
Abstract
Exome sequencing is an effective way to identify genetic causes of etiologically heterogeneous conditions such as developmental delay and intellectual disabilities. Using exome sequencing, we have identified four patients with similar phenotypes of developmental delay, intellectual disability, failure to thrive, hypotonia, ataxia, and tooth enamel defects who all have the same de novo R331W missense variant in C-terminal binding protein 1 (CTBP1). CTBP1 is a transcriptional regulator critical for development by coordinating different regulatory pathways. The R331W variant found in these patients is within the C-terminal portion of the PLDLS (Pro-Leu-Asp-Leu-Ser) binding cleft, which is the domain through which CTBP1, interacts with chromatin-modifying enzymes and mediates chromatin-dependent gene repression pathways. This is the first report of mutations within CTBP1 in association with any human disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Whole exome sequencing (WES) is an effective method to identify the molecular basis of etiologically complex conditions such as neurodevelopmental disorders and intellectual disability and is able to determine a genetic etiology in 20–30 % of cases [1–4]. In individuals with severe neurodevelopmental disorders with decreased reproductive fitness, the majority of the causative variants identified are due to de novo mutations that are more readily identified by using a trio (proband-parent) based sequencing strategy [5].
Here we describe a single, recurrent de novo R331W missense variant in C-terminal binding protein 1 (CTBP1) in four unrelated individuals with similar phenotypes of developmental delay, intellectual disability, hypotonia, ataxia, difficulty with weight gain, and enamel defects of the teeth. CTBP1 is located on chromosome 4p16 and is a transcriptional co-repressor critical for gene regulation during human development and in cancer. CTBP1 serves as an important scaffolding protein that recruits chromatin-modifying enzymes to specific areas of the genome and coordinates gene expression programs [6]. CTBP1 specifically regulates gene expression during development, apoptosis, and oncogenesis. Despite the critical role of CTBP1 in many cellular processes, this is the first report of a mutation within CTBP1 causing human disease.
Materials and methods
Informed consent was obtained from all individual participants included in the study. This study was approved by the Institutional Review Board of Columbia University.
Whole-exome sequencing
Genomic DNA was extracted from whole blood from affected children and their parents. Exome sequencing was performed on exon targets captured using the Agilent SureSelect Human All Exon V4 (50 Mb) kit or Clinical Research Exome kit (Agilent Technologies, Santa Clara, CA). The sequencing methodology and variant interpretation protocol have been previously described [7].
Results
WES was performed on 5471 trios containing probands with neurodevelopmental disorders. WES produced an average of ∼13 GB of sequence per sample. Mean coverage of captured regions was ∼150× per sample, with >96 % covered with at least 10× coverage, an average of >92 % of base call quality of Q30 or greater, and an overall average mean quality score of >Q36.
Among the 5471 trios sequenced, three unrelated individuals were found to have the same novel de novo genetic variant, C991T, in CTBP1, resulting in a R331W missense substitution. In the fourth patient, there was evidence of low-level somatic mosaicism with the variant found present in 4/75 (5.3 %) maternal reads (95 % CI = 1.5–13 %). These exons had similar depth and extent of coverage to our overall WES, and the C991T variant was confirmed to be present and de novo by Sanger sequencing in all four families. This C991T CTBP1 variant has not been previously reported and is not present in ClinVar, dbSNP, ExAC, COSMIC, CBIOportal, or our local database of 24,578 exomes. The R331W variant, a change from the positively charged arginine to the large aromatic tryptophan amino acid, is predicted to be deleterious by SIFT, MutationTaster, FATHMM, MetaSVM, PROVEAN, and Polyphen prediction programs [8–13]. CTBP1 is predicted to be among the top 10 % of haploinsufficient genes [14]. The RVIS score for CTBP1 is 0.74 predicting it to be among the 13.94 % most intolerant genes to variation [15]. CTBP1 has an estimated mutation rate of 3.127e−05 leading to a TADA corrected p-value of 0.039 for identifying four de novo missense variants within CTBP1 over our sample size. Additionally, there are no reported copy number variants of CTBP1 alone, although the gene is localized within the Wolf-Hirschhorn syndrome critical region (4p16.3) (Database of Genomic Variants).
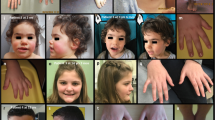
The four unrelated patients with the identical de novo R331W variant in CTBP1 have similar phenotypes. These four patients range in age from 8 to 20 years old and all have developmental delay, ataxia, hypotonia, difficulty with weight gain, and tooth defects (Table 1). All patients were delayed in reaching their motor milestones mainly related to ataxia and muscle weakness. All four patients had normal growth parameters at birth but in childhood had difficulty with feeding, requiring gastric tube feeding in three of the patients, and associated with being underweight with short stature. Muscle biopsies were performed in all cases and demonstrated non-specific findings. All four patients demonstrated ataxia manifested through impaired walking, standing, and dysarthria present on the first physical examination by a geneticist. Three patients have tooth enamel hypoplasia, and one has wide-spaced incisors with brownish discolored primary incisors (Fig. 1a). Three patients have intellectual disability. Dysmorphic features are not prominent among these patients, although one patient has a highly arched palate and retrognathia and another has frontal bossing and deep-set eyes. Two patients had recurrent pneumonias attributed to aspiration events. All four patients had a MRI of the brain performed and in two of these patients, there was evidence of cerebellar volume loss with vermian atrophy (Fig. 1b). Additional clinical features found in each individual case are summarized in Table 1. The proband’s mother who was mosaic for the R331W variant is phenotypically normal with no major neurologic deficits.

a Tooth enamel hypoplasia along with enamel discoloration found in patient 2. b Evidence of cerebellar volume loss and vermian atrophy in patient 1. Representative MRI images from patient 1 showing sagittal (top row) and axial views (bottom row) of cerebellum at 8 (left column) and 4 (right column) years of age showing progressive vermian atrophy. Arrows in the sagittal view show marked vermian atrophy while arrows in the axial view highlight cerebellar volume loss
Discussion
We have identified a recurrent de novo R331W missense variant in CTBP1 associated with severe developmental delay, intellectual disability, hypotonia, ataxia, difficulty with weight gain, and tooth enamel defects. CTBP1 is a highly conserved transcriptional co-repressor that modulates gene expression in multiple cellular pathways (Fig. 1). In invertebrates such as Drosophila, there is a single homolog of CTBP that is essential for development whereas in vertebrates there are two paralogs, CTBP1 and CTBP2 [16, 17]. CTBP1 and CTBP2 are highly homologous and R331 is conserved between the two genes. In mice, loss of Ctbp1 is associated with 30 % smaller offspring and one quarter of the Ctbp1 −/− mice die by postnatal day 20. Loss of CTBP2 or loss of both CTBP1 and CTBP2 causes early embryonic lethality suggesting overlapping but distinct functions for these two genes [18]. Both in mice and in humans, CTBP1 is ubiquitously expressed in all tissues [18, 19].
CTBP1 was originally identified as an E1 oncogene-binding partner and thus has been linked to oncogenesis, likely via its role in DNA damage repair [20]. Subsequent studies better elucidated the function of CTBP1 in transcriptional regulation. CTBP1 is thought to function mainly in transcriptional repression through recruitment of histone-modifying enzymes such as histone deacetylases and methyltransferases. CTBP1 has also been shown to have nicotinamide adenine dinucleotide (NAD)-dependent hydrogenase activity that is thought to be important for dimerization [21].
CTBP1 has multiple domains that mediate protein-protein interactions including PDZ, NAD(H), Arg-Arg-Thr (RRT), and Pro-Leu-Asp-Leu-Ser (PLDLS) binding cleft domains (Fig. 2). The R331W variant is within the PLDLS binding cleft. Through these domains, CTBP1 plays a critical role as a scaffolding protein for transcription factors and chromatin-modifying enzymes. CTBP1 has been shown to bind to many transcription factors including ZEB1/2, ZNF217, RUNX1, MYC, WNT, and COREST. Similarly, CTBP1 binds many chromatin-modifying enzymes including HDAC1, HDAC2, LSD1, PC2, and G9a [22]. By biochemical purification, CTBP1 was shown to complex with multiple chromatin-modifying enzymes and transcription factors simultaneously [22]. CTBP1 is thought to dimerize and direct histone-modifying enzymes to specific areas of the genome by binding to transcription factors that have DNA sequence specificity.

Domain structure of CTBP1 and cross-species conservation. Domain structure of CTBP1 showing the PLDLS binding cleft (cross-hatch) at both the N terminus and C terminus, as well as the RRT binding domain (black), NAD (H) binding region (gray), the dimerization domain, and the PDZ domain (stippling). The R331W missense mutation is marked with a triangle. Conservation of amino acid 331 of CTBP1 across 12 different species including H. Sapiens, P. troglodytes, M. mulatta, C. lupus, B. Taurus, M. musculus, R. norvegicus, G. gallus, X. tropicalis, D. rerio, C. elegans, and D. melanogaster. Red residues are conserved across all species, blue most, and gray are not conserved. R331 is highlighted with a box and is conserved in all organisms analyzed, except D. melanogaster
CTBP1 interacts with chromatin-modifying enzymes through its PLDLS binding cleft [6]. The PLDLS binding cleft is formed by two regions, one towards the N terminus and the other toward the C terminus [21]. Both the N- and C-terminal regions of the PLDLS binding cleft are required for both transcriptional repression and binding of many of the histone-modifying enzymes including LSD1, HDAC2, G9a, and several transcription factors. The CTBP1 R331W variant identified in our patients is found within the C-terminal PLDLS binding cleft region and due to the change in charge at this residue may disrupt important protein-protein interactions [6]. This mutation may cause changes in chromatin modification and thereby affect gene expression. Chromatin-modifiers are a class of genes tightly linked to neurodevelopmental disorders, autism, and congenital heart disease [3, 23–25].
Enamel defects, perhaps the most specific aspect of the phenotype of the patients in this study, are observed in Sotos syndrome that is caused by pathogenic variants in NSD1, a histone methyltransferase [26]. Patients with Sotos syndrome have overgrowth, macrocephaly, dysmorphic features, hypotonia, and intellectual disability, and nearly 50 % of patients have been reported to have enamel defects and missing teeth. Tooth development is initiated through stratified epithelium and coordinated in part through transcription, suggesting an important role for chromatin regulation in this process [27]. Thus, pathogenic variants in other histone-modifying enzymes have previously been shown to phenotypically overlap with some features of our patients and these findings are likely due to gene expression changes.
As mentioned above, the R331W CTBP1 variant has not been previously reported and is not found in any exome databases; however, within ExAC there are four different predicted loss of function frameshift variants. These frameshift variants all cluster within first three exons of CTBP1 (http://exac.broadinstitute.org). We therefore speculate that the R331W variant could be acting through a dominant negative mechanism. Other missense variants (>400) have been identified throughout CTBP1 and haploinsufficiency in another possible, but we believe less likely, mechanism. The number of independent recurrences of the R331W CTBP1, variant in four independent patients with similar phenotypes including the highly specific enamel defect of the teeth further supports the important role of the 331 amino acid residue and suggests it is likely pathogenic.
To our knowledge, the de novo R331W variant described in our series of four patients is the first reported association of germline variants in CTBP1 with human disease and suggests an important role for CTBP1-coordinated chromatin regulation in human neurodevelopment. Additional functional studies and evaluation of this gene in a larger patient population are necessary to further elucidate the role of CTBP1 in human development and disease and to define the mechanism of the R331W allele.
References
Retterer K et al., Clinical application of whole-exome sequencing across clinical indications. Genet Med 2015
Yang Y et al. (2014) Molecular findings among patients referred for clinical whole-exome sequencing. JAMA 312(18):1870–1879
Gao Z et al. (2014) An AUTS2-Polycomb complex activates gene expression in the CNS. Nature 516(7531):349–354
Iglesias A et al. (2014) The usefulness of whole-exome sequencing in routine clinical practice. Genet Med 16(12):922–931
Veltman JA, Brunner HG (2012) De novo mutations in human genetic disease. Nat Rev Genet 13(8):565–575
Kuppuswamy M et al. (2008) Role of the PLDLS-binding cleft region of CtBP1 in recruitment of core and auxiliary components of the corepressor complex. Mol Cell Biol 28(1):269–281
Tanaka AJ et al. (2015) Mutations in SPATA5 are associated with microcephaly, intellectual disability, seizures, and hearing loss. Am J Hum Genet 97(3):457–464
Ng PC, Henikoff S (2003) SIFT: predicting amino acid changes that affect protein function. Nucleic Acids Res 31(13):3812–3814
Schwarz JM et al. (2010) MutationTaster evaluates disease-causing potential of sequence alterations. Nat Methods 7(8):575–576
Shihab HA et al. (2013) Predicting the functional, molecular, and phenotypic consequences of amino acid substitutions using hidden Markov models. Hum Mutat 34(1):57–65
Mohiyuddin M et al. (2015) MetaSV: an accurate and integrative structural-variant caller for next generation sequencing. Bioinformatics 31(16):2741–2744
Plasterer TN (2000) PROTEAN. Protein sequence analysis and prediction. Mol Biotechnol 16(2):117–125
Adzhubei IA et al. (2010) A method and server for predicting damaging missense mutations. Nat Methods 7(4):248–249
Huang N et al. (2010) Characterising and predicting haploinsufficiency in the human genome. PLoS Genet 6(10):e1001154
Petrovski S et al. (2013) Genic intolerance to functional variation and the interpretation of personal genomes. PLoS Genet 9(8):e1003709
Nibu Y, Zhang H, Levine M (1998) Interaction of short-range repressors with Drosophila CtBP in the embryo. Science 280(5360):101–104
Poortinga G, Watanabe M, Parkhurst SM (1998) Drosophila CtBP: a hairy-interacting protein required for embryonic segmentation and hairy-mediated transcriptional repression. EMBO J 17(7):2067–2078
Hildebrand JD, Soriano P (2002) Overlapping and unique roles for C-terminal binding protein 1 (CtBP1) and CtBP2 during mouse development. Mol Cell Biol 22(15):5296–5307
Uhlen M et al. (2005) A human protein atlas for normal and cancer tissues based on antibody proteomics. Mol Cell Proteomics 4(12):1920–1932
Schaeper U et al. (1995) Molecular cloning and characterization of a cellular phosphoprotein that interacts with a conserved C-terminal domain of adenovirus E1A involved in negative modulation of oncogenic transformation. Proc Natl Acad Sci U S A 92(23):10467–10471
Kumar V et al. (2002) Transcription corepressor CtBP is an NAD(+)-regulated dehydrogenase. Mol Cell 10(4):857–869
Shi Y et al. (2003) Coordinated histone modifications mediated by a CtBP co-repressor complex. Nature 422(6933):735–738
Montgomery RL et al. (2007) Histone deacetylases 1 and 2 redundantly regulate cardiac morphogenesis, growth, and contractility. Genes Dev 21(14):1790–1802
Lagger G et al. (2002) Essential function of histone deacetylase 1 in proliferation control and CDK inhibitor repression. EMBO J 21(11):2672–2681
Tachibana M et al. (2002) G9a histone methyltransferase plays a dominant role in euchromatic histone H3 lysine 9 methylation and is essential for early embryogenesis. Genes Dev 16(14):1779–1791
Kotilainen J et al. (2009) Premolar hypodontia is a common feature in Sotos syndrome with a mutation in the NSD1 gene. Am J Med Genet A 149A(11):2409–2414
Balic A, Thesleff I (2015) Tissue interactions regulating tooth development and renewal. Curr Top Dev Biol 115:157–186
Acknowledgments
We thank the families for their generous contributions. This work was supported in part by a grant from the Simons Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Megan Cho, Francisca Millan, Carin Yates, Kyle Retterer, Amber Begtrup, and Renkui Bai are employees of GeneDx. Wendy Chung is a consultant to BioReference Laboratories. The other authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Beck, D.B., Cho, M.T., Millan, F. et al. A recurrent de novo CTBP1 mutation is associated with developmental delay, hypotonia, ataxia, and tooth enamel defects. Neurogenetics 17, 173–178 (2016). https://doi.org/10.1007/s10048-016-0482-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10048-016-0482-4