
Abstract
To explore whether femoral cartilage thickness is related (and changes) with muscle strength in subjects with knee osteoarthritis (OA). Forty patients (27 F, 13 M) with knee OA—who were under quadriceps muscle strengthening program—were enrolled in the study. Isokinetic/isometric knee muscle strength measurements (at 30–60° angles and 60–180° velocity) were performed at baseline, end of the muscle strengthening program, and third month control visit using a biodex dynamometer. Femoral cartilage thicknesses (at medial/lateral condyle and intercondylar area) were measured using ultrasonography. Seventy-nine knees of 40 patients (27 F, 13 M) aged 52.03 ± 11.72 years (range, 26–71) were analyzed. Mean VAS scores on the first and third months were significantly lower than the initial values (p < 0.001, p = 0.049). Isometric peak torque and total work values at 180 °/s were significantly higher than the baseline measurements at first and third month controls (all p < 0.05). Cartilage thicknesses (at three sites) were significantly higher than the baseline measurements (all p < 0.05) on the third month but not on the first month (all p > 0.05). Femoral cartilage thicknesses were positively correlated with isometric strength values at baseline and third month. We propose that femoral cartilage thicknesses increase on the third month of strengthening therapy. Since this late-phase thickening parallels the earlier increase in muscle strength (starting, on the first month), we speculate that regeneration rather than edema might be the primary underlying cause.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis (OA) is a chronic inflammatory disease which is characterized by loss of articular cartilage and one of the most common diseases of the elderly population [1, 2]. Knee OA is the most common type and it is associated with decreased knee muscle strength [3, 4].
In the literature, it has been reported that femoral cartilage thickness changed in various diseases that might cause muscle weakness e.g. hemiparetic stroke, spinal cord injury, systemic sclerosis, and systemic lupus erythematosus [5–8]. Herewith, to the best knowledge of the authors, the relationship between the femoral cartilage thickness and the knee muscle strength has not been reported until now. Accordingly, in this study, we aimed to explore whether femoral cartilage thickness is related (and changes) with muscle strength in subjects with knee OA. Similar to the previous studies, we used ultrasound (US) imaging which has been shown to be a reliable method for assesing distal femoral cartilage [9, 10].
Patients and methods
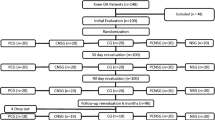
Subjects with knee OA—who were under quadriceps muscle strengthening program—were consecutively recruited. They fulfilled the American College of Rheumatology criteria for knee OA [11]. Subjects who had inflammatory rheumatic disease, meniscal lesions, cruciate ligament lesion, recent knee trauma, and any disease causing muscle weakness were excluded. Overall, 40 patients (27 F, 13 M) were enrolled in the study. Subjects were informed about the study procedure and they consented to participate. The local ethics committee approved the study protocol.
Demographic characteristics (age, profession, height, weight) of the subjects were noted. Pain and functional status were evaluated using VAS and WOMAC (Turkish version), respectively [12–14].
Bilateral quadriceps and hamstring muscle strengths were measured with an isokinetic dynamometer (Cybex NORM 6000). Patients were seated upright and fixed with pelvic and distal thigh belts. They were allowed to hold on both sides of the chair with their hands. Isokinetic muscle strength was measured concentrically at two angular velocities; 5 repetitions at 60 °/s and 10 repetitions at 180 °/s. Isometric muscle strength was measured at 30 and 60° of knee flexion. Subjects performed trial repetitions before each set and a 20 s resting interval was provided between the sets. Vocal encouragement was kept constant during the testing procedure.
Patients were then enrolled in an isokinetic strengthening program, i.e., 10 repetitions at 30 °/s, 10 repetitions at 60 °/s, 10 repetitions at 90 °/s, 10 repetitions at 180 °/s, one times a day. Then, patients were given a home based exercise regimen which comprised quadriceps isometric and hamstring stretching exercises.
Femoral cartilage thicknesses were measured while subjects lied supine on the examination bed with maximum knee flexion. Ultrasound imaging was done using suprapatellar axial view and measurements were taken from the midpoints of the medial femoral cartilage, intercondylar area, and lateral femoral cartilage. The same sonographer (ST) performed all the measurements which were substantially evaluated by the expert sonographer (LÖ) (Fig. 1). Cartilage and strength measurements were performed at baseline, at the end of the muscle strengthening program (first month) and third month control visits. US and cybex measurements were done by different persons, i.e., one sonographer and one technician. The sonographer was blinded to the cybex measurements.

Ultrasound image (suprapatellar axial view) shows the femoral cartilage thickness measurements. 1 medial femoral condyle, 2 intercondylar area, 3 lateral femoral condyle
Statistical analyses were done using SPSS 20.0. Friedman test were used for comparisons between the repeated three measures. Bonferroni-Dunn procedure was used for comparing the pairs of repeated measurements. Pearson or Spearman coefficients were used for correlation analysis. P values less than 0.05 were considered statistically significant.
Results
Seventy-nine knees of 40 patients (27 F, 13 M) aged 52.03 ± 11.72 years (ranged 26–71) with knee OA were analyzed. The average body mass index (BMI) of patients was 28.22 ± 5.37 (range 18.42–39.61).
The mean VAS scores on the first and third months were significantly lower than the initial values (p < 0.001, p = 0.049, respectively). WOMAC scores were similar between the evaluations (Table 1).
Flexion and extension peak torque values at 30 and 60°, and total work values at 180 °/s were significantly higher than the baseline measurements at first and third month controls (all p < 0.05).
Cartilage thicknesses (at three sites) were significantly higher than the baseline measurements (all p < 0.05) on the third month but not on the first month. Measurements pertaining to the first and third months were similar (all p > 0.05) (Table 2).
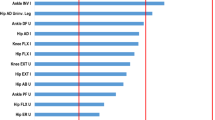
Correlation analyses are given in Table 3. In the baseline evaluations, femoral cartilage thicknesses were positively correlated with isometric strength values at 30° and isokinetic work values at 180 °/s. While no correlations were detected on the first month measurements; similar to the baseline evaluations, femoral cartilage thicknesses were positively correlated with isokinetic strength values at 60 °/s and isokinetic work values at 180 °/s on the third month measurements.
Discussion
In this study, we aimed to explore whether/how femoral cartilage thickness might change with knee muscle strengthening. Our results have shown that while the knee muscle strength starts to increase on the first month, a parallel/positive change in the femoral cartilage thickness starts to be seen on the third month of exercise therapy.
Although there are no studies in the literature that have examined directly the relationship between cartilage thickness and knee muscle strength; it has been reported that femoral cartilage thickness decreases in conditions where there is immobilization and a generalized decrease in muscle strength [7, 15, 16]. Likewise, in some rheumatic diseases that may cause muscle weakness, femoral cartilage thickness was found to be thinner [8, 17]. Taking into account the parallelism between knee muscle strength and femoral cartilage thickness in our study, the findings of the aforementioned studies might be considered to noteworthy as regards the parallelism in the reverse direction.
In an animal study by Maldonado et al. [18], rats were evaluated in four—control, immobilized, exercised, and exercised and then immobilized—groups. While cartilage thicknesses decreased significantly in the immobilized group, they were unaffected in the exercised and then immobilized group, and significantly increased in the exercised group. Their findings seem to be in line with our results of increased cartilage thicknesses on the third month controls. Herewith, although we were not able to exclude the possibility of cartilage edema (actually causing the increased thickness), we considered it to be less likely since increased thickness was significant on the third month but not in the early phase of exercise therapy. Further, it is well-known that as the periarticular muscle strength increases, mechanical load is shifted from the joint to the muscle compartment (i.e., the main goal of exercise therapy) [19]. Therefore, we imply that the increased cartilage thickness in the late phase might be more likely associated with cartilage regeneration as the muscles have already started to mechanically support the joint (load) after the first month.
The lack of a histological examination seems to be major drawback of our study. Yet, our discussion as regards increased cartilage thickness (edema vs. regeneration) would have been readily clarified in that sense.
To conclude, in the light of our first and preliminary findings, we propose that femoral cartilage thicknesses increase on the third month of exercise therapy. Since this late-phase thickening parallels the earlier increase in muscle strength (starting on the first month), we speculate that the regeneration rather than the edema might be the primary underlying cause. Further studies with longer follow up and histological evaluations are definitely warranted to explore the exact mechanism(s) and the long term maintenance of increased cartilage thickness.
References
Hunter DJ, Eckstein F (2009) Exercise and osteoarthritis. J Anat 214(2):197–207. doi:10.1111/j.1469-7580.2008.01013.x
Sezer I, Illeez OG, Tuna SD, Balci N (2010) The relationship between knee osteoarthritis and osteoporosis. Eurasian J Med 42(3):124–127. doi:10.5152/eajm.2010.35
Tuna S, Balci N (2014) The relationship between radiological severity and functional status in patients with knee osteoarthritis. Clin Rheumatol 33(5):667–670. doi:10.1007/s10067-014-2511-8
Omori G, Koga Y, Tanaka M, Nawata A, Watanabe H, Narumi K, Endoh K (2013) Quadriceps muscle strength and its relationship to radiographic knee osteoarthritis in Japanese elderly. J Orthop Sci 18(4):536–542. doi:10.1007/s00776-013-0383-4
Kaya A, Kara M, Tiftik T, Tezcan ME, Ozturk MA, Akinci A, Ozcakar L (2013) Ultrasonographic evaluation of the femoral cartilage thickness in patients with systemic lupus erythematosus. Rheumatol Int 33(4):899–901. doi:10.1007/s00296-012-2462-9
Kara M, Tiftik T, Oken O, Akkaya N, Tunc H, Ozcakar L (2013) Ultrasonographic measurement of femoral cartilage thickness in patients with spinal cord injury. J Rehabil Med 45(2):145–148. doi:10.2340/16501977-1092
Tunc H, Oken O, Kara M, Tiftik T, Dogu B, Unlu Z, Ozcakar L (2012) Ultrasonographic measurement of the femoral cartilage thickness in hemiparetic patients after stroke. Int J Rehabil Res Int Z Rehabilitationsforschung Rev İnt Rech Readapt 35(3):203–207. doi:10.1097/MRR.0b013e3283532736
Kilic G, Kilic E, Akgul O, Ozgocmen S (2014) Decreased femoral cartilage thickness in patients with systemic sclerosis. Am J Med Sci 347(5):382–386. doi:10.1097/MAJ.0b013e31829a348b
Lee CL, Huang MH, Chai CY, Chen CH, Su JY, Tien YC (2008) The validity of in vivo ultrasonographic grading of osteoarthritic femoral condylar cartilage: a comparison with in vitro ultrasonographic and histologic gradings. Osteoarthr Cartil/OARS, Osteoarthr Res Soc 16(3):352–358. doi:10.1016/j.joca.2007.07.013
Mathiesen O, Konradsen L, Torp-Pedersen S, Jorgensen U (2004) Ultrasonography and articular cartilage defects in the knee: an in vitro evaluation of the accuracy of cartilage thickness and defect size assessment. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA 12(5):440–443. doi:10.1007/s00167-003-0489-x
Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, Christy W, Cooke TD, Greenwald R, Hochberg M et al (1986) Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum 29(8):1039–1049
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 15(12):1833–1840
Tuzun EH, Eker L, Aytar A, Daskapan A, Bayramoglu M (2005) Acceptability, reliability, validity and responsiveness of the Turkish version of WOMAC osteoarthritis index. Osteoarthritis Cartilage 13(1):28–33. doi:10.1016/j.joca.2004.10.010
Lequesne MG (1997) The algofunctional indices for hip and knee osteoarthritis. J Rheumatol 24(4):779–781
Vanwanseele B, Lucchinetti E, Stussi E (2002) The effects of immobilization on the characteristics of articular cartilage: current concepts and future directions. Osteoarthr Cartil/OARS, Osteoarthr Res Soc 10(5):408–419. doi:10.1053/joca.2002.0529
Ando A, Suda H, Hagiwara Y, Onoda Y, Chimoto E, Saijo Y, Itoi E (2011) Reversibility of immobilization-induced articular cartilage degeneration after remobilization in rat knee joints. Tohoku J Exp Med 224(2):77–85
Batmaz I, Kara M, Tiftik T, Yildiz M, Cevik R, Ozcakar L (2015) Ultrasonographic measurement of the femoral cartilage thickness in patients with Behcet’s disease. West Indian Med J 63(7). doi:10.7727/wimj.2013.337
Maldonado DC, Silva MC, Neto Sel R, de Souza MR, de Souza RR (2013) The effects of joint immobilization on articular cartilage of the knee in previously exercised rats. J Anat 222(5):518–525. doi:10.1111/joa.12036
Sharifnezhad A, Marzilger R, Arampatzis A (2014) Effects of load magnitude, muscle length and velocity during eccentric chronic loading on the longitudinal growth of the vastus lateralis muscle. J Exp Biol 217(Pt 15):2726–2733. doi:10.1242/jeb.100370
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Subjects were informed about the study procedure and they consented to participate. The local ethics committee approved the study protocol.
Disclosures
None.
Rights and permissions
About this article

Cite this article
Tuna, S., Balcı, N. & Özçakar, L. The relationship between femoral cartilage thickness and muscle strength in knee osteoarthritis. Clin Rheumatol 35, 2073–2077 (2016). https://doi.org/10.1007/s10067-016-3271-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-016-3271-4