
Abstract
Purpose
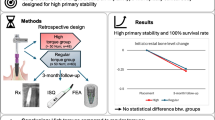
This retrospective chart review study assessed patient records to determine implant insertion torque (IT) and implant stability quotient (ISQ) values during implant placement to evaluate the correlation with cortical bone anchorage (mono- or bicortical).
Methods
Primary stability data (IT during implant placement surgery and ISQ values immediately after implant placement) and cone beam computed tomography of 33 patients (165 implants) were assessed. Patients were divided into the following groups: G1, implants with apical cortical bone contact; G2, implants with bicortical bone contact (apical and cervical regions); and G3, implants with cervical cortical bone contact.
Results
Sixty-eight implants were excluded due to cortical bone contact on regions other than implant apical or cervical. Ninety-seven implants were therefore assessed for this study. No implant failure was found after a mean 70.42-month follow-up time. Implants with bicortical anchorage (G2) showed higher IT (64.1 Ncm) during implant placement and higher ISQ values (76) (p < 0.05). Monocortical implants (G1, apical, and G3, cervical) showed similar IT (G1 52.3 and G3 54.3) and ISQ values (G1 71.9 and G3 73) (p > 0.05). No correlation (Pearson correlation coefficient) was found between the two stability measurement devices for the different cortical bone anchorages that were analyzed (G1 0.190, G2 0.039, and G3 − 0.027) (p > 0.05).
Conclusions
Insertion torque values and implant stability quotients were influenced by cortical bone contact. No significant correlation was found between IT and ISQ values—higher insertion torque values do not necessarily lead to higher implant stability quotients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The choice to immediately load a dental implant is guided by the primary stability after implant placement. Insertion torque (IT) and resonance frequency analysis (RFA) are often used to assess implant stability [1]. Measurement of the IT value using a torque ratchet is an easy and effective method. However, secondary stability cannot be assessed by the torque ratchet. RFA is a non-invasive method that can assess both primary and secondary stability—it can therefore be used to assess implant stability during different follow-up times and with implants under functional loads [2, 3].
The correlation between insertion torque and resonance frequency analysis remain unclear. Earlier studies [4, 5] found strong correlation between insertion torque and RFA during implant placement surgery. However, other studies [6, 7] found no correlation between the two methods used to assess implant stability. Initial implant stability is influenced by implant design, implant length, bone density, cortical bone thickness, and implant placement depth [6, 8,9,10,11,12].
Cortical anchorage is related with a higher insertion torque. Bicortical bone contact is commonly recommended to improve osseointegration [12,13,14]. Denser type II bone led to higher implant stability quotient (ISQ) values compared to bone types III and IV [8]. However, a 15-year retrospective study found no correlation between cortical bone contact and marginal bone remodeling [13]. The influence of cortical anchorage on the primary stability of internal tapered implants requires further analysis. This retrospective observational study assessed patient records to determine implant IT and ISQ values during implant placement and the achieved cortical bone contact (mono- or bicortical) to investigate the correlation between each parameter. The tested null-hypothesis was that there would be no significant correlation between the two methods used to evaluate implant stability and that the different cortical bone anchorage would not significantly influence the achieved stability.
Methods
Human subject ethical approval for this study was obtained from the Research Ethics Committee of the Pontifical Catholic University of Paraná (PUC/PR) (approval no. 1.004.033). All participants provided written informed consent before entering the study. The study included data recorded on dental charts that assessed the primary stability of dental implants (Morse taper, Neodent, Curitiba, PR, Brazil) and cone beam computed tomography (CBCT) of patients who participated in previous clinical studies.
Thirty-three patients were enrolled according to the following inclusion criteria: (a) postoperative CBCT images of dental implants with apical and/or cervical cortical bone contact (mono- or bicortical anchorage); (b) primary stability achieved during implant placement assessed by the torque ratchet (Neodent) and by resonance frequency analysis (RFA) (Osstell™, Osstell, Gothenburg, Sweden); (c) presence of five implants placed in the mandible interforaminal region. The following exclusion criteria was followed: (a) implants in contact with cortical bone in regions other than apical or cervical; (b) CBCT images with artifacts that interfered with the full visualization of the implant portion in contact with cortical bone; (c) examination charts with incomplete information of the implant primary stability.
All included patients had maxillary complete dentures and mandibular implant-supported full-arch fixed dental prosthesis (FAFDP). Each patient had five implants in the mandible interforaminal region that were placed at the Latin American Institute for Dental Research and Education (ILAPEO) between 2008 and 2013. A total amount of 165 implants were initially analyzed.
Cross sections of the CBCT images were analyzed in specialized software (Galaxis, Sirona Dental GmbH, Salzburg, Austria) by two calibrated examiners. Implant position was classified according to cortical bone anchorage (mono- or bicortical anchorage). The following groups were divided (Figs. 1 and 2): G1—implants with apical cortical bone contact (Fig. 1a); G2—implants with bicortical bone contact (apical and cervical regions) (Fig. 1b); and G3—implants with cervical cortical bone contact (Fig. 1c). Implant stability data for each implant assigned to its respective group was assessed. Insertion torque was assessed by a torque ratchet (Ncm) during implant placement surgery and the ISQ was assessed by resonance frequency analysis immediately after implant placement surgery. Both IT and ISQ values were assessed by the same surgeon that was placing the implants. The protocol for the ISQ measurements was the same for all implants—the measurements were performed on the buccal and proximal surfaces of the prosthetic abutments that were installed on the implants.

Cross sections of a cone beam computed tomography. a Apical cortical bone anchorage (G1). b Bicortical bone anchorage (G2). c Cervical cortical bone anchorage (G3)

Three-dimensional cone beam computed tomography reconstructions. a Apical cortical bone anchorage (G1). b Bicortical bone anchorage (G2). c Cervical cortical bone anchorage (G3)
Statistical comparison between groups was performed by one-way analysis of variance (ANOVA) and Kruskal-Wallis nonparametric statistical test (α = 0.05). Correlation between the different variables was assessed by Pearson correlation coefficient (α = 0.05).
Results
Sixty-eight CBCT images of implants were excluded from the study due to cortical bone contact on regions other than the implant apical or cervical. Ninety-seven implants were therefore analyzed and assigned to the following groups: G1 with 24 implants (6 patients); G2 with 32 implants (8 patients); and G3 with 41 implants (16 patients). Patients in group G1 aged 59 to 76 years (64.2 mean), patients in group G2 aged 46 to 69 years (58.9 mean), and patients in group G3 aged 42 to 85 years (62.2 mean). No implant failure was found after a mean 70.42-month follow-up time (40-month minimum and 88-month maximum follow-up times).
Table 1 shows the implant stability results that were found for each group in the study. Implants with bicortical anchorage (G2) showed both higher insertion torque during implant placement and higher ISQ values (p < 0.05). Monocortical implants (G1, apical, and G3, cervical) showed similar insertion torque and ISQ values (p > 0.05). No correlation was found between the values found by the two stability measurement devices for the different cortical bone contacts that were analyzed (p > 0.05) (Table 2).
Discussion
This retrospective study assessed patient records and investigated the achieved implant insertion torque and ISQ values during implant placement. Cortical bone anchorage (mono- or bicortical) was evaluated on CBCT images of patients with five interforaminal implants placed in the mandible. The results support partial rejection of the tested null-hypothesis. Bicortical bone contact significantly increased implant stability results. However, no significant correlation was found between the two methods used to evaluate implant stability.
Higher ISQ values were previously reported in thicker cortical bone in the mandible compared to the more trabecular bone in the maxilla [11]. Cortical bone thickness is important for the implant primary stability, whereas trabecular bone is of considerable importance for peri-implant bone healing [11]. Other studies [15,16,17] have also found that higher cortical bone thickness increases initial implant stability, which is in agreement with the present study. This is also in agreement with an earlier study that found that resonance frequency analysis was highly influenced by cortical density and thickness [10]. It can therefore be suggested that bicortical bone contact is a valuable resource to increase primary stability when planning to immediately load a dental implant.
Implant insertion torque is a mechanical parameter usually influenced by the surgical procedure, by the implant design, and by the bone quality at the implant insertion site [5]. Correlation between RFA and IT values is controversial. Some studies [5, 18] found a strong correlation between the two methods whereas others [6, 7] found no significant correlation. This study found no correlation between IT values and ISQ values for the implants that were analyzed. Higher insertion torque values therefore do not necessarily lead to higher implant stability quotients. A minimum insertion torque of 32 Ncm is recommended to immediately load the implant. However, an excessively high IT could lead to bone damage—friction between the implant surface and the bone wall should therefore be minimized during implant placement surgery [12].
The present study was a retrospective research. As with all retrospective studies, some chart data may not be so accurate and therefore patients with incomplete chart data were excluded from this study. Another limitation is that different clinicians placed the implants that were analyzed for this study. To minimize implant placement and measurement bias, the Research and Education Center (ILAPEO) where the implants were placed standardizes surgical procedures and IT measurements during implant placement surgeries. ISQ measurements are also standardized for all placed implants. Despite that, some inherent placement and measurement bias can be expected because of the different clinicians performing the procedures.
Conclusions
It can be concluded that insertion torque values and the implant stability quotient are influenced by cortical bone contact since bicortical bone anchorage led to a higher insertion torque and higher implant stability quotient compared to the other tested bone anchorages. No significant correlation was found between insertion torque and implant stability quotient values.
References
Thome E, Lee HJ, Sartori IA, Trevisan RL, Luiz J, Tiossi R (2015) A randomized controlled trial comparing interim acrylic prostheses with and without cast metal base for immediate loading of dental implants in the edentulous mandible. Clin Oral Implants Res 26:1414–1420
Meredith N (1998) Assessment of implant stability as a prognostic determinant. Int J Prosthodont 11:491–501
Atsumi M, Park SH, Wang HL (2007) Methods used to assess implant stability: current status. Int J Oral Maxillofac Implants 22:743–754
Turkyilmaz I, Tozum TF, Tumer C, Ozbek EN (2006) Assessment of correlation between computerized tomography values of the bone, and maximum torque and resonance frequency values at dental implant placement. J Oral Rehabil 33:881–888
Ohta K, Takechi M, Minami M, Shigeishi H, Hiraoka M, Nishimura M, Kamata N (2010) Influence of factors related to implant stability detected by wireless resonance frequency analysis device. J Oral Rehabil 37:131–137
da Cunha HA, Francischone CE, Filho HN, de Oliveira RC (2004) A comparison between cutting torque and resonance frequency in the assessment of primary stability and final torque capacity of standard and TiUnite single-tooth implants under immediate loading. Int J Oral Maxillofac Implants 19:578–585
Friberg B, Sennerby L, Meredith N, Lekholm U (1999) A comparison between cutting torque and resonance frequency measurements of maxillary implants. A 20-month clinical study. Int J Oral Maxillofac Surg 28:297–303
Sim CP, Lang NP (2010) Factors influencing resonance frequency analysis assessed by Osstell mentor during implant tissue integration: I. Instrument positioning, bone structure, implant length. Clin Oral Implants Res 21:598–604
Turkyilmaz I, McGlumphy EA (2008) Influence of bone density on implant stability parameters and implant success: a retrospective clinical study. BMC Oral Health 8:32
Bardyn T, Gedet P, Hallermann W, Buchler P (2009) Quantifying the influence of bone density and thickness on resonance frequency analysis: an in vitro study of biomechanical test materials. Int J Oral Maxillofac Implants 24:1006–1014
Roze J, Babu S, Saffarzadeh A, Gayet-Delacroix M, Hoornaert A, Layrolle P (2009) Correlating implant stability to bone structure. Clin Oral Implants Res 20:1140–1145
Park KJ, Kwon JY, Kim SK, Heo SJ, Koak JY, Lee JH, Lee SJ, Kim TH, Kim MJ (2012) The relationship between implant stability quotient values and implant insertion variables: a clinical study. J Oral Rehabil 39:151–159
Ivanoff CJ, Grondahl K, Bergstrom C, Lekholm U, Branemark PI (2000) Influence of bicortical or monocortical anchorage on maxillary implant stability: a 15-year retrospective study of Branemark System implants. Int J Oral Maxillofac Implants 15:103–110
Ivanoff CJ, Sennerby L, Lekholm U (1996) Influence of mono- and bicortical anchorage on the integration of titanium implants. A study in the rabbit tibia. Int J Oral Maxillofac Surg 25:229–235
Miyamoto I, Tsuboi Y, Wada E, Suwa H, Iizuka T (2005) Influence of cortical bone thickness and implant length on implant stability at the time of surgery—clinical, prospective, biomechanical and imaging study. Bone 37:776–780
Nkenke E, Hahn M, Weinzierl K, Radespiel-Troger M, Neukam FW, Engelke K (2003) Implant stability and histomorphometry: a correlation study in human cadavers using stepped cylinder implants. Clin Oral Implants Res 14:601–609
Boronat-Lopez A, Penarrocha-Diago M, Martinez-Cortissoz O, Minguez-Martinez I (2006) Resonance frequency analysis after the placement of 133 dental implants. Med Oral Patol Oral Cir Bucal 11:E272–E276
Turkyilmaz I (2006) A comparison between insertion torque and resonance frequency in the assessment of torque capacity and primary stability of Branemark system implants. J Oral Rehabil 33:754–759
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
de Oliveira Nicolau Mantovani, A.K., de Mattias Sartori, I.A., Azevedo-Alanis, L.R. et al. Influence of cortical bone anchorage on the primary stability of dental implants. Oral Maxillofac Surg 22, 297–301 (2018). https://doi.org/10.1007/s10006-018-0705-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-018-0705-y