
Abstract
This article critically reviews HPV vaccine serious adverse events described in pre-licensure randomized trials and in post-marketing case series. HPV vaccine randomized trials were identified in PubMed. Safety data were extracted. Post-marketing case series describing HPV immunization adverse events were reviewed. Most HPV vaccine randomized trials did not use inert placebo in the control group. Two of the largest randomized trials found significantly more severe adverse events in the tested HPV vaccine arm of the study. Compared to 2871 women receiving aluminum placebo, the group of 2881 women injected with the bivalent HPV vaccine had more deaths on follow-up (14 vs. 3, p = 0.012). Compared to 7078 girls injected with the 4-valent HPV vaccine, 7071 girls receiving the 9-valent dose had more serious systemic adverse events (3.3 vs. 2.6%, p = 0.01). For the 9-valent dose, our calculated number needed to seriously harm is 140 (95% CI, 79–653). The number needed to vaccinate is 1757 (95% CI, 131 to infinity). Practically, none of the serious adverse events occurring in any arm of both studies were judged to be vaccine-related. Pre-clinical trials, post-marketing case series, and the global drug adverse reaction database (VigiBase) describe similar post-HPV immunization symptom clusters. Two of the largest randomized HPV vaccine trials unveiled more severe adverse events in the tested HPV vaccine arm of the study. Nine-valent HPV vaccine has a worrisome number needed to vaccinate/number needed to harm quotient. Pre-clinical trials and post-marketing case series describe similar post-HPV immunization symptoms.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
There is an ongoing debate on HPV vaccine safety. On the one hand, international regulatory health agencies have endorsed HPV vaccine security [1, 2]. On the other hand, clinicians from different parts of the world have independently described a disabling multisystem illness occurring rarely after HPV immunization [3,4,5,6,7,8,9,10,11,12,13,14]. In response to adverse events reports, Japan’s Health Ministry suspended HPV immunization program in 2013. Internet-based social media have also published dramatic cases of HPV vaccine adverse events. This information led to decreased vaccine uptake in several countries [15]. HPV vaccine is given to healthy youngsters; therefore, of outmost importance is the continuous safety surveillance.
Three different types of HPV vaccine are currently marketed: Cervarix (GlaxoSmithKline) is a bivalent HPV vaccine directed at types 16, 18.Cervarix contains 20 μg of HPV-16 L1 protein and 20 μg of HPV-18 L1 protein assembled as virus-like particles as the vaccine antigens. The L1 proteins are formulated with the adjuvant containing aluminum salts system, which is composed of 50 μg of 3-O-desacyl-4′-monophosphoryl lipid A and 500 μg of aluminum hydroxide salt. Gardasil or Silgard (Merck & Co) is a quadrivalent human recombinant papillomavirus vaccine adsorbed on 225 μg amorphous aluminum hydroxyphosphate sulfate adjuvant and directed at serotypes 6, 11, 16, and 18. There is a new approved HPV vaccine; Gardasil 9, directed at HPV serotypes 6, 11, 16, 18, 31, 33, 45, 52, and 58, adsorbed on 500 μg of amorphous aluminum hydroxyphosphate sulfate adjuvant [16].
This article critically reviews the adverse events, particularly those of serious nature, described in HPV vaccine pre-licensure randomized studies as well as in post-marketing case series.
Methods
Randomized controlled trials on HPV vaccine published up to January 31, 2017 were identified in PubMed with the keywords “HPV vaccine” and the filter “Clinical trial.” Results were screened for randomized controlled trials testing any of the three currently licensed HPV vaccines. The following data were extracted from each randomized study: vaccine type, comparator composition, number of subjects in each arm of the study, gender, age range, adverse events, serious adverse events, vaccine-related serious adverse events, and most frequent adverse symptoms.
Serious adverse event is conventionally defined as any adverse event or adverse reaction that results in death, is life-threatening, requires hospitalization or prolongation of existing hospitalization, results in persistent or significant disability or incapacity, or is a congenital anomaly or birth defect [17].
Post-marketing adverse events case series were identified in PubMed with the keyword “HPV vaccine,” linked to the diagnoses that have been associated to HPV vaccination; complex regional pain syndrome, fibromyalgia, chronic fatigue syndrome, postural orthostatic tachycardia syndrome, or ovarian failure. Post-marketing studies on HPV vaccine safety and international health authorities’ stance in the matter were also analyzed.
Results
Table 1 contains all reviewed HPV vaccine randomized trials [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. The relatively small HPV vaccine randomized double-blind studies did not find significantly increased systemic adverse events in the HPV vaccine group vs. the control group. These studies did not use inert placebo as comparator but rather an aluminum adjuvant or a previously licensed aluminum-containing vaccine (Table 1).
Only one quadrivalent HPV vaccine randomized double-blind trial utilized inert saline placebo [20]. In this trial, boys (n = 842) and girls (n = 939) from 9 to 15 years of age were given the quadrivalent HPV vaccine (n = 1184) or saline placebo (n = 597). When describing efficacy outcomes, boys and girls were separately evaluated. When describing adverse events, they were analyzed in a single group. Safety data included 1165 individuals in the HPV vaccine group vs. 584 in the saline placebo group. The percentage of adverse events was 46.4% in the active ingredient group vs. 44.5% in the placebo group. The difference has no statistical significance. Our calculated 2 × 2 contingency table is p value = 0.24. Serious adverse events occurred in 5 (0.4%) of HPV-vaccinated subjects and none in the placebo group. None of the serious adverse events were considered vaccine-related. In the “Discussion” section, the authors stated “Regardless of vaccination group, a higher proportion of girls than boys reported adverse experiences, although no formal comparisons between genders were performed” [20].
Nine-valent HPV vaccine was compared to saline placebo in only one randomized trial [32]. In this study, 608 females 12–26 years of age were compared to 305 who receive saline placebo. Systemic adverse events were more common in the 9-valent group (59.7 vs. 55.7% in the placebo group). But the difference was not significant (our calculated p value is 0.27).
The FDA webpage on approved products contains the results of several clinical trials in 3088 women from 8 to 26 years of age injected with Gardasil, compared to 3470 age matched women injected with placebo containing amorphous aluminum hydroxyl phosphate sulfate and to 320 women given saline placebo. Injection site swelling developed in 25.4% of women injected with Gardasil, 15.8% injected with aluminum placebo, and 7.3% receiving saline placebo. The intergroup differences are obvious [16].
The bivalent HPV vaccine-manufacturing company performed a pooled safety analysis of all trials comparing bivalent HPV vaccine vs. hepatitis A vaccine. Analysis comprised 29,953 girls and women. In all age groups, some solicited general symptoms reported during the 7-day period after each vaccine dose (fatigue, arthralgia myalgia, and others) were significantly higher in the HPV vaccine group when compared to those of the hepatitis A vaccine cohort [34].
Two of the largest HPV vaccine randomized trials did find significantly more severe adverse events in the tested vaccine group vs. the comparator group: The 4-year interim follow-up VIVIANE study safety analysis compared 2881 healthy women older than 25 years injected with the bivalent HPV vaccine vs. 2871 age-matched women injected with aluminum placebo [29]. As expected in large randomized trials, both groups displayed remarkably similar baseline characteristics. General solicited symptoms during the 7-day post-vaccination period occurred more often in the HPV vaccine group (65%) than those in the control group (58%). Our calculated 2 × 2 contingency table p value was <0.01. Vaccine-related general solicited symptoms during the 7-day post-vaccination period were also more frequent after HPV vaccination (41%) than those after placebo injection (36%) p < 0.001. Fourteen deaths occurred in the vaccine group vs. three deaths in the control group (p = 0.012 by Fisher’s exact test). None of the deaths were believed to be related to vaccination. One less death was reported in the 84-month follow-up VIVIANE study, a woman diagnosed with breast cancer 6 months after the third dose of the vaccine [35]. Even after this correction, the death rate difference (13 vs. 3) remains significant (p = 0.021).
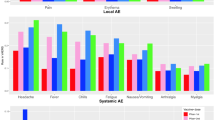
As already stated [36], the largest Gardasil randomized double-blind HPV vaccine study contrasted the 9-valent dose vs. the quadrivalent formulation [30]. The new 9-valent formulation has more than double virus-like particles and aluminum adjuvant than the 4-valent counterpart. The study pre-specified primary end-points were the following: development of high-grade cervical epithelial neoplasia, adenocarcinoma in-situ, cervical cancer, high-grade vulvar intraepithelial neoplasia, high-grade vaginal intraepithelial neoplasia, vulvar cancer, and vaginal cancer. Again, both groups had very similar baseline features. Safety analysis evaluated 7071 women (16 to 26 years of age) immunized with the HPV 9-valent dose vs. 7078 women injected with the quadrivalent HPV formula. Severe (>5 cm) injection site swelling was seen more often in the 9-valent group; 3.8 vs. 1.5% (p < 0.01). Vaccine-related systemic events occurred significantly more frequently in the 9-valent group (n = 2086 or 29.5%) than those in the 4-valent group (n = 1929 or 27.3%). Our calculated p value is 0.003. Serious systemic adverse events were more frequent in the 9-valent arm of the study; 233 (3.3%) vs.183 (2.6%) in the quadrivalent arm. Our calculated p value is 0.0125. Oddly, only two serious adverse events (0%) in each arm of the study were deemed by the investigators to be vaccine-related. In both groups, the most common systemic adverse events related to vaccination (incidence ≥2%) were headache, pyrexia, nausea, dizziness, and fatigue [30].
We characterize the likelihood to be helped or harmed by the 9-valent HPV vaccine as compared to the 4-valent version. The average number needed to vaccinate with the 9-valent dose to prevent one episode of the pre-specified primary end-points that would not otherwise have been prevented by the 4-valent immunization is 1757 with 95% CI ranging from 131 to infinity. The number needed to harm indicates how many individuals on average need to be vaccinated with the 9-valent dose to cause harm (in this case, a serious adverse event) in one individual who would not otherwise have been harmed by the 4-valent dose. This number is 140 with 95% CI ranging from 79 to 653. Therefore, the likelihood to be helped or harmed by the 9-valent HPV vaccine is 0.07.
HPV vaccine adverse events: post-marketing case series
Table 2 contains case reports and case series of chronic illnesses developing soon after HPV vaccination. Independent case series have described similar clinical features of headache, fatigue, musculoskeletal pain, and orthostatic intolerance symptoms. Nevertheless, this cluster of symptoms was labeled with different diagnoses such as chronic fatigue syndrome/myalgia encephalomyelitis [7, 10], postural orthostatic tachycardia syndrome [6, 7, 10, 12], fibromyalgia [11], or complex regional pain syndrome [3, 5]. Available follow-up information disclosed that the vast majority of affected individuals remain disabled. There are case reports of ovarian insufficiency after HPV vaccination [4, 9]. Some of these cases also had headache, sleep disturbances, and arthralgia [4].
Post-marketing safety reviews
The United Kingdom Medicines and Healthcare Products Regulatory Agency looked at the UK incidence rate of fatigue syndromes in girls before and after the start of the HPV vaccination campaign. There was no change in the incidence of fatigue syndromes in girls aged 12–20 years after the introduction of the HPV vaccination despite high uptake [37].
An investigation done in the Valencian Community of Spain contrasted the HPV vaccine adverse events rate vs. other types of vaccines given to girls of similar age. Data included all notification from doctors and nurses to the health authorities between 2007 and 2011. HPV vaccine-related adverse events had an approximate incidence rate of 1 per 1000 inoculations. This incidence was ten times higher than the ones described with other types of vaccines administered to girls of similar age. The authors suggested that this marked difference was due to HPV vaccine bad publicity. Thirty-two percent of the HVP vaccine adverse events were classified as “severe.” The most frequent post-HPV vaccination symptoms were dizziness, headache, and syncope [38].
Investigators from Alberta Canada identified all reported adverse events after HPV immunization between 2006 and 2014 and all emergency department utilization or hospitalizations within 42 days following HPV vaccination. Approximately 1 of 1000 vaccinees had an adverse event. Allergic reaction, other unusual events, other rash, and pain/swelling were the most frequently coded adverse events. Ten percent of all HPV vaccinated individuals visited a hospital emergency department within 42 days after immunization. The authors did not elaborate on this later finding [39].
A US Kaiser Permanent Health System study compared the risk of emergency department visits and hospitalizations during the interval soon after vaccination with risk during a comparison interval more remote from vaccination. The studied population comprised all females (n = 189,629) who received one or more doses of HPV vaccine between August 2006 and March 2008. Skin infections during days 1 to 14 post-vaccination and syncope on day of vaccination were noted by an independent Safety Review Committee as likely associations with HPV vaccine. The emergency department visit rate was not described [40].
A large Scandinavian hospital-based retrospective analysis found no increased incidence of specific autoimmune, neurological, or thromboembolic disease entities after immunization of adolescent girls with the quadrivalent HPV vaccine [41].
A meta-analysis of two quadrivalent vaccine studies and eight bivalent vaccine studies conducted in six Asian countries included 4681 individuals receiving HPV vaccine compared to 4524 injected with placebo. The risks of arthralgia (RR at 1.94; 95% CI 1.55–2.43) and myalgia (RR at 1.84; 95% CI 1.61–2.10) were higher in the vaccinated groups than those in the control groups. The risk of overall systemic adverse events in the vaccinated groups was higher than that in the controls (RR at 1.33; 95% CI 1.18–1.50). This meta-analysis did not evaluate serious adverse events [42].
The Slovenian Adverse Events Following Immunization Registry analyzed the school-based quadrivalent HPV vaccination program from 2009 to 2013. There were 149 quadrivalent HPV vaccine adverse events reported per 100,000 distributed doses. Serious adverse events reports were 8 per 100,000 distributed doses. The most frequent notified events were as follows: fatigue, headache, fever, sleep disorder, dizziness, and syncope [43].
Case series of HPV vaccine adverse events originated from Denmark and other countries, led by the Danish Health and Medicines Authorities in 2015 to ask the European Medicines Agency to give its opinion on whether there is a causal association between HPV vaccines and the two syndromes: complex regional pain syndrome and/or postural orthostatic tachycardia. The agency review found no evidence that the overall occurrence of these illnesses in vaccinated girls was different from that expected in these age groups, even taking into account a variety of possible scenarios for underreporting and reports that did not fully meet diagnostic criteria for these syndromes [1].
The World Health Organization has the largest international database of suspected adverse drug reactions (VigiBase). VigiBase used a novel data-driven cluster analysis approach to study HPV vaccine adverse events. All individual case safety reports for HPV vaccines until January 2015 were identified. Cluster analysis revealed reports of adverse events following HPV vaccination that were serious in nature but did not contain explicit diagnoses. The most commonly reported adverse events terms were headache, dizziness, fatigue, and syncope. This cluster of symptoms was more common and more severe in HPV vaccine reports compared with non-HPV vaccine reports for females of similar age [44].
Discussion
This critical review of HPV vaccine randomized controlled trials and post-marketing adverse events case series raises several safety concerns.
-
1.
The lack of inert placebo in the vast majority of pre-licensure HPV vaccine randomized studies
The overwhelming majority of randomized HPV vaccine trials did not use inert placebo. They used aluminum-containing placebo or other aluminum-adjuvanted vaccines. For clinical studies, a placebo is defined as a “pharmaceutically inert substance.” This definition cannot be applied to an adjuvant substance. Aluminum adjuvant mechanism of action remains poorly understood and its safety has been questioned. Aluminum adjuvants are known to stimulate TH2 immune response, activate dendritic cells, and activate NLRP3 inflammasome [45, 46].
Aluminum adjuvants have been implicated in the development of chronic illnesses such as the autoimmune/inflammatory syndrome induced by adjuvants (ASIA) syndrome and macrophagic myofasciitis. In 2011, Shoenfeld and Agmon-Levin suggested the name ASIA to a syndrome that may appear after the exposure to an adjuvant substance. Myalgia, muscle weakness, arthralgia, chronic fatigue, and neurological manifestations are the main clinical features of the ASIA syndrome [47].
Macrophagic myofasciitis is a multisystem illness that occurs rarely after vaccination, particularly after hepatitis B immunization. The clinical features of chronic macrophagic myofasciitis are myalgia, chronic fatigue, and cognitive impairment among others [48]. The ASIA syndrome and macrophagic myofascitis symptoms cluster are similar to those reported after HPV vaccination.
-
2.
Large randomized trials disclosed significantly more severe adverse events in the tested HPV vaccine cohort
In randomized double-blind trials, confounding variables are canceled out minimizing the influence of external factors on the results. In large randomized drug trials, the comparison groups are expected to have similar incidence of drug-independent adverse events.
The two relatively small randomized trials testing HPV vaccine against true inert saline placebo revealed a tendency to have more adverse events in the vaccine group. Unfortunately, Reisinger et al. safety analysis lumped boys and girls in a single group even though girls reported more adverse events than boys [20].
Two of the largest HPV vaccine randomized trials showed significantly more severe adverse events in the investigated vaccine arm of the study: Compared to aluminum placebo, bivalent HPV immunization was accompanied by significantly more vaccine-related general solicited symptoms during the 7-day post-vaccination period and a statistically significant four-fold increase in death rate [29]. Compared to the 4-valent formula, the “high dose” 9-valent HPV vaccine was associated to significantly more severe local swelling, more vaccine-related systemic adverse events, and more serious systemic adverse events [30]. These disparities suggest that HPV immunization adverse events may be dose-dependent. In contrast to the 9-valent vs. 4-valent group significant difference in serious adverse events, vaccine-related serious adverse events were reported as being 0% in both groups [30]. This incongruity advocates that at least in the 9-valent group, vaccine-related serious adverse events were under-recognized. Furthermore, this large trial disclosed a disturbing 9-valent HPV vaccine number needed to vaccinate/number needed to harm ratio.
The unquestionable statistical results derived from two of the largest HPV vaccine randomized trials must take preeminence over the investigators’ judgment ascribing the disproportionate severe adverse events and excessive death rate to external factors. One possible explanation for the apparent severe side-effects under-recognition might be that HPV vaccine adverse reaction may not look as the usual drug-related untoward response. Another possible explanation would be the investigator leniency towards a promising vaccine trial, which would decrease vaccine-related adverse events in both arms of the study.
-
3.
Pooled safety analysis found more post-immunization symptoms in bivalent HPV vaccine vs. hepatitis A vaccine
Pooled analysis of all trials comparing 29,953 healthy girls and women injected with bivalent HPV vaccine vs. hepatitis A vaccine showed significantly more post-immunization symptoms in the HPV vaccine group. This difference was present in all studied age groups [34].
-
4.
Post-marketing HPV vaccine adverse events case series describe similar cluster of symptoms than those reported in pre-clinical trials
Both pre-licensure randomized trials and post-marketing-independent reports describe similar cluster of adverse events symptoms, namely, headache, fatigue, dizziness, musculoskeletal pain, and gastrointestinal symptoms among others (Tables 1 and 2). In the post-marketing studies, this cluster of symptoms was labeled with different diagnoses such as complex regional pain syndrome, chronic fatigue syndrome, fibromyalgia, or postural orthostatic tachycardia syndrome. When looking at these diagnoses separately, HPV vaccine safety signals may be diluted. This possible post-marketing HPV vaccine adverse reaction under-recognition is reinforced by the recent WHO VigiBase report [44]. Symptoms clusters of headache and dizziness with either fatigue or syncope were found to be more commonly described, and more severe, in HPV vaccine reports compared with non-HPV vaccine reports for females of similar age. Only a minority of reports included in these clusters contained specific diagnoses to explain these symptoms.
-
5.
The European Medicines Agency report on HPV vaccine safety looked at specific diagnoses and not at symptoms clusters
The European Medicine Agency investigation found no evidence that the overall rates of complex regional pain syndrome and/or postural orthostatic tachycardia in vaccinated girls were different from expected rates in these age groups [1]. Nevertheless, as recognized in the European Medicine Agency report, there is great variability in the background yearly incidence for these syndromes [49]. Complex regional pain syndrome and postural orthostatic tachycardia syndrome are difficult to diagnose clinical entities. Many physicians prefer to ignore them or to reject them [50].
-
6.
In-depth analysis of some supportive post-marketing HPV vaccine safety studies discloses disquieting findings
HPV vaccine post-marketing safety studies done in Valencia, Spain, and Alberta, Canada, endorsed HPV vaccine safety. Nevertheless, these investigations contain disquieting findings. It seems perilous to blame “bad press” for the 10 times higher than expected HPV vaccine adverse events notification by Valencian doctors and nurses [38]. Similarly intriguing is the description of 10% of HPV-vaccinated healthy Canadian girls needing to visit a hospital emergency department within 42 days following HPV immunization [39].
HPV vaccine adverse events: possible pathogenetic mechanisms
As already stated, at this stage of knowledge, it seems premature and risky to propose any pathogenetic mechanism linking HPV vaccination to the purported adverse events. Based on our previous fibromyalgia research, we speculate that in susceptible individuals, the HPV virus-like particles and/or aluminum adjuvant may be neurotoxic, damaging the dorsal root ganglia and triggering dysautonomia and small fiber neuropathy [51]. The recent case reports describing antibodies to different autonomic nervous system receptors in patients that became ill after HPV immunization go along with this hypothesis [6, 12].
Conclusion
Scrutiny of two of the largest randomized trials unveiled significantly more serious adverse events in the investigated HPV vaccine arm of the study. Compared to the 4-valent dose, 9-valent HPV vaccine had significantly more serious adverse events. Considering this statistical difference, the reported 0% incidence of vaccine-related serious adverse events is probably an under-estimation. Nine-valent HPV vaccine has a worrisome number needed to vaccinate/number needed to harm quotient. Nine-valent vs. 4-valent HPV vaccine local and systemic adverse events disparities raise the possibility of a dose-dependent untoward effect. Compared to aluminum placebo, the group of individuals receiving the bivalent HPV vaccine had more deaths on follow-up. Pre-clinical randomized trials and independent post-marketing case series describe similar post-HPV immunization symptom clusters.
These findings raise further doubt on HPV vaccine safety.
Change history
29 July 2017
An erratum to this article has been published.
References
HPV vaccines: EMA confirms evidence does not support that they cause CRPS or POTS. http://www.ema.europa.eu/docs/en_GB/document_library/Referrals_document/HPV_vaccines_20/European_Commission_final_decision/WC500196773.pdf. Accessed 5 Mar 2017
(2017) Human papillomavirus vaccines: WHO position paper, May 2017. Wkly Epidemiol Rec 92:241–68
Richards S, Chalkiadis G, Lakshman R, Buttery JP, Crawford NW (2012) Complex regional pain syndrome following immunisation. Arch Dis Child 97:913–915
Colafrancesco S, Perricone C, Tomljenovic L, Shoenfeld Y (2013) Human papilloma virus vaccine and primary ovarian failure: another facet of the autoimmune/inflammatory syndrome induced by adjuvants. Am J Reprod Immunol 70:309–316
Kinoshita T, Abe RT, Hineno A, Tsunekawa K, Nakane S, Ikeda S (2014) Peripheral sympathetic nerve dysfunction in adolescent Japanese girls following immunization with the human papillomavirus vaccine. Intern Med 53:2185–2200
Blitshteyn S (2014) Postural tachycardia syndrome following human papillomavirus vaccination. Eur J Neurol 21:135–139
Tomljenovic L, Colafrancesco S, Perricone C, Shoenfeld Y (2014) Postural orthostatic tachycardia with chronic fatigue after HPV vaccination as part of the “autoimmune/auto-inflammatory syndrome induced by adjuvants”: case report and literature review. J Investig Med High Impact Case Rep 2:2324709614527812
Poddighe D, Castelli L, Marseglia GL, Bruni PA (2014) Sudden onset of a pseudo-neurological syndrome after HPV-16/18 AS04-adjuvated vaccine: might it be an autoimmune/inflammatory syndrome induced by adjuvants (ASIA) presenting as a somatoform disorder? Immune Res 60:236–246. doi:10.1007/s12026-014-8575-3
Little DT, Ward HR (2014) Adolescent premature ovarian insufficiency following human papillomavirus vaccination: a case series seen in general practice. J Investig Med High Impact Case Rep 4:1–12
Brinth L, Theibel AC, Pors K, Mehlsen J (2015) Suspected side effects to the quadrivalent human papilloma vaccine. Dan Med J 62:A5064
Martínez-Lavín M, Martínez-Martínez LA, Reyes-Loyola P (2015) HPV vaccination syndrome. A questionnaire-based study. Clin Rheumatol 34:1981–1983
Hendrickson JE, Tormey CA (2016) Human papilloma virus vaccination and dysautonomia: considerations for autoantibody evaluation and HLA typing. Vaccine 34:4468
Palmieri B, Poddighe D, Vadalà M, Laurino C, Carnovale C, Clementi E (2017) Severe somatoform and dysautonomic syndromes after HPV vaccination: case series and review of literature. Immunol Res 65:106–116
Kafaie J, Kim M, Krause E (2016) Small fiber neuropathy following vaccination. J Clin Neuromuscul Dis 18:37–40
Statens Serum Institut. Available at: http://www.ssi.dk/Smitteberedskab/Sygdomsovervaagning/VaccinationSurveillance.aspx?vaccination=5&xaxis=Cohort&sex=0&landsdel=100&show=Graph&datatype=Vaccination&extendedfilters=True#HeaderText. Accessed 3 May 2017
Food and Drug Administration. Approved products. Human papillomavirus vaccine. Available at: https://www.fda.gov/biologicsbloodvaccines/vaccines/approvedproducts/ucm172678.htm. Accessed 2 May 2017
Food and Drug Administration. Safety Medwatch. Available at: http://www.fda.gov/safety/medwatch/howtoreport/ucm053087.htm. Accessed 16 Apr 2017
Harper DM, Franco EL, Wheeler C, Ferris DG, Jenkins D, Schuind A, Zahaf T, Innis B, Naud P, De Carvalho NS, Roteli-Martins CM, Teixeira J, Blatter MM, Korn AP, Quint W, Dubin G (2004) Efficacy of a bivalent L1 virus-like particle vaccine in prevention of infection with human papillomavirus types 16 and 18 in young women: a randomised controlled trial. Lancet 364:1757–1765
Villa LL, Costa RL, Petta CA, Andrade RP, Ault KA, Giuliano AR, Wheeler CM, Koutsky LA, Malm C, Lehtinen M, Skjeldestad FE, Olsson SE, Steinwall M, Brown DR, Kurman RJ, Ronnett BM, Stoler MH, Ferenczy A, Harper DM, Tamms GM, Yu J, Lupinacci L, Railkar R, Taddeo FJ, Jansen KU, Esser MT, Sings HL, Saah AJ, Barr E (2005) Prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in young women: a randomised double-blind placebo-controlled multicentre phase II efficacy trial. Lancet Oncol 6:271–278
Reisinger KS, Block SL, Lazcano-Ponce E, Samakoses R, Esser MT, Erick J, Puchalski D, Giacoletti KE, Sings HL, Lukac S, Alvarez FB, Barr E (2007) Safety and persistent immunogenicity of a quadrivalent human papillomavirus types 6, 11, 16, 18 L1 virus-like particle vaccine in preadolescents and adolescents: a randomized controlled trial. Pediatr Infect Dis J 26:201–209
Garland SM, Hernandez-Avila M, Wheeler CM, Perez G, Harper DM, Leodolter S, Tang GW, Ferris DG, Steben M, Bryan J, Taddeo FJ, Railkar R, Esser MT, Sings HL, Nelson M, Boslego J, Sattler C, Barr E, Koutsky LA (2007) Quadrivalent vaccine against human papillomavirus to prevent anogenital diseases. N Engl J Med 356:1928–1943
Muñoz N, Manalastas R Jr, Pitisuttithum P, Tresukosol D, Monsonego J, Ault K, Clavel C, Luna J, Myers E, Hood S, Bautista O, Bryan J, Taddeo FJ, Esser MT, Vuocolo S, Haupt RM, Barr E, Saah A (2009) Safety, immunogenicity, and efficacy of quadrivalent human papillomavirus (types 6, 11, 16, 18) recombinant vaccine in women aged 24-45 years: a randomised, double-blind trial. Lancet 373:1949–1957
Paavonen J, Naud P, Salmerón J, Wheeler CM, Chow SN, Apter D, Kitchener H, Castellsague X, Teixeira JC, Skinner SR, Hedrick J, Jaisamrarn U, Limson G, Garland S, Szarewski A, Romanowski B, Aoki FY, Schwarz TF, Poppe WA, Bosch FX, Jenkins D, Hardt K, Zahaf T, Descamps D, Struyf F, Lehtinen M, Dubin G, HPV PATRICIA Study Group (2009) Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lancet 374:301–314
Medina DM, Valencia A, de Velasquez A, Huang LM, Prymula R, García-Sicilia J, Rombo L, David MP, Descamps D, Hardt K, Dubin G (2010) Safety and immunogenicity of the HPV-16/18 AS04-adjuvanted vaccine: a randomized, controlled trial in adolescent girls. J Adolesc Health 46:414–421
Bhatla N, Suri V, Basu P, Shastri S, Datta SK, Bi D, Descamps DJ, Bock H (2010) Immunogenicity and safety of human papillomavirus-16/18 AS04-adjuvanted cervical cancer vaccine in healthy Indian women. J Obstet Gynaecol Res 36:123–132
Ngan HY, Cheung AN, Tam KF, Chan KK, Tang HW, Bi D, Descamps D, Bock HL (2010) Human papillomavirus-16/18 AS04-adjuvanted cervical cancer vaccine: immunogenicity and safety in healthy Chinese women from Hong Kong. Hong Kong Med J 16:171–179
Giuliano AR, Palefsky JM, Goldstone S, Moreira ED Jr, Penny ME, Aranda C, Vardas E, Moi H, Jessen H, Hillman R, Chang YH, Ferris D, Rouleau D, Bryan J, Marshall JB, Vuocolo S, Barr E, Radley D, Haupt RM, Guris D (2011) Efficacy of quadrivalent HPV vaccine against HPV infection and disease in males. N Engl J Med 364:401–411
Yoshikawa H, Ebihara K, Tanaka Y, Noda K (2013) Efficacy of quadrivalent human papillomavirus (types 6, 11, 16 and 18) vaccine (GARDASIL) in Japanese women aged 18-26 years. Cancer Sci 104:465–472
Skinner SR, Szarewski A, Romanowski B, Garland SM, Lazcano-Ponce E, Salmerón J, Del Rosario-Raymundo MR, Verheijen RH, Quek SC, da Silva DP, Kitchener H, Fong KL, Bouchard C, Money DM, Ilancheran A, Cruickshank ME, Levin MJ, Chatterjee A, Stapleton JT, Martens M, Quint W, David MP, Meric D, Hardt K, Descamps D, Geeraerts B, Struyf F, Dubin G (2014) Efficacy, safety, and immunogenicity of the human papillomavirus 16/18 AS04-adjuvanted vaccine in women older than 25 years: 4-year interim follow-up of the phase 3, double-blind, randomised controlled VIVIANE study. Lancet 84:2213–2227
Joura EA, Giuliano AR, Iversen OE, Bouchard C, Mao C, Mehlsen J, Moreira ED Jr, Ngan Y, Petersen LK, Lazcano-Ponce E, Pitisuttithum P, Restrepo JA, Stuart G, Woelber L, Yang YC, Cuzick J, Garland SM, Huh W, Kjaer SK, Bautista OM, Chan IS, Chen J, Gesser R, Moeller E, Ritter M, Vuocolo S, Luxembourg A (2015) A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N Engl J Med 372:711–723
Vesikari T, Brodszki N, van Damme P, Diez-Domingo J, Icardi G, Petersen LK, Tran C, Thomas S, Luxembourg A, Baudin MA (2015) Randomized, double-blind, phase III study of the immunogenicity and safety of a 9-valent human papillomavirus L1 virus-like particle vaccine (V503) versus Gardasil® in 9-15-year-old girls. Pediatr Infect Dis J 34:992–998
Garland SM, Cheung TH, McNeill S, Petersen LK, Romaguera J, Vazquez-Narvaez J, Bautista O, Shields C, Vuocolo S, Luxembourg A (2015) Safety and immunogenicity of a 9-valent HPV vaccine in females 12-26 years of age who previously received the quadrivalent HPV vaccine. Vaccine 33:6855–6864
Van Damme P, Meijer CJ, Kieninger D, Schuyleman A, Thomas S, Luxembourg A, Baudin M (2016) A phase III clinical study to compare the immunogenicity and safety of the 9-valent and quadrivalent HPV vaccines in men. Vaccine 34:4205–4212
Descamps D, Hardt K, Spiessens B, Izurieta P, Verstraeten T, Breuer T, Dubin G (2009) Safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine for cervical cancer prevention: a pooled analysis of 11 clinical trials. Hum Vaccin 5:332–340
Wheeler CM, Skinner SR, Del Rosario-Raymundo MR, Garland SM, Chatterjee A, Lazcano-Ponce E, Salmerón J, McNeil S, Stapleton JT, Bouchard C, Martens MG, Money DM, Quek SC, Romanowski B, Vallejos CS, TerHarmsel B, Prilepskaya V, Fong KL, Kitchener H, Minkina G, Lim YK, Stoney T, Chakhtoura N, Cruickshank ME, Savicheva A, da Silva DP, Ferguson M, Molijn AC, Quint WG, Hardt K, Descamps D, Suryakiran PV, Karkada N, Geeraerts B, Dubin G, Struyf F (2016) Efficacy, safety, and immunogenicity of the human papillomavirus 16/18 AS04-adjuvanted vaccine in women older than 25 years: 7-year follow-up of the phase 3, double-blind, randomised controlled VIVIANE study. Lancet Infect Dis 16:1154–1168
Martínez-Lavín M (2017) Vaccine-related serious adverse events might have been under-recognized in the pivotal HPV vaccine randomized trial. Clin Rheumatol 36:975
Donegan K, Beau-Lejdstrom R, King B, Seabroke S, Thomson A, Bryan P (2013) Bivalent human papillomavirus vaccine and the risk of fatigue syndromes in girls in the UK. Vaccine 31:4961–4967
Rodríguez-Galán MA, Pérez-Vilar S, Díez-Domingo J, Tuells J, Gomar-Fayos J, Morales-Olivas F, Pastor-Villalba E (2014) Adverse reactions to human papillomavirus vaccine in the Valencian Community (2007-2011). An Pediatr (Barc) 81:303–309
Liu XC, Bell CA, Simmonds KA, Svenson LW, Russell ML (2016) Adverse events following HPV vaccination, Alberta 2006-2014. Vaccine 34:1800–1805
Klein NP, Hansen J, Chao C, Velicer C, Emery M, Slezak J, Lewis N, Deosaransingh K, Sy L, Ackerson B, Cheetham TC, Liaw KL, Takhar H, Jacobsen SJ (2012) Safety of quadrivalent human papillomavirus vaccine administered routinely to females. Arch Pediatr Adolesc Med 166:1140–1148
Arnheim-Dahlström L, Pasternak B, Svanström H, Sparén P, Hviid A (2013) Autoimmune, neurological, and venous thromboembolic adverse events after immunisation of adolescent girls with quadrivalent human papillomavirus vaccine in Denmark and Sweden: cohort study. BMJ 347:f5906
Setiawan D, Luttjeboer J, Pouwels KB, Wilschut JC, Postma MJ (2017) Immunogenicity and safety of human papillomavirus (HPV) vaccination in Asian populations from six countries: a meta-analysis. Jpn J Clin Oncol 47:265–276
Šubelj M, Učakar V, Kraigher A, Klavs I (2016) Adverse events following school-based vaccination of girls with quadrivalent human papillomavirus vaccine in Slovenia, 2009 to 2013. Euro Surveill. doi:10.2807/1560-7917.ES.2016.21.14.30187
Chandler RE, Juhlin K, Fransson J, Caster O, Edwards IR, Norén GN (2017) Current safety concerns with human papillomavirus vaccine: a cluster analysis of reports in VigiBase. Drug Saf 40:81–90
Exley C, Siesjö P, Eriksson H (2010) The immunobiology of aluminium adjuvants: how do they really work? Trends Immunol 31:103–109
Awate S, Babiuk LA, Mutwiri G (2013) Mechanisms of action of adjuvants. Front Immunol 4:114
Shoenfeld Y, Agmon-Levin N (2011) ‘ASIA’—autoimmune/inflammatory syndrome induced by adjuvants. J Autoimmun 36:4–8
Rigolet M, Aouizerate J, Couette M, Ragunathan-Thangarajah N, Aoun-Sebaiti M, Gherardi RK, Cadusseau J, Authier FJ (2014) Clinical features in patients with long-lasting macrophagic myofasciitis. Front Neurol 5:230
de Mos M et al (2007) The incidence of complex regional pain syndrome: a population-based study. Pain 129:12–20
Del Piñal F (2014) Editorial. I have a dream ... reflex sympathetic dystrophy (RSD or Complex Regional Pain Syndrome - CRPS I) does not exist. J Hand Surg Eur 38:595–597
Martínez-Lavin M (2015) Human papillomavirus vaccination syndrome—small fiber neuropathy and dysautonomia could be its underlying pathogenesis. Clin Rheumatol 34:1165–1169
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
The original version of this article was revised: The above article originally published with an error present in the 9-valent dose listed within the abstract. Originally reading “…For the 9-valent dose, our calculated number needed to seriously harm is 140 (95% CI, 796–53)…”, this should instead have read “…For the 9-valent dose, our calculated number needed to seriously harm is 140 (95% CI, 79–653)…” [bold text used to highlight problem area].
An erratum to this article is available at https://doi.org/10.1007/s10067-017-3782-7.
Rights and permissions
About this article

Cite this article
Martínez-Lavín, M., Amezcua-Guerra, L. Serious adverse events after HPV vaccination: a critical review of randomized trials and post-marketing case series. Clin Rheumatol 36, 2169–2178 (2017). https://doi.org/10.1007/s10067-017-3768-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-017-3768-5