
Abstract
The Routine Assessment of Patient Index Data 3 (RAPID3) is a patient-reported disease activity measure used to assess physical function, pain, and global health in patients with rheumatoid arthritis (RA) without formal joint counts. Since hand involvement and its decreased function are hallmarks of RA, the aim of our study was to investigate the performance of RAPID3 scores with regard to hand function and to confirm previous findings that the RAPID3 score as a disease activity measure is strongly correlated with the DAS28 score. Sixty-eight consecutive patients with RA (85% female), aged 18–75 years, were included in the study and were recruited during their outpatient visit. Apart from demographic and clinical data, the obtained parameters of interest included RAPID3 scores and assessments of the function of the hand, namely, the signal of functional impairment (SOFI)-hand, grip strength, and pulp-to-palm distance, as well the Health Assessment Questionnaire- Disability Index (HAQ-DI) and DAS28 scores. Pearson’s correlation coefficient, Student’s t test and linear regression were used in the statistical analysis of the results. The significance was set to p < 0.05. A positive correlation was found between RAPID3 scores and HAQ-DI scores, SOFI-hand scores, and pulp-to-palm distance, and negative correlation was observed between RAPID3 scores and grip strength. The order regarding the strength of correlations between RAPID3 scores and other variables (from the strongest to the weakest) was as follows: HAQ-DI, grip strength, SOFI-hand and pulp-to-palm distance. The hand assessment variables had stronger correlations with RAPID3 scores than with DAS28 scores. Our preliminary study showed that RAPID3 scores were strongly correlated with measurements of the functional ability of the hand, demonstrating that RAPID3 can be used as a measure of disease activity in clinical practice and to characterize hand function. Further studies are needed to confirm this result.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is a lifelong, inflammatory rheumatic disease, characterized by chronic synovial inflammation and joint damage [1]. Pain, swelling, stiffness, and other signs and symptoms of RA occurring alongside structural damage and joint deformities result in reduced grip force and decreased range of motion and eventual functional impairment [2, 3]. Disease activity is the essential parameter that needs to be measured in patients with RA because it is a major driver of structural damage and disability [4]. The Routine Assessment of Patient Index Data 3 (RAPID3) is a patient-reported disease activity measure that assesses physical functioning, pain, and global health but without formal joint counts. It is a relatively novel simple index that has been developed to assess and monitor patients with RA in routine practice. It was shown to have reasonable similarity to other more frequently used measurements of disease activity such as the Disease Activity Score-28 (DAS28) and the Clinical Disease Activity Index (CDAI) [5, 6]. Hand function has the most impact on overall disability in patients with RA [7]. We sought to analyze correlations between RAPID3 scores and hand function tests since the physical function part of the assessment incorporates 7 out of 13 questions, tasks for which hand use is needed. Therefore, it is important to know how RAPID3 scores, which are used in clinical practice, correlate with hand function. The aim of this cross-sectional study was to investigate the association of RAPID3 scores with hand functional ability as measured with different hand-specific assessment tools, and to confirm previous findings that RAPID3, as a disease activity measure has a strong correlation with DAS28.
Method
Patients and data collection
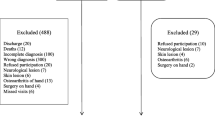
Between September 2013 and July 2014, 68 consecutive RA patients from the Outpatient Department of Rheumatology Clinic of the University Centre of Kosova were enrolled in the study. All of the patients were diagnosed according to the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) 2010 criteria [8]. The additional inclusion criteria were 18 to 75 years of age, a diagnosis that had been established for at least 6 months, and no changes to therapy (DMARDs, glucocorticoidsand NSAIDs) in the preceding 3 months. The exclusion criteria were previous hand surgical interventions, present or previous fractures of the hand, patients who attended physical therapy within the last month, diagnosis with a neurologic disease, severe renal or hepatic failure, severe heart failure (NYHA III or IV), malignant disease with the exception of non-melanoma skin cancer, severe psychiatric disorders, psoriasis or other skin defects of the hand that could compromise hand function, and a congenital physical malformation of the hand. The pharmacological therapy consisted of non-steroidal anti-inflammatory drugs (NSAIDs), disease-modifying anti-rheumatic drugs (DMARDs), and low-dose corticosteroids (on average ≤ 7.5 mg of prednisolone). None of the patients were treated with biological drugs. The study was approved by the Ethics Committee of the University Clinical Centre of Kosova and was conducted in accordance with the principles of the Helsinki Declaration. Prior to data collection, each patient was informed about the purpose of this research, an explanation of the protocol of the study was provided, and the patients provided informed consent. The data were obtained on the same day with a structured questionnaire that assessed demographic and clinical data. During the data collections, grip function was obtained by a different investigator blinded to DAS28.
Disease activity.
We measured disease activity by RAPID3 scores, a patient-reported outcome that consists of three sections: physical function, level of pain and patient global estimate of disease. The scores of each section are summed, and the sum (range 0–30) is recorded on the right side at the bottom of the page. More details of the RAPID3 scores, including the scoring, are explained elsewhere [5]. We also performed the DAS28 assessment, a widely-known composite measure of disease activity that includes the number of tender joints and the number of swollen joints, general health assessed by the patient, and ESR or CRP evaluated with a complex formula [9]. In this study, we used a version of DAS28 with ESR.
Hand function.
Grip strength was evaluated with the hydraulic hand dynamometer, (North Coast Medical, Inc., Morgan Hill, CA, USA) [10]. The subjects were positioned and evaluated according to the recommendations of the American Society of Hand Therapists as explained elsewhere [11]. The outcome values were recorded in kilograms.
A signal of functional impairment (SOFI) was used to assess hand function. It is a performance test consisting of hand, upper limb and leg function evaluations. In our study, we used the SOFI-hand section of the assessment. The overall score ranges 0 to16, where a low score indicates full function [12]. Total finger flexion was assessed by measuring pulp-to-palm distance according to the American Society for Surgery of the Hand [13]. The average distances for the right and left hands were recorded in centimeters.
Functional disability.
Overall functional disability was measured with a self-assessed Health Assessment Questionnaire-Disability Index (HAQ-DI) which is an established measurement of the functional ability of patients with RA. The questionnaire consisted of 20 questions within 8 domains and generated a score from 0 to 3 for each question. Based on the sum of the worst scores for each domain, the result was obtained by dividing them by the number of domains that were addressed [14].
Statistical analysis
In the correlation analysis between RAPID3 scores and other variables, the Pearson product-moment correlation coefficient was used, and the inference of significance was based on Student’s t-test for significance. Linear regression was used to evaluate the percentage of contribution of a number of selected variables on RAPID3 scores. The Spearman rank correlation used to test the relationships among RAPID3 scores, grip strength, SOFI-hand scores, pulp-to-palm distance and HAQ-DI scores, in each of the subgroups stratified by gender, age, and disease duration. Moreover, multivariate regression analysis was used to determine the relationship between a number of selected variables and RAPID3 scores. STATA version 11 software (StataCorp, College Station, TX) was used for statistical analyses. The significance level was set at p < 0.05.
Results
Patients’ demographic and clinical data are presented in Table 1. The mean RAPID3 score was 14.1 (SD 5.2), the mean DAS28 was 5.9 (SD 1.3), the mean HAQ-DI score was 1.8 (SD 0.7), the mean grip strength was 16.6 kg (SD 8.4), the mean SOFI-hand score was 4.7 (SD 3.9), and the mean value for pulp-to-palm distance was 1.7 cm (SD 0.9). The correlations between study variables were investigated as crude values and were adjusted by age, gender, and disease duration, with particular attention paid to the comparisons between RAPID3 scores and hand function data (Table 2 and Table 3). Most importantly, a positive correlation was found between RAPID3 scores and HAQ-DI scores (r = 0.81), RAPID3 scores and SOFI-hand scores (r = 0.57), and RAPID3 scores and pulp-to-palm distance (r = 0.44), and a negative correlation was found between RAPID3 scores and grip strength (r = −0.69), meaning that patients’ hand function worsen with higher disease activity measured by RAPID3 scores. In regards to gender, age, and disease duration, we did not find significant correlations between RAPID3 scores, SOFI-hand scores, and pulp-to-palm distance in males in the early disease group (duration 0–1 years) or in the long-term disease group (duration >20 years),implying that RAPID3 scores cannot mirror total finger flexion motion as measured by the pulp-to-palm distance. Moreover, we investigated whether each component of RAPID3 scores (FN- physical function, PN- pain, GE-global estimate) performs well to predict hand function. The strongest correlation was found between the Rapid3 FN score and the HAQ-DI score (r = 0.86), followed by correlations between the Rapid3 PN score and the HAQ-DI score (r = 0.71) and the Rapid3 PN score and grip strength (r = −0.70) (see Supplementary file 1 for details).
In the hand function data, the strongest correlation was found between the SOFI-hand score and the pulp-to-palm distance (r = 0.77), followed by correlations between the HAQ-DI score and grip strength (r = −0.76), the SOFI-hand score and grip strength (r = −0.70), and grip strength, and pulp-to-palm distance (r = −0.64) (Table 3).
In order to evaluate which variable contributed the most to RAPID3 scores, we performed linear regression analysis. Each of the above factors was regressed on RAPID 3 and the relevant R-squared coefficients and the percentage of contribution as well as the results of a t test on the significance of the relationship between the two variables indicated that the factor was significantly related to RAPID3 scores. The results demonstrated that the most influential factor on RAPID3 score was the HAQ-DI score (66.22%) followed by grip strength (45.88%), SOFI-hand score (32.52%), and pulp-to-palm distance (19.83%), all independently significant at the 1% level (Table 4).
Discussion
Since RA is a complex disease, the use of various objective and subjective instruments has been proposed in order to obtain optimal information about patient conditions. Because the disease typically affects the small joints of the hand, the aim of our study was to investigate the relationship between RAPID3 scores, a novel disease activity tool, and the function of the hand, which, to our knowledge, has not been studied before. This is important because, by using the RAPID3 scores, we could determine whether it correlates with hand function, which is the major contributor of disability in these patients. Disease activity in RA is most often measured with the DAS28 scale [9]. Our results confirmed previous findings regarding the similarity between RAPID3 scores and DAS28 scores, which have presented the benefit of RAPID3 use as disease activity measure in clinical practice [5, 6]. Interestingly, we found a stronger correlation between RAPID3 scores and hand outcome measurements than between DAS28 scores and hand outcome measurements, which implies that the damage is reflected in the RAPID3 score but not in the DAS28 score. These findings further reinforce the clinical usefulness of RAPID3. The relationship between DAS28 scores and different hand outcome measurements was confirmed by other studies [15–20]. The study by Dedeogluret al. reported a correlation between grip strength and other RA assessments and found negative correlations with DAS28, HAQ, and SOFI indices. Additionally, there was a correlation between DAS28 scores with SOFI and HAQ scores [15], results that are in accordance with our findings. Hallertet al. showed that grip strength and SOFI were significant predictors of disease activity [16]. In contrast, Bircanet al. reported a significant but weak correlation between hand function and disease activity; hand function was evaluated with the Grip Ability Test (GAT) [21], which may explain the discordance between their findings and our study results.
Sheehy et al. examined patients with early rheumatoid arthritis and found a strong correlation between DAS28 scores and grip strength in patients with a disease duration of less than 2 years, emphasizing the importance of assessing grip strength, which acts as a disease activity measure in RA patients [19]. These results are in agreement with our current findings. Namely, our patients with a disease duration of less than 1 year or a duration of 2–5 years showed a significant correlation between RAPID3 scores and grip strength as well as between RAPID3 scores and other hand measurements. In contrast, Eberhard et al. did not observe a correlation between DAS28 scores and hand outcome measurements, with the reasoning that the majority of the RA patients had disturbed hand function [7]. This may have been due to the long average disease duration of 15 years, while the average disease duration was 9.6 years in our study. In addition, when we analyzed the correlation between RAPID3 scores and hand outcome measurements in patients with longer disease duration (>11 years), we found a strong correlation between RAPID3 scores, HAQ-DI scores, and grip strength. In accordance with the results of Erbehard et al. we did not find a significant correlation between RAPID3 scores and SOFI-hand scores in patients with late disease (disease duration >20 years). Kapetanovic et al. presented the results of 20 year follow-up and concluded that disease activity contributed to HAQ-DI scores and impairment (assessed by SOFI) [22]. Our results show that hand function measurements contribute to RAPID3 scores at a level of 19.8 to 66.2%.
It is of note that the correlation between RAPID3 scores and HAQ-DI scores was expected since the RAPID3 is part of the MD-HAQ, which was derived from HAQ-DI [5, 6]. Our study supports the results of other studies that found a correlation between overall functional disability (HAQ) and grip strength [15, 17, 23–25], as well as studies that established a significant correlation between HAQ and SOFI [7, 22]. In line with the results of other studies [7, 15], our results also showed considerable correlations between hand outcome measurements. The strongest correlation was between SOFI-hand scores and pulp-to-palm distance, which is understandable since the SOFI-hand index actually measures the range of motion in the hands [7, 25]. In contrast to our study, Bjork et al. found a weak correlation between hand outcome measurements (grip strength, Grip Ability Test (GAT), and SOFI-hand), with the plausible explanation that they measured different aspects of hand function [25].
The main strength of our study is that it was performed using a predefined standardized method in a sample of patients with established disease. The patients were enrolled in a consecutive way, reflecting the settings of clinical practice. There were several limitations to our study. The cross-sectional design and the lack of a control group were the most obvious limitations. There was an imbalance between genders, with a larger number of females (approx. 6:1), which might have influenced the results of the hand function assessment; it has been shown that women have better hand performance than men [16, 25]. Another limitation was that the majority of the patients had moderate to high disease activity. In addition, we are aware of the inherent shortcomings due to the design of the study, especially regarding the external validity.
In conclusion, in this preliminary study we found a strong to moderate correlation between RAPID3 scores and various measurements of hand function in patients with established RA. Based on the results of our study, RAPID3 scores could be seen as a simple tool to assess disease activity in everyday clinical practice, which encompasses the function of the hand, regardless of the patient’s gender, age, or disease duration. This is valuable since damage of the hands in patients with RA leads to difficulties in performing activities of daily life, greatly impacting quality of life.
The use of RAPID3 may be seen as an advantage in the busy clinical setting where medical professionals do not regularly perform joint counts and even do not measure acute phase reactants, although this assessment cannot be a substitute for testing hand function. Longitudinal studies with larger samples of patients, embracing those with low disease activity as well, are needed to further evaluate our findings, with the inclusion of sensitivity to change as an important parameter in clinical practice.
References
Scott D, Wolfe F, Huizinga TWJ (2010) Rheumatoid arthritis. Lancet 376:1094–1108. doi:10.1016/S0140-6736(10)60826-4
Poole JL, Santhanam DD, Latham AL (2013) Hand impairment and activity limitations in four chronic diseases. J Hand Ther 26:232–237. doi:10.1016/j.jht.2013.03.002
Andrade JABM, Pinto MR, Lanna CC (2016) Factors associated with activity limitations in people with rheumatoid arthritis. Am J OccupTher 70:1–7. doi:10.5014/ajot.2016.017467
Choy E (2012) Understanding the dynamics: pathways involved in the pathogenesis of rheumatoid arthritis. Rheumatology (Oxford) 51:v3–11. doi:10.1093/rheumatology/kes113
Pincus T, Swearingen CJ, Bergman MJ, Colglazier CL, Kaell AT, Kunath AM, Siegel EL, Yazici Y (2010) RAPID3 (routine assessment of patient index data) on an MDHAQ (multidimensional health assessment questionnaire): agreement with DAS28 (disease activity score) and CDAI (clinical disease activity index) activity categories, scored in five versus more than ninety seconds. Arthritis Care Res (Hoboken) 62:181–189. doi:10.1002/acr.20066
Kim SK, Park SH, Bae J, Son JT, Choe JY (2014) Performance of routine assessment of patient index data 3 (RAPID3) for assessment of rheumatoid arthritis in clinical practice: differential agreement of RAPID3 according to disease activity categories. RheumatolInt 34:1311–1318. doi:10.1007/s00296-014-3042-y
Eberhardt K, Sandqvist G, Geborek P (2008) Hand function tests are important and sensitive tools for assessment of treatment response in patients with rheumatoid arthritis. Scand J Rheumatol 37:109–112. doi:10.1080/03009740701747129
Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, Birnbaum NS, Burmester GR, Bykerk VP, Cohen MD, Combe B, Costenbader KH, Dougados M, Emery P, Ferraccioli G, Hazes JM, Hobbs K, Huizinga TW, Kavanaugh A, Kay J, Kvien TK, Laing T, Mease P, Ménard HA, Moreland LW, Naden RL, Pincus T, Smolen JS, Stanislawska-Biernat E, Symmons D, Tak PP, Upchurch KS, Vencovský J, Wolfe F, Hawker G (2010). 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 62:2569–81. doi:10.1002/art.27584
Prevoo ML, van't Hof MA, Kuper HH, van Leuwwen MA, van der Putte LB, van Riel PL (1995) Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum 38:44–48. doi:10.1002/art.1780380107
North Coast Medical & Rehabilitation Products (2013) https://www.ncmedical.com/item_699.html Accessed 15 September 2013
Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Rogers S (1985) Grip and pinch strength: normative data for adults. Arch Phys Med Rehabil 66:69–74
Eberhardt KB, Svensson B, Moritz U (1988) Functional assessment of early rheumatoid arthritis. Br J Rheumatol 27:364–371. doi:10.1093/rheumatology/27.5.364
Macey AC, Burke FD (1995) Outcome of hand surgery. J Hand Surg Eur 20:841–855. doi:10.1016/S0266-7681(95)80059-X
Fries J, Kraines R, Holman H (1980) Measurement of patient outcome in arthritis. Arthritis Rheum 23:137–145. doi:10.1002/art.1780230202
Dedeoglu M, Gafuroglu U, Yilmaz O, Bodur H (2013) The relationship between hand grip and pinch strengths and disease activity, articular damage, pain, and disability in patients with rheumatoid arthritis. Turk J Rheumatol 28:69–78. doi:10.5606/tjr.2013.2742
Hallert E, Bjork M, Dahlstrom O, Skogh T, Thyberg I (2012) Disease activity and disability in women and men with early rheumatoid arthritis (RA): an 8-year followup of a Swedish early RA project. Arthritis Care & Research 64:1101–1107
Hakkinen A, Kautiainen H, Hannonen P, Ylinen J, Makinen H, Sokka T (2006) Muscle strength, pain, and disease activity explain individual subdimensions of the health assessment questionnaire disability index, especially in women with rheumatoid arthritis. Ann Rheum Dis 65:30–34. doi:10.1136/ard.2004.034769
Adams J, Burridge J, Mullee M, Hammond A, Cooper C (2004) Correlation between upper limb functional ability and structural hand impairment in an early rheumatoid population. Clin Rehabil 18:405–413. doi:10.1191/0269215504cr732oa
Sheehy C, Gaffney K, Mukhtyar C (2013) Standardized grip strength as an outcome measure in early rheumatoid arthritis. Scand J Rheumatol 42:289–293. doi:10.3109/03009742.2012.747624
Piquer PN, Palomares CN, Cortes JI, Grau E, Verdejo IC, Almela CM (2014) Relationship between HAQ, DAS28 and radiological damage with functional capacity of the hand in rheumatoid arthritis. Ann Rheum Dis 73:879–880. doi:10.1136/annrheumdis-2014-eular.4977
Bircan C, Gunduz NE, Tekgul A, Cetin P, Onen F, Kizil R, Gulbahar S (2014) Grip ability test in rheumatoid arthritis patients: relationship with disease activity and hand-specific self-report questionnaires. Turk J Rheumatol 29:160–167. doi:10.5606/tjr.2014.4590
Kapetanovic MC, Lindqvist E, Nilsson J-Å, Geborek P, Saxne T, Eberhardt K (2015) Development of functional impairment and disability in rheumatoid arthritis patients followed for 20 years: relation to disease activity, joint damage, and comorbidity. Arthritis Care Res (Hoboken) 67:340–348. doi:10.1002/acr.22458
Lopez Lopez CO, Alvarez-Hernandez E, Medrano Ramirez G, Montes Castillo ML, Hernandez-Diaz C, Ventura Rios L, Arreguin Lopez R, Vazquez-Mellado J (2014) Hand function in rheumatic diseases: patient and physician evaluations. Int J Rheum Dis 17:856–862. doi:10.1111/1756-185X.12466
Bjork MA, Thyberg IS, Skogh T, Gerdle BU (2007) Hand function and activity limitation according to health assessment questionnaire in patients with rheumatoid arthritis and healthy referents: 5-year followup of predictors of activity limitation (the Swedish TIRA project). J Rheumatol 34:296–302
Bjork M, Thyberg I, Haglund L, Skogh T (2006) Hand function in women and men with early rheumatoid arthritis. A prospective study over three years (the Swedish TIRA project). Scand J Rheumatol 35:15–19. doi:10.1080/03009740510026562
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None.
Funding
None
Electronic supplementary material
ESM 1
(DOCX 12 kb)
Rights and permissions
About this article

Cite this article
Qorolli, M., Hundozi-Hysenaj, H., Rexhepi, S. et al. RAPID3 scores and hand outcome measurements in RA patients: a preliminary study. Clin Rheumatol 36, 1379–1385 (2017). https://doi.org/10.1007/s10067-016-3514-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-016-3514-4