
Abstract
Objective
To evaluate the short-term effects of hard and soft splints of different thicknesses on maximum bite force (MBF) and sleep quality (SQ) in participants with sleep bruxism (SB).
Methods
One-hundred-fifteen patients were randomly allocated to five groups: Groups H2(Hard splint-2 mm), H3(Hard splint-3 mm), S2(Soft splint-2 mm), S3(Soft splint-3 mm), and C (control). Outcomes were MBF (assessed with a digital gnathodynamometer) and SQ (assessed with the Pittsburgh Sleep Quality Index). Measurements were performed at T0 (before the splints), T1 (1-month follow-up), and T2 (2-months follow-up). Data were analyzed using one-way analysis of variance(ANOVA), Tukey’s HSD, and chi-square tests (alpha = 0.05).
Results
At T1, the highest MBF values were observed in group H3 (658.01 ± 22.6 N), while the lowest in group S2 (585.45 ± 8.68 N). For T2, the highest values were obtained in H3 group (676.85 ± 21.9 N), and the lowest in group S2 (565.65 ± 10.9 N) (p < 0.05).For SQ, groups S2 and S3 revealed the lowest PSQI values at T1 (9.1; 9.6) and T2 (9; 9.5) (p < 0.001).
Conclusions
The short-term use of both 2 and 3-mm thick soft splints resulted in a decrease in MBF. Improvement in SQ in patients using soft splints was observed in the 1st month and was maintained in the 2nd month.
Clinical Relevance
This study provides insights on short-term clinical effects as regards to increased sleep quality and regulated maximum bite force as a function of splint material type and the thickness of the splint.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bruxism is described by the 3rd edition of the International Classification of Sleep Disorders as ‘repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible’ [1]. Bruxism most commonly occurs during sleep (sleep bruxism(SB)) and the prevalence ranging from 8 to 10% being more common in young adults [2, 3]. According to the International Consensus on Bruxism held in 2018, SB defined as a masticatory muscle activity during sleep that is characterised as rhythmic (phasic) or non-rhythmic (tonic) and is not a movement disorder or a sleep disorder in otherwise healthy individuals[4]. The current state of the art is that three types of main factors cause SB: 1) psychological factors(anxiety, stress sensitivity, and personality), 2)biological factors(genetics, sleep arousals, and neurotransmitters), 3)exogenous factors(alcohol, coffee, tobacco, drugs, and medications) [5, 6]. In the current literature, it is reported that SB can be efficiently and objectively diagnosed using polysomnography [6,7,8,9].
Important clinical problems such as damage to hard and soft tissues, orofacial pain, and headache, may occur with SB [6]. Since it is a critical problem in dental clinics, various treatment methods, including occlusal, psychological, pharmacological, and physiotherapy, have been suggested for SB [3, 10]. Among these methods, occlusal splint therapy is accepted as the ‘gold standard’ [11]. Occlusal splint used during sleep helps to inhibit the outcomes of tooth grinding and SB (tooth wear, pain, and grinding sounds), distributes occlusal force, and reduces stress in the structures of the masticatory system and temporomandibular joint [11, 12]. It has also been reported in the literature that occlusal splints significantly reduce SB-related events and the sleep motor activity index of SB patients [3, 13]. These splints, which have different thicknesses, are generally produced in two forms as hard and soft materials [14, 15]. Although there is no clear information in the literature to date, it is generally accepted that the therapeutic effect of hard occlusal splints is similar to or superior to that of soft splints [16,17,18].
Sleep quality(SQ) is an effective factor in the emergence of bruxism and it has been shown that SB is associated with poor SQ and quality of life in these patients [19, 20]. Micro-awakenings, repeated arousals during sleep, increased stress, and anxiety are shown as the main reasons for this negative relationship between SB and SQ [21]. Therefore, particular attention should be paid to elements that affect sleep architecture [21, 22]. In order to improve SQ, occlusal splints of various designs were used in patients with SB and positive clinical results were obtained [3, 23,24,25]. However, these studies have not considered comprehensively which splint type (soft or hard) and thickness are ideal for improved SQ. This question constitutes one of the starting points of the current study.
Although little is known about the mechanism of occlusal splints’ action, this treatment has a reducing effect on nocturnal masticatory muscle activities and protects the teeth from damage caused by jaw muscle contractions related to SB [26, 27]. The occlusal splint also plays a role in the maintenance of a stable and physiologically optimal occlusal force, as it has a reducing effect on asymmetry and hyperactivity of the jaw elevator muscles [28]. Thus, occlusal splints can change occlusal forces due to their force-distributing and bruxism-reducing effects [26]. When the few studies in the literature on the occlusal splint-occlusal force relationship are examined, the results show vast differences[17, 26, 28,29,30]. While some of these studies applying different splint usage times claimed that soft splints were more advantageous in terms of regulation of occlusal force, other groups of researchers reported results in favor of hard splints [17, 26, 28,29,30]. Despite these studies, there is no study evaluating how hard and soft occlusal splint types in different thickness options affect occlusal force. Therefore, the lack of data was the another question that was addressed in this study.
In light of the above-mentioned information, the aim of the present study was to evaluate the short-term effects of hard and soft splints of different thicknesses on occlusal force and SQ in patients with SB. The null hypotheses of the study were as follows: 1) Hard/soft occlusal splints of different thicknesses would bot show significant difference in improving the SQ of SB patients in short-term therapy. 2) Different occlusal splint thicknesses would not affect the occlusal force in short-term therapy.
Materials and methods
Study design
This five-arm parallel design, randomized clinical trial was performed on subjects from the Istanbul University, Faculty of Dentistry, Istanbul-Turkey. Intervention and follow-up sessions were performed between August 2021 and December 2021. The study was approved by the Ethics Committee of the Istanbul University, Faculty of Medicine (protocol number 2019/19; ClinicalTrials Identifier: NCT04934449), and the ethical guidelines of the Declaration of Helsinki were followed. Patients gave written informed consent to participate in the study after a full explanation of the procedures. This study fulfilled the guidelines of the Consolidated Standards of Reporting Trials (CONSORT) to enhance the quality of the results [31].
Study population
Subjects were recruited from the student list of Istanbul University, Faculty of Dentistry. Students who had SB signs and symptoms were enrolled in the study if they met the following inclusion criterion:
-
1.
Being healthy with complete permanent dentition.
The exclusion criteria were as follows:
-
1.
Presence of a systemic disorder that could compromise the masticatory system (e.g., epilepsy, neurological disorders, cerebral palsy, among others),
-
2.
Presence of signs and/or symptoms of TMD based on Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) [32],
-
3.
Current use of drugs or systemic disorders that could interfere with muscle activity and sleep (directly or indirectly),
-
4.
Inappropriate behavior and/or refusal to cooperate with data collection and dental procedures,
-
5.
Tooth loss (except for third molars),
-
6.
Toothache report,
-
7.
Active periodontitis (presence of periodontal pockets involvement of the supporting tissues),
-
8.
Caries lesions,
-
9.
Use of orthodontic appliances,
-
10.
Use of dental prosthesis (removable or fixed partial),
-
11.
Subjects with moderate to severe malocclusions, diagnosed by using the Orthodontic Treatment Need Index (IOTN) (scores 5 or 6-severe and extreme need for orthodontic treatment),
-
12.
Alcohol or drug abuse.
-
13.
Pregnancy,
-
14.
Having mental illness or cancer,
-
15.
Presence of snoring or sleep apnea.
Sample size assumption, allocation, and study groups
The sample size determination was performed based on previous studies, evaluating interocclusal appliance therapy on bite force and/or sleep quality [19, 21]. Power analysis (PS software; Dupont and Plummer, 1997) was conducted by considering power = 0.80, and alpha = 0.05 with a d = 0.76 effect size. The minimum number of samples required for each group was 18, but 115 patients were invited to this study due to potential losses.
Groups were allocated based on a randomized controlled trial, and the random sampling method was performed using a web-based number generator [33]. All files were enumerated and divided into one to five groups consecutively. Patients were randomly assigned to one of the following groups, depending on the type of occlusal splint applied:
-
Group H2: Test group; hard occlusal splint with 2-mm thickness; n = 23
-
Group H3: Test group; hard occlusal splint with 3-mm thickness; n = 23
-
Group S2: Test group; soft occlusal splint with 2-mm thickness; n = 23
-
Group S3: Test group; soft occlusal splint with 3-mm thickness; n = 23
-
Group C: Control group; without occlusal splint therapy; n = 23
Clinical examination and SB diagnosis
Due to the presence of signs and/or symptoms of TMD being an exclusion criterion for the groups, DC/TMD were used to define TMD patients [32]. Axis I of the DC/TMD was administered by one trained examiner and axis II was carried out by the patients individually without time restriction. Patients exhibiting symptoms and signs of TMD were excluded from the study.
The SB diagnosis of the participants was determined by the following criteria:
-
1.
Reporting nocturnal tooth grinding and sounds mostly by the room partner at least three days a week, awakening with cervical and/or facial muscle fatigue and/or pain with dental and/or joint discomfort, and having fractures in dental restorations or teeth.
-
2.
Presence of shiny and polished wear facets between opposing teeth detected during mandibular excursions and clinical examination.
-
3.
Having moderate frequency SB according to the results of the polysomnography exam [29]. Electromyographic analysis of SB episodes was performed by a trained and calibrated technician according to American Sleep Medicine Association criteria [21]. The assessment was made taking into account the number of episodes of rhythmic masticatory muscle activity per hour and by type (tonic,phasic, or mixed) at different stages of sleep. Among the patients evaluated according to these criteria, those with an index of more than 2 episodes/sleep hour were considered positive, while those with an index of 4 or higher were categorized as high-grade SB.
Patients who met the first two criteria mentioned above were considered eligible for polysomnography to provide a definitive diagnosis of SB [20]. The polysomnographic exams were carried out at the Neurology-Sleep Disorders Unit, Istanbul University, Istanbul, Turkey. These evaluations were carried out by using the laboratory-based system(Embla NDx,Natus Embla, Middleton, USA) in a temperature-controlled and quiet room from 9 PM until the patient woke [24].
Occlusal splint therapy and group applications
Mandibular and maxillary casts were obtained from the groups for hard (H2 and H3 groups) and soft occlusal splint (S2 and S3 groups) construction and these casts were mounted on semi-adjustable articulators (Hanau™ Wide-Vue Articulator; Whip Mix Corporation, KY, USA) at maximum intercuspation. Wax-up was performed on the maxillary casts and hard stabilization splints were fabricated from heat polymerized acrylic resin (Trevalon; Dentsply Sirona, NC, USA) according to the instructions of the manufacturer. Complete coverage maxillary splints were 2 mm and 3 mm thick between the mandibular and maxillary first molars, and the splint thickness in the anterior region varied between 3–5 mm according to the occlusal relationship of the patient. Symmetric and simultaneous occlusal contacts with canine guidance were established and all devices were finished and polished [34].
For soft occlusal splint groups (S2 and S3), ethylene vinyl acetate-based material with two different thickness values of 2 mm and 3 mm (KEYSTONE-Soft Eva; Keystone Dental Inc., Cherry Hill, NJ, USA) was used for the fabrication of the maxillary splints. Soft sheets were formed by using a dental vacuum forming machine (Ultraformer; Ultradent Products Inc., South Jordan, UT, USA) according to the manufacturer’s instructions. All devices were fabricated and adjusted by one researcher. All test groups used occlusal splints for at least 8 h during sleep for 2 months.
For the control group, the patients did not receive any treatment and were informed that they would be eligible for SB treatment after one year of symptom follow-up. Group C was not reported to be a control group throughout this study, but they were asked to come to the clinic several times in order to increase group homogeneity, and these patients were evaluated using the same parameters. All groups were requested to avoid taking any medications like antidepressants, tranquilizers, sleeping pills, or muscle relaxants during the research. In addition, no further advice was given to patients, such as sleep hygiene, to avoid confounding factors.
Data collection
Data collection was carried out by a single-blinded researcher by interviewing all patients face to face. Parameters of maximum bite force and sleep quality were evaluated three times: T0, before occlusal splint therapy, T1, one month, and T2, two months after occlusal splint therapy began [24].
Patients' comfort, the experience of splint use, and self-reported symptoms, as well as the parameters measured at each follow-up session, were recorded by the same researcher because of the possibility of influencing the study results.
Maximum bite force(MBF)
Unilateral MBF was measured using a digital gnathodynamometer (Model DDK/M; Kratos, Sao Paolo, Brazil) with fork connection [35]. Maximum force values were provided in Newtons(N) by bite fork with the following dimensions: 10 mm thickness, 15 mm width, and 12 mm high. The appliance was calibrated by loading known force values on the gnathodynamometer.
MBF values of all participants were measured between 11:00 and 15:00, which is the same time interval of the day and after the meal. The examination was performed in a quiet room by having participants seated with their heads in a natural posture, providing the Frankfurt plane parallel to the ground. The fork was placed between the mandibular and maxillary arches and on the first permanent molars, which are the higher force-generating teeth [24].
Before recordings, the participants were trained and instructed to bite the fork with maximum force. After that, they were asked to apply their maximum bite force on both sides (left and right) of the dental arches for three times. The highest value of each bite force was recorded and the mean value of these measurements was considered as the final value with approximately 0.1 N. During sessions, patients were also evaluated for covariables that might affect the study results, such as chewing gum.
SQ
Evaluation of SQ was performed with the Pittsburgh Sleep Quality Index (PSQI) consisting of 19 self-report questions and 5 questions to be answered by a spouse or roommate [36]. The 19 scored questions of the index consist of 7 components and each component is evaluated over 0–3 points. These components are subjective SQ, sleep latency, sleep duration, the efficiency of habitual sleep, sleep disturbances, use of sleep medication, and diurnal dysfunction, respectively. The total score of these 7 components gives the final score, and the final score ranges from 0 to 21. Accordingly, a total score greater than 5 indicates "poor sleep quality".
Statistical analysis
Statistical analysis was carried out using standard statistical software (SPSS V23; IBM Armonk, NY, USA), considering a significance level of p < 0.05. Conformity to normal distribution was evaluated by the Shapiro-Wilk test. Intra-group time comparisons of normally distributed data were analyzed by repeated-measures analysis of variance (ANOVA). The difference between groups over time was analyzed by one-way ANOVA. Multiple comparisons were performed with Tukey’s HSD. ANOVA was applied to compare quantitative descriptive statistics by groups, and the chi-square test was performed for the comparison of categorical data.
Results
During the study, participants did not report any adverse effects or compliance issues related to the use of occlusal splints or the application of polysomnography.
The overall fit of the occlusal splints was performed with a contact point evaluation method. Static occlusion was assessed using an occlusion foil (12 µm thickness, Hanel; Coltene, Langenau, Germany) for each patient, based on the technique mentioned in the study by Patzelt et al.(63y). According to the results, there was no patient who was in need of additive rework or new splint fabrication during sessions.
Demographic data
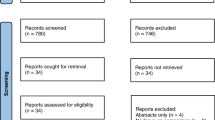
As shown in the flowchart of the study (Fig. 1), 115 SB patients out of 132 were selected to be eligible and randomly assigned. Eleven patients (2 from Group H2, 4 from Group S2, 3 from Group S3, and 2 from the control group) dropped out of the study as they did not respond and were not able to come to the clinic. Statistical analyzes showed that those who dropped out after randomization were not significantly different from those who completed the study in terms of pretreatment demographics or dependent variables.

Flowchart of the study
The demographic data of the participants are displayed in Table 1. The duration of the SB ranged from 3.5 to 5.1 years, and the ages ranged between 18 and 33 years. The majority of the participants were female (p = 0.63), and height and weight parameters were significantly different between the groups (p < 0.05).
MBF
The mean and standard deviation of MBF values of the groups at T0, T1, and T2 are shown in Fig. 2. At T0, total MBF values were equivalent for all groups (Group C = 626.65 ± 6.5 N; Group S2 = 625.9 ± 8.24 N; Group S3 = 634.45 ± 29.9 N; Group H2 = 624.6 ± 10.35 N; Group H3 = 632.95 ± 15.84 N) (p > 0.05). However, there were intragroup and intergroup differences in the right and left measurement values (p < 0.05). While there was a significant decrease in total MBF values of S2 (585.45 ± 8.68 N) and S3 groups (601.20 ± 25.63 N) at T1 time, an increase was detected in H2 (654.5 ± 13.21 N) and H3 groups (658.01 ± 22.6 N) (p < 0.05). The increase and decrease trends observed in the groups (except group C) at time T1 continued in the same way at time T2 and the values were as follows: C = 626.8 ± 5.8 N, S2 = 565.65 ± 10.9 N, S3 = 579.85 ± 24.94 N, H2 = 672.25 ± 11.62 N, H3 = 676.85 ± 21.9 N) (p < 0.05). While this difference in T1 and T2 times was seen only in total MBF values, this situation was not valid for right and left measurement values measured at both times.

Maximum bite force values of the groups from baseline to 1 and 2 months (N,Newton; R,Right; L,Left; S2, Soft splint group-2 mm; S3, Soft splint group-3 mm; H2, Hard splint group-2 mm; H3, Hard splint group-3 mm; T0,before the splints; T1,1-month follow-up; T2,2-months follow-up;*, significant difference)
SQ-PSQI
The PSQI score decrease in patients using soft occlusal splints at T1 was greater than patients using hard splints (Fig. 3) (p < 0.001). In this time interval, while the S2 and S3 groups showed statistically no difference, the same was valid for the H2 and H3 groups (p > 0.05). At T2, however, the PSQI results obtained at T1 were preserved. There was no significant change in the values of the control group during the evaluation process.

Comparison of PSQI global score from baseline to 1 and 2 months(PSQI, Pittsburgh Sleep Quality Index; S2, Soft splint group-2 mm; S3, Soft splint group-3 mm; H2, Hard splint group-2 mm; H3, Hard splint group-3 mm; T0,before the splints; T1,1-month follow-up; T2,2-months follow-up;*, significant difference)
Discussion
The null hypothesis of this study was rejected because MBF decreased in soft splint groups (S2 and S3) after short-term use, but increased in hard splint groups (H2 and H3). Additionally, soft splint groups showed lower PSQI values compared to the others, reflecting an improvement in self-reported SQ.
Occlusal splints are elements that balance the force distribution in the entire masticatory system [37]. Despite this importance, only one study in the literature investigated the occlusal splint types of two different thicknesses (3 mm and 6 mm) in individuals with bruxism, and one study evaluated the effectiveness of hard and soft occlusal splints [26, 38]. Therefore, the current study is the first in the literature to evaluate both different occlusal splint types (soft and hard) and different thickness values (2 mm and 3 mm) together. While Abekura emphasized that 3 mm-thick occlusal splints were more comfortable in their study, Karakis et al. found that both soft and hard splints helped to improve clinical symptoms of bruxism [26, 38]. In this study, soft occlusal splints of both thicknesses were found to be clinically more effective in short-term use in terms of PSQI, while the results obtained in both splint types in terms of MBF require further studies.
It is known that occlusal splints in different thicknesses can cause a change in occlusal force, and occlusal force has an effect on the functional state of the masticatory system and muscle efficiency [26, 39]. Regarding the increased MBF values of 2 and 3 mm hard occlusal splints, the results of this study were in agreement with other short-term studies that previously evaluated 0.6, 1, 2, and 3 mm thick splints [24, 26, 39]. The present study also found a significant increase in MBF on both sides (right/left) during hard occlusal splint therapy, and this increase may be associated with the positive effect of hard occlusal splints on neurobiological regulation of jaw-muscle activity (Fig. 2) [40]. While there is only one study in the literature showing that the use of hard splints (1 mm) reduces MBF in patients with bruxism, there are also studies claiming that the use of hard splints does not affect MBF (1.5 mm, 2 mm, 3 mm and 6 mm thick splints) [17, 26, 29, 41]. These variable findings may be from splint usage time, diversity of participants, frequency of therapy, type of splint material, the production method of occlusal splints, and evaluation methods.
In the present study, short-term use of soft occlusal splints of both thicknesses reduced MBF (Fig. 2). The reduction of MBF in soft splints was consistent with the findings of other previous studies evaluating 2 and 3 mm thick occlusal splints and reporting similar MBF values [17, 25, 26, 39]. These studies, similar to the present study, investigated the short-term effect of occlusal splints( 6 weeks, 30 days, or 1 day), and the authors of this study postulated that the results obtained in soft and hard splints will continue in the long term in the same manner [17, 25, 26]. This decrease in MBF may be attributed to muscle relaxation or increased awareness of the patient as a result of the use of soft splints [25, 26]. As there is only one study investigating both soft and hard occlusal splints in SB, direct comparison of this study with the current study showed partial consistency with the findings of Karakis et al., who conducted a short-term study(6 weeks) that reported no significant change in MBF for hard occlusal splints and a decrease for soft occlusal splints(2 mm thickness) [26].
At the beginning of the study (T0), there was a significant intragroup difference for H3, and intergroup differences for other groups between the right and left MBF values (Fig. 2). This situation changed at T1 and T2, where only total MBF values were statistically different between the groups. These data of the current study are corroborated by the study of Canay et al., who reported no significant change in the asymmetry index after four weeks of splint therapy [42]. Additionally, MBF levels are accepted to be related to bruxism and the findings of the current study may change based on occlusal contact area, interocclusal separations, malocclusion, the location of the measuring device on the jaw, body size, age, weight, height, gender, and posture of the patient [39, 43,44,45,46]. Therefore, in future studies in patients with bruxism, the above-mentioned parameters can be evaluated with longer use.
The choice of biomaterial for occlusal splints has a significant effect on the neurobiological regulation of jaw muscle activity during sleep, and splint thickness has been reported to play a role in the incidence of SB in short-term use [40, 47]. In this study, the soft splint groups (S2 and S3) showed the lowest PSQI scores among all groups, indicating an improvement in SQ with soft splint use (Fig. 3). These findings may be attributed to the theory that soft splints increase awareness of tiredness of the muscles by reducing occlusal force, as stated in the study by Narita et al. [17]. The current study showed inconsistency with the findings of the only study in the literature that evaluated soft and hard splints (2 mm thickness) together and found that the use of both soft and hard splints improved SQ in individuals with SB [21]. Another point worth noting is that patients included in this study reported a better SQ after one month of soft splint use, with a non-statistically significant decrease in PSQI scores in the second month. Therefore, we anticipate that longer-term use of occlusal splints will not make a clinical difference in PSQI values. Taken together, one month of splint use may be accepted as sufficient to increase SQ based on the findings of this study, while the placebo effect should be evaluated in future studies [48, 49].
Since there are not enough studies in the literature in which soft splints are used in patients with SB, the comparison was made over studies evaluating hard splints. The current study did not corroborate with the results of a study from Harada et al., who reported that the use of hard splints (1–2 mm thickness) was effective only immediately after the insertion and that the use of splints for 6 weeks did not produce a clinical effect [11]. Because the use of hard splints in the current study did not cause a significant decrease in PSQI scores from the beginning of the study to the completion of the 2-month follow-up period. The reason for this variation may be the difference in splint thicknesses, the production method of splints, the characteristics of the included population, and the difference in the evaluation methods. Last but not least, some studies evaluating hard splints (1 mm, 2 mm, 3 mm thickness) reported improvement in SQ, whereas others showed no change (1 mm, and 2 mm thickness) [3, 11, 14, 16, 23, 24, 47, 50,51,52,53]. Thus, the efficacy of hard and soft splints in SQ remains controversial.
The current study investigated only the use of hard and soft occlusal splints in the treatment of SB patients. However, according to a recent study which is a critical evaluation of systematic reviews, it has been reported that botulinum toxin injection, biofeedback, centrally acting drugs(clonidine, clonazepam), hard stabilization splint, vibratory feedback, and maxillary occlusal splints are also effective in the treatment of SB [54]. Therefore, future studies evaluating these reported treatment types alone or in combination are needed, in order to confirm the results of the current study and to find the most optimal treatment for SB.
The limitations of this study are implementation of only a two-month follow-up period, lack of precise assessment of the masticatory muscles activity during sleep, lack of assessment of masticatory muscle stiffness before and after occlusal splint therapy, including only one grade (moderate) SB patient group, not considering SB duration, not blinding, the inclusion of only SB, and one-way therapy evaluation (using PSQI). Future research should use polysomnography to further evaluate specific areas of sleep improvement after an occlusal splint is used. Nevertheless, this study addressed the effect of hard and soft occlusal splints at various thicknesses which addresses a current clinical question during fabrication of occlusal splints.
Conclusions
Short-term use of soft occlusal splints produced in both thicknesses caused a decrease in the MBF scores of the patients with SB, while the use of hard splints in both thicknesses caused gradually increasing MBF values one to two months of use. The findings suggested that 1 month of therapy with a soft occlusal splint had a positive effect on SQ and maintained the obtained improvement from one month to two months of treatment.
Data availability
The data that support the findings of this study are available in Clinical Trials [repository name] at ClinicalTrials.govhttps://clinicaltrials.gov, reference number [ClinicalTrials Identifier: NCT04934449].
References
Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL (2017) Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med 13:307–349. https://doi.org/10.5664/jcsm.6470
Lobbezoo F, van der Zaag J, van Selms MK, Hamburger HL, Naeije M (2008) Principles for the management of bruxism. J Oral Rehabil 35:509–523. https://doi.org/10.1111/j.1365-2842.2008.01853.x
Singh PK, Alvi HA, Singh BP, Singh RD, Kant S, Jurel S, Singh K, Arya D, Dubey A (2015) Evaluation of various treatment modalities in sleep bruxism. J Prosthet Dent 114:426–431. https://doi.org/10.1016/j.prosdent.2015.02.025
Lobbezoo F, Ahlberg J, Raphael KG, Wetselaar P, Glaros AG, Kato T, Santiago V, Winocur E, De Laat A, De Leeuw R, Koyano K, Lavigne GJ, Svensson P, Manfredini D (2018) International consensus on the assessment of bruxism: Report of a work in progress. J Oral Rehabil 45:837–844. https://doi.org/10.1111/joor.12663
Wieczorek T, Wieckiewicz M, Smardz J, Wojakowska A, Michalek-Zrabkowska M, Mazur G, Martynowicz H (2020) Sleep structure in sleep bruxism: A polysomnographic study including bruxism activity phenotypes across sleep stages. J Sleep Res 29:e13028. https://doi.org/10.1111/jsr.13028
Smardz J, Martynowicz H, Wojakowska A, Winocur-Arias O, Michalek-Zrabkowska M, Mazur G, Wieckiewicz M (2022) A polysomnographic study on the relationship between sleep bruxism intensity and sleep quality. Cranio 40:107–112. https://doi.org/10.1080/08869634.2020.1716466
Smardz J, Martynowicz H, Michalek-Zrabkowska M, Wojakowska A, Mazur G, Winocur E, Wieckiewicz M (2019) Sleep bruxism and occurrence of temporomandibular disorders-related pain: A Polysomnographic Study. Front Neurol 10:168. https://doi.org/10.3389/fneur.2019.00168
Wieckiewicz M, Smardz J, Martynowicz H, Wojakowska A, Mazur G, Winocur E (2020) Distribution of temporomandibular disorders among sleep bruxers and non-bruxers-A polysomnographic study. J Oral Rehabil 47:820–826. https://doi.org/10.1111/joor.12955
Sinclair A, Wieckiewicz M, Ettlin D, Junior R, Guimarães AS, Gomes M, Meira E, Cruz M (2022) Temporomandibular disorders in patients with polysomnographic diagnosis of sleep bruxism: a case-control study. Sleep Breath 26:941–948. https://doi.org/10.1007/s11325-021-02449-2
Ommerborn MA, Schneider C, Giraki M, Schäfer R, Handschel J, Franz M, Raab WH (2007) Effects of an occlusal splint compared with cognitive-behavioral treatment on sleep bruxism activity. Eur J Oral Sci 115:7–14. https://doi.org/10.1111/j.1600-0722.2007.00417.x
Harada T, Ichiki R, Tsukiyama Y, Koyano K (2006) The effect of oral splint devices on sleep bruxism: a 6-week observation with an ambulatory electromyographic recording device. J Oral Rehabil 33:482–488. https://doi.org/10.1111/j.1365-2842.2005.01576.x
Câmara-Souza MB, de Figueredo OMC, Rodrigues Garcia RCM (2019) Association of sleep bruxism with oral health-related quality of life and sleep quality. Clin Oral Investig 23:245–251. https://doi.org/10.1007/s00784-018-2431-0
Matsumoto H, Tsukiyama Y, Kuwatsuru R, Koyano K (2015) The effect of intermittent use of occlusal splint devices on sleep bruxism: a 4-week observation with a portable electromyographic recording device. J Oral Rehabil 42:251–258. https://doi.org/10.1111/joor.12251
Wang S, Li Z, Ye H, Zhao W, Liu Y, Zhou Y (2020) Preliminary clinical evaluation of traditional and a new digital PEEK occlusal splints for the management of sleep bruxism. J Oral Rehabil 47:1530–1537. https://doi.org/10.1111/joor.13083
Akbulut N, Altan A, Akbulut S, Atakan C (2018) Evaluation of the 3mm thickness splint therapy on temporomandibular joint disorders (TMDs). Pain Res Manage 3657587:1–8. https://doi.org/10.1155/2018/3756587
Cruz-Reyes RA, Martínez-Aragón I, Guerrero-Arias RE, García-Zura DA, González-Sánchez LE (2011) Influence of occlusal stabilization splints and soft occlusal splints on the electromyographic pattern, in basal state and at the end of six weeks treatment in patients with bruxism. Acta Odontol Latinoam 24(1):66–74
Narita N, Funato M, Ishii T, Kamiya K, Matsumoto T (2009) Effects of jaw clenching while wearing an occlusal splint on awareness of tiredness, bite force, and EEG power spectrum. J Prosthodont Res 53:120–125. https://doi.org/10.1016/j.jpor.2009.02.006
Silva CAGD, Grossi ML, Araldi JC, Corso LL (2020) Can hard and/or soft occlusal splints reduce the bite force transmitted to the teeth and temporomandibular joint discs? A finite element method analysis [published online ahead of print, 2020 Dec 5]. Cranio 1–8. https://doi.org/10.1080/08869634.2020.1853464
Matsuda S, Yamaguchi T, Mikami S, Okada K, Gotouda A, Sano K (2016) Rhythm and amplitude of rhythmic masticatory muscle activity during sleep in bruxers - comparison with gum chewing. Cranio 34:234–241. https://doi.org/10.1080/08869634.2015.1106807
Lobbezoo F, Ahlberg J, Glaros AG, Kato T, Koyano K, Lavigne GJ, de Leeuw R, Manfredini D, Svensson P, Winocur E (2013) Bruxism defined and graded: an international consensus. J Oral Rehabil 40:2–4. https://doi.org/10.1111/joor.12011
American Academy of Sleep Medicine (2014) International Classification of Sleep Disorders, 3rd edn. American Academy of Sleep Medicine, Darien
Manfredini D, Serra-Negra J, Carboncini F, Lobbezoo F (2017) Current concepts of bruxism. Int J Prosthodont 30:437–438. https://doi.org/10.11607/ijp.5210
Vilanova LS, Gonçalves TM, Pimentel MJ, Bavia PF, Rodrigues Garcia RC (2014) Mastication movements and sleep quality of patients with myofascial pain: occlusal device therapy improvements. J Prosthet Dent 112:1330–1336. https://doi.org/10.1016/j.prosdent.2014.07.008
Rosar JV, Barbosa TS, Dias IOV, Kobayashi FY, Costa YM, Gavião MBD, Bonjardim LR, Castelo PM (2017) Effect of interocclusal appliance on bite force, sleep quality, salivary cortisol levels and signs and symptoms of temporomandibular dysfunction in adults with sleep bruxism. Arch Oral Biol 82:62–70. https://doi.org/10.1016/j.archoralbio.2017.05.018
Mainieri VC, Saueressig AC, Fagondes SC, Mainieri ET, Shinkai RSA, Grossi ML (2008) Bite force and sleep quality in patients with bruxism before and after using a mandibular advancement device. Rev Odonto Cienc 23:229–233
Karakis D, Dogan A, Bek B (2014) Evaluation of the effect of two different occlusal splints on maximum occlusal force in patients with sleep bruxism: a pilot study. J Adv Prosthodont 6:103–108. https://doi.org/10.4047/jap.2014.6.2.103
Nakazato Y, Takaba M, Abe Y, Nakamura H, Ohara H, Suganuma T, Clark GT, Baba K (2021) Effect of contingent vibratory stimulus via an oral appliance on sleep bruxism after the splint adaptation period. J Oral Rehabil 48:901–908. https://doi.org/10.1111/joor.13182
Kurita H, Ikeda K, Kurashina K (2000) Evaluation of the effect of a stabilization splint on occlusal force in patients with masticatory muscle disorders. J Oral Rehabil 27:79–82
Alkan A, Bulut E, Arici S, Sato S (2008) Evaluation of treatments in patients with nocturnal bruxism on bite force and occlusal contact area: A preliminary report. Eur J Dent 2:276–282 (PMID: 19212534)
Solanki N, Singh BP, Chand P, Siddharth R, Arya D, Kumar L, Tripathi S, Jivanani H, Dubey A (2017) Effect of mandibular advancement device on sleep bruxism score and sleep quality. J Prosthet Dent 117:67–72. https://doi.org/10.1016/j.prosdent.2016.04.009
Juszczak E, Altman DG, Hopewell S, Schulz K (2019) Reporting of multi-arm parallel-group randomized trials: extension of the CONSORT 2010 statement. JAMA 321:1610–1620. https://doi.org/10.1001/jama.2019.3087
Polat S, Polat N, Cetioglu A (2016) Diagnostic Criteria for Temporomandibular Disorders: Assessment instruments (Turkish) (2016). [Temporomandibuler düzensizlikler için teşhis kriterleri: Değerlendirme araçları]. Turkish translation. 2016
Research Randomizer. https://www.randomizer.org/. Accessed July 2, 2021
Okeson JP (2019) Management of Temporomandibular Disorders and Occlusion (ed 8).St Louis, Mo: Elsevier Mosby Inc
Scudine KGO, Pedroni-Pereira A, Araujo DS, Prado DGA, Rossi AC, Castelo PM (2016) Assessment of the differences in masticatory behavior between male and female adolescents. Physiol Behav 163:115–122. https://doi.org/10.1016/j.physbeh.2016.04.053
Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28:193–213. https://doi.org/10.1016/0165-1781(89)90047-4
Dylina TJ (2001) A common-sense approach to splint therapy. J Prosthet Dent 86:539–545. https://doi.org/10.1067/mpr.2001.118878
Abekura H, Yokomura M, Sadamori S, Hamada T (2008) The initial effects of occlusal splint vertical thickness on the nocturnal EMG activities of masticatory muscles in subjects with a bruxism habit. Int J Prosthodont 21:116–120
Tang Y, Li H, Chen Y, Zhu L, Kang H (2018) Effect of different splint thicknesses on occlusal function and temporomandibular joint sounds: a clinical report. OJST 8:326–337. https://doi.org/10.4236/ojst.2018.812031
Arima T, Takeuchi T, Tomonaga A, Yachida W, Ohata N, Svensson P (2012) Choice of biomaterials-Do soft occlusal splints influence jaw-muscle activity during sleep? A Pre Rep 262:159–162. https://doi.org/10.1016/j.apsusc.2012.04.013
Pita MS, Ribeiro AB, Garcia AR, Pedrazzi V, Zuim PR (2011) Effect of occlusal splint thickness on electrical masticatory muscle activity during rest and clenching. Braz Oral Res 25:506–511. https://doi.org/10.1590/s1806-83242011000600006
Canay S, Cindaş A, Uzun G, Hersek N, Kutsal YG (1998) Effect of muscle relaxation splint therapy on the electromyographic activities of masseter and anterior temporalis muscles. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85:674–679. https://doi.org/10.1016/s1079-2104(98)90034-8
Ahlgren J, Omnell KA, Sonesson B, Toremalm NG (1969) Bruxism and hypertrophy of the masseter muscle: a clinical, morphological and functional investigation. Pract Otorhinolaryngol 31:22–29. https://doi.org/10.1159/000274876
Lyons M, Baxendale RH (1990) A preliminary electromyographic study of bite force and jaw-closing muscle fatigue in human subjects with advanced tooth wear. J Oral Rehabil 17:311–318. https://doi.org/10.1111/j.1365-2842.1990.tb00014.x
Nishigawa K, Bando E, Nakano M (2001) Quantitative study of bite force during sleep associated bruxism. J Oral Rehabil 28:485–491. https://doi.org/10.1046/j.1365-2842.2001.00692.x
Gibbs CH, Mahan PE, Mauderli A, Lundeen HC, Walsh EK (1986) Limits of human bite strength. J Prosthet Dent 56:226–229. https://doi.org/10.1016/0022-3913(86)90480-4
Takahashi H, Masaki C, Makino M, Yoshida M, Mukaibo T, Kondo Y, Nakamoto T, Hosokawa R (2013) Management of sleep-time masticatory muscle activity using stabilisation splints affects psychological stress. J Oral Rehabil 40:892–899. https://doi.org/10.1111/joor.12110
Dubé C, Rompré PH, Manzini C, Guitard F, de Grandmont P, Lavigne GJ (2004) Quantitative polygraphic controlled study on efficacy and safety of oral splint devices in tooth-grinding subjects. J Dent Res 83:398–403. https://doi.org/10.1177/154405910408300509
Pomponio FB (2010) Sleep bruxism: Polysomnographic study on the evaluation of the intraoral splints effectiveness. [Dissertation]. Universidade de São Paulo [Available at: http://www.teses.usp.br/teses/disponiveis/5/5160/tde-20092010-114919/en.php.]
Landry ML, Rompré PH, Manzini C, Guitard F, de Grandmont P, Lavigne GJ (2006) Reduction of sleep bruxism using a mandibular advancement device: an experimental controlled study. Int J Prosthodont 19:549–556
Castroflorio T, Bargellini A, Lucchese A, Manuelli M, Casasco F, Cugliari G, Cioffi I, Deregibus A (2018) Effects of clear aligners on sleep bruxism: randomized controlled trial. J Biol Regul Homeost Agents 32:21–29
Madani AS, Abdollahian E, Khiavi HA, Radvar M, Foroughipour M, Asadpour H, Hasanzadeh N (2013) The efficacy of gabapentin versus stabilization splint in management of sleep bruxism. J Prosthodont 22:126–131. https://doi.org/10.1111/j.1532-849X.2012.00914.x
van der Zaag J, Lobbezoo F, Wicks DJ, Visscher CM, Hamburger HL, Naeije M (2005) Controlled assessment of the efficacy of occlusal stabilization splints on sleep bruxism. J Orofac Pain 19:151–158
Cerón L, Pacheco M, Delgado Gaete A, Bravo Torres W, Astudillo Rubio D (2022) Therapies for sleep bruxism in dentistry: A critical evaluation of systematic reviews. Dent Med Probl. https://doi.org/10.17219/dmp/156400
Funding
The authors declare that this study has received no financial support.
Author information
Authors and Affiliations
Contributions
MB and MÖ designed and planned the study, MB performed the experiments, MO made statistical analysis, MB and MÖ wrote the manuscript. Authors have read and agreed with the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the Ethics Committee of the Istanbul University, Faculty of Medicine (protocol number 2019/19), and the ethical guidelines of the Declaration of Helsinki were followed.
Competing interests
The authors declared that they have no conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Benli, M., Özcan, M. Short-term effect of material type and thickness of occlusal splints on maximum bite force and sleep quality in patients with sleep bruxism: a randomized controlled clinical trial. Clin Oral Invest 27, 4313–4322 (2023). https://doi.org/10.1007/s00784-023-05049-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-05049-4