
Abstract
Accumulating literature demonstrates that immigration detention is harmful to children. However, there is a scarcity of scientifically rigorous and reliable data about the health of children held in detention facilities. The aim of the study was to compare a community-based population of recently arrived refugee children flown into Australia, not detained, resettled in a non-urban area, with a population of children who arrived by boat seeking asylum, detained since arrival. The parent-version of the strength and difficulties questionnaire (SDQ) of children aged 4–15 years was compared in children living in the community with those held in detention. We compared 86 children who had a parent-completed SDQ performed, 38 (44%) in the community group and 48 (56%) in the detention group. The community sample had been living in Australia for 325 days, with no time in detention. The detention sample had been living in detention for a mean of 221 days. The mean age was similar for the community and detention sample at 8.4 years (P = 0.18). In the total sample, children in the detention group had significantly higher SDQ total difficulties scores than children in the community group (P < 0.0001). There was no difference between age groups (P = 0.82). The children in the detention group had, on average, an SDQ total difficulties score that was 12 points higher than children in the community group. Four of the five SDQ subscale scores indicated greater disturbance amongst children in detention (< 0.0001) compared to children living in the community. The detention group had significantly higher scores (P < 0.001) for all except Pro-social scores as compared to Australian norms for the 4–6 and 7–15 years age group. This study presents a rare opportunity to compare the wellbeing of displaced children who were detained following arrival in Australia with those settled in the Australian community since arrival. The community children’s scores approximated data from the general Australian childhood population. Children held in detention had significantly more social, emotional and behavioural difficulties than children living in the community, and at levels resembling a clinical cohort. Despite the small sample size, data restrictions and other limitations of the data, statistical significance in differences between the community and detention children is marked and arguably demonstrates the negative impact of post-arrival detention in children who are presumed to have similar levels of pre-arrival adversity. If the objective is to optimise the health and wellbeing of children seeking asylum, removal of post-arrival detention is one of the most powerful interventions available to host countries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
According to the United Nations High Commission for Refugees (UNHCR), the world is witnessing the highest level of forced population displacement on record. The estimated 65.3 million people around the world who have fled their homes include 21.3 million formally recognised as refugees by the UN. Importantly, half of all refugees are children under the age of 18 years [1]. There is a remarkable convergence in the findings of extant studies in identifying a consistent profile of risk factors for poor health and wellbeing outcomes for refugee children. These include female gender, unaccompanied child status, time held in immigration detention centres, pre-migration and/or postmigration exposure to violence, family separations, psychological morbidity amongst carers, negative school and peer experiences, perceived discrimination, parental unemployment, reduced family socio-economic status and ongoing financial stress [2,3,4,5,6,7,8,9,10]. Reducing the time held in immigration detention centres may be one of the risk factors most amenable to public health interventions, particularly in reception countries of the west.
Recipient nations have shown increasing reluctance to provide protection to those seeking asylum with restrictive immigration practices being driven by policies of so-called ‘‘humane deterrence’’, despite evidence that these policies cause harm to children and adults [11,12,13,14,15]. Relevant policies include the confinement of asylum seekers, including children, in immigration detention facilities, increased border surveillance, and the outsourcing of procedures for determining refugee status to other countries [12, 13]. The current system in Australia is that 13,000–20,000 refugees each year are resettled in the community after the processing of their protection claims by the United Nations overseas. However, asylum seekers who have not had their claims processed on arrival in Australia and who arrive by boat are routinely subject to mandatory detention, off-shore processing in remote islands and denial of permanent protection, family reunification or resettlement in Australia [16, 17]. The detention of children is not confined to Australia, the practice being applied in more than 60 countries worldwide across the spectrum of high and low income nations, making this an issue of global concern [12].
Logistic and administrative obstacles present formidable obstacles for researchers in obtaining representative samples of asylum seekers. Access to detention centres in remote settings in countries like Australia is made difficult by geographical constraints and administrative provisions that restrict information gathering and dissemination of data by researchers and health professionals. In addition, obtaining informed consent remains a complex challenge given that asylum seekers may perceive participation in research as a threat to achieving positive refugee determinations [11,12,13,14, 18,19,20,21,22]. Routine health care within immigration detention centres is largely provided by contracted medical services, reducing the incentive for employees to release health data for fear of adverse employment consequences and, in some countries, there are legal prohibitions against disclosing information [18, 20, 23, 24]. In the case of unaccompanied children, Australian law requires consent to participate in research from their legal guardian, which in this instance, is mandated to be the Minister of Immigration, the state officer who is responsible for the detention policy. As with all studies relating to traumatic stress reactions, retrospective reporting holds the inherent risks of recall bias, and the possibility of either under- or over-reporting of symptoms [14, 23].
Despite these limitations, existing research studies in the field converge to indicate that immigration detention is a cause of psychological harm to both adults and children. Studies in the peer-reviewed literature internationally, including those conducted in the UK, Europe, Canada, Japan, the USA and Australia, consistently show high rates of mental distress amongst children who have been detained [11, 13, 18, 19, 21, 23,24,25,26,27,28,29,30,31]. Well documented reactions amongst detainees include depression, anxiety, post-traumatic stress disorder (PTSD), fear and hopelessness, responses that are accompanied by impaired functioning. Rates of emotional disturbance vary between a third and four fifths of detained children across studies [11,12,13, 18,19,20, 22, 24, 25, 32]. In addition, detention has negative impacts on children’s physical health and developmental progression [11, 20, 25].
The longer the period of detention, the greater the risk of adverse mental health outcomes [14, 15, 20, 24, 33, 34]. However, even brief periods of detention may be harmful [19, 25]. Children are detained in Canadian and British detention centres for far shorter periods (mean of 43–56 days) than was the case in Australia (16–20 months) at the time of this study, and had high rates of emotional distress, behavioural difficulties, depression, anxiety, sleep problems, somatic complaints and symptoms of PTSD, even if they did not report exposure to physical violence or deprivation [15, 19, 25, 32]. Similarly, in Sweden, regarded as providing better detention standards than many other nations, detainees including children reported lower quality of life than newly settled refugees in the community [28]. This suggests that even short periods of detention under relatively ‘safe’ conditions may be damaging for asylum seeker children [19].
Including a group for comparison represents an important methodological improvement in studies examining the psychological status of detained refugee children, an approach that has been pursued in studies amongst adult asylum seekers. Robjant [21] compared levels of psychological distress in asylum seekers in the community with the same indices in detained asylum seekers and non-refugee criminal detainees. The researchers found that asylum seekers in detention had the highest scores of all three groups on depression, anxiety and PTSD symptoms. Ichikawa [27] also found that ex-detained adult asylum seekers had higher levels of emotional disturbance once released than their refugee counterparts who had never been detained. Cohen [23] found suicide and self-harm rates in asylum seekers in UK detention centres to be higher than those amongst refugees in the community and comparable to the prevalence amongst general prison populations. To date, there are no published studies comparing asylum seeker children in detention with children in the community in relation to indices of mental health and wellbeing.
These considerations prompted the present study. We recognised at the outset that there were substantial methodological constraints in comparing children in detention and in the community given that the sampling frames could not be matched precisely. Nevertheless, we included a community sample in this analysis to provide a broad yardstick of the level of mental disturbance amongst refugee children in Australia who had not been detained. Our aim was to examine whether, as hypothesised, refugee children in detention showed poorer levels of social–emotional wellbeing than their counterparts living in the community. The samples included a community-based population of refugee children who arrived by plane, were not detained, were allowed to reside in a non-urban area and followed for 2–3 years after arrival; and the index group of children who arrived by boat seeking asylum, were immediately detained and held in detention for the duration of their residency in Australia.
Methods
The two populations from which our samples were drawn are described in detail below.
Community population
Between 2009 and 2013, a population cohort of all newly arrived refugee children settled in a non-urban area were visited at home by nurses shortly after arrival in Australia, and their families were invited to participate in a prospective longitudinal study [35]. Recruited children had health and wellbeing assessments conducted at year 2 (average 13 months) and year 3 (average 31 months) post-arrival. During the specified timeframe, 228 refugee children arrived in the study region, 158 meeting the eligibility criteria (aged 6 months to 15 years), of whom 61 (39%) were recruited to the study. Fewer children were initially recruited than anticipated due to logistic difficulties (unavailability of language interpreters when needed) (n = 52;33%), families/children declining to participate (n = 24;15%), relocation out of the area (n = 13;8%), or not contactable (n = 8;5%).
Of those recruited, 43 were eligible to complete the main mental health assessment measure, the strengths and difficulties questionnaire (SDQ—described below) (for ages 4–15 years) and parents completed the parent-report version in 38 of 43 (88%) children at year 2 of follow-up. Face-to-face interpreters were used during all assessment interviews; translated versions of the SDQ were used for literate Arabic and Farsi speaking participants. SDQ scores in the study children were compared to Australian normative data.
The community sample consisted of 48% male and 52% female children. Children’s families originated from the South East Asian (29%), African (20%) and Eastern Mediterranean (13%) World Health Organization (WHO) designated regions. On arrival, 30% of children were living in single-parent families. Other population characteristics, physical and developmental health and predictors of social–emotional wellbeing are described elsewhere [35,36,37]. The children retained in the study (85%) over 2–3 years were similar to those not recruited and lost to follow-up in terms of gender, WHO region of origin and language spoken at home [35].
Detention population
Data for detained children were collected in March 2014 during the Australian Human Rights Commission (AHRC) National Inquiry into Children in Immigration Detention [38]. Some of the authors (KZ and SM) were invited as consultants to the AHRC Inquiry and were involved in the design of the inquiry methodology including selection of the SDQ and other indices of data collected during the visit to Christmas Island. The data collected were later obtained for analysis under Freedom of Information (FOI) legislation in July 2015; the main findings have been published elsewhere [18]. At the time, 356 children aged 0–17 years were held in detention on Christmas Island, a remote Indian Ocean island which forms part of Australia situated off the northwest coast of the mainland. The AHRC provided data relating to 365 people under FOI, which included adults and children in 69 family groups (at least one adult and one child) with 37% of children in single-parent families; 29% had two parents and 4% were with other adult carers. The number of children ranged from one to six per family, with 40% of families having one or two children. The 191 children in the dataset represent 48% of the 356 children detained at the time on Christmas Island. Time in detention and ages of children were provided for most children. Information concerning gender, individual country of origin, and language group of child was redacted to protect participants and therefore are not available for analysis. However, accessible data indicate that the whole population of children in detention at the time (1089 children) were of Eastern Mediterranean (50%), South East Asian (18%), Western Pacific (12%), African (< 1%) and ‘Stateless’ (19%) origin. Complete SDQ data were available for 70 children (20%) aged 3–17. The English language parent-report version of the SDQ was completed during interview with parents and children using face-to-face interpreters.
Inclusion criteria for the study sample
In order to increase comparability of the two populations, we selected children aged 4–15 years. This meant exclusion of SDQ data for children under 4 and aged 16–17 years from the detention sample, reducing the detention sample from 70 to 48 children. We compared the year 2 SDQ assessment of the community sample with the SDQ assessments of the detention sample.
Measures
The SDQ was selected as a tool with high sensitivity and specificity and validated in past studies for assessing social–emotional wellbeing across cultures and in migrant and refugee children [39,40,41,42]. It includes 25 items with five symptom scales (Hyperactivity–inattention, Emotional symptoms, Peer problems, Conduct problems and Pro-social behaviour), all of which except the Pro-social subscale were used to produce the total difficulties score; the impact supplement was not used [43]. Psychometric studies have attested to the robustness of the measure for diverse populations around the world including Australia [41]. Means and standard deviations for each subscale and total difficulties scores are available for the Australian population [43]. In population and clinical studies, high SDQ scores are routinely used to indicate increased risk of mental illness [39, 40].
Statistical methods
The SDQ total difficulties score was calculated using the usual procedure which includes four subscales but not Pro-social subscale. Depending on the analysis, the SDQ total difficulties score was treated as either a continuous variable, or categorised into: (1) normal and (2) borderline and abnormal. Categorical data were described according to frequencies and percentages and differences in these indices between community and detention children were examined using contingency tables with Pearson’s Chi-square. Test statistics are reported with degrees of freedom (DF). Two-way analysis of variance was used to examine differences in mean SDQ total difficulties scores between age groups and community and detention children with least significant difference post hoc tests used to generate mean differences and 95% confidence intervals (95% CI). Independent sample t tests were used to compare the mean values of the SDQ domains between the community and detention samples with non-parametric Mann–Whitney U tests used to validate P values where the data were non-normally distributed. Two-tailed tests were used and P values < 0.05 were considered statistically significant. Study data were compared with normative Australian data for the SDQ [43,44,45]. Data were analysed using SPSS version 22.0 [IBM, USA].
Results
The study sample comprised a total of 86 children aged 4–15 years who had a completed SDQ, 38 (44%) of whom were in the community group and 48 (56%) in the detention group (Fig. 1).

Formation of study sample (n = 86)
Time in the community or in detention
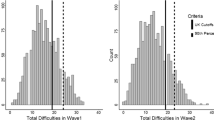
The community sample had lived in the community since arrival in Australia for an average of 325 days (11 months; range 161–727 days or 5–24 months). Of the children in the detention sample, only 29 (60%) had time in detention data, with a mean stay of 221 days (7 months) in detention (range 90–390 days or 3–13 months) (Fig. 2). This was not significantly different from the mean length of time that the total population of children aged 0–17 years had spent in immigration detention on Christmas Island (222 days), or the population of children detained elsewhere in Australia at that time, which was 231 days [38, 46].

Number and distribution of days in the community and in detention for the community sample (n = 38; mean = 325 days) and the detention sample (n = 29; mean = 221)
The sample of children in the community had resided for a longer period in Australia than those in detention, with a mean difference of 104 days (95% CI 61, 149; P < 0.0001).
Age distribution
Although the detention sample included a lower percentage of pre-school children, the overall age profile for the community and detention sample was similar (P = 0.18), with a mean of 8.4 years (Table 1).
SDQ scores
For the total samples and all age bands within them, children in the detention group had significantly higher SDQ total difficulties scores than children in the community group (F = 66.9; P < 0.0001) (Table 2). Specifically, the children in the detention group had an average SDQ total difficulties score that was 12 points higher than the average for children in the community group. Analysis of variance showed a significant difference between the two groups (P < 0.0001). As can be seen, there was no overlap in mean SDQ total difficulties scores with 95% CIs by age group in the two groups (Fig. 3). There was also no difference in SDQ total scores between groups according to age bands (P = 0.82).

Mean SDQ total difficulties scores in children living in the community and children living in detention, by age group
In addition to the mean SDQ total difficulties scores, four of the five subscale scores indicated greater levels of disturbance amongst children in detention compared to children living in the community (P < 0.0001) (Table 3). The community children’s scores on SDQ subscales approximated data from the general Australian childhood population, where rates of mental disorder are between 9 and 14% [44, 45].
The detention group had significantly higher scores (P < 0.001) for all except for the Pro-social scale when compared to Australian norms for the 4–6 and 7–15 year age group [43,44,45, 47] (Table 4).
Represented graphically, the most striking differences are evident in Emotional problems and total difficulties (Fig. 4).

Mean and 95% CI of each SDQ total difficulties (full band) and subscale score in the community and detention group
Considering the proportion of children in the abnormal, borderline and normal range of SDQ scores, a higher proportion of detention children had abnormal total difficulties scores (54.2 vs. 13.2%) and a small proportion normal scores (20.8 vs. 76.3%) (P < 0.0001) (Table 5). For all subscale scores except Peer Relations, detention children had a higher proportion with abnormal and borderline scores and a lower proportion with normal scores (P < 0.05). For Peer Relations, a higher proportion of community children had abnormal (21.1 vs. 18.8%) but also normal scores (63.2 vs. 37.5%), and lower borderline scores (15.8 vs. 43.8%).
The difference between community and detention children’s subscale scores is most striking for Emotional, Hyperactivity and Conduct Disorder subscales, where the difference between the proportion normal between the two groups is 55, 39 and 30%, respectively. The least difference is in Peer relations, at 26% difference. All differences between the two groups are statistically significant (P < 0.05).
In the 29 (60%) detained children with available data, there was no correlation between SDQ scores and days in detention (r = 0.004; P = 0.98) for SDQ total difficulties score.
Discussion
This study presents a rare opportunity to compare the wellbeing of asylum seeker children living in detention and refugee children living in the community since arrival in Australia. Children in the detention group had significantly impaired social–emotional wellbeing represented by higher SDQ total difficulties scores than children in the community group, both in the respective samples as a whole and across all age groups. The social–emotional wellbeing of community refugee children approximated Australian normative data [43, 45] and were similar to findings amongst 530 refugee children and adolescents living in the South Australian community [47, 48]. Consistent with existing evidence about the harms caused by immigration detention, over half the children living in detention had SDQ scores significantly in excess of the normal range for the total difficulties score and four of the five SDQ subscales across all age groups. The detention children in our study also had a higher proportion of abnormal SDQ total scores (54%) compared with asylum seeking children detained in open centres in Denmark (31%) [49] and the Netherlands (38%) [50].
The SDQ subscale scores were significantly worse for detention children compared to community children for all except the Pro-social subscale. The subscale scores demonstrated greatest difficulties for detained children in the domains of Emotional problems, Hyperactivity and Conduct Disorder. This distribution of problems resonates with other studies of detained children [49]. SDQ measurement of Emotional problems (indicated by the child often complaining of headaches, and being fearful, unhappy and nervous in new situations), Hyperactivity (restless, easily distracted and impulsive with difficulties concentrating) and Conduct Disorder (easily angered, disobedient, fights with other children, and often lies, cheats and steals) indicates that children are significantly symptomatic across multiple domains of functioning, consistent with clinical observations and other studies of detained children [11,12,13, 18,19,20, 22, 24, 25, 32].
For both our community sample and the South Australian refugee children, scores on Peer Relations were relatively more problematic than in the detention children [48]. The Peer Relations subscale includes indicators that the child has few friends, is bullied and gets on better with adults than same aged peers. This may reflect conditions in the community where refugee children experience difficulties integrating into mainstream society in their first year of settlement. Other studies have shown that this initial impediment improves over time and is no longer problematic by the third year of settlement [36].
The only subscale in which detention children had better mean scores than community children was the Pro-social subscale. This measures whether the child is considerate of other people’s feelings, shares readily with others, is helpful if someone is hurt, kind to younger children and volunteers to help others. Increases in Pro-social scores have been found in studies of children of parents with mental illness in the general community [51]. It is well documented that there are high rates of mental illness and psychological distress in adults living in detention [15, 18, 20, 23, 51]. We hypothesise that Pro-social skills may be required for survival and wellbeing in children living in difficult circumstances, especially if the adults around them are not able to adequately respond to their needs. As these children were living in close proximity to similarly detained children from comparable circumstances and with whom they could potentially identify, their capacity for kindness to other children may have been promoted and reflected in the Pro-social score. They also may have had reduced exposure to the lack of belonging, discrimination, bullying or exclusion that some refugee children encounter when first settled in the community [36]. Our finding of better mean Pro-social scores for detained children also indicates that there was not uniform reporting of abnormal adjustment, or “plaintive” bias, in response to the SDQ for the detention group.
The total difficulties score on the SDQ is likely to be more accurate and replicable than subscale scores, especially when comparing different ethnic groups [52, 53]. This study found that worse social–emotional wellbeing in children in detention was consistent whether total difficulties scores or subscale scores were considered. Despite the small sample size and other limitations of the data, differences between the community and detention children were substantial and statistically significant, suggesting the negative impact that post-arrival detention has amongst children who are presumed to have similar exposure to pre-arrival adversity.
An important risk factor for poor social–emotional wellbeing is unaccompanied child status [2,3,4,5,6,7,8,9,10, 54]. Of the 15 unaccompanied children in the detention population, only one was 14 years of age and therefore eligible for inclusion in this study (age range of 4–15 years). The remaining unaccompanied children were 16–17 years of age and were therefore excluded; however, analysis of their SDQ data showed that the older unaccompanied children had the same distribution of total difficulties scores on the SDQ as the rest of the detained sample population.
Limitations
This study has limitations for reasons that were largely unavoidable. Data from the detention sample were cross-sectional, preventing longitudinal analysis which has been possible in the community sample. Because of constraints on assessment and in data release, insufficient information was available to exclude differences in the pre-arrival adversities experienced by the two groups of children, although they are assumed to have faced similar levels of adversity in their countries of origin. The refugee children settled in the community had not experienced the boat journey to Australia that preceded arrival of the detained children. Previous reports indicate that detained children on Christmas Island remained distressed by transit experiences including the boat journey [55, 56]. Conversely, however, the children processed by the UN, flown to Australia and settled in the community are likely to have had longer periods of transit in refugee camps outside Australia while their refugee claims were processed.
The community children had been living in the Australian community longer than the detention children had been detained, with a mean difference of 104 days (3½ months). The higher level of social–emotional wellbeing identified in community children may be a reflection of their longer stay outside of countries of transit and origin. Other studies show that the longer displaced children are in the community in Australia or other host countries, the more their social–emotional wellbeing approximates local norms [36]. However, it is implausible that this difference adequately explains the marked disparity in SDQ scores. Unfortunately, no published literature was identified that would allow a direct comparison between displaced children resettled in the community with the precise post-arrival time period of the detention children in our study.
In the detained children there was no correlation between social–emotional distress (SDQ total score) and time detained despite evidence of an association in other studies [14, 15, 20, 24, 33, 34]. This is most likely due the small sample size of 29 children included in this analysis.
Restricted access to the detained population required that data collection was opportunistic and occurred during a brief period when the authors visited Christmas Island as part of the Australian Human Rights Commission Inquiry in 2014 [38]. The data provided for analysis under Freedom of Information provisions were heavily redacted and excluded data on gender, countries of origin, language group and other factors such as family separation and parental mental health that are known to impact on children’s social–emotional wellbeing [2, 4,5,6,7,8,9,10, 18, 57,58,59,60,61,62,63]. Differences in these characteristics could have accounted in part for the disparity in SDQ scores found between the two samples. For example, in the community sample, although not associated with gender, the SDQ score was related to the presence of the child’s father [37]. Notwithstanding the proportion of single-parent families was similar between the community and detention groups. The detention sample comprised a proportionately higher number from the Eastern Mediterranean region and lower proportions from the African region. Origin from the latter region is known to be associated with lower levels of distress amongst children in general, although the literature on the impact of region of origin is inconsistent [4, 7, 8, 37]. In spite of these caveats, the magnitude of the SDQ differences strongly suggests that detention remained a major factor shaping distress amongst children in that setting.
Although the use of a self-report instrument such as the SDQ provides information directly from the parent, and arguably provides a more accurate indication of distress than clinician-rated screening tools, distortions in reporting still may occur in cross-cultural settings arising from differences in understanding underlying concepts of health and illness; fears of mental health stigmatisation; social desirability effects; and levels of literacy [64,65,66]. The difference in cultural mix of the two samples may have influenced the extent to which these biases were operating in each group.
Levels of distress in parents and children in the detention or community sample may have influenced participation in data collection in either direction, such as inclusion of more children with poor social–emotional wellbeing in one or other sample. Without additional data on the detention population it is difficult to ascertain the extent of that potential bias. The community sample was less likely to be biased in that the study was prospectively designed to include all newly arrived refugee children in a specified geographic location and, to a large extent, achieved this aim [35]. In addition, the recruitment rate was higher in that sample. At minimum, the observation that SDQ total difficulties scores amongst the detention sample (79%) approached the prevalence found in a child and adolescent mental health service (85%) suggests that in at least a substantial subgroup residing in detention, high levels of psychopathology are present [62].
Despite the acknowledged limitations, this study is significant in that it is the first in Australia and possibly worldwide to compare the social and emotional wellbeing of displaced children settled in the community with those detained on arrival in a country of resettlement. The findings are consistent with and add to the evidence of the harms caused by post-arrival detention of displaced children, an issue of substantial public health and human rights interest considering the policies of deterrence pursued by the Australian and other governments worldwide. The Australian Human Rights Commission National Inquiry into Children in Immigration Detention [38] found detention centres to be unsafe places for children, with unacceptable risk of sexual assault, self-harm and suicide, and the stresses of confinement being instrumental in acts of voluntary starvation and hunger strikes in children. Unaccompanied children are consistently identified as a particularly vulnerable group [20, 55, 67]. In spite of the methodological challenges in undertaking studies in this area, the public interest imperative to do so therefore is clear.
Medical professionals in Australia who speak publicly about their experiences working with children in detention were, until a recent legal challenge, subject to potential imprisonment under the Australian Border Force Act of 2015; the “secrecy and disclosure provisions” of these laws remain operational for other professionals including lawyers, teachers, social workers and detention officers. (https://www.legislation.gov.au/Details/C2016C00650) [11, 18, 68,69,70]. This has led to sustained opposition from a wide range of professional organisations in Australia, the only country where mandatory detention is enshrined in legislation [16, 20, 26, 69, 71, 72]. Professional allegations that detention is tantamount to torture and a 2013 survey showing that over 80% of Australian paediatricians consider that mandatory detention of children constitutes child abuse have failed to alter Australian government policy [20, 69, 73, 74].
Given the present findings, there is a case for ensuring that the same or higher standards are provided in immigration detention centres compared to prisons in relation to accountability of governance structures, quality and independence of health care, access to services, and meaningful activity for children including education [23, 32]. The imperative of such a comprehensive duty of care is magnified for children, given that they have committed no crime and are amongst the most vulnerable and traumatised of our global population.
Conclusions
Australian and international policies increasingly subject displaced children to immigration detention. There are formidable restrictions to undertaking independent research and analysis of the health and human rights impacts of these policies. In this context, the present study adds to the growing body of data concerning the mental health impacts of detention by comparing the social–emotional wellbeing of asylum seeker children living in detention and refugee children living in the Australian community since arrival. Children in detention have markedly worse social–emotional wellbeing at all ages than their community-based counterparts. The detained children’s scores resemble a clinical sample of children referred to child and adolescent mental health services while the community-based children resemble Australian community norms. The difference between the two groups of children is significant at a statistical level in spite of the modest sample sizes. When considered in the context of past observations by professionals and human rights groups and the body of scientific research already accrued, our findings add to the case that detention itself most likely contributes to the high levels of social–emotional distress experienced by children held in detention. Clearly, if the overriding objective is to safeguard and promote the health and wellbeing of children seeking asylum, removal of detention provisions may be one of the most powerful interventions available to host countries.
References
UNHRC (2017) United Nation Refugee Agency. Figures at a glance http://www.unhcr.org/figures-at-a-glance.html. Accessed 17 May 2017
Measham T, Guzder J, Rousseau C, Nadeau L (2014) Refugee children and their families: supporting psychological wellbeing and positive adaptation following migration. Curr Probl Pediatr Adolesc Health Care 44(7):208–215
Edge S, Newbold B (2013) Discrimination and the health of immigrants and refugees: exploring Canada’s evidence base and directions for future research in newcomer receiving countries. J Immigr Minor Health 15(1):141–148
Fazel M, Reed RV, Panter-Brick C, Stein A (2012) Mental health of displaced and refugee children resettled in high-income countries: risk and protective factors. Lancet 379:266–282
Warfa N, Curtis S, Watters C, Carswell K, Ingleby D, Bhui K (2012) Migration experiences, employment status and psychological distress among Somali immigrants: a mixed-method international study. BMC Public Health 12:749. https://doi.org/10.1186/1471-2458-12-749
Sanders-Phillips K, Settles-Reaves B, Walker D, Brownlow J (2009) Social inequality and racial discrimination: risk factors for health disparities in children of color. Pediatrics 124(Suppl 3):S176–S186
Montgomery E (2008) Long-term effects of organized violence on young Middle Eastern refugees’ mental health. Soc Sci Med 67:1596–1603. https://doi.org/10.1016/j.socscimed.2008.07.020
Porter M, Haslam N (2005) Pre-displacement and post-displacement factors associated with mental health of refugees and internally displaced persons: a meta-analysis. JAMA 294(5):602–612. https://doi.org/10.1001/jama.294.5.602
Hjern A, Angel B (2000) Organized violence and mental health of refugee children in exile: a 6-year follow-up. Acta Paediatr 89(6):722–727
Almqvist K, Broberg AG (1999) Mental health and social adjustment in young refugee children 3½ years after their arrival in Sweden. J Am Acad Child Adolesc Psychiatry 38(6):723–730
Mares S (2016) Fifteen years of detaining children who seek asylum in Australia—evidence and consequences. Australas Psychiatry 24(1):11–14
Fazel M, Karunakara U, Newnham EA (2014) Detention, denial, and death: migration hazards for refugee children. Lancet Glob Health 2(6):e313–e314
Dudley M, Steel Z, Mares S, Newman L (2012) Children and young people in immigration detention. Curr Opin Psychiatry 25(4):285–292
Robjant K, Hassan R, Katona C (2009) Mental health implications of detaining asylum seekers: systematic review. Br J Psychiatry 194(4):306–312
Newman L, Steel Z (2008) The child asylum seeker: psychological and developmental impact of immigration detention. Child Adolesc Psychiatr Clin N Am 17(3):665–683
Royal Australasian College of Physicians (2017) https://www.racp.edu.au/advocacy/policy-and-advocacy-priorities/refugee-and-asylum-seeker-health. Accessed 17 May 2017
Zwi K, Chaney G (2013) Refugee children: rights and wrongs. J Paediatr Child Health 49:87–93. https://doi.org/10.1111/jpc.12101
Mares S (2016) The mental health of children and parents detained on Christmas Island: secondary analysis of an Australian human rights commission data set. Health Hum Rights 18(2):219–232
Kronick R, Rousseau C, Cleveland J (2015) Asylum-seeking children’s experiences of detention in Canada: a qualitative study. Am J Orthopsychiatr 85(3):287–294
Paxton G, Tosif S, Graham H, Smith A, Reveley C, Standish J, McCloskey K, Ferguson G, Isaacs D, Gunasekera H, Marais B, Britton P, Khatami A, Zwi K, Raman S, Elliot E, Levitt D, Francis J, Bauert P, Morris P, Whybourne A, Cherian S, Mutch R, Forbes D, Rutherford D, Packer S (2015) Perspective: the forgotten children: national inquiry into children in immigration detention (2014). J Paediatr Child Health 51(4):365–368
Robjant K, Robbins I, Senior V (2009) Psychological distress amongst immigration detainees: a cross-sectional questionnaire study. Br J Clin Psychol 48:275–286
Steel Z, Silove D (2004) Science and the common good: indefinite, non-reviewable mandatory detention of asylum seekers and the research imperative. Monash Bioeth Rev 23(4):93–103
Cohen J (2008) Safe in our hands?: a study of suicide and self-harm in asylum seekers. J Forensic Leg Med 15(4):235–244
Young P, Gordon M (2016) Mental health screening in immigration detention: a fresh look at Australian government data. Australas Psychiatry 24(1):19–22
Lorek A, Ehntholt K, Nesbitt A, Wey E, Githinji C, Rossor E, Wickramasinghe R (2009) The mental and physical health difficulties of children held within a British immigration detention center: a pilot study. Child Abuse Negl 33(9):573–585
Cleveland J, Rousseau C (2012) Mental health impact of detention and temporary status for refugee claimants under Bill C-31. CMAJ 184(15):1663–1664
Ichikawa M, Nakahara S, Wakai S (2006) Effect of post-migration detention on mental health among Afghan asylum seekers in Japan. Aust N Z J Psychiatry 40(4):341–346
Puthoopparambil S, Bjerneld M, Kallestal C (2015) Quality of life among immigrants in Swedish immigration detention centres: a cross-sectional questionnaire study. Glob Health Action 8:28321
Graf M, Wermuth P, Hafeli D, Weisert A, Reagu S, Pfluger M, Taylor P, Dittmann V, Jones R (2013) Prevalence of mental disorders among detained asylum seekers in deportation arrest in Switzerland and validation of the Brief Jail Mental Health Screen BJMHS. Int J Law Psychiatry 36(3–4):201–206
Hodes M (2010) The mental health of detained asylum seeking children. Eur Child Adolesc Psychiatry 19(7):621–623
Shields L, Stathis S, Mohay H, van Haeringen A, Williams H, Wood D, Bennett E (2004) The health of children in immigration detention: how does Australia compare? Aust N Z J Public Health 28(6):513–519
Mares S, Jureidini J (2004) Psychiatric assessment of children and families in immigration detention—clinical, administrative and ethical issues. Aust N Z J Public Health 28(6):520–526
Green J, Eagar K (2010) The health of people in Australian immigration detention centres. MJA 192(2):65–70
Steel Z, Silove D (2000) The mental health implications of detaining asylum seekers. MJA 175(11–12):596–599
Zwi K, Rungan S, Woolfenden S, Williams K, Woodland L (2016) Methods for a longitudinal cohort of refugee children in a regional community in Australia. BMJ Open 6:e011387
Zwi K, Rungan S, Woolfenden S, Woodland L, Palasanthiran P, Williams K (2017) Refugee children and their health, development and well-being over the first year of settlement: a longitudinal study. J Paediatr Child Health. https://doi.org/10.1111/jpc.13551
Zwi K, Woolfenden S, Williams K, Rungan S, Woodland L, Jaffe A (2017) Protective factors for social-emotional well-being of refugee children in the first 3 years of settlement in Australia. Arch Dis Child. https://doi.org/10.1136/archdischild-2016-312495
Australian Human Rights Commission (2015) The forgotten children: national inquiry into children in immigration detention 2014. ISBN 978-1-921449-56-7
Goodman R (2001) Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry 40(11):1337–1345
Vostanis P (2006) Strengths and difficulties questionnaire: research and clinical applications. Curr Opin Psychiatry 19(4):367–372
Achenbach TM, Becker A, Döpfner M, Heiervang E, Roessner V, Steinhausen HC, Rothenberger A (2008) Multicultural assessment of child and adolescent psychopathology with ASEBA and SDQ instruments: research findings, applications, and future directions. J Child Psychol Psychiatry 49(3):251–275
Leavey G, Hollins K, King MB, Grayson K (2004) Psychological disorder amongst refugee and migrant schoolchildren in London. Soc Psychiatry Psychiatr Epidemiol 39(3):191–195
Youthinmind (2017) Strengths and difficulties questionnaire: normative SDQ data from Australia. http://www.sdqinfo.com/norms/AusNorm.html. Accessed 17 May 2017
Mellor D (2005) Normative data for the strengths and difficulties questionnaire in Australia. Aust Psychol 40(3):215–222
Sawyer MG, Arney FM, Baghurst PA, Clark JJ, Graetz BW, Kosky RJ, Nurcombe B, Patton GC, Prior MR, Raphael B, Rey JM, Whaites LC, Zubrick SR (2001) The mental health of young people in Australia: key findings from the child and adolescent component of the national survey of mental health and well-being. Aust New Z J Psychiatry 35(6):806–814
Australian Human Rights Commission (2014) Handout for hearing: National Inquiry into Children in Immigration Detention 2014. https://www.humanrights.gov.au/our-work/asylum-seekers-and-refugees/national-inquiry-children-immigration-detention-2014/handout. Accessed 12 May 2017
Kremer P, de Silva A, Cleary J, Santoro G, Weston K, Steele E, Nolan T, Waters E (2015) Normative data for the strengths and difficulties questionnaire for young children in Australia. J Paediatr Child Health 51(10):970–975. https://doi.org/10.1111/jpc.12897
Ziaian T, Anstiss H, Antoniou G, Baghurst P, Sawyer M (2011) Emotional and Behavioural Problems Among Refugee Children and Adolescents Living in South Australia. Aust Psychol. https://doi.org/10.1111/j.1742-9544.2011.00050.x
Nielsen S, Norredam M, Christiansen K, Obel C, Hilden J, Krasnik A (2008) Mental Health Among children seeking asylum in Denmark—the effect of length of stay and number of relocations: a cross sectional study. BMC Public Health 8:293
Wiegersma PA, Stellinga-Boelen A, Reijneveld SA (2011) Psychosocial problems in asylum seekers’ children: the parent, child, and teacher perspective using the strengths and difficulties questionnaire. J Nerv Ment Dis 199:85–90
Maybery D, Reupert A, Goodyear M, Ritchie R, Brann P (2009) Investigating the strengths and difficulties of children from families with a parental mental illness. Aust E J Adv Mental Health 8(2):165–174
Richter J, Sagatun Å, Heyerdahl S, Oppedal B, Røysamb E (2011) The strengths and difficulties questionnaire (SDQ)—self-report. An analysis of its structure in a multiethnic urban adolescent sample. J Child Psychol Psychiatry 52:1002–1011
Mieloo CL, Bevaart F, Donker MC, van Oort FV, Raat H, Jansen W (2014) Validation of the SDQ in a multi-ethnic population of young children. Eur J Public Health 24(1):26–32
Derluyn I, Broekaer E (2007) Different perspectives on emotional and behavioural problems in unaccompanied refugee children and adolescents. Ethn Health 12:141–162
Zwi K, Mares S (2015) Stories from unaccompanied children in immigration detention: a composite account. J Paediatr Child Health 51(7):658–662. https://doi.org/10.1111/jpc.12953
Mares S, Zwi K (2015) Sadness and fear: the experiences of children and families in remote Australian immigration detention. J Paediatr Child Health 51:663–669
Lovejoy MC, Graczyk PA, O’Hare E, Neuman G (2000) Maternal depression and parenting behavior: a meta-analytic review. Clin Psychol Rev 20(5):561–592
Murray L, Halligan SL, Cooper PJ (2010) Effects of postnatal depression on mother–infant interactions, and child development. In: Wachs T, Bremner G (eds) Handbook of infant development. Wiley-Blackwell, Malden
Murray L, Arteche A, Fearon P, Halligan S, Goodyer I, Cooper P (2011) Maternal postnatal depression and the development of depression in offspring up to 16 years of age. J Am Acad Child Adolesc Psychiatry 50(5):460–470
Cunningham J, Harris G, Vostanis P, Oyebode F, Blissett J (2004) Children of mothers with mental illness: attachment, emotional and behavioural problems. Early Child Dev Care 174(7–8):639–650
Cowling V, Luk E, Mileshkin C, Birleson P (2004) Children of adults with severe mental illness: mental health, help seeking and service use. Psychiatr Bull 28:43–46
Mathai J, Jespersen S, Bourne A, Donegan T, Akinbiyi A, Gray K (2008) Use of the strengths and difficulties questionnaire in identifying emotional and behavioural problems in children of parents with a mental illness in Australia. Aust E J Adv Mental Health. https://doi.org/10.5172/jamh.7.3.200
Najman JM, Williams GM, Nikles JMB, Spence S, Bor W, O’Callaghan M, LeBrocque R, Andersen MJ (2000) Mothers’ mental illness and child behaviour problems: cause-effect association or observation bias? J Am Acad Child Adolesc Psychiatry 39:592–602
Bronstein I, Montgomery P (2011) Psychological distress in refugee children: a systematic review. Clin Child Fam Psychol Rev 14:44–56
Kersten P, Dudley M, Nayar S, Elder H, Robertson H, Tauroa R, McPherson KM (2016) Cross-cultural acceptability and utility of the strengths and difficulties questionnaire: views of families. BMC Psychiatry 16:347
Zwi K, Kalowski J, Parmeter J, Woodland L (2017) The impact of health perceptions and beliefs on access to care for migrants and refugees. J Cult Divers 24(3):63–72
Hodes M, Jagdev D, Chandra N, Cunniff A (2008) Risk and resilience for psychological distress amongst unaccompanied asylum seeking adolescents. J Child Psychol Psychiatry 49(7):723–732
Dudley M (2016) Helping professionals and Border Force secrecy: effective asylum-seeker healthcare requires independence from callous policies. Aust Psychiatry 24(1):5–18
Isaacs D (2015) Nauru and detention of children. J Paediatr Child Health 51(4):353–354
Booth A (2016) Health workers exempt from immigration detention secrecy provisions, SBS News. http://www.sbs.com.au/news/article/2016/10/20/government-lifts-gag-doctors-over-speaking-out-asylum-seeker-treatment. Accessed 12 May 2017
Talley N, Zwi K (2015) Let the children go—advocacy for children in detention by the Royal Australasian College of Physicians. MJA 202(11):555–557
Triggs G (2015) The forgotten children: national inquiry into children in immigration detention 2014. MJA 202(11):553–555
Isaacs D (2016) Are healthcare professionals working in Australia’s immigration detention centres condoning torture? J Med Ethics 42:413–415
Corbett EJ, Gunasekera H, Maycock A, Isaacs D (2014) Australia’s treatment of refugee and asylum seeker children: the views of Australian paediatricians. MJA 201(7):393–398
Acknowledgements
The authors acknowledge participating families and children involved in the community study, Refugee Health Nurses Jenny Lane, Colleen Allen and Lisa Atkins, and Statistician Jenny Peat. The analysis of the detention sample is possible because the Australian Human Rights Commission (AHRC) collected the primary data from families seeking asylum and detained on Christmas Island. This was subsequently released under Freedom of Information legislation (FOI). Any errors or omissions are the sole responsibility of the authors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors received no financial support for the research, authorship, and/or publication of this article and have no conflict of interest.
Funding
The community study was funded by Financial Markets Foundation for Children (AUD$158 000 July 2009–June 2011). The funders had no involvement in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Ethics
The research involving the community sample in this study and the comparison with the detention sample was granted by the Human Research Ethics Committee Northern Hospitals Network, South Eastern Sydney (SES) Illawarra Area Health Service/SES Local Health District (HREC Ref No 09/163). The research involving the detention sample in this study was assessed by the South Western Sydney Local Health District Human Research Ethics Committee (HREC/15/LPOOL/556), which was satisfied with provisions to protect the rights of participants. All participants gave their informed consent prior to their inclusion in the study.
Additional information
This article is part of the focused issue ‘Mental health issues in refugees’.
Rights and permissions
About this article

Cite this article
Zwi, K., Mares, S., Nathanson, D. et al. The impact of detention on the social–emotional wellbeing of children seeking asylum: a comparison with community-based children. Eur Child Adolesc Psychiatry 27, 411–422 (2018). https://doi.org/10.1007/s00787-017-1082-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-017-1082-z