
Abstract
The purpose of this study is to find out if the biological behavior and the capacity of the odontogenic keratocyst (OKC) in maintaining pathologic cells alive are more similar to the dentigerous cyst or to the ameloblastoma by assessing bcl-2. We searched MEDLINE, Web of Science, and Scopus for immunohistochemical studies reporting OKCs, dentigerous cysts, and ameloblastomas. Risk difference between the lesions expressing bcl-2 was the effect measure and a P value < 0.05 was considered to provide evidence to the effect estimates. OKCs have an estimated difference of 91% in the probability to express the bcl-2 over dentigerous cysts, but there is no difference in the expression of bcl-2 between OKCs and ameloblastomas. The present study demonstrated a great risk difference in the expression of bcl-2 between OKCs and dentigerous cysts and no risk difference between OKCs and ameloblastomas. OKC’s growth may indirectly be attributed to the anti-apoptotic effect of bcl-2 in the cystic epithelium and not only to the increase of its intraluminal pressure. Therefore, the classification of this lesion into keratocystic odontogenic tumor should be carefully reconsidered.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The latest World Health Organization (WHO) atlas on tumors of the head and neck (2017) [1] reclassified the keratocystic odontogenic tumor to odontogenic keratocyst (OKC). This odontogenic lesion is clinically more aggressive and presents a higher recurrence rate than other odontogenic cysts after treatment. OKCs are derived from remnants of the dental lamina or epithelial cell nests and microcysts located in the oral mucosa overlying the alveolar ridges [2,3,4], mainly in the posterior region of the jaws [5,6,7]. In this respect, the latest classification of the OKC [1] may bring about some confusion among surgeons and tends to lessen the alertness on how to treat this lesion adequately [6, 7]. The high recurrence rate of OKCs may be attributed to fragments of the cyst wall left behind after enucleation due to its fragile capsule [8]. Furthermore, the OKC may be difficult to be enucleated in scalloped regions of the lesion, which are possibly formed by its multicentric pattern of growth. This clinical scenario requires the complementary treatment of the bone cavity after an incomplete cyst enucleation [3, 7].
In recent years, assessment of proliferation markers has gained importance in the histological exam of cysts and tumors, particularly concerning the grade, stage, response to treatment, and prognosis of tumors. Several markers have already been investigated in the OKC and one of them is the B cell lymphoma/leukemia-2 gene (bcl-2). Bcl-2 is an anti-apoptotic gene that prevents normal and tumor cells from killing themselves, regulating the homeostasis of the cell population. It has been first discovered because chromosomal translocations involving the bcl-2 locus frequently occurred in certain human lymphomas, mainly in the follicular center B cell lymphoma [9]. Although bcl-2 plays an important role in tumorigenesis, tumor progression, and its overexpression detected in most low-grade malignancies in humans [10], it does not stimulate cell growth and proliferation, but “save” tumor cells from apoptosis by keeping them in the quiescent G0 state of the cell cycle when growth factors are lacking or absent [9]. These saved cells can proliferate once again under the stimulus of growth factors.
The present systematic review was performed to collect reliable data on the expression of bcl-2 in OKCs as compared with the dentigerous cyst (DC) and ameloblastoma (AMB). These data will provide a basis for a better understanding of the biological behavior of OKCs as being a cyst or a tumor. To the best of our knowledge, such a systematic review has not been carried out yet, but the results may have implications for the future understanding of the OKC.
Material and methods
Protocol
The present review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol [11] and the recommendations from the Cochrane Group [12], and it was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42019120997).
Focused question
We intended to answer the following focused question: is the biological behavior of the OKC regarding the expression of bcl-2 more similar to the dentigerous cyst or the ameloblastoma?
Eligibility criteria
Original immunohistochemical (IHC) studies written in English were considered in the present systematic review. Records that fulfilled the following items were considered: (a) inclusion of OKCs as well as dentigerous cysts (odontogenic cyst reference) and/or solid/multicystic ameloblastoma (odontogenic tumor reference); (b) outcome data considering the expression of bcl-2. The expression of bcl-2 in the OKC was compared with the DC and AMB, pointing to a cystic or tumor behavior of this lesion, respectively.
Records clearly including OKCs associated with the nevoid basal cell carcinoma syndrome, orthokeratocysts, and recurrent OKCs in their sample were not considered. Studies that met the inclusion criteria or those with doubtful information either in the title or abstract were selected for full-text assessment in the second round of this review. Reasons for rejection of studies were recorded for each report.
According to our protocol, OKCs, DCs, and AMBs should be preferably diagnosed based on the World Health Organization (WHO) criteria [1, 13, 14].
Search strategy
The first hit was conducted online by two independent reviewers (YSS and MN), in MEDLINE (via PubMed), Web of Science, and Scopus, from the inception until February 10 of 2019. Duplicate records were subsequently removed.
The following strategy was used: (((((bcl-1) OR bcl-2)) AND ((odontogenic keratocyst) OR keratocystic odontogenic)) AND ((dentigerous cyst) OR odontogenic cysts)) AND ((ameloblastoma) OR odontogenic tumors).
Study selection
Records that remained from the first hit were independently selected by reading their titles and abstract (first round). Disagreements in this selection were resolved by mutual discussion. Afterward, all records screened from the first round had their full text independently assessed for eligibility by the same reviewers.
Data collection process
The reviewers YSS and MN separately submitted all eligible studies to a qualitative synthesis using an extraction data form, including mainly (a) investigated marker(s); (b) primary and secondary antibodies used; (c) number of OKCs, DCs, and solid/multicystic AMBs; and (d) number of each lesion expressing the marker.
Subsequently, all extraction data forms with the results of each included study were verified together to calibrate the validity and reliability of this process.
Risk of bias across studies
To assess the quality of the studies, we adapted the checklist from the study of Slusarenko da Silva et al. [5] and from the “reporting recommendations for tumor marker prognostic studies” [15] to be used in the Review Manager Software 5.3 (Review Manager (RevMan) (Computer program). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). The queries of the included studies are briefly explained as follows:
-
a.
Lesions diagnosed as OKCs, DCs, and AMBs based on the WHO criteria;
-
b.
Detection and exclusion of confounding factors: syndromic OKCs;
-
c.
Detection and exclusion of confounding factors: recurrent OKCs;
-
d.
Detection and exclusion of confounding factors: AMBS other than solid/multicystic.
-
e.
State the marker examined, the study objectives, and any prespecified hypotheses;
-
f.
Specify the assay method used and provide a detailed protocol, including specific reagents or kits used, quality control procedures, reproducibility assessments, quantitation methods, and scoring and reporting protocols.
Summary measures and synthesis of results
OKCs have been separately confronted with DCs and AMBs. Meta-analysis was performed in the Review Manager software 5.3 and the risk difference (RD) between lesions expressing bcl-2 with a confidence interval (CI) of 95% was the effect measure. The inverse variance method was applied in a random-effect model. P value, from the Z test, for the meta-analysis summary effect of < 0.05 was considered to provide evidence to the effect estimates. The heterogeneity among studies was obtained from the chi-squared test.
Results
Study selection
The first hit retrieved 60 records from databases. The distribution of the searched records and the number of studies finally selected are shown in Fig. 1. Excluded studies [16,17,18] and reasons for refusal are shown in Table 1.

Flow diagram
Results of individual studies and synthesis of results
The characteristics of the studies are shown in Table 2. The risk of bias across studies is expressed in Fig. 2.

Risk of bias across studies
All 36 examined OKCs expressed the bcl-2 and 4 DCs out of the 36 DCs examined expressed the bcl-2 in the studies reporting both OKCs and DCs [19, 21]. The RD of − 0.91 (− 1.11, − 0.72) (P < 0.00001) of the pooled values pointed that OKCs have an estimated difference of 91% (statistically significant) in the probability to express the bcl-2 if compared with DCs (Fig. 3).

Meta-analysis and forest plots
There were 93 OKCs and 93 AMBs expressing bcl-2 out of the 96 OKCs and 96 AMBs examined in the studies reporting both lesions [20,21,22,23]. The RD of 0.00 (− 0.04, 0.04) (P = 1.00) of the pooled values pointed that there is no difference (not statistically significant) in the probability to express the bcl-2 between OKCs and AMBs (Fig. 3).
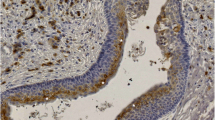
Regarding the detection of bcl-2 in OKCs of the included studies, it was expressed exclusively in the basal layer [19, 22], in the basal and suprabasal layer [20], and in the basal and parabasal layer [23], and 1 study did not mention where the bcl-2 was found [21].
Discussion
The prevalent difference of 91% in the risk to express the bcl-2 may suggest that the anti-apoptotic effect plays an important role in the growth of OKCs.
According to our results, we can assume that intramedullary expansion of OKCs may occur regardless of the increase of its intraluminal pressure. On the other hand, the cystic architecture of OKCs may be explained by the balance between cell proliferation in the basal layer and apoptosis in the surface layer of the lining epithelium, as stated by Kichi et al. [19]. They found an expression of bcl-2 exclusively in the basal layer of OKCs and concluded that the high potential of proliferative activity of cells and the inhibition of apoptosis by the expression of bcl-2 occur mainly in this layer. In turn, the apoptosis that occurs in the surface layer regulates the thickness of the cystic capsule. The abundant keratin and other exudates produced by such apoptosis drain into the cyst lumen, facilitating the expansion of OKCs [19], but the authors of the present systematic review believe that it is not enough to determine the local aggressiveness of OKCs.
The epithelial layer where the bcl-2 is most expressed also seems to predict the biological behavior of OKCs. Piattelli et al. [24] found a strong positivity of bcl-2 in the cells of the basal layer, reporting that this layer represents the proliferative compartment of this lesion and the bcl-negative suprabasal cells suggest downregulation of bcl-2 during the process of final differentiation of cells. This downregulation of bcl-2 in the suprabasal layer may be attributed to a low activity of the Hedgehog (Hh) signaling pathway mediated by Gli2 [25].
Gli2 belongs to a group of transcription factors that controls the Hh-mediated alterations in gene expression in responsive cells and it regulates a broad range of downstream gene targets, including bcl-2. The Hh/Gli signaling plays an important role in the regulation of epithelial cell proliferation and Gli2 overexpression may also contribute to bcl-2 overexpression and tumorigenesis due to alterations in the upstream activity of the Hedgehog pathway [25, 26].
Despite the expression of bcl-2 which is equal between OKCs and ameloblastomas, bcl-2 alone cannot be conclusive to determine the OKC as an odontogenic tumor because the comprehension of the biological behavior of a tumor is far more complex. Nonetheless, this result adds weight of evidence to the concept that the OKC is prone to behave as an odontogenic tumor.
Interestingly, despite the cystic architecture of OKCs, they did not behave as an odontogenic cyst for several times. For example, Emerson et al. [27] described the extension of two recurrent OKCs in the mediastinum, via the neck. Other authors have already reported the extension of OKCs into the base of the skull [28,29,30]. Regular odontogenic cysts do not behave this way [6].
Eight percent of the studies included in the meta-analysis of the present systematic review did not report at all on what WHO histological criteria they diagnosed their sample [19,20,21,22].
Regarding the detection of confounding factors that may have introduced bias and influenced the results expressed in the meta-analysis, unfortunately, in 60% of the included studies, no mention was made of the presence of syndromic OKCs [19, 21, 22] and in 100%, no mention was made of the presence of recurrent OKCs [19,20,21,22,23]. Furthermore, all studies reporting ameloblastomas could have included AMBs other than solid/multicystic [20,21,22,23]. All studies but one [22] reported in detail the IHC assay methods, validating the IHC data of the present systematic review.
Although no heterogeneity was detected among studies reporting OKCs vs. AMBs (I2 = 0%, P = 1.00), a considerable heterogeneity was detected among studies reporting OKCs vs. DCs (I2 = 69%, P = 0.07). Therefore, we incorporated the random-effect model in both meta-analyses [12] considering that the clinical behavior of OKCs may be unpredictable.
Conclusion
The present study demonstrated a great risk difference in the expression of bcl-2 between OKCs and dentigerous cysts and no risk difference between OKCs and ameloblastomas. Seen in these terms, OKC’s growth should also be attributed to the anti-apoptotic effect of bcl-2 in the cystic epithelium and not only to the increase of its intraluminal pressure, commonly seen in regular odontogenic cysts. Therefore, the classification of this lesion into keratocystic odontogenic tumor should be carefully reconsidered, and provided further systematic reviews on other tumor markers expressed in the OKC give strength or refute to the concept that OKC is an odontogenic tumor.
References
El-Naggar AK, JKC C, Grandis JR, Takata T, Slootweg PJ (2017) WHO classification of head and neck tumours, 4th edn. IARC, Lyon
Stoelinga PJ, Peters JH (1973) A note on the origin of keratocysts of the jaws. Int J Oral Surg 2:37–44
Stoelinga PJ (2001) Long-term follow-up on keratocysts treated according to a defined protocol. Int J Oral Maxillofac Surg 30:14–25
Stoelinga PJ (2003) Etiology and pathogenesis of keratocysts. Oral Maxillofac Surg Clin North Am 15:317–324
Slusarenko da Silva Y, Stoelinga PJW, Naclério-Homem MDG (2019) The presentation of odontogenic keratocysts in the jaws with an emphasis on the tooth-bearing area: a systematic review and meta-analysis. Oral Maxillofac Surg 23:133–147
Stoelinga PJW (2019) Keratocystic odontogenic tumour (KCOT) has again been renamed odontogenic keratocyst (OKC). Int J Oral Maxillofac Surg 48:415–416
Slusarenko da Silva Y, Naclério-Homem MG (2018) Conservative treatment of primary and nonsyndromic odontogenic keratocyst: an overview of the practice. Int J Oral Dent Health 4:1–6
DeGould MD, Goldberg JS (1991) Recurrence of an odontogenic keratocyst in a bone graft. Report of a case. Int J Oral Maxillofac Surg 20:9–11
Strasser A, Vaux DL (2018) Viewing BCL2 and cell death control from an evolutionary perspective. Cell Death Differ 25:13–20
Lo Muzio L, Staibano S, Pannone G, Bucci P, Nocini PF, Bucci E, De Rosa G (1999) Expression of cell cycle and apoptosis-related proteins in sporadic odontogenic keratocysts and odontogenic keratocysts associated with the nevoid basal cell carcinoma syndrome. J Dent Res 78:1345–1353
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097
Higgins JPT, Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. Available from http://handbook-5-1.cochrane.org/ [Accessibility verified December 1, 2019]
Kramer IRH, Pindborg JJ, Shear M (1992) Histological typing of odontogenic tumours, 2nd edn. Springer Verlag, Berlin
Barnes L, Eveson JW, Reichart P, Sidransky (2005) Head and neck tumours WHO classification of tumours, 3rd edn. IARC Press, Lyon
McShane LM, Altman DG, Sauerbrei W, Taube SE, Gion M, Clark GM (2005) Statistics Subcommittee of the NCI-EORTC Working Group on Cancer Diagnostics. Reporting recommendations for tumour MARKer prognostic studies (REMARK). Br J Cancer 93:387–391
Soluk Tekkeşın M, Mutlu S, Olgaç V (2012) Expressions of bax, bcl-2 and Ki-67 in odontogenic keratocysts (Keratocystic Odontogenic Tumor) in comparison with ameloblastomas and radicular cysts. Turk Patoloji Derg 28:49–55
Zhang LZ, Man QW, Liu JY, Zhong WQ, Zheng YY, Zhao YF, Liu B (2018) Overexpression of Fra-1, c-Jun and c-Fos in odontogenic keratocysts: potential correlation with proliferative and anti-apoptotic activity. Histopathology 73:933–942
Vered M, Peleg O, Taicher S, Buchner A (2009) The immunoprofile of odontogenic keratocyst (keratocystic odontogenic tumor) that includes expression of PTCH, SMO, GLI-1 and bcl-2 is similar to ameloblastoma but different from odontogenic cysts. J Oral Pathol Med 38:597–604
Kichi E, Enokiya Y, Muramatsu T, Hashimoto S, Inoue T, Abiko Y, Shimono M (2005) Cell proliferation, apoptosis and apoptosis-related factors in odontogenic keratocysts and in dentigerous cysts. J Oral Pathol Med 34:280–286
Phull K, Metgud R, Patel S (2017) A study of the distribution of B-cell lymphoma/leukemia-2 in odontogenic cyst and tumors: histochemical study. J Cancer Res Ther 13:570–575
Razavi SM, Torabinia N, Mohajeri MR, Shahriyary S, Ghalegolab S, Nouri S (2015) Expression of Bcl-2 and epithelial growth factor receptor proteins in keratocystic odontogenic tumor in comparison with dentigerous cyst and ameloblastoma. Dent Res J (Isfahan) 12:342–347
Sindura C, Babu C, Mysorekar V, Kumar V (2013) Study of immunohistochemical demonstration of Bcl-2 protein in ameloblastoma and keratocystic odontogenic tumor. J Oral Maxillofac Pathol 17:176–180
Tenorio JR, Santana T, Queiroz SI, de Oliveira DH, Queiroz LM (2018) Apoptosis and cell cycle aberrations in epithelial odontogenic lesions: an evidence by the expression of p53, Bcl-2 and Bax. Med Oral Patol Oral Cir Bucal 23:e120–e125
Piattelli A, Fioroni M, Rubini C (1998) Differentiation of odontogenic keratocysts from other odontogenic cysts by the expression of bcl-2 immunoreactivity. Oral Oncol 34:404–407
Shimada Y, Katsube K, Kabasawa Y, Morita K, Omura K, Yamaguchi A, Sakamoto K (2013) Integrated genotypic analysis of hedgehog-related genes identifies subgroups of keratocystic odontogenic tumor with distinct clinicopathological features. PLoS One 8:e70995
Grachtchouk M, Liu J, Wang A, Wei L, Bichakjian CK, Garlick J, Paulino AF, Giordano T, Dlugosz AA (2006) Odontogenic keratocysts arise from quiescent epithelial rests and are associated with deregulated hedgehog signaling in mice and humans. Am J Pathol 169:806–814
Emerson TG, Whitlock RI, Jones JH (1972) Involvement of soft tissue by odontogenic keratocysts (primordial cysts). Br J Oral Surg 9:181–185
Jackson IT, Potparic Z, Fasching M, Schievink WI, Tidstrom K, Hussain K (1993) Penetration of the skull base by dissecting keratocyst. J Craniomaxillofac Surg 21:319–325
Franc C, Cresseaux P, Richard L, Breton P, Freidel M (1996) The keratocyst or epidermoid cyst: the current state of understanding apropos of a case with intracranial involvement. Rev Stomatol Chir Maxillofac 97:270–282
Soost F, Stoll C, Gerhardt O, Neumann HJ (1999) Keratocysts of the jaws with an expansion to the skull base. Zentralbl Neurochir 60:11–14
Acknowledgments
The first author of the present work acknowledges the Faculty of Dentistry of the University of São Paulo because this study is derived from a major project of the post-doctorate program of this institution.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
For this type of study, formal consent is not required.
Informed consent
Not applicable. This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Slusarenko da Silva, Y., Naclério-Homem, M. A systematic review on the expression of bcl-2 in the nonsyndromic odontogenic keratocyst: should it be considered a cyst or a tumor?. Oral Maxillofac Surg 24, 277–282 (2020). https://doi.org/10.1007/s10006-020-00856-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-020-00856-5