
Abstract
Objective
We analyzed outcomes from immunocompromised patients with scalp squamous cell carcinoma (SCC) treated with surgical excision with and without radiation in order to explore 3-year disease-free survival and overall survival.
Study design
The study design was a retrospective chart review.
Setting
This study was conducted in a private practice setting.
Subjects and methods
The study included 53 immunocompromised patients with an average age of 63.2 years, with scalp squamous cell carcinoma. Pre-operative imaging dictated the extent of resection. Patients with bony involvement received wide local excision including full-thickness craniectomy and cranioplasty. Patients without bony involvement underwent wide local excision and outer-table calvarial resection. All patients were recommended to have post-operative radiation. Patients were followed for a minimum of 3 years.
Results
A total of 53 patients were included in the study. Six patients had pre-operative CT showing bone involvement and were treated with full-thickness craniectomy along with post-operative radiation. Fourteen patients without bone involvement on pre-operative CT were found to have positive bone involvement on final pathology. Forty-five patients underwent post-operative radiation. Patients treated with adjuvant radiation demonstrated a 3-year survival of 80 % and the overall survival was 62 %. In the surgery-only group, the 3-year survival was 62.5 % and the overall survival was 32.5 %.
Conclusions
Immunocompromised patients with scalp SCC have a poor prognosis. Early detection and treatment are crucial. Based on our results, we recommend wide local excision with at least outer-table calvarial resection, and post-operative radiation. Despite aggressive therapy, patients may still have distant, local, or regional recurrence.
Level of evidence: level 2b (retrospective cohort)
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Nonmelanoma skin cancer is currently the most common malignancy affecting humans, largely thought to be due to increasing exposure to ultraviolet radiation (UVR). Light skin color, freckles, older age, blue eyes, and history of previous skin cancer are other known risk factors [1]. Exposure to UVR can cause mutations in the deoxyribonucleic acid (DNA) chain, resulting in the formation of pyrimidine dimers that ultimately affect the integrity of the p53-mediated tumor suppression mechanism [2]. Additionally, ultraviolet radiation is thought to cause local immunosuppression by adversely affecting the ability of Langerhans cells in the skin to present antigen, leading to a decrease in activation of class 1 helper T cells (Th1). This cascade leads to a vast decrease in cell-mediated immunity [3].
Immunocompromised patients are at an increase risk of cutaneous and other malignancies. Patients suffering from chronic lymphocytic leukemia (CLL) have been shown to develop cutaneous malignancies with more aggressive behavior [4]. Decreased co-stimulation between T cells and antigen-presenting cells is a result of CD40 ligand downregulation in these patients. Decreased co-stimulation, inhibited antibody class switching, and decreased IL-2 cytokine together inhibit the immune system from mounting a robust anti-tumor response [5–8]. In addition, patients with blood dyscrasias treated with hematopoietic cell transplant (HCT) were found to have an increased incidence of cutaneous squamous cell carcinoma (SCC), melanoma, and basal cell carcinoma based on a meta-analysis and Cochrane review of 18 studies examining a conglomerate of over 1800 patients that were treated with HCT [9–12]. Similar to the general population, nonmelanoma skin cancer is also the most common skin cancer found in patients after solid organ transplant [13–15].
The increased incidence of cutaneous malignancy in immunocompromised patients has been well studied; however, there is a dearth of information specific to cutaneous SCC of the scalp in the immunocompromised patient. This information is important to the multidisciplinary team treating these patients, namely the head and neck surgeon, Mohs surgeon, and radiation oncologist. In this paper, we report our outcomes on 53 immunocompromised patients afflicted with scalp SCC in order to provide recommendations for treatment in this complicated group. To our knowledge, this is the only study of this nature in the English literature.
Methods
This study was approved by the institutional review board (IRB) at John Peter Smith Hospital. This was a retrospective study examining 53 immunocompromised patients treated for biopsy-proven scalp SCC. The cohort was comprised of 29 males and 24 females. Of the males, 15 patients had solid organ transplant, 12 had CLL, and 2 had HIV. Of the females, 16 were transplant patients, 7 had CLL, and 1 had HIV (Table 1). Patients were deemed to be immunocompromised by leukocyte count and functionality, presence of certain defining illnesses, and general medical condition. The average patient age was 63.2 years. Patients were followed for a minimum of 3 years. Any patient that did not follow up for a minimum of 3 years, had distant metastases on initial exam, or was suffering from active acquired immunodeficiency syndrome (AIDs) was excluded from the study.
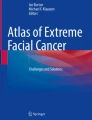
Pre-operative computed tomography (CT) was performed on all patients to assess tumor involvement of the calvarium. If the pre-operative CT was free of bone involvement, patients were treated with wide local excision including resection of the outer table of the calvarium. Patients with bone involvement on CT were treated with wide local excision including full-thickness craniectomy followed by cranioplasty (Fig. 1). Patients treated with Mohs excision had surgical margins at least 1 cm from obvious tumor extension; if treated with surgical excision, the margin was at least 1.5 cm from obvious tumor extent. All patients were recommended to have post-operative external beam radiation therapy (EBRT) for cutaneous treatment.

Algorithm for cranial bone resection based on pre-operative CT scan
Following resection, specimens were sent to the pathology lab to be evaluated for degree of differentiation, bone involvement, perineural involvement, and vascular involvement. Two separate pathologists from the same group evaluated all specimens.
Patients were followed for a minimum of 3 years, and outcomes measured included disease-free survival at 3 years and overall survival. To assess for locoregional recurrence or distal metastases, patients were routinely sent for post-treatment PET/CT. Patients with recurrence (local, regional, or distal) were appropriately referred for salvage surgery and radiation.
Results
Of the 53 patients, 6 patients were found to have pre-operative bone involvement while 47 patients did not have bone involvement on imaging. These 6 patients were treated with full-thickness craniectomy and subsequently reconstructed with cranioplasty. Of the 47 patients without bone involvement that were treated with outer-table resection, 14 (29.7 %) were found to have bone involvement on the final pathology.
Thirty-seven (69.8 %) patients were found to have perineural invasion, 2 (3.7 %) were found to have vascular involvement, and 11 (20.7 %) were noted to have both perineural and vascular invasion. Twenty-one (39.6 %) samples were poorly differentiated, 18 (33.9 %) were moderately differentiated, and 14 (26.4 %) were well differentiated (Table 2).
With regard to adjuvant radiation treatment, 45 patients complied with our recommendation, while 8 patients were not able due to patient refusal or prior irradiation. Of the 45 patients who were treated with surgery and adjuvant radiation, local recurrence occurred in 8 patients, regional lymph node metastases in 4 patients, and distant metastases in 4 patients. All of the patients with distant metastases and 3 of the patients with local recurrence expired. Two of the patients with local recurrence were offered salvage surgery but refused, while 1 developed late dermal metastatic disease following clearance of cancer. The 4 patients with regional recurrence were salvaged with surgery and radiation to the neck, after which 2 developed late dermal metastases and expired. These results are shown in Fig. 2. Each of the 4 patients with distant metastases had vascular involvement on initial surgical pathology. Of the patients with regional and local recurrence, all had perineural involvement on the initial specimen except 1 patient. The overall disease-free survival at 3 years was found to be 80 % while the overall survival was 62 %.

Treatment outcomes of patients that received post-operative radiation
Of the 8 patients who did not receive post-operative radiation, 2 were found to have distant metastases and expired. Three patients had local recurrence, and no patients had regional recurrence. In the patients with local recurrence, 2 were salvaged with surgery but 1 patient later expired from late distal dermal metastases. These results are shown in Fig. 3. Patients with distant metastases were found to have vascular involvement on pathology. The overall disease-free survival at 3 years was 62.5 % while the overall survival was 37.5 %.

Treatment outcomes of patients that did not receive post-operative radiation
Subgroup analysis based on tumor differentiation revealed 17 out of 21 (80.9 %) patients with a poorly differentiated tumor were disease free at 3 years, 13 out of 18 (72.2 %) patients with a moderately differentiated tumor were disease free at 3 years, and 11 out of 14 (78.5 %) patients with a well-differentiated tumor were disease free at 3 years. This data can be seen in Fig. 4. In order to analyze whether there was a relationship between differentiation and 3-year survival, a chi-square test was performed. The chi-square statistic was found to be 0.437 with a p value of 0.8. Comparing against an alpha value of 0.05, the two variables were found to be independent of each other, suggesting that degree of differentiation did not affect 3-year survival.

Disease-free patients stratified by degree of differentiation
Of the 6 patients with pre-operative bone involvement on CT scan, 2 developed local recurrence, 1 developed regional recurrence, and 1 developed distant metastases. Of the 14 patients with negative bone involvement on CT but found to have positive bone involvement on final pathology, 1 developed distant metastases, 1 had local recurrence, and no patients had regional recurrence.
Discussion
In the immunocompromised patient population, squamous cell carcinoma of the scalp presents a challenging problem for the treating physicians, as cutaneous malignancies in this group tend to be more aggressive in nature [4]. Due to the poor outcomes that these conditions portend, it is vital for the multidisciplinary team to diagnose and treat these malignancies in an expedited fashion.
It is well known that cutaneous malignancies have a higher incidence in the immunocompromised population; however, to our knowledge, this study is the first of its kind to be centered on outcomes and treatment strategies of scalp SCC. Our study retrospectively analyzed 53 immunocompromised patients who developed scalp SCC and were subsequently treated with surgical resection with or without radiation.
On pre-operative imaging, 6 out of 53 (11.3 %) patients were found to have bone involvement and underwent full-thickness craniectomy, while the remainder of the patients had no bone involvement on imaging and were treated with resection of the outer calvarial table. Interestingly, of these 47 patients, 14 (29.7 %) were found to have bone involvement on pathology review, suggesting that CT scan may not be accurate enough to detect early or microscopic bone involvement. However, due to the sample size limitations, it is difficult to recommend full-thickness craniectomy for all the patients due to the increased morbidity. Advanced imaging modalities, such as single-photon emission tomography (SPECT) combined with high-resolution CT (SPECT/CT), have been studied and show superior sensitivity and specificity in predicting bony involvement in oral cavity SCC compared to CT and MRI. The addition of SPECT/CT has potential in guiding treatment protocols for patients [16].
In our study, we found that perineural and vascular invasion were poor prognostic indicators. Isolated perineural invasion was found in 69.8 % (37 patients), 3.7 % (2 patients) were found to have only vascular involvement, and 20.7 % (11 patients) were found to have both perineural and vascular involvement. In the group of patients treated with both surgery and radiation, it was noted that all patients with distant metastases had vascular involvement on initial pathology while all patients with local or regional recurrence had only perineural involvement on initial pathology. In the group of patients that were not treated with radiation, all patients with distant metastases were found to have vascular involvement as well. Although a larger sample size is needed for statistical analysis, our results suggest that patients with vascular involvement may be more likely to develop distant metastases while those with perineural invasion may be more likely to develop local and regional recurrence.
Patients that were treated with surgery and radiation had a 3-year survival of 80 % and an overall survival of 62 %, while the 3-year survival in the nonradiation group was only 62.5 % and overall survival was 37.5 %. It seems that the addition of post-operative radiation lends to an increased disease-free and overall survival at the minimum follow-up period of 3 years. It is important to note that regardless of therapy regimen, significant recurrence has been found, suggesting that this population may have a poor prognosis even in the setting of aggressive treatment.
As our results are based on treatment data from the senior author (YD), future studies should be focused on multicenter collaboration. Although difficult to assess in this population, possibly from ethical limitations, prospective randomized controlled trials would be helpful in determining true differences in treatment regimen. This patient population may also suffer from co-morbidities confounding the true cause of mortality. Due to the disparity in patients receiving post-operative radiation and those being solely treated with surgery, statistical analysis is limited and heavily influenced by the small subject size in the nonradiation cohort.
Stockfleth et al. have suggested that the human papillomavirus (HPV) may play a role in cutaneous SCC in transplant patients. Their data have shown that 75 % of squamous cell carcinoma specimens from immunocompromised patients were positive for HPV DNA while only 35 % of specimens were positive in immunocompetent patients. Moreover, the amount of HPV viral DNA was also greater in the immunocompromised subjects. In order to evaluate specificity to SCC, the same study was performed on patients with basal cell carcinoma and no difference between immunocompromised and immunocompetent patients was found [17]. Findings from this study raise the possibility of HPV being a causative factor in scalp SCC in this population, or perhaps a risk factor that may act synergistically with local immune system derangement. Future studies may also seek to examine the use of HPV quadrivalent vaccination in immunocompromised patients at the time of diagnosis.
Conclusion
Immunocompromised patients with squamous cell carcinoma of the scalp have a poor prognosis at baseline, especially when perineural and vascular involvement is present. Based on our findings, we recommend an aggressive treatment approach with at least wide surgical excision, outer-table calvarial resection, and post-operative radiation in all patients without contraindication to these procedures. Immunocompromised patients without skin malignancies should be encouraged to perform routine self-examinations and have regular dermatologic evaluation.
References
Berg D, Otley CC (2002) Skin cancer in organ transplant recipients: epidemiology, pathogenesis, and management. J Am Acad Dermatol 47(1):1–17
Brin L, Zubair AS, Brewer JD (2014) Optimal management of skin cancer in immunosuppressed patients. Am J Clin Dermatol 15(4):339–56
Yu SH, Bordeaux JS, Baron ED (2014) The immune system and skin cancer. Adv Exp Med Biol 810:182–91
Velez NF, Karia PS, Vartanov AR, Davids MS, Brown JR, Schmults CD (2014) Association of advanced leukemic stage and skin cancer tumor stage with poor skin cancer outcomes in patients with chronic lymphocytic leukemia. JAMA Dermatol 150(3):280–287
Cantwell M, Hua T, Pappas J, Kipps TJ (1997) Acquired CD40-ligand deficiency in chronic lymphocytic leukemia. Nat Med 3(9):984–9
Cerutti A, Zan H, Schaffer A et al (1998) CD40 ligand and appropriate cytokines induce switching to IgG, IgA, and IgE and coordinated germinal center and plasmacytoid phenotypic differentiation in a human monoclonal IgM+IgD+ B cell line. J Immunol 160(5):2145–57
Semenzato G, Foa R, Agostini C et al (1987) High serum levels of soluble interleukin 2 receptor in patients with B chronic lymphocytic leukemia. Blood 70(2):396–400
Pavlidis NA, Manoussakis MN, Germanidis GS, Moutsopoulos HM (1992) Serum-soluble interleukin-2 receptors in B-cell lymphoproliferative malignancies. Med Pediatr Oncol 20(1):26–31
Depry JL, Vyas R, Lazarus HM, Caimi PF, Gerstenblith MR, Bordeaux JS (2015) Cutaneous malignant neoplasms in hematopoietic cell transplant recipients: a systematic review. JAMA Dermatol
Rizzo JD, Curtis RE, Socié G et al (2009) Solid cancers after allogeneic hematopoietic cell transplantation. Blood 113(5):1175–1183
Oddou S, Vey N, Viens P et al (1998) Second neoplasms following high-dose chemotherapy and autologous stem cell transplantation for malignant lymphomas: a report of six cases in a cohort of 171 patients from a single institution. Leuk Lymphoma 31(1-2):187–194
Yokota A, Ozawa S, Masanori T et al (2012) Secondary solid tumors after allogeneic hematopoietic SCT in Japan. Bone Marrow Transplant 47(1):95–100
Engels EA, Pfeiffer RM, Fraumeni JF Jr et al (2011) Spectrum of cancer risk among US solid organ transplant recipients. JAMA 306(17):1891–1901
Hartevelt MM, Bavinck JN, Kootte AM, Vermeer BJ, Vandenbroucke JP (1990) Incidence of skin cancer after renal transplantation in the Netherlands. Transplantation 49(3):506–509
Jensen P, Hansen S, Møller B et al (1999) Skin cancer in kidney and heart transplant recipients and different long-term immunosuppressive therapy regimens. J Am Acad Dermatol 402(1):177–186
Kolk A, Schuster T, Chlebowski A et al (2014) Combined SPECT/CT improves detection of initial bone invasion and determination of resection margins in squamous cell carcinoma of the head and neck compared to conventional imaging modalities. Eur J Nucl Med Mol Imaging 41(7):1363–74
Stockfleth E, Nindl I, Sterry W, Ulrich C, Schmook T, Meyer T (2004) Human papillomaviruses in transplant-associated skin cancers. Dermatol Surg 30(4 Pt 2):604–9
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study had IRB approval from John Peter Smith Hospital.
Conflict of interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Kadakia, S., Ducic, Y., Marra, D. et al. Cutaneous squamous cell carcinoma of the scalp in the immunocompromised patient: review of 53 cases. Oral Maxillofac Surg 20, 171–175 (2016). https://doi.org/10.1007/s10006-016-0545-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-016-0545-6