thrombosis and Haemostasis ISTH [26]. Simplified Dilute Russell’s Viper Venom Test (dRVVT) was performed using LA1 screening reagent and LA2 confirmatory reagent (Siemens) following manufacturer’s instructions [27]. A dRVVT ratio (LA1 screen/LA2 confirmation) above 1.2 was considered positive for LA activity. Activity of LA was quantified as follows: low positive (LA1/LA2 = 1.2–1.5), medium (LA1/LA2 = 1.5–2.0) and high positive (LA1/LA2 > 2.0).
Statistical analysis
Categorical variables were presented as numbers and percentages, and continuous variables as means. The significance of baseline differences was determined by the χ2 test or the unpaired t test, as appropriate. The results of multivariate logistic models were approximated by odds ratio with its 95% confidence interval (OR [95%]). A two-sided P < 0.05 was considered statistically significant.
Univariate and multivariate logistic regression analyses were used to determine the contribution of a different variable to a specific condition. To calculate and develop the thrombotic risk score (TRS) and the obstetric risk score (ORS), we followed the previously used model for GAPSS score calculations [17]. Briefly, specific risk factors, identified with univariate analysis, were assigned weighted points calculated as its corresponding β-regression coefficient divided by the value of the lowest β-coefficient (βx/βmin). A risk score was then calculated for each patient by adding together the specific weighted points. The receiver operating characteristic (ROC) analysis and the area under the curve (AUC), diagnostic sensitivity, specificity and positive and negative predictive value (PPV and NPV, respectively) were used to assess the diagnostic performance of the TRS, GAPSS and ORS. Statistical analyses were performed using the SPSS 15.0 program.
Results
Analysis of prothrombotic risk factors and aPL for thrombosis
Univariate logistic regression revealed that among conventional prothrombotic risk factors hyperlipidaemia (P = 0.009), arterial hypertension (P = 0.047) and use of oral contraceptives (P = 0.024) were significantly associated with thrombosis in our cohort (Table 2). Next, we also found thrombocytopenia (P = 0.042) and LA (P = 0.019), as well as aCL, anti-β2GPI and aPS/PT of IgG (P ≤ 0.005) and IgA (P ≤ 0.026) isotypes to be significantly associated with thrombosis. On the other hand, not of IgM subtypes of aCL, anti-ß2GPI and aPS/PT showed association to thrombosis.
A thrombotic risk score calculation (TRS) was constructed following the same model as used in GAPSS [17]. Multivariate logistic analysis was used for the calculation of the β-regression coefficient. We assigned a number of points proportional to its β-regression coefficient divided by the value of the lowest β-coefficient (βx/βmin) to each of the 11 variables showing significant correlation to thrombosis. Each patient had calculated both scores, TRS and GAPSS, by adding together the specific weighted points. Both, TRS and GAPSS values were significantly higher in thrombotic than non-thrombotic patients (mean TRS 6.6 vs. 3.5 and mean GAPSS 6.9 vs. 3.9; P < 0.001), showing similar area under the ROC curve (AUC = 0.649 and AUC = 0.666, respectively) (Table 3).
Analysis of aPL for obstetric complications
Among 235 female patients, 147 patients had a relevant obstetric history. For the remaining patients, they were either not pregnant or data was not available. Forty-three patients had a history of obstetric complications, as included in the APS classification criteria. Specifically, 15 experienced three or more unexplained consecutive miscarriages before the 10th week of gestation, 16 experienced unexplained death of a morphologically normal foetus after the 10th week of gestation, and 12 patients gave premature birth to a morphologically normal neonate before the 34th week of gestation, due to eclampsia, preeclampsia or placental insufficiency. The control group comprised of 104 female patients with different autoimmune conditions, negative for obstetric and thrombotic events.
A univariate logistic regression revealed that all aPL, except LA, aCL IgM and anti-β2GPI IgM, were statistically significantly associated with obstetric complications (P ≤ 0.022) (Table 4).
The obstetric risk score (ORS) was calculated in the same manner, as TRS. ORS values were significantly higher in patients with a history of obstetric complications compared to patients without obstetric complications (mean ORS 10.07 vs. 2.85 P < 0.001), with ROC curve (AUC = 0.705 and diagnostic sensitivity 0.565 and specificity 0.832) (Table 5).
Added value of non-criteria aPL for thrombosis and obstetric complications
We investigated the distribution of aPL positivity in the cohort of patients with a history of thrombosis (n = 116) and in the cohort of patients with a history of obstetric complications (n = 43).
In the group of patients with thrombosis, 13.0% had IgA aCL, 15.5% IgA anti-β2GPI and 24.1% aPS/PT (Table 2). In the group of patients with obstetric complications, 11.1% had IgA aCL, 16.3% IgA anti-β2GPI and 34.9% aPS/PT (Table 4).
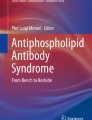
None of the patients was single positive for IgA aCL or IgA anti-β2GPI; however, three patients in the thrombotic cohort and one patient in the obstetric cohort expressed a single aPS/PT positivity (Fig. 1). In our cohort of autoimmune patients, we could additionally identify (3/116) 3% thrombotic patients and (1/43) 2% obstetric patients, when considering results of aPS/PT ELISA.

Distribution of aPL positivity among patients with a history of thrombosis (n = 116) and obstetric complications (n = 43)
Discussion
In current clinical practice, aCL and anti-β2GPI detected by ELISA and the LA detected by clotting assays are the laboratory classification biomarkers for APS [1]. There have been many attempts to improve and standardize these methods since each individual method has several drawbacks. In addition, LA measurement is precluded by concurrent anticoagulant treatment [24].
Next, these tests may give negative results, even though a diagnosis of APS is very likely due to typical, often multiple clinical manifestations (SN-APS patients). Clinicians occasionally test for non-criteria aPL such as IgA aCL, IgA anti-β2GPI or IgG/M/A aPS/PT antibodies. Several studies have found an association between IgA anti-β2GPI and an increased risk of thromboembolic vascular disease [9, 12, 25]. A systematic literature review concluded that routine measurement of aPS/PT antibodies of IgG and/or IgM isotype might be useful in supporting data for establishing thrombotic risk of patients with previous thrombosis or SLE [26]. In addition, a very recent international multicentre study advised measurement of IgG aPS/PT that might contribute to a better and more complete identification of patients with APS [27]. Our group recently showed IgA aPS/PT to highly correlate with LA activity and thrombosis [28].
The present study is, to our knowledge, the first to date, analysing IgA aCL and IgA anti-β2GPI as well as aPS/PT of all three isotypes, measured in a routine clinical laboratory practice, evaluating their potential as an added value (e.g. non-criteria aPL). We found a significant association between the presence of IgA aCL, IgA anti-β2GPI and IgG/IgA aPS/PT and thrombotic event. Conversely an association between IgM aPL and thrombosis was not confirmed. Although none of the patients was single positive for IgA aPL, we clearly showed that these antibodies were present in APS patients and were associated with an increased risk for thrombotic vascular events.
Furthermore, three patients (one with a history of arterial thrombosis, the second with a history of venous thrombosis and the third with a history of venous thrombosis and foetal death during the second trimester of pregnancy) expressed single aPS/PT positivity. Besides, aPS/PT levels were persistently elevated in 2 years of follow-up and none of the patients later became positive either for aCL, anti-β2GPI or LA. Therefore, in our cohort of autoimmune patients, we could additionally identify 3% thrombotic patients and 2% obstetric patients, when considering the results of the aPS/PT ELISA. These results confirmed our previous study, where we reported that aPS/PT are associated with adverse pregnancy outcome and that these antibodies are the only aPL associated with early pregnancy complications [8].
Recently, two research groups proposed different quantitative scoring (aPL-S and GAPSS) in which testing for multiple aPL may better evaluate thrombotic risk in APS patients instead of individual aPL measurements [16, 17]. Both risk scores include aPL profiles of IgG and IgM isotypes; however, none comprises IgA measurements. Since IgM isotype of aPL was not independently associated with thromboses in our cohort, but IgA did, we constructed a version of thrombotic risk scoring TRS, that included also the IgA isotype. We found 11 variables to be independently associated with thrombosis including hyperlipidaemia, arterial hypertension, use of oral contraceptives, thrombocytopenia, LA, aCL, anti-β2GPI and aPS/PT of IgG and IgA isotypes. Additionally to TRS, we calculated GAPSS in our cohort of patients for the exact comparison. Both, TRS and GAPSS values were significantly higher in thrombotic than non-thrombotic patients, showing similar area under ROC curve (AUC = 0.689 and AUC = 0.690, respectively). Although different aPL profiles were included in both scoring calculations, no apparent difference was found. In our cohort, GAPSS > 4 produced the highest AUC, which is lower than the cut-off (GAPSS > 10) proposed by the original study [17].
Moreover, in the present study, we are proposing quantitative scoring also for evaluating the risk of adverse pregnancy events in aPL-positive patients namely the obstetric risk score—ORS. Similar to GAPSS and TRS calculations, ORS comprises all with obstetric manifestations significantly associated aPL, specifically aCL and anti-β2GPI of IgG and IgA isotypes, as well as all three isotypes of aPS/PT antibodies. ORS was significantly higher in patients with a history of obstetric events as compared to patients without and showed much higher diagnostic accuracy as compared to each individual aPL measurement. Our results show that scoring calculations can be a suitable quantitative marker for APS; however, we are also suggesting that improved scoring systems are needed.
Conclusions
All non-criteria aPL, including IgA aCL, IgA anti-β2GPI and IgA/IgG aPS/PT were significantly associated to thrombosis. aPS/PT could represent an additional biomarker in SN-APS patients. Importantly, following 2 years of systematic testing, three patients were serologically identified as single aPS/PT positive. Risk scores including non-criteria aPL in addition to conventional risk factors, better assesses risk for adverse events, as compared to evaluating individual factors alone. An update of the current classification criteria for APS should be considered, incorporating new serological markers into a potential quantitative index, acting as a predictive marker for adverse events.
Take home messages:
• aCL, anti-β2GPI and aPS/PT of IgG and IgA isotype are associated with thrombosis.
• aPS/PT (all isotypes), aCL (IgG and IgA) and anti-β2GPI (IgG and IgA) are associated with obstetric complications.
• aPS/PT could represent an additional biomarker for SN-APS patients.
• Thrombotic and obstetric risk scores better assess risk for adverse events as compared to evaluating individual factors alone.
References
Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, Derksen RH, De Groot PG, Koike T, Meroni PL, Reber G, Shoenfeld Y, Tincani A, Vlachoyiannopoulos PG, Krilis SA (2006) International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). JThrombHaemost 4(2):295–306
Hughes GR, Khamashta MA (2003) Seronegative antiphospholipid syndrome. Ann Rheum Dis 62(12):1127
Bertolaccini ML, Amengual O, Atsumi T, Binder WL, de LB FR, Kutteh WH, Lambert M, Matsubayashi H, Murthy V, Petri M, Rand JH, Sanmarco M, Tebo AE, Pierangeli SS (2011) ‘Non-criteria’ aPL tests: report of a task force and preconference workshop at the 13th International Congress on Antiphospholipid Antibodies, Galveston, TX, USA, April 2010. Lupus 20(2):191–205
Zohoury N, Bertolaccini ML, Rodriguez-Garcia JL, Shums Z, Ateka-Barrutia O, Sorice M, Norman GL, Khamashta M (2017) Closing the serological gap in the antiphospholipid syndrome: the value of “non-criteria” antiphospholipid antibodies. J Rheumatol 44(11):1597–1602. https://doi.org/10.3899/jrheum.170044
Zigon P, Ambrozic A, Cucnik S, Kveder T, Rozman B, Bozic B (2011) Modified phosphatidylserine-dependent antithrombin ELISA enables identification of patients negative for other antiphospholipid antibodies and also detects low avidity antibodies. Clin Chem Lab Med 49(6):1011–1018
Zigon P, Cucnik S, Ambrozic A, Kveder T, Semrl SS, Rozman B, Bozic B (2013) Detection of antiphosphatidylserine/prothrombin antibodies and their potential diagnostic value. Clin Dev Immunol 2013:8–8. https://doi.org/10.1155/2013/724592
Zigon P, Cucnik S, Ambrozic A, Sodin Semrl S, Kveder T, Bozic B (2012) Antibodies to phosphatidylserine/prothrombin complex as an additional diagnostic marker of APS? Lupus 21(7):790–792. https://doi.org/10.1177/0961203312444173
Zigon P, Perdan Pirkmajer K, Tomsic M, Kveder T, Bozic B, Sodin Semrl S, Cucnik S, Ambrozic A (2015) Anti-phosphatidylserine/prothrombin antibodies are associated with adverse pregnancy outcomes. J Immunol Res 2015:975704–975708. https://doi.org/10.1155/2015/975704
Ciesla M, Wypasek E, Undas A (2014) IgA antiphospholipid antibodies and anti-domain 1 of Beta 2 glycoprotein 1 antibodies are associated with livedo reticularis and heart valve disease in antiphospholipid syndrome. Adv Clin Exp Med 23(5):729–733
Hood DB, Snyder KR, Buckner TR, Hurley BL, Pitts KR, Lopez LR (2015) Differential assay reactivity of immunglobulin a anti-beta(2) glycoprotein I antibodies: implications for the clinical interpretation of antiphospholipid antibody testing. Eur J Rheumatol 2(4):135–138. https://doi.org/10.5152/eurjrheum.2015.0012
Mavropoulos A, Sully G, Cope AP, Clark AR (2005) Stabilization of IFN-gamma mRNA by MAPK p38 in IL-12- and IL-18-stimulated human NK cells. Blood 105(1):282–288. https://doi.org/10.1182/blood-2004-07-2782
Meijide H, Sciascia S, Sanna G, Khamashta MA, Bertolaccini ML (2013) The clinical relevance of IgA anticardiolipin and IgA anti-beta2 glycoprotein I antiphospholipid antibodies: a systematic review. Autoimmun Rev 12(3):421–425. https://doi.org/10.1016/j.autrev.2012.08.002
Despierres L, Beziane A, Kaplanski G, Granel B, Serratrice J, Cohen W, Bretelle F, Rossi P, Morange PE, Weiller PJ, Robert Harle J, Bongrand P, Bardin N (2014) Contribution of anti-beta2glycoprotein I IgA antibodies to the diagnosis of anti-phospholipid syndrome: potential interest of target domains to discriminate thrombotic and non-thrombotic patients. Rheumatology (Oxford) 53(7):1215–1218. https://doi.org/10.1093/rheumatology/keu003
Paulmyer-Lacroix O, Despierres L, Courbiere B, Bardin N (2014) Antiphospholipid antibodies in women undergoing in vitro fertilization treatment: clinical value of IgA anti-beta2glycoprotein I antibodies determination. Biomed Res Int 2014:314704–314705. https://doi.org/10.1155/2014/314704
Andreoli L, Fredi M, Nalli C, Piantoni S, Reggia R, Dall'Ara F, Franceschini F, Tincani A (2013) Clinical significance of IgA anti-cardiolipin and IgA anti-beta2glycoprotein I antibodies. Curr Rheumatol Rep 15(7):343. https://doi.org/10.1007/s11926-013-0343-1
Otomo K, Atsumi T, Amengual O, Fujieda Y, Kato M, Oku K, Horita T, Yasuda S, Koike T (2012) Efficacy of the antiphospholipid score for the diagnosis of antiphospholipid syndrome and its predictive value for thrombotic events. Arthritis Rheum 64(2):504–512. https://doi.org/10.1002/art.33340
Sciascia S, Sanna G, Murru V, Roccatello D, Khamashta MA, Bertolaccini ML (2013) GAPSS: the global anti-phospholipid syndrome score. Rheumatology (Oxford) 52(8):1397–1403. https://doi.org/10.1093/rheumatology/kes388
Oku K, Amengual O, Bohgaki T, Horita T, Yasuda S, Atsumi T (2015) An independent validation of the global anti-phospholipid syndrome score in a Japanese cohort of patients with autoimmune diseases. Lupus 24(7):774–775. https://doi.org/10.1177/0961203314561284
Zuily S, de Laat B, Mohamed S, Kelchtermans H, Shums Z, Albesa R, Norman GL, Lamboux-Matthieu C, Rat AC, Ninet J, Magy-Bertrand N, Pasquali JL, Lambert M, Lorcerie B, Kaminsky P, Guillemin F, Regnault V, Wahl D (2015) Validity of the global anti-phospholipid syndrome score to predict thrombosis: a prospective multicentre cohort study. Rheumatology (Oxford) 54(11):2071–2075. https://doi.org/10.1093/rheumatology/kev238
Zigon P, Ambrozic A, Cucnik S, Kveder T, Rozman B, Bozic B (2011) Modified phosphatidylserine-dependent antiprothrombin ELISA enables identification of patients negative for other antiphospholipid antibodies and also detects low avidity antibodies. Clin Chem Lab Med 49(9):1573
Bozic B, Kveder T, Stegnar M, Morosini-Berus E, Kos-Golja M, Peternel P, Rozman B (1997) Influence of degraded phosphatidylserine on binding of antiphospholipid antibodies. IntArchAllergy Immunol 112(1):19–26
Čučnik S, Krizaj I, Rozman B, Kveder T, Božič B (2004) Concomitant isolation of protein C inhibitor and unnicked beta2-glycoprotein I. ClinChemLab Med 42(2):171–174
Reber G, Schousboe I, Tincani A, Sanmarco M, Kveder T, De MP, Boffa MC, Arvieux J (2002) Inter-laboratory variability of anti-beta2-glycoprotein I measurement. A collaborative study in the frame of the European forum on antiphospholipid antibodies standardization group. ThrombHaemost 88(1):66–73
Chighizola CB, Raschi E, Banzato A, Borghi MO, Pengo V, Meroni PL (2016) The challenges of lupus anticoagulants. Expert Rev Hematol 9(4):389–400. https://doi.org/10.1586/17474086.2016.1140034
Mattia E, Ruffatti A, Tonello M, Meneghel L, Robecchi B, Pittoni M, Gallo N, Salvan E, Teghil V, Punzi L, Plebani M (2014) IgA anticardiolipin and IgA anti-beta2 glycoprotein I antibody positivity determined by fluorescence enzyme immunoassay in primary antiphospholipid syndrome. Clinical chemistry and laboratory medicine : CCLM / FESCC 52:1329–1333. https://doi.org/10.1515/cclm-2014-0039
Sciascia S, Sanna G, Murru V, Roccatello D, Khamashta MA, Bertolaccini ML (2013) Anti-prothrombin (aPT) and anti-phosphatidylserine/prothrombin (aPS/PT) antibodies and the risk of thrombosis in the antiphospholipid syndrome: a systematic review. Thrombosis and Haemostasis 111(2):354–364. https://doi.org/10.1160/TH13-06-0509
Amengual O, Forastiero R, Sugiura-Ogasawara M, Otomo K, Oku K, Favas C, Delgado Alves J, Zigon P, Ambrozic A, Tomsic M, Ruiz-Arruza I, Ruiz-Irastorza G, Bertolaccini ML, Norman GL, Shums Z, Arai J, Murashima A, Tebo AE, Gerosa M, Meroni PL, Rodriguez-Pinto I, Cervera R, Swadzba J, Musial J, Atsumi T (2016) Evaluation of phosphatidylserine-dependent antiprothrombin antibody testing for the diagnosis of antiphospholipid syndrome: results of an international multicentre study. Lupus 26:266–276. https://doi.org/10.1177/0961203316660203
Zigon P, Ambrozic A, Mali P, Tomsic M, Sodin Semrl S, Cucnik S (2017) The prevalence and clinical significance of Iga anti-phosphatidylserine/ prothrombin antibodies in systemic autoimmune diseases. Immunome research 13:130. https://doi.org/10.4172/1745-7580.1000130
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the National Medical Ethics Committee, Ljubljana, Slovenia (#99/04/15), and all patients provided informed consent. We confirm that all experiments were performed in accordance with relevant guidelines and regulations.
Disclosures
None.
Additional information
Rheumatology in Slovenia: Clinical practice and translational research
Rights and permissions
About this article

Cite this article
Žigon, P., Podovšovnik, A., Ambrožič, A. et al. Added value of non-criteria antiphospholipid antibodies for antiphospholipid syndrome: lessons learned from year-long routine measurements. Clin Rheumatol 38, 371–378 (2019). https://doi.org/10.1007/s10067-018-4251-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-018-4251-7