
Abstract
Background
The World Health Organization considers malocclusion one of the most essential oral health problems. This disease influences various aspects of patients’ health and well-being. Therefore, making it easier and more accurate to understand and diagnose patients with skeletal malocclusions is necessary.
Objectives
The main aim of this research was the establishment of machine learning models to correctly classify individual Arab patients, being citizens of Israel, as skeletal class II or III. Secondary outcomes of the study included comparing cephalometric parameters between patients with skeletal class II and III and between age and gender-specific subgroups, an analysis of the correlation of various cephalometric variables, and principal component analysis in skeletal class diagnosis.
Methods
This quantitative, observational study is based on data from the Orthodontic Center, Jatt, Israel. The experimental data consisted of the coded records of 502 Arab patients diagnosed as Class II or III according to the Calculated_ANB. This parameter was defined as the difference between the measured ANB angle and the individualized ANB of Panagiotidis and Witt. In this observational study, we focused on the primary aim, i.e., the establishment of machine learning models for the correct classification of skeletal class II and III in a group of Arab orthodontic patients. For this purpose, various ML models and input data was tested after identifying the most relevant parameters by conducting a principal component analysis. As secondary outcomes this study compared the cephalometric parameters and analyzed their correlations between skeletal class II and III as well as between gender and age specific subgroups.
Results
Comparison of the two groups demonstrated significant differences between skeletal class II and class III patients. This was shown for the parameters NL-NSL angle, PFH/AFH ratio, SNA angle, SNB angle, SN-Ba angle. SN-Pg angle, and ML-NSL angle in skeletal class III patients, and for S-N (mm) in skeletal class II patients. In skeletal class II and skeletal class III patients, the results showed that the Calculated_ANB correlated well with many other cephalometric parameters. With the help of the Principal Component Analysis (PCA), it was possible to explain about 71% of the variation between the first two PCs. Finally, applying the stepwise forward Machine Learning models, it could be demonstrated that the model works only with the parameters Wits appraisal and SNB angle was able to predict the allocation of patients to either skeletal class II or III with an accuracy of 0.95, compared to a value of 0.99 when all parameters were used (“general model”).
Conclusion
There is a significant relationship between many cephalometric parameters within the different groups of gender and age. This study highlights the high accuracy and power of Wits appraisal and the SNB angle in evaluating the classification of orthodontic malocclusion.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The World Health Organization (WHO) considers malocclusion one of the most essential oral health problems after caries and periodontal disease [1, 2]. Skeletal class II malocclusion (SCIIMO) accounts for over one-third of all malocclusions worldwide and is more frequent in Caucasians [2]. In contrast, Skeletal class III malocclusion (SCIIIMO) is the least frequent, with a mean frequency of 7.2%. Reports have shown that the countries with the lowest prevalence index were Italy (1.6%), Nigeria (1.6%), and Jordan (1.4%) [3, 4]. Skeletal Class II is usually defined as a change in the relationship between the two jaw (Maxilla and Mandible) bases, with a protruded position of the upper jaw to the mandible (maxillary protrusion or maxillary prognathism) or a mandibular retrusion (mandibular retrognathism) or a combination of both situations [2, 5]. Skeletal Class III is usually defined as a change of the relationship between the two jaw (Maxilla and Mandible) bases, with the mandible protruding (mandibular prognathism) from the upper jaw or a retrusion of the upper jaw (maxillary retrognathism (midface) or a combination of both conditions [1, 3].
Previous studies defined Skeletal malocclusion as a complicated disorder produced by the combination of multiple factors, such as genetics, environment, ethnic factors, nonnutritive sucking habits, impaired nasal breathing, and functional atrophy of the maxilla [3, 6,7,8,9].
The diagnosis of skeletal deformities depends on accurate measurement of distances, planes, and angles between landmarks of hard and soft tissues using lateral cephalogram and cone-beam computed tomography (CBCT), which are then traced to assess the craniofacial relationships of the teeth to the jaws and the jaws to the rest of the facial skeleton to aid in orthodontic diagnosis [10, 11]. Many approaches are applied to diagnose skeletal malocclusion. According to Steiner [12], analysis was made by the ANB angle (SNA - SNB) for classes II and III as follows - ANB angle with values > 4° = Skeletal Class II, and ANB angle with values < 0° = Skeletal Class III.
According to Jacobson [13], the Wits appraisal and ANB angle define the relation between the two jaws, with an advantage of the ‘Wits” appraisal over that of the conventional ANB angle, with a more reliable indication of the extent or severity of anteroposterior skeletal disharmony of the jaws [13]. In the following years, various studies demonstrated equations that consider the individual properties of the ANB angle. In 1977, Panagiotidis and Witt [14] showed an equation for the individualized ANB individual as ANBind = (− 35.16 + 0.4 · SNA + 0.2 · ML-NSL). Järvinen estimated the individualized ANB by applying another formula as ANBind = (ANB − (0.472 × SNA) + (0.204 × SN-MP) − 43.386) [15], and also established a regression equation to individualize the norm of the Wits appraisal as: Wits = (1.636 × ANB – 0.512 × NSL/OL – 0.830 × SNA + 71.36) [16]. In a separate study that was done on the Chinese population, the derived equations were: ANBind = (0.42 × (SNA) + 0.31 × (SN-MP) – 41.1) for males; ANBind = (0.31 × (SNA) + 0.20 × (SN-MP) – 28.9) for females [17].
Very recently, Paddenberg et al. [18] established improved and extended regression equations for equations derived by Panagiotidis/Witt and Järvinen for the individualized ANB and Wits appraisal [18].
It is well documented that individualized ANB and Wits appraisal are considered to be more useful cephalometric parameters for diagnosing skeletal class, because they are based on individually determined norm values instead of empirical norms, representing a population’s mean value.
According to a cross-sectional study done on SCIIIMO South Korean and Spanish participants, the results of the varimax factorial analysis (VFA) and cluster analysis (CA), showed a distinct distribution of the two ethnic groups, as well as differences within the same ethnic group [19]. According to Dehesa-Santos et al., cluster 1 was predominantly Spanish, and clusters 2 and 3 were mainly South Korean, with opposite phenotypes of mandibular projection and craniofacial pattern [19]. In another study that compared the craniofacial characteristics of skeletal and dental SCIIMO traits from Indian and Vietnamese individuals, it was found that the ANB angle was significantly greater in males (+ 1.4 deg) and females (+ 1.9 deg) in South Indian individuals. In addition, this study detected differences in the plane angle, articular angle, anterior facial height, and lower anterior facial height and described that SCIIMO was more severe in South Indian compared to Vietnamese adults [20]. However, to our knowledge there is no study comparing the cephalometric parameters between different subgroups of Arab patients, presenting skeletal class II or III.
Over the last decade, artificial intelligence (AI), especially machine learning (ML), has emerged in the field of dentistry, and assists the clinicians in the processing of images as well as in treatment decisions [10]. In addition, deep learning algorithms has been applied in the cephalometric analysis, and many approaches have focused on the detection of cephalometric landmarks [21].
The non-uniformity among orthodontics regarding the definition of these landmarks, in addition to the quality of the image, leads to significantly different outcomes of landmark coordinates and geometrical parameters [10]. The most common AI fields in dentistry are classification, regression, detection, and segmentation [10]. The constraint with all the currently available equations for individualizing the ANB angle and Wits appraisal is the fact there are many different and various equations that were used.
Therefore, the primary aim of this study was to derive a new machine learning model, based on the most important parameters and results from principal component analysis, to correctly identify Palestinian Arab residents of Israel as skeletal class II or III. We intended to use various machine learning models and different input variables to detect the best fitting one. Furthermore, additional analysis were done to investigate the effect of age and gender specific subgroups. It was the null hypothesis of our study that machine-learning models without using the classic equations of Calculated_ANB, won’t be able to classify either its SCIIMO or SCIIIMO with a high accuracy.
First, we applied a general Machine Learning (ML) model that included all parameters to classify the patients. Then, after excluding the Calculated_ANB and measured ANB, the most important variables were used to conduct a stepwise machine-learning process. The machine-learning models that were performed to classify patients as SCIIMO or SCIIIMO are- Linear Discriminant Analysis (LDA), Support Vector Machine (SVM), K-Nearest Neighbors (KNN), Random Forest (RF), and classification and regression trees (CART).
Materials and methods
Ethical statement
All human samples presented in this study were assessed and treated according to current guidelines and followed the regulations of the Ethics Committee of the University of Regensburg. The committee had reviewed and approved this research project and study design with approval number 19-1596-101 (dated 13.11.2019). All patients were assessed and treated at the Orthodontic Research Center based in Jatt, Israel, and agreed to participate in this quantitative, observational study after detailed explanation by signing a corresponding consent form. The experimental data consisted of the coded records of 502 patients, who were Palestinian Arab citizens of Israel and diagnosed as skeletal class II or III. All data were collected as part of the routine orthodontic diagnostics, which had been taken for the purpose of the orthodontic treatment only. The research sample consisted of 502 patients with skeletal class II (n = 237, 47.21%) and III (n = 265, 52.78%).
The sample size was determined by the maximum number of cases, presenting skeletal class II and III, available within the period of recruitment. In addition, each machine-learning model was cross-validated to estimate its performance on unseen data in correctly classifying, and the sample size was sufficient to get the desired accuracy results.
Only orthodontic patients assessed and treated at the Orthodontic Research Center based in Jatt, Israel, were included in this study.
The inclusion criteria were, 1.Patients diagnosed with skeletal class II (Calculated_ANB > 1) or skeletal class III (Calculated_ANB<-1) according to the definition of Panagiotidis and Witt (Calculated ANB = ANB – individualized ANB of Panagiotidis and Witt [14]); and 2. Patients with pre-treatment lateral cephalograms available.
Cephalometric variables
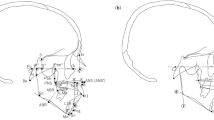
The cephalometric parameters included in this study analysis, with complete information and location, are presented in Supplementary Fig. 1A and described in Supplementary Table 1. In the present study, patients were included according to the Calculated_ANB. In fewer cases, they were included and diagnosed SCIIMO and SCIIIMO, even when they were not in the expected range of the Calculated_ANB that was proposed by Panagiotidis and Witt, but according to the orthodontist’s team clinical diagnosis, and according to other crucial parameters, like ANB angle and Wits appraisal. The fact that the Calculated_ANB doesn’t fit all cases is expected and was examined by Panagiotidis and Witt and can be explained by the correlation coefficient of the ANBind equation, r = 0.808 [14].
The mean age of skeletal class II patients was 17 (M = 17, SD = 6.5), with an age range of 7–44. Among class II patients, females constituted more than half (n = 162,68%). Concerning skeletal class III patients, the mean age of the patients was 18 (M = 18, SD = 8.1), with an age range of 6–54, and here also, females were more than half of the patients in this class (n = 140,52.83%). Supplementary Tables 2A and 2B summarize the full detailed information about the tested SCIIMO and SCIIIMO patients, respectively.
Data analysis
Data analysis was performed using the R software platform using the one-way analysis of variance tests (ANOVA). Post-hoc analysis was used to understand the differences between different subgroups of gender and age within the same and other classifications.
In addition, to understand the correlations between the different cephalometric parameters among the various (sub)groups, the Spearman Correlation was applied and visualized as a Heatmap correlation matrix. Furthermore, to estimate better our data structure and to gain thorough knowledge about the most informative and variant cephalometric parameters in our data, Principal Component Analysis (PCA) was done to identify if the information of the cephalometric parameters is well represented by the principal components chosen. We used different figures to illustrate the importance, but also the weight for each cephalometric parameter when calculating the principal component. In this study, we analyzed the first four components that explained about 92% of the variation in our data. Finally, machine-learning models were applied to examine our main hypothesis.
Machine learning methods
LDA was proposed by R. Fischer in 1936. It consists of finding the projection hyperplane that minimizes the interclass variance and maximizes the distance between the projected means of the classes [22]. The next model we used was the SVM model, which implements the following idea: input vectors are non-linearly mapped to a very high-dimension feature space. In this feature space, a linear decision surface is constructed [23]. This model can be relatively simple and flexible for addressing various classification problems. SVMs distinctively afford balanced predictive performance, even in studies where sample sizes may be limited [24]. We also applied the nearest neighbor decision (KNN) rule, which assigns to an unclassified sample point the classification of the closest of a set of previously classified points [25, 26]. This study used Accuracy to select the optimal model using the most considerable value. The final value used for the model that includes Wits appraisal only was k = 9 (9 neighbors), and k = 7 (7 neighbors) for the model that contains Wits appraisal and SNB angle. In addition, we applied RF model, which uses many decision trees. This algorithm is a combination of tree predictors such that each tree depends on the values of a random vector sampled independently and with the same distribution for all trees in the forest [27, 28]. Finally, we applied the CART model, and the data was partitioned along the predictor axes into subsets with homogeneous values of the dependent variable, a process represented by a decision tree that can be used to make predictions from new observations [29].
Classification models
Classification models - Linear Discriminant Analysis (LDA), Support Vector Machine (SVM), K Nearest Neighbor (KNN), Random Forest (RF), and Classification and Regression Tree (CART). They were all applied using the K-fold cross-validation (K = 10) implementation of the R package Caret.
Model validation
We validated our models using the k-fold cross-validation approach. Cross-validation provides a simple and effective method for both model selection and performance evaluation; under k-fold cross-validation, the data are randomly partitioned to form k-disjoint subsets of approximately equal size [30, 31]. K (10)-fold cross-validation was employed in this research. Finally, we used a separate validation set (30%) to provide a more reliable estimate of model performance on unseen data and visualized the data on a confusion matrix.
Results
Comparison of cephalometric parameters
Our observations show that there are variations in cephalometric parameters in different gender and age specific subgroups within the same skeletal malocclusion class, and between the different classes. To evaluate the effect of the potential confounders gender and age on the cephalometric measurements, we compared each group with the other groups by conducting multiple comparison tests. Table 1A and 1C show the multiple tests performed, and the adjusted p-values were obtained by Tukey test. Values were regarded as significant at p < 0.01 and p < 0.05.
Comparison of cephalometric parameters within the same skeletal class group
The results of our analyses showed that the results of skeletal class III males presented a significantly more prognathic mandible (SNB) and anterior position of the chin (SN-Pg) than females. In the vertical direction and compared to females, skeletal class III males had a more horizontal growth pattern (PFH/ AFH) and a bigger counterclockwise rotation of the maxilla (NL-NSL) and the mandible (ML-NSL) (p < 0.05) (Table 1A).
Furthermore, the analysis of skeletal class II patients revealed that adult patients (age > 21 years) presented a significant more open vertical configuration than younger ones, as evident from the divergence of the jaw bases (NL-ML) and the inclination of the mandible (ML-NSL) (p < 0.01). In line with this, the growth pattern was more vertical in adults compared to younger individuals, according to the parameters PFH/ AFH and facial axis (p < 0.05). As shown by the Gonion angle, adolescents (age 14–20) showed a more horizontal growth pattern compared to children (age 0–13), as well as more retroinclined and retropositioned upper front teeth (p < 0.05) (Table 1B).
Concerning the effect of age, among skeletal class III patients’ adults presented a more severe degree of the sagittal skeletal discrepancy (Wits appraisal) than younger ones (p < 0.05). Furthermore, the upper incisors of adults were more retroinclined (+ 1/NL, + 1/NSL) and anteriorly positioned (+ 1/NA (mm)) than in younger patients, although the interincisal angle was smaller in adults compared to adolescents and children (p < 0.05). Patients, aged 14–20 years, also had a more pronounced skeletal class III (Wits appraisal) (p < 0.05) and more retroinclined (+ 1/NL, + 1/NSL) and anteriorly positioned (+ 1/NA (mm)) upper incisors compared to children (p < 0.01) (Table 1B).
Moreover, adult females with skeletal class II presented more hyperdivergent jaw bases (NL-ML), and more posteriorly rotated mandible (ML-NSL) (p < 0.05). In line with the above-mentioned findings, according to the facial axis, these adult females with skeletal class II had a more vertical growth pattern than adolescent females (p < 0.01). Among males, the upper incisors were more retroinclined (+ 1/NA) in adolescents than in children (p < 0.05), but among females with skeletal class II, adolescents had more retroinclined lower incisors (1/ML) than children (p < 0.01). Regarding patients with skeletal class III, adult males presented a more pronounced sagittal skeletal discrepancy (Wits appraisal) than children. Furthermore, in male adolescents with skeletal class III the growth pattern (PFH/ AFH) was more horizontal than in female adolescents (p < 0.05) (Table 1C).
Variation of cephalometric parameters between patients with different skeletal classes
Our results demonstrated a large variety of significant differences when comparing different skeletal classes and subgroups of gender and age, among which the most important parameters were Gonion angle, SNB angle, ANB angle, Calculated_ANB, SN-Pg angle, and Wits appraisal (Supplementary Table 3).
Heatmaps of spearman correlation
Global heatmap correlation matrices of assessed cephalometric parameters under different classifications and sub-groups
The overall heatmap correlation matrices of cephalometric parameters in skeletal class II and III groups demonstrated many correlations between the variables. Results show a strong and significant correlation between parameters in the same dimension. In both skeletal classes, the results revealed many correlations between Calculated_ANB and other parameters. For example, among skeletal class II patients, Calculated_ANB presented significant correlations with the following skeletal variables: SNB (ρ=-0.274, P < 0.01), ANB (ρ = 0.430, P < 0.01), SN-Pg (ρ=-0.302, P < 0.01) and Wits appraisal (ρ = 0.574, P < 0.01). Regarding skeletal class III, Calculated_ANB was associated with the following skeletal parameters: Facial axis (ρ=-0.474, P < 0.01), SNB (ρ=-0.670, P < 0.01), ANB (ρ = 0.822, P < 0.01) SN-Pg (ρ=-0.644, P < 0.01), and Wits appraisal (ρ = 0.655, P < 0.01) (Fig. 1).

The heatmaps present the Spearman correlation between different cephalometric parameters for SCIIMO and SCIIIMO patients. Color coding signifies the strength and direction of the correlation: blue indicates a negative correlation (strongest at ρ = -1), red indicates a positive correlation (strongest at ρ = 1), and the intensity of the color reflects the correlation strength. This Figure shows SCIIMO and SCIIIMO correlations regardless of gender and age
Gender and age variation
The heatmaps for each subgroup revealed many specific significant correlations, although they varied between different subgroups. Detailed results are available in the supplementary Tables 2A and 2B.
Principal component analysis (PCA)
We ran a PCA analysis with all cephalometric parameters to better estimate our data structure and gain thorough knowledge about the most informative parameters in our data. After normalizing our data, the results demonstrated that the first component explains more than half of the total variance (53%) and adding three further principal components lead to a cumulative proportion of variance of 92% (Table 2A). To better understand, which components are included in the first component, the loading matrix was calculated, showing high positive values for ANB, and Calculated_ANB, and ML-NSL. Furthermore, high negative values were identified for SN-Pg, SNB, and facial axis. Variables, which had a high impact on the second component were Gonion angle, ML-NSL, and NL-ML (positive), and − 1/ML, Wits appraisal, Calculated_ANB, and PFH/AFH ratio (negative). The specific details of all parameters are represented in Table 2B.
Subsequently, we calculated the contribution of each parameter to the first four components using the cosine squared function. The results showed that the parameters SN-Pg, Calculated_ANB, ANB angle, and ML-NSL contributed the most to the first four components (Fig. 2A). Finally, as presented in Fig. 2B, we observed a similar result with a different visualization.

The results of a Principal Component Analysis (PCA) on the assessed cephalometric parameters. Figure 2A shows the contribution of each cephalometric parameter to the first four principal components (PCs) through their cosine squared values. The X-axis lists all variables, and the Y-axis shows the values of the Cos2 quality of the presentation. Variables with the highest contributions to the first four PCs are SN-ML angle, ML-NSL angle, SN-Pg angle, and PFH/AFH ratio. Figure 2B presents a PCA biplot that visualizes the relationships between the variables and the first two PCs (PC1 and PC2). PC1 captures 51.2% and PC2 captures 19.3% of the data variance. The X and Y axes represent PC1 and PC2, respectively. High contributing variables (identified in Fig. 2A) are colored green, while variables with lower contributions are shown in black. This combined analysis helps to understand how the original variables relate to the first four components and identify the most influential factors contributing to the variation in the data
Machine learning models
The main aim of this study was to establish machine learning (ML) models to increase the precision in the diagnosis of skeletal class II and III instead of applying the individualized ANB of Panagiotidis and Witt, combined with the measured ANB only. When we tested different ML models based on all parameters (general model) in the LDA and RF models, we received 0.99 accuracy (Accuracy = 0.99, Kappa = 0.99) in the classification of skeletal class II and III. Then, we analyzed the performance of ML models, which varied according to the ML-type and the amount of input parameters. We used that general model that contained all the input variables to estimate the importance of each parameter to the model, thereby determining the other models to be evaluated (Fig. 3).

Summary of the General Machine Learning model showing the importance of each parameter to the model in predicting SCIIMO or SCIIIMO. X-axis shows the prediction importance of the different assessed variables. Y-axis shows the list of the assessed variables
In the first stage, we tested an ML model using only the most important variable that followed the Calculated_ANB and measured ANB angle. Hence, the first model included the Wits appraisal only and achieved an accuracy of 0.93 (Accuracy = 0.93, Kappa = 0.86) in the CART model (Fig. 4A-B). The second model included the Wits appraisal and the SNB angle, increasing the accuracy to 0.95 in the SVM model. Finally, adding the third slightly improved the performance of the machine learning models (Table 3).

Summary of model 1 (one predictor) of the different Machine Learning models. Figure 4A presents a Summary of the five Machine-Learning classification models, including Linear Discriminant Analysis (LDA), Support Vector Machine (SVM), K-Nearest Neighbors, Random Forest (RF), Classification, and Regression Tree (CART), which are presented on the Y-axis. The X-axis shows the Accuracy and Kappa scores for each model. The first model included the Wits appraisal only; in the LDA and SVM models, we received an Accuracy of 0.90 and Kappa of 0.80, while Fig. 4B presents the LDA Machine Learning Model Confusion Matrix for Wits appraisal to predict the classification (Predicted) compared to the Actual classification, based on using this variable only. The X-axis shows the SCIIMO and SCIIIMO predictions, and the Y-axis shows the number of identified patients in each classification
The results of the machine learning models that include the first two variables (Wits appraisal and SNB angle), were satisfying in classifying patients as skeletal class II or III. The highest mean accuracy value was obtained by the models SVM, and KNN, with an accuracy of 0.95 (Kappa SVM = 0.91, Kappa KNN = 0.908). The model LDA,, and RF revealed a high accuracy of approximately 0.93 too (Accuracy = 0.93, Kappa LDA = 0.85, Kappa RF = 0.87). Finally, the CART model also had a high accuracy score of 0.91 (Accuracy = 0.91, Kappa = 0.82) (Fig. 5A).

Summary of model 2 (two predictors) of the different Machine Learning models. Figure 5A presents a summary of the five Machine-Learning classification models tested, including Linear Discriminant Analysis (LDA), Support Vector Machine (SVM), K-Nearest Neighbors, Random Forest (RF), Classification and Regression Tree (CART) as presented on the Y-axis. The X-axis shows the Accuracy and Kappa scores for each model. At the same time, Fig. 5B presents the Machine Learning Model Confusion Matrix, which shows the ability of the KNN model to predict the classification (Predicted) compared to the Actual classification based on Wits appraisal and SNB angle. The X-axis shows the SCIIMO and SCIIIMO predictions, and the Y-axis shows the number of identified patients in each classification
Finally, 30% of the recruited patients were used to validate the ML model by comparing the classification obtained by the ML model with the classification made by Calculated_ANB.70 skeletal class II patients were classified as class II both by the model and by the Calculated_ANB, 75 skeletal class III patients were classified as class III both by the model and by the Calculated_ANB. (Fig. 5B). To understand the confounding effect of gender and age, we repeated the previous model with same cephalometric parameters. We included gender and age as additional variables, and from the results, we can understand that the addition of gender and age did not improve the accuracy.
Discussion
This research’s main objective was to establish a machine learning model that accurately determines the skeletal class II or III of Arab individuals. Secondary aims included comparing cephalometric parameters and their correlations between skeletal class II and III (sub)groups. We intended to illustrate the association of vertical and sagittal cephalometric parameters to define the sagittal discrepancy of the jaw bases with high precision, improving individualized diagnostics and treatment planning in orthodontics. For this purpose, first, cephalometric parameters were compared between skeletal class II and III patients and between age and gender-specific subgroups. Then, correlations between all cephalometric variables, including Calculated_ANB, were assessed for all skeletal class II/ III patients and the different subgroups concerning age and gender. Next, following PCA to detect the most relevant parameters in skeletal class II/ III diagnosis, we finally evaluated the primary outcome, i.e., the performance of machine learning models. During this process, different ML models in terms of the kind of model and the amount of input variables were tested to identify the best fitting one. We used the Calculated_ANB, i.e., the difference between the individualized ANB of Panagiotidis and Witt and the measured ANB, as a reference test to validate the ML model and to determine its accuracy, reliability (kappa), sensitivity, and specificity. Finally, we could reject the null hypothesis, as we established an accurate machine learning model for diagnosing skeletal class II/ III and identified significant differences in cephalometric measurements between different skeletal malocclusion and age and gender-specific subgroups.
Different groups comparisons
The results showed that that there were many significant differences between gender and age specific subgroups. Although we identified some differences in cephalometric variables between subgroups of the same skeletal class, most significant differences were detected between subgroups of different skeletal classes. Many previous studies did not find that there is no significant difference between males and females [32]. For example, In research that studied the Lateral cephalograms of 105 Chinese subjects with Class II, there were no significant differences were detected between males and females for any of the parameters between males and females [32]. These results were also supported by Sharma and Xin [38],
who identified only small gender specific differences for six parameters. However, another study reported significant differences in cephalometric parameters between male and female adolescents, although variations were found for different malocclusion classes. In class II males, the maxilla was placed more protrusively (R2ANS; R2A) and the mandible was found to be larger both in the position and dimension (CoGn; R2M), whereas in class III adolescents no significant differences were detected [33]. Contrary to these findings, we did not observe any significant variation between male and female skeletal class II patients.
According to our results, age was identified to influence cephalometric measurements significantly
In summary, older patients revealed more hyperdivergent jaw bases (NL-ML), posteriorly rotated mandibles (ML-NSL), retroinclined (+ 1/NA angle) and retropositioned (+ 1/NA (mm)) upper incisors. According to van Diepenbeek et al. study, which investigated age-dependent changes of the parameters SNA, SNB, ANB and SN/GoMe in white adolescents, who were aged between 9 and 14, partly different results were described: the degree of prognathism of the maxilla (SNA: 0.1–0.3 per year) and the mandible (SNB: 0.2–0.4 per year) increased, although the sagittal discrepancy between the jaw bases (ANB: 0.1–0.2 per year) decreased at higher ages. Furthermore, van Diepenbeek et al. described a counterclockwise rotation of the mandible (SN/GoMe: 0.2–0.6 per year) [34]. In contrast, our results revealed a clockwise rotation of the mandible (ML-NSL) at higher ages, which might be explained by differences in the study populations.
Considering cephalometric parameters of skeletal class III patients, our findings presented several significant differences with respect to gender and age. In male subjects, both jaw bases were more anteriorly inclined (NL-NSL, ML-NSL), the growth pattern was more horizontal (PFH/ AFH), the mandible (SNB) was more prognathic and the sagittal position of chin (SN-Pg) was more anterior compared to females. Contrary to our results, Taner et al. [33] found mostly similar sagittal and vertical skeletal cephalometric variables in male and female skeletal class III children, aged between 10 and 11.5 years, except for the posterior (R2PNS) and anterior (R2ANT) nasal spine position, being more anterior in males. This contradicting finding might be due to differences in the study population and the method used to determine skeletal class (ANB vs. Calculated_ANB). Regarding the effect of age on cephalometric parameters in our skeletal class III sample, adult patients (age > 21) demonstrated a more pronounced skeletal class III (Wits appraisal) than younger subjects. Furthermore, skeletal class III adults presented more retroinclined (+ 1/NL angle, + 1/NSL angle) and anteriorly positioned (+ 1/NA (mm)) upper incisors, but a smaller interincisal angle compared to younger patients. Similarly, among skeletal class III patients, adolescents (age 14–20) showed a more severe skeletal class III (Wits appraisal) as well as more retroinlcined (+ 1/NL angle, + 1/NSL angle) but anteriorly positioned (+ 1/NA (mm)) upper front teeth compared to children (age 0–13). These findings demonstrate that the skeletal sagittal discrepancy increases during growth, and that upper incisors partly (sagittal position only) compensate the skeletal disharmony. Furthermore, this skeletal observation can be supported by the results of van Diepenbeek et al. [34], who reported a reduction in ANB-angle and, hence, a trend towards a more mesial basal relation during growth.
Regarding the correlations between cephalometric parameters, we detected many between patients with skeletal class II and III, especially between variables measured in the same dimension. Furthermore, many correlations were found between Calculated_ANB and other parameters in both skeletal classes. These findings demonstrate that skeletal class, determined by Calculated_ANB, mainly depends on other sagittal skeletal parameters and some vertical variables. Our findings are supported by several other studies already published. Using bivariate analysis, Jan et al. [35] showed that the ANB angle and Wits appraisal were significantly correlated (ρ = 0.469, P = 0.00). Moreover, another study identified statistically significant correlations between seven sagittal parameters. The correlation was robust between AXB and AF-BF distance, A-B plane and ANB angle, AXB and FABA, and AF-BF distance and FABA, but weak between ANB and beta angle [36]. Saad et al. [37] reported the most statistically significant and robust correlation between Calculated_ANB (with a different formula) and ANB, followed by the Wits appraisal. In addition, this study found that Calculated_ANB was not significantly associated with SNA and SN-GoMe.
The results of the PCA, which considered all cephalometric parameters, were very satisfying, as PC1 explained more than half of the variance, and the addition of PC2 + PC3 + PC4 resulted in a cumulative proportion of variance of 92% in the cephalometric data generated by skeletal class II/ III.
Among all cephalometric variables, the most important ones contributing to the first PC were the anteroposterior relationship (ANB angle, and Calculated_ANB, positive), the inclination of the mandible (ML-NSL, positive) as well as the sagittal position of the chin (SN-Pg) and mandible (SNB), the facial axis and PFH/ AFH (negative). Concerning the second principal component, the most relevant parameters according to their loading values were the growth pattern (Gonion angle), inclination of the mandible (ML-NSL), divergence of the jaw bases (NL-ML) (positive) as well as the skeletal class (Wits appraisal, Calculated_ANB, ANB) and inclination of the lower incisors (-1/ ML) (negative). These results demonstrate that both sagittal and vertical skeletal parameters influence the true anteroposterior discrepancy between the upper and the lower jaw.
In a previous study that performed PCA with cephalometric results found that 68.2% of the total sample’s shape variability was explained by the first 5 principal components. The most important parameter of the first principal component, which explained 29% of the variability, was the divergence of skeletal pattern, and the most relevant variable contributing to the second principal component, which added 20% to the total variance, was the anteroposterior maxillary relationship [38]. Another study, which evaluated 16 measurements using Steiner analysis [12] for 120 patients, identified five principal components, which covered 88.545% of the total variance of variables. The rotated components matrix showed that the PCs corresponded to the following measurement order: SND, Maxl-NA, 1I-NB S-E, and ANB [39].
The Machine Learning model, which included the Wits appraisal and SNB only, revealed an accuracy of 0.95, suggesting that the application of two cephalometric parameters only may be sufficient to diagnose an Arab individual as skeletal II or III because considering all variables in the general models added only 4% in accuracy. This finding demonstrates the necessity of accurately identifying the corresponding landmarks of the Wits appraisal and SNB. Even though the number of included parameters (Wits appraisal, SNB) in the ML model is comparable with the one used in the method suggested by Panagiotidis and Witt (SNA, ML-NSL, ANB), an advantage of our technique is its possible application in potential future feasibility studies, allowing an automated diagnosis of skeletal class II and III. Furthermore, future studies might combine the results of this study with a computerized detection of landmarks in lateral cephalograms, which might help orthodontists in precise and fast diagnosis of an individual’s skeletal class. Still, bigger sample sizes and validations in new data sets are necessary to develop such systems for clinical applications.
Another application of ML models in the field of orthodontics was described by Taraji et al. [40]. They analyzed lateral cephalograms and dental records of 182 post circumpubertal participants with skeletal and dental class III and aimed to identify critical morphological features that influence the decision camouflage vs. surgery in treatment planning to develop a machine learning model. According to their findings neither gender nor age were significantly different between groups, whereas Wits appraisal, anterior overjet and Mx/Md ratio were found as a key predictors [40].
This study presented a high accuracy in the ML model in Arab patients, but it’s important to check if similar results will be gained from other ethnic groups. For this purpose, in another study that it’s still under review, we examined SCIIMO and SCIIIMO German patients ML models, and found that Wits appraisal as an input variable only resulted in accuracy of 94.9% in the RF model (study under review). In another study that was done on all skeletal classes orthodontic patients in Sri Lanka, using cephalometric radiographs, and categorized patients according to the measured ANB, found that the accuracy of the multinomial logistic regression model, k-NN algorithm, random forest, and Naïve Bayes classification of malocclusion patterns are 88.89%, 83.33%, 88.89%, and 55.56%, respectively, using SNA, SNB and ANB parameters [41].
Limitations
The study pool comprised patients presenting only skeletal class II and III, whereas patients with skeletal class I were not included in this investigation. Hence, within this analysis, we could not prove the machine learning model’s performance, i.e., the sensitivity, specificity, reliability, and accuracy, in a broader population with all skeletal classes. However, this is of significant importance in orthodontic diagnostics. However, this study tried to cover several research questions with a specific focus on skeletal malocclusions, and therefore, future studies are intended to address this shortcoming. Another limitation was the partly heterogeneous size of the age- and gender-specific subgroups, which the retrospective allocation of patients can be explained into different (sub)groups. Again, future studies should try to ensure homogenous sample sizes.
Conclusion and future research
Based on the results of our study, we emphasize that gender and age influence the cephalometric measurements in patients with skeletal class II and III. In addition, PCA can be an effective tool to simplify many cephalometric parameters to two PCs that explain 71% of the variability of skeletal class II/ III diagnosis. Finally, A machine learning model, which considered the Wits appraisal and SNB only, achieved a high accuracy of 0.95 in diagnosing skeletal class II/ III. In summary, the study provides valuable information about the complexity of cephalometric measurement in an Arab population and, more importantly, presents an accurate machine learning model for the identification of individuals as skeletal class II or III, which might support clinicians in fast and precise diagnosis, thereby advancing personalized orthodontic diagnostics and treatment planning.
Data availability
No datasets were generated or analysed during the current study.
References
Cenzato N, Nobili A, Maspero C (2021) Prevalence of dental malocclusions in different geographical areas: scoping review. Dentistry J 9. https://doi.org/10.3390/dj9100117
Lone IM, Zohud O, Midlej K et al (2023) Skeletal class II malocclusion: from clinical treatment strategies to the Roadmap in identifying the Genetic Bases of Development in humans with the support of the Collaborative Cross Mouse Population. J Clin Med 12. https://doi.org/10.3390/jcm12155148
Zohud O, Lone IM, Midlej K et al (2023) Towards genetic dissection of skeletal class III malocclusion: a review of genetic variations underlying the phenotype in humans and future directions. J Clin Med 12. https://doi.org/10.3390/jcm12093212
Lone IM, Zohud O, Nashef A et al (2023) Dissecting the complexity of skeletal-malocclusion-Associated phenotypes: mouse for the rescue. Int J Mol Sci 24. https://doi.org/10.3390/ijms24032570
Maspero C, Galbiati G, Giannini L et al (2018) Class II division 1 malocclusions: comparisons between one- and two-step treatment. Eur J Paediatr Dent 19:295–299. https://doi.org/10.23804/ejpd.2018.19.04.8
Katz CRT, Rosenblatt A, Gondim PPC (2004) Nonnutritive sucking habits in Brazilian children: effects on deciduous dentition and relationship with facial morphology. Am J Orthod Dentofac Orthop 126:53–57. https://doi.org/10.1016/j.ajodo.2003.06.011
Peres KG, Barros AJD, Peres MA, Victora CG (2007) Effects of breastfeeding and sucking habits on malocclusion in a birth cohort study. Rev Saude Publica 41:343–350. https://doi.org/10.1590/s0034-89102007000300004
Heimer MV, Tornisiello Katz CR, Rosenblatt A (2008) Non-nutritive sucking habits, dental malocclusions, and facial morphology in Brazilian children: a longitudinal study. EORTHO 30:580–585. https://doi.org/10.1093/ejo/cjn035
de Sousa RV, Pinto-Monteiro AK, de Martins A CC, et al (2014) Malocclusion and socioeconomic indicators in primary dentition. Braz Oral Res 28:54–60. https://doi.org/10.1590/s1806-83242013005000032
Liu J, Chen Y, Li S et al (2021) Machine learning in orthodontics: challenges and perspectives. Adv Clin Exp Med 30:1065–1074. https://doi.org/10.17219/acem/138702
Manosudprasit A, Haghi A, Allareddy V, Masoud MI (2017) Diagnosis and treatment planning of orthodontic patients with 3-dimensional dentofacial records. Am J Orthod Dentofac Orthop 151:1083–1091. https://doi.org/10.1016/j.ajodo.2016.10.037
Steiner CC (1953) Cephalometrics for you and me. Am J Orthod 39:729–755. https://doi.org/10.1016/0002-9416(53)90082-7
Jacobson A (1975) The wits appraisal of jaw disharmony. Am J Orthod 67:125–138. https://doi.org/10.1016/0002-9416(75)90065-2
Panagiotidis G, Witt E (1977) Der Individualisierte ANB-Winkel. Fortschr Der Kieferorthopädie 38:408–416. https://doi.org/10.1007/BF02163219
Järvinen S (1986) Floating norms for the ANB angle as guidance for clinical considerations. Am J Orthod Dentofac Orthop 90:383–387. https://doi.org/10.1016/0889-5406(86)90004-1
Järvinen S (1988) Relation of the Wits appraisal to the ANB angle: a statistical appraisal. Am J Orthod Dentofac Orthop 94:432–435. https://doi.org/10.1016/0889-5406(88)90134-5
Yen CH (1990) [The individualized ANB angle of Chinese adults]. Gaoxiong Yi Xue Ke Xue Za Zhi 6:449–453
Paddenberg E, Proff P, Kirschneck C (2023) Floating norms for individualising the ANB angle and the WITS appraisal in orthodontic cephalometric analysis based on guiding variables. J Orofac Orthop 84:10–18. https://doi.org/10.1007/s00056-021-00322-1
Dehesa-Santos A, Park J-A, Lee S-J, Iglesias-Linares A (2024) East Asian and southern European craniofacial class III phenotype: two sides of the same coin? Clin Oral Investig 28:84. https://doi.org/10.1007/s00784-023-05386-4
Sivakumar A, Nalabothu P, Thanh HN, Antonarakis GS (2021) A Comparison of Craniofacial Characteristics between Two Different Adult Populations with Class II Malocclusion-A Cross-Sectional Retrospective Study. Biology (Basel) 10:. https://doi.org/10.3390/biology10050438
Shin W, Yeom H-G, Lee GH et al (2021) Deep learning based prediction of necessity for orthognathic surgery of skeletal malocclusion using cephalogram in Korean individuals. BMC Oral Health 21:130. https://doi.org/10.1186/s12903-021-01513-3
Xanthopoulos P, Pardalos PM, Trafalis TB (2013) Linear Discriminant Analysis. Robust Data Mining. Springer New York, New York, NY, pp 27–33
Cortes C, Vapnik V (1995) Support-vector networks. Mach Learn 20:273–297. https://doi.org/10.1007/BF00994018
Pisner DA, Schnyer DM (2020) Support vector machine. Machine learning. Elsevier, pp 101–121
Cover T, Hart P (1967) Nearest neighbor pattern classification. IEEE Trans Inf Theory 13:21–27. https://doi.org/10.1109/TIT.1967.1053964
Qahaz N, Lone IM, Khadija A et al (2023) Host genetic background effect on body weight changes influenced by heterozygous smad4 knockout using collaborative cross mouse population. Int J Mol Sci 24. https://doi.org/10.3390/ijms242216136
Breiman L (2001) Random forests. Springer Sci Bus Media LLC 45:5–32. https://doi.org/10.1023/a:1010933404324
Lone IM, Nun NB, Ghnaim A et al (2023) High-fat diet and oral infection induced type 2 diabetes and obesity development under different genetic backgrounds. Anim Models Exp Med 6:131–145. https://doi.org/10.1002/ame2.12311
Krzywinski M, Altman N (2017) Points of significance: classification and regression trees. Nat Methods 14:757–758. https://doi.org/10.1038/nmeth.4370
Cawley GC, Talbot NLC (2010) On over-fitting in model selection and subsequent selection bias in performance evaluation. The Journal of Machine Learning Research
Lone IM, Midlej K, Nun NB, Iraqi FA (2023) Intestinal cancer development in response to oral infection with high-fat diet-induced type 2 diabetes (T2D) in collaborative cross mice under different host genetic background effects. Mamm Genome 34:56–75. https://doi.org/10.1007/s00335-023-09979-y
Lau JW, Hägg U (1999) Cephalometric morphology of Chinese with class II division 1 malocclusion. Br Dent J 186:188–190. https://doi.org/10.1038/sj.bdj.4800059
Taner L, Gürsoy GM, Uzuner FD (2019) Does gender have an effect on craniofacial measurements? Turkish J Orthod 32:59–64. https://doi.org/10.5152/TurkJOrthod.2019.18031
van Diepenbeek AF, Buschang PH, Prahl-Andersen B (2009) Age-dependant cephalometric standards as determined by multilevel modeling. Am J Orthod Dentofac Orthop 135:79–87. https://doi.org/10.1016/j.ajodo.2006.11.025
Jan A, Bangash AA, Shinwari S (2017) The correlation between wits and ANB Cephalometric Landmarks in Orthodontic pateints. Pakistan Armed Forces Med J 67:S267–S271
Gul-e-Erum, Fida M (2008) A comparison of cephalometric analyses for assessing sagittal jaw relationship. J Coll Physicians Surg Pak 18:679–683
Saad A, Saqib N, Hamid WU (2007) Corelaton of corrected ANB angle with other sagital discrepancy indicators
Halazonetis DJ (2004) Morphometrics for cephalometric diagnosis. Am J Orthod Dentofac Orthop 125:571–581. https://doi.org/10.1016/j.ajodo.2003.05.013
Dascalu CG, Zegan G Statistical methods for variables space reduction in cephalometric studies. In: 2013 E-Health and, Conference B (2013) (EHB). IEEE, pp 1–4
Taraji S, Atici SF, Viana G et al (2023) Novel machine learning algorithms for prediction of treatment decisions in adult patients with class III malocclusion. J Oral Maxillofac Surg 81:1391–1402. https://doi.org/10.1016/j.joms.2023.07.137
Jayathilake AMICK, Nawarathna LS, Nagarathne PNPS (2021) Prediction of malocclusion pattern of the orthodontic patients using a classification model. In: Shakya S, Balas VE, Haoxiang W, Baig Z (eds) Proceedings of international conference on sustainable expert systems: ICSES 2020. Springer Singapore, Singapore, pp 279–287
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by a core fund from Tel Aviv University, orthodontic research center, and the University Hospital of Regensburg.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization, F.A.I., P.P. and N.W.; methodology, I.M.L., O.Z., K.M.,O.A., S.M., S.K., A.W, E.P. and C.K.; validation, F.A.I.; investigation, I.M.L., O.Z., K.M., N.W., O.A., S.M., S.K. and C.K.; resources, F.A.I., P.P., N.W., S.K. and C.K.; data curation, I.M.L., O.Z. and K.M.; writing—original draft preparation, K.M. and I.M.L.; writing—review and editing, P.P., N.W. and F.A.I.; supervision, F.A.I., P.P. and N.W.; project administration, F.A.I.; funding acquisition, F.A.I., P.P. and N.W. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Institutional review board statement
According to current guidelines and following the Ethics Committee of the University of Regensburg ethics and regulations, the committee reviewed and approved this research project and study design with approval number 19-1596-101 (dated 13.11.2019).
Informed consent
Informed consent was obtained from all subjects involved in the study, as shown in supplement # 2.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Midlej, K., Watted, N., Awadi, O. et al. Lateral cephalometric parameters among Arab skeletal classes II and III patients and applying machine learning models. Clin Oral Invest 28, 511 (2024). https://doi.org/10.1007/s00784-024-05900-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00784-024-05900-2