
Abstract
Objectives
The effect of combined orthodontic-orthognathic treatment was estimated, specifically the impact of pre-surgical orthodontic treatment, on oral health-related quality of life (OHRQoL).
Materials and methods
The research question was formulated using the PICO method. The search was carried out in MEDLINE via PubMed, CINAHL, psychINFO, Embase, and Cochrane (until February 3, 2020). Inclusion criteria were patients aged ≥ 17 years who underwent combined orthodontic-surgical treatment, quality of life assessment, and study design of randomized controlled trial, controlled clinical trial, prospective cohort study, observational study, intervention study, or cross-sectional study. The ROBINS-1 tool was used to assess the risk of bias within studies. A random effects meta-analysis was conducted when appropriate. The quality of evidence was assessed using the GRADE approach.
Results
Six studies were analyzed. The OHIP-14 and/or OQLQ-22 questionnaires were used to measure the OHRQoL. All six studies had a serious risk of bias. Two studies (87 participants) were included in a meta-analysis showing improvement of OHRQoL when comparing before and after treatment were compared (mean 14.85 scale points, 95% confidence interval 10.36;19.35).
Conclusions
Studies indicate a decrease in OHRQoL during the pre-surgical orthodontic treatment phase but improvement after orthodontic-orthognathic treatment. Data substantiating these results are limited, and the quality of evidence is low. Further research is needed to assess the impact of pre-surgical orthodontic treatment on the OHRQoL in an orthognathic trajectory.
Clinical relevance
Patients should be well informed about the effect facial/esthetic changes may have on their OHRQoL during sequential phases of orthodontic-orthognathic treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Malformation of the face and/or dentition can have a negative influence on the patient’s oral health-related quality of life (OHRQoL). Conditions such as crowded teeth, difficulties with food consumption, and temporomandibular joint problems may impact a person’s daily life through discomfort, pain, and embarrassment in public. In addition, problems with facial and/or dental esthetics can result in low self-esteem and low confidence [1]. These factors can be a reason for people to seek orthodontic-orthognathic treatment [2]. The patient has expectations about the result of orthodontic-orthognathic treatment, including improved function and/or esthetics.
In 2016, oral health was redefined by the FDI World Dental Federation: “multifaceted and includes the ability to speak, smile, smell, taste, touch, chew, swallow, and convey a range of emotions through facial expressions with confidence and without pain, discomfort, and disease of the craniofacial complex” [3]. To achieve these goals, the orthodontist and oral maxillofacial surgeon aim for the perfect dimensions and function of the face and dentition. The traditional patient perception that the specialist is always right and knows best is disappearing. The perspective and wish of patients today should be better understood and addressed by a team of specialists that also includes the patient to come to a shared decision. An objective understanding of the patient’s opinion can be derived from OHRQoL tools, such as validated questionnaires. A 2019 systematic review [4] based on this approach concluded that this treatment seems to improve the condition-specific OHRQoL, especially regarding social well-being, oral function, and facial esthetics. However, this systematic review had some methodological drawbacks.
Orthodontic-orthognathic treatment can be divided into three consecutive phases: (1) a pre-surgical phase, including start of (orthodontic) treatment; (2) a surgical phase; (3) a post-surgical orthodontic phase. In a so-called surgery first approach, a pre-surgical orthodontic phase is not included, and the post-surgical orthodontic phase may be extended. During the pre-surgical orthodontic phase, the orthodontist prepares the patient for surgery. For class II and class III cases, this sometimes involves extraction of two premolars, in the lower jaw and upper jaw, respectively. The maxillofacial surgeon sometimes requests an increased overjet in a Class II patient and a negative overjet in a class III patient. This means that, during this phase, the orthodontist actually increases the malocclusion, worsening patients’ pre-existing complaints [5, 6], which may result in a lower OHRQoL. The surgical phase is a short phase during which esthetics greatly change. These significant changes can have a mixed influence on the quality of life [2]. On one hand, the treatment meets expectations and may result in a better OHRQoL score. However, on the other hand, patients may face difficulties recognizing and accepting their changed appearance and/or may experience surgical complications and not be completely satisfied.
To assess the OHRQoL during orthodontic-orthognathic treatment, measuring moments are needed at the start of each phase and at the end of the treatment. This enables the measurement of possible fluctuations in OHRQoL during treatment and provides information that can be used to further personalize patient care. To the best of our knowledge, a systematic review summarizing the evidence regarding changes in OHRQoL during the pre-surgical orthodontic phase, surgical phase, and post-surgical orthodontic phase is lacking. Our research question was to establish the effect of all phases of the orthodontic-orthognathic treatment on OHRQoL, and more specifically the orthodontic part of orthognathic treatment.
Materials and methods
Protocol and registration
The protocol is registered in the International Prospective Register of Systematic Reviews, PROSPERO (https://www.crd.york.ac.uk/prospero/) under number CRD42018114539. The PRISMA checklist was used for reporting in this systematic review [7].
Eligibility criteria
The research question was formulated by means of the population, intervention, comparison, and outcome (PICO) method. The research question was whether patients > 17 years of age with a dentofacial deformity who underwent combined orthodontic-surgical treatment have improved OHRQoL, with special emphasis on the orthodontic part of the treatment. The components “patient” and “comparison” were not defined in the PICO formulation to avoid a too restrictive search (intervention: orthognathic treatment, outcome: OHRQoL).
The characteristics of the participants were age ≥ 17 years and combined orthodontic-surgical treatment, full treatment (orthodontic-surgical) from start until end, with evaluation of quality of life. The types of studies included in the review were randomized controlled trials (RCTs), controlled clinical trials, prospective cohort studies, observational studies, intervention studies, and cross-sectional studies.
The exclusion criteria were retrospective studies, case–control studies and case reports, research protocols, descriptive or systematic reviews, meta-analyses, studies of development and psychometric validation of questionnaires, congenital syndromes, obstructive sleep apnea syndrome, and systemic diseases relating to bone metabolism or maxillofacial region, cleft lip, and/or palate.
Information sources and search strategy
The search strategy was developed together with a senior health science librarian for different electronic databases. The following electronic databases were used: MEDLINE via PubMed, CINAHL, psychINFO, Embase, and the Cochrane Library. Grey literature was not searched. Full-text publications were obtained from licensed publishers. All articles published through October 2018 that met the search criteria, with no restrictions on language or article status, were included. Eventually, the search was updated until February 3, 2020.
The search strategy was developed for MEDLINE and adapted for the other databases. The search in PubMed was conducted as follows: ((“Self Concept”[MeSH] OR “Quality of Life”[MeSH] OR Quality of Life[tiab] OR HRQOL OR OHRQOL OR wellbeing OR “well-being” OR Self Concept* OR Self-Perception* OR Self Esteem* OR Psychosocial*)) AND (“Orthognathic Surgical Procedures”[MeSH OR “Orthognathic Surgery”[MeSH] OR “Jaw/surgery”[MeSH] OR “Osteotomy, Le Fort”[MeSH] OR “Osteotomy/methods”[MeSH] OR advancement osteotom* OR Genioplast* OR Mandibular Osteotom* OR Mandibular Reconstruction* OR Maxillary Osteotom* OR orthognathic*).
Study selection
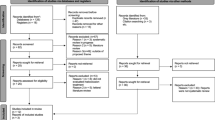
The study assessment was unblinded and performed independently by two reviewers (V.B. and A.W.). The search results from the five electronic databases were collected in EndNote X9 (2013, Clarivate Analytics, Philadelphia). Duplicates were removed. The articles were exported to the website covidence.org (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). In the Covidence software, screening was performed in two phases as shown in Fig. 1. First, studies were excluded based on title and abstract. The review team had three response options for excluding records or promoting them to the next stage: “yes,” “no,” and “maybe.” Secondly, the full-text of the remaining articles was assessed and the articles excluded if they did not meet the inclusion criteria. Furthermore, the references of the selected studies were hand-searched to identify any additional relevant studies. Disagreements were resolved by discussion with a third reviewer (E.O.).

PRISMA flow diagram of the study selection
Data items and data collection process
A data extraction form was developed and piloted in Covidence. Two reviewers (V.B. and A.W.) extracted the data from the included studies. Data were needed for orthodontic-orthognathic treatment from the start until the end of treatment. If disagreement existed, it was resolved through discussion with the third reviewer (E.O.). If the results were unclear or incomplete, the authors were contacted via email to gain complete datasets so that a meta-analysis could be performed.
Risk of bias in individual studies
The Risk of Bias in Non-randomized Studies – of Interventions (ROBINS-I) tool was used to assess the risk of bias of non-randomized studies of interventions [8]. Two reviewers (V.B. and A.W.) independently assessed the quality of the included articles and conflicts were solved through discussion with a third reviewer (E.O.). The ROBINS-I tool consists of seven domains, and each domain can be judged as having a low, moderate, serious, or critical risk of bias or no information. If at least one domain was assessed to be at serious risk of bias, the concerning study was defined as a study with a severe risk of bias.
Certainty of the evidence
We used the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) to assess the quality of a body of evidence [9]. The quality of evidence was rated per outcome as one of four categories: high, moderate, low, or very low.
Summary measures
Changes in means, standard deviation (SD), and 95% confidence intervals (CIs) for outcomes on validated (OHR) QoL questionnaires during orthodontic-orthognathic treatment were the primary outcomes. Validated questionnaires, such as the Oral Health Impact Profile (OHIP-14) and/or the Orthognathic Quality of Life Questionnaire (OQLQ-22) were preferred. The OHIP-14 [10] contains seven domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap. A total of 14 questions are scored using a 5-point Likert-type scale. Scores are clustered per domain with a score ranging from 0 to 56, and the mean score of all domains is considered the ‘total score’. The OQLQ [11, 12] contains four domains: facial esthetics, oral function, awareness of dentofacial deformity, and social relationship. A total of 22 questions are scored using a 5-point scale. Scores are clustered per domain with a score range of 0 to 88, and the mean score of all domains is considered the ‘total score’. For both questionnaires, a higher score corresponds with a lower OHRQoL.
Planned methods of analysis
First, we considered heterogeneity between the studies based on population, treatment, and age. Then we assessed heterogeneity between studies, using the I2 statistic and associated p value. As the presence of heterogeneity is not a simple dichotomy, we used relatively wide margins. An I2 > 50% is considered an indication of heterogeneity, as is a p value < 0.05. In either case, random effect models are used to calculate the overall effects and the source of heterogeneity is investigated. In absence of these indicators of heterogeneity, the mean difference is based on fixed effects analysis.
Risk of bias across studies
Specific time points are needed to determine changes in OHRQoL between different treatment phases. These time points are start of orthodontic-orthognathic treatment, before surgery; pre-surgical orthodontic phase; surgery; post-surgical orthodontic phase; and end of orthodontic treatment. When time points were not the same for each of the included studies, and studies did not report specific time points, there was a risk of bias of missing outcomes.
Additional analyses
Because of a lack of data from each of the included studies, further statistical analyses of all (sub)domains of the OHIP-14 and OQLQ were not performed except for the total OHIP-14 score between T0 and T3 (Fig. 2).

Forest plot of the change in mean OHRQoL scores between treatment start (T0) and end of treatment (T3) based on OHIP-14. The two trial arms in the study of Baherimoghaddam et al. (2016) were combined
Results
Study selection
The search of the five electronic databases yielded a total of 2903 articles. An overview of the study selection is presented in the flowchart in Fig. 1. After removing duplicate records, 2277 articles remained for screening. During the first round of screening, 2161 articles did not meet the inclusion criteria and were removed. The full-text was screened in the remaining 116 articles. One article was not available through the university library or other means and was excluded. At the end of the study selection process, six articles [5, 6, 14,15,16,17] were included in the systematic review. The excluded articles did not correspond with the criteria and were excluded based on wrong setting (n = 71), wrong study design (n = 35), wrong outcomes (n = 5), or wrong patient population (n = 2) (Supplementary Table 1). Two included articles were likely based on identical data [16, 18]. The corresponding author was contacted about the results of these two articles [16, 18] but did not respond. We excluded the article by Wang et al. [18] based on possibly using the same data as Huang et al. [16]. We processed this as a duplicate article in the identification phase.
Study characteristics
The six articles were longitudinal, prospective studies [5, 6, 14,15,16,17], and the details are summarized in Table 1. Antoun et al. [15] did not mention the study design, but the structure of the article corresponds to a prospective study. Ni et al. [6] presented their study results in graphs and accessory numerical data were lacking. Silvola et al. [17] did not present data from the orthodontic-orthognathic group and control group, but presented the total of these two groups.
Four of the six articles used the OHIP-14 questionnaire [5, 15,16,17], one used the OQLQ-22 [14], and one used both questionnaires [6]. The time during treatment when questionnaires were administered varied greatly. The duration and follow-up of the included studies differed. The duration of the observational period varied from a minimum of 12 months to a maximum of 19 months in surgery-first cases and a minimum of 22.9 months to a maximum of 41 months in orthodontics-first cases. All articles had a questionnaire administered both before and after combined orthodontic-surgical treatment.
The present systematic review included a total of 216 participants in the research group and 91 participants in control groups. The performed surgery differed among studies between a Le Fort 1 and/or bilateral sagittal split osteotomy (BSSO). However, the type of surgery was not always mentioned.
The primary outcome in six studies was change in the mean OHRQoL when using the OQLQ-22 and/or OHIP-14 for patients who underwent orthodontic-orthognathic treatment, from the start of preoperative orthodontic treatment and surgery to the end of postoperative orthodontic treatment. One article differentiated between surgery-first (no pre-surgical orthodontic phase) and orthodontics-first cases [16].
Evaluating the changes in OHRQoL and determining which phase has the greatest impact on the patient during treatment was difficult. Most studies did not measure this for each phase of combined orthodontic-orthognathic treatment. All six studies applied questionnaires at the start of treatment and after the completion of treatment. Only two studies [5, 14] used time points that enabled measurement of the mean change in OHRQoL during treatment, i.e., at the start of treatment, before surgery, after surgery, and end of treatment. However, different questionnaires were used. Alanko et al. [14] used the OQLQ-22 and Baherimoghaddam et al. [5] used the OHIP-14. The impact of orthodontic treatment in the pre-surgical orthodontic phase can be determined by comparing data from the start of treatment to data from a time point just before surgery. Three articles mention these specific time points: Alanko et al. [14], Baherimoghaddam et al. [5], and Ni et al. [6]. Because Silvola et al. [17] did not mention numerical data, the authors were contacted. Authors from other articles were also contacted to obtain missing data. We received SPSS files from Alanko et al. [14], but no complete datasets were provided, so no statistics could be performed for the requested time points in this systematic review. Ni et al. [6] and Silvola et al. [17] did not respond to repeated requests.
Risk of bias within studies
The ROBINS-I tool was used to assess individual risks of bias as summarized in Table 2 [8]. All six articles were rated as severe risk of bias [5, 6, 14,15,16,17]. In each study, participants were already selected and underwent both orthodontic and surgical treatment. No randomization was applied, as specific treatments cannot be carried out for research purposes only, which makes any type of randomization ethically unacceptable. During the treatment, there were some missing data because not all patients completed the questionnaires at each time point. Reasons for missing data were not always mentioned [5, 14, 17].
Certainty of the evidence
The GRADE tool was used to assess the certainty of evidence for the outcome OHRQoL (Table 3). Evidence from observational studies started as low quality of evidence. The quality of evidence for all stages of the combined orthodontic-surgical treatment was assessed as very low due to limitations in the studies. This means we have low confidence in the effect estimate; the true effect is likely to be substantially different from the estimated effect.
Synthesis of results
Our research question was to establish the effect of all phases of the orthodontic-orthognathic treatment on OHRQoL, more specifically of the orthodontic part of an orthognathic treatment. Antoun et al. [15] and Baherimoghaddam et al. [5] were the only two studies that reported workable data to perform a meta-analysis. Descriptive statistics were further used to expound the results per treatment phase in the other four studies in Table 1.
The results of the articles were divided according to the four phases of treatment. The first phase (T1-T0) involves the pre-surgical orthodontic phase from the start of treatment (T0) to shortly before surgery (T1). The second phase (T2-T1) involves the time period from shortly before surgery (T1) until shortly after surgery (T2). The third phase (T3-T2) involves the post-surgical orthodontic phase, from shortly after surgery (T2) until the end of the post-surgical orthodontic-orthognathic treatment (T3). The fourth phase involves the complete treatment (T3-T0), from the start of treatment (T0) to the completion of treatment (T4). For each phase, only the articles that described the concerning phase were included in the synthesis of the results.
Pre-surgical orthodontic phase (T0-T1)
Two of the six articles evaluated the pre-surgical orthodontic phase [5, 6]. Baherimoghaddam et al. [5] used the OHIP-14 for patients with a class II and class III malocclusion. In the class II group, overall OHIP-14 scores showed significant deterioration of OHRQoL from T0 to T1 (mean + 3.71, SD 4.32, p = 0.002). Significant deterioration was reported for the following three subdomains: functional limitations (mean + 0.78, SD 1.75, p = 0.024), physical disability (mean + 0.86, SD 2.21, p = 0.044), and psychological disability (mean + 1.10, SD 1.87, p = 0.010). Class III patients showed a significant increase in psychological discomfort (mean − 2.00, SD 1.51, p < 0.001), physical disability (mean + 0.77, SD 1.48, p = 0.013), psychological disability (mean − 0.70, SD 1.37, p = 0.014), and overall OHIP-14 (mean -2.03, SD 4.85, p = 0.029). Ni et al. [6] combined the orthodontic-orthognathic group with the orthodontic group and found an increase in OHIP-14 scores, i.e., a deterioration of OHRQoL, but it was not significant. For the OQLQ, they found a significant decrease in OHRQoL in the first phase in overall score (p < 0.001), oral function (p < 0.05), and facial esthetics (p < 0.01). Awareness of dentofacial esthetics and social aspects of dentofacial deformity decreased, but not significantly. The results of both studies show a worsened OHRQoL during the first phase of orthodontic-orthognathic treatment.
Second phase from shortly before surgery until shortly after surgery (T1-T2)
None of the studies reported statistical outcomes for shortly before surgery to shortly after surgery (T1-T2). Two articles reported OHRQoL results at T1 (before surgery) until after surgery. Ni et al. [6] specified “after surgery” as 6–8 months after surgery or the end of treatment. This means that the exact time point used to determine OHRQoL after surgery was ambiguous. Baherimoghaddam et al. [5] measured the OHRQoL before and after surgery but did not register numerical changes or whether a significant change occurred in this phase of the treatment. For class II patients, the mean overall OHIP-14 was 22.84 (SD 3.40) at T1 and 8.64 (SD 3.21) at T2. For class III patients, the mean overall OHIP-14 was 17.63 (SD 3.83) at T1 and 6.71 (SD 2.45) at T2.
Post-surgery orthodontic phase(T2-T3)
One study reported OHRQoL changes in the post-surgery orthodontic phase [5]. Changes were reported for both class II and class III groups. “After surgery” was specified as 6 months after surgery to 12 months after debonding, resulting in a time period instead of a fixed time point. Class II patients presented significant improvement in scores for physical pain (mean − 0.50 SD 1.17, p = 0.003) and physical disability (mean − 0.61, SD 1.37, p = 0.028). The class III patients had no significant improvement in any domain.
Complete treatment period (T0-T3)
Five studies presented the changes between the start and end of treatment [5, 6, 14,15,16]. Alanko et al. [14] measured changes using the OQLQ-22 and found significant improvement in the OHRQoL (total score: mean − 22.72, range − 61.00 to 4.00, p < 0.001). According to Antoun et al. [15], all of the domains of the OHIP-14 improved significantly. The largest effect was measured in the domain of psychological discomfort. Baherimoghaddam et al. [5] reported significant improvement for class II and class III patients in all individual OHIP-14 domains. According to Ni et al. [6], OHRQoL improved significantly using the OHIP-14 or OQLQ-22. Furthermore, Silvola et al. [17] reported that all individual domains in OHIP-14 improved significantly. Based on all study results, patients’ OHRQoL improved significantly in this treatment phase.
Figure 2 shows the results of the meta-analysis of the difference in OHIP-14 scores between the start and end of treatment. Antoun et al. [15] included 29 participants and Baherimoghaddam et al. [5] included 28 class II patients and 30 class III patients. We combined the two trial arms from the study of Baherimoghaddam et al. [5] for the overall analysis. There was a large effect of treatment on the overall OHRQoL for patients who underwent orthodontic-orthognathic treatment, and both studies showed similar improvement in the OHRQoL. The overall results showed a significant increase in OHRQoL. Antoun et al. [15] showed a higher decrease (− 17.48 scale points) in the overall score compared to the decrease (− 12.85 scale points) in OHRQoL reported by Baherimoghaddam et al. [5]. We considered the heterogeneity between these two studies. Both investigated OHRQoL in patients who underwent orthodontic-orthognathic treatment. The patient group of Antoun et al. is younger and Baherimoghaddam et al. mentioned type of surgery. This in itself is already a reason to consider these studies to be heterogeneous.
Huang et al. [16] reported overall improvement in OHRQoL in the surgery-first and orthodontics-first groups. The results show an immediate improvement in OHRQoL after surgery. The surgery-first group scored consistently lower.
Improvement in OHRQoL expressed as percentages
In the included studies, the OHIP-14 and/or OQLQ were used to measure OHRQoL. To compare OHRQoL improvements between the included studies, we calculated improvements in OHRQoL as percentages of the initial OHRQoL (Table 4). The percentages reflect deterioration or improvement per phase of orthodontic-orthognathic treatment. Each phase showed improvement except the first phase, as the pre-surgical orthodontic phase had deteriorated OHRQoL. Alanko et al. [14] showed minimal improvement compared to Baherimoghaddam et al. [5]. The greatest improvement in OHRQoL during phase 3 was found by Alanko et al. [14]. Baherimoghaddam et al. [5] investigated the OHRQoL of class II and class III patients who sought orthodontic-orthognathic treatment. Class II patients had significant deterioration in OHRQoL during the orthodontic phase because of the required dental compensation pre-surgically.
Huang et al. [16] investigated surgery-first vs. surgery with pre-surgical orthodontics. In both types of treatment approaches, the OHRQoL improved. The average treatment duration was shorter in surgery-first cases. The mean treatment duration was 16.6 + 2.4 month for surgery-first and 25.3 + 2.4 month for orthodontics-first groups. The satisfaction of patients in the surgery-first group was relatively high.
Risk of bias across studies
Due to incomplete data, it was not possible to assess the risk of bias across studies.
Discussion
Summary of evidence
The overall OHRQoL greatly improved after orthodontic-orthognathic treatment in the included studies [5, 6, 14,15,16,17] and an earlier systematic review [4]. This improvement is also shown in Table 4 for phases 2, 3, and 4. However, this improvement may be substantially different from the estimated effect, as shown by the very low certainty of the evidence assessed by the GRADE (Table 3) in the present review. We included six studies but performed a meta-analysis of two studies comprising 87 patients [5, 15]. All studies showed a high risk of bias. This improvement in OHRQoL is not linear from the start to the end of treatment. Multiple studies reported obvious changes in the patients’ OHRQoL during treatment [4]. The pre-surgical orthodontic phase had a negative influence on the OHRQoL (Table 4, phase 1), which is the only phase that showed deterioration of OHRQoL in the orthodontic-orthognathic trajectory. During this phase, orthodontic treatment was started to prepare the patient for surgery, and this preparation often takes quite some time. This relatively long treatment phase causes discomfort because the malformation is enhanced and the patient’s pre-existing complaints tend to worsen, which has a negative psychological impact [5, 6]. Cunningham et al. [19] studied the influence of pre-surgical orthodontic treatment on OHRQoL. We did not include this study because they only studied the first phase of an orthodontic-orthognathic treatment, but the results show an opposing view in the differences between quality of life at T0 and T1. Their results showed that the impact of this phase is negligible, which contradicts the results of Huang et al. [16], Baherimoghaddam et al. [5], Ni et al. [6], and Alanko et al. [14]. It seems that surgery improves the OHRQoL immediately within the short period of time of the orthognathic phase. Only Alanko et al. [14] and Baherimoghaddam et al. [5] presented numerical data for this phase, and Baherimoghaddam et al. [5] showed great improvement directly after surgery. Patients see immediate positive changes after surgery; thus, the surgical period is relatively short and associated with positive changes, whereas the pre-surgical orthodontic phase takes a long time and is associated with negative changes in OHRQoL. However, these results should be interpreted with caution because these studies still exhibited high heterogeneity, had a small sample size, did not have the same measurements points throughout treatment, or lacked complete datasets [6, 14, 17].
Various tools were used to assess OHRQoL in the studies included in this review, most commonly the OHIP-14 and OQLQ-22 questionnaires. These two differ in the type and number of questions and domains. However, the questionnaires have the same outcome because they both measure the impact of deformities on patients’ OHRQoL. Furthermore, both questionnaires assess esthetic and functional aspects [20]. The OQLQ is a condition-specific questionnaire for dentofacial deformities, and the OHIP-14 is more generally oral health-related and more directed to the teeth and mouth. Depending on the aims of the individual studies, authors decided on one of these questionnaires to measure OHRQoL. Since the included studies in this review used different questionnaires to measure OHRQoL and the results were presented in different ways, an accurate comparison of the included studies was not always possible.
Only one study (n = 50) compared surgery first versus pre-surgical orthodontic treatment [16], and this study had a high risk of bias according to the ROBINS-I tool. Therefore, the results should be interpreted with caution. The total treatment time of surgery-first cases is supposed to be shorter, not only because of the absence of a pre-operative orthodontic phase, but also because the malocclusion after surgery facilitates orthodontic tooth movement in the post-surgical treatment phase [16]. In the surgery-first approach, there is no pre-operative orthodontic phase to measure and the post-operative orthodontic phase is similar to that of the orthodontics-first approach. Patients will see immediate improvements in their facial esthetics and facial profile in an early stage of treatment when they are treated according to the surgery-first approach. This will positively affect the OHRQoL [16, 21]. This early shift of the patients’ OHRQoL towards the final improved scores may give precedence to the surgery-first approach over the orthodontics-first approach. However, the evidence presented is of low quality; therefore, more research is needed on OHRQoL in surgery-first approaches. Furthermore, a surgery-first approach is not always applicable or possible. The orthodontist and surgeon should communicate well to assess whether a surgery-first approach is possible and whether it will result in a shorter treatment time. The treatment time could affect OHRQoL, but this variable is not evaluated in this review.
An important impediment to systematic analysis was that not all studies reported results at all time points. Either a systematic review design includes studies that report only on select phases and not on all phases, as in the systematic review by Yi et al. [4], or only includes studies that report on all phases, perhaps missing study outcomes of studies not reporting on all phases. In this study, we chose the latter approach, and studies were only included if they concerned the entire combined orthodontic-orthognathic treatment and the different phases of this treatment were clearly described. Sometimes, it was unclear if the study was started before the orthodontic-orthognathic treatment or only before surgery. These were reasons for exclusion, resulting in fewer articles in this systematic review than in the review by Yi et al. [4].
Questionnaires were mostly completed at the start and end of treatment, but not shortly before or after surgery. This makes it difficult to explain the changes in OHRQoL and to determine which treatment phase has the greatest impact on patients’ OHRQoL. Only two studies had complete numerical datasets [5, 14] and studied the three phases of an orthodontic-orthognathic treatment. It is important to start with the evaluations before the first appointment. The patient’s opinion can change after the first appointment with the orthodontic-surgical team, when they receive further information from the professionals. Furthermore, it is important to longitudinally follow the same patients from the start to end of treatment instead of comparing OHRQoL for different groups of patients in different treatment phases. Longitudinal analysis will reduce the risk of bias in study results. This is a drawback of an earlier systematic review [4] that included every study regardless of the longitudinal follow-up.
It is important to inform the patient about the different phases of orthodontic-orthognathic treatment and the facial/esthetic changes that will occur during treatment. The results show that the pre-surgical orthodontic treatment tends to negatively impact the patient’s OHRQoL (Table 4) [5, 6, 14]. During the first appointment, patients should get the correct information about the first phase of the combined orthodontic-orthognathic treatment. It is difficult to properly inform and prepare a patient for this stressful treatment phase because it is difficult to estimate how the patient will react to the facial changes during this treatment. Despite these difficulties, informing and explaining will help prepare the patient for the expected changes in order to regulate the impact on psychological wellbeing [22, 23]. Professional counseling during the pre-surgical orthodontic treatment phase may help reduce the negative impact of this phase on the patient’s OHRQoL. The literature suggests that pre-treatment information should be improved [23]. Kettle et al. [22] studied the effects of an online information resource for patients, and Bergkulla et al. [23] evaluated the effects of an information clinic for patients on their preparedness for orthodontic-orthognathic treatment. It is easy to provide objective information to patients, but it is hard to predict how patients will experience specific changes, and this may also be subject to further investigation by OHRQoL measures to determine whether the fluctuations in OHRQoL during combined orthodontic-orthognathic treatment can be positively influenced by improving the provided information.
Limitations
We were not able to include RCTs because none were published on the subject of OHRQoL in orthodontic-orthognathic patients. However, not all clinical questions can be studied in a RCT design. In surgical trials, it is often unethical to randomize the patients. The studies we were able to include had a serious risk of bias in certain domains of the ROBIN-I tool, mainly due to domain 2, patient selection. Authors did not always report reasons for loss to follow-up. Another limitation is in domain 6, the type of measurement outcome, which is subject to patients’ expectations. Most patients expect that their OHRQoL will improve and, because of that, will see improvement. Patients could be influenced by certain expectations because of the impossibility of performing a blind measurement.
Another factor that impeded the comparison of results from the included studies is that the measured time points throughout the complete treatment course were not identical between studies. Only OHRQoL before the start of the orthodontic treatment phase and the end of treatment were comparable between studies. However, all intermediate time points were defined differently between studies and may be the reason for bias.
Finally, two different questionnaires were used to measure OHRQoL in the included studies. This complicated the comparison of outcomes between studies.
Recommendations for future research
The low quality of evidence in this review shows that there is a need for more research. To understand the fluctuations of OHRQoL during combined orthodontic-orthognathic treatment, assessment of OHRQoL in a standardized manner is recommended, with well-defined time points and validated and relevant questionnaires to combine results from multiple studies. Studies should report numerical data for mean, standard deviation, and change with standard deviation for all time points, and each phase should be well-defined.
Conclusions
The results of this systematic review point to a decrease in OHRQoL during the pre-surgical orthodontic treatment phase and improvement after orthodontic-orthognathic treatment, but limited data were available to substantiate these results and the quality of the evidence is low. More standardized quality of life research in the orthodontic-orthognathic treatment field is needed.
References
Silva I, Cardemil C, Kashani H, Bazargani F, Tarnow P, Rasmusson L, Suska F (2016) Quality of life in patients undergoing orthognathic surgery - a two-centered Swedish study. J Craniomaxillofac Surg 44(8):973–978. https://doi.org/10.1016/j.jcms.2016.04.005
Oland J, Jensen J, Elklit A, Melsen B (2011) Motives for surgical-orthodontic treatment and effect of treatment on psychosocial well-being and satisfaction: a prospective study of 118 patients. J Oral Maxillofac Surg 69(1):104–113. https://doi.org/10.1016/j.joms.2010.06.203
Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, Weyant RJ (2016) A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. Int Dent J 66(6):322–324. https://doi.org/10.1111/idj.12294
Yi J, Lu W, Xiao J, Li X, Li Y, Zhao Z (2019) Effect of conventional combined orthodontic-surgical treatment on oral health-related quality of life: a systematic review and meta-analysis. Am J Orthod Dentofacial Orthop 156(1):29–43. https://doi.org/10.1016/j.ajodo.2019.03.008
Baherimoghaddam T, Tabrizi R, Naseri N, Pouzesh A, Oshagh M, Torkan S (2016) Assessment of the changes in quality of life of patients with class II and III deformities during and after orthodontic-surgical treatment. Int J Oral Maxillofac Surg 45(4):476–485. https://doi.org/10.1016/j.ijom.2015.10.019
Ni J, Song S, Zhou N (2019) Impact of surgical orthodontic treatment on quality of life in Chinese young adults with class III malocclusion: a longitudinal study. BMC Oral Health 19(1):109. https://doi.org/10.1186/s12903-019-0782-9
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7). https://doi.org/10.1371/journal.pmed.1000100
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan AW, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JP (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 12:355. https://doi.org/10.1136/bmj.i4919
GRADE working group, From evidence to recommendations – transparent and sensible, https://www.gradeworkinggroup.org/.
Slade GD (1997) Derivation and validation of a short-form oral health impact profile. Community Dent Oral Epidemiol 25:284–290. https://doi.org/10.1111/j.1600-0528.1997.tb00941.x|
Cunningham SJ, Garratt AM, Hunt NP. Development of a condition-specific quality of life measure for patients with dentofacial deformity: I. Reliability of the instrument. Community Dent Oral Epidemiol. 2000 Jun;28(3):195–201. https://doi.org/10.1034/j.1600-0528.2000.280305.x|
Cunningham SJ, Garratt AM, Hunt NP. Development of a condition-specific quality of life measure for patients with dentofacial deformity: II. Validity and responsiveness testing. Community Dent Oral Epidemiol. 2002 30(2):81–90. https://doi.org/10.1034/j.1600-0528.2002.300201.x|
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, Norris S, Falck-Ytter Y, Glasziou P, DeBeer H, Jaeschke R, Rind D, Meerpohl J, Dahm P, Schünemann HJ. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011 64(4):383–94. https://doi.org/10.1016/j.jclinepi.2010.04.026
Alanko O, Tuomisto MT, Peltomäki T, Tolvanen M, Soukka T, Svedström-Oristo AL (2017) A longitudinal study of changes in psychosocial well-being during orthognathic treatment. Int J Oral Maxillofac Surg 46(11):1380–1386. https://doi.org/10.1016/j.ijom.2017.05.004
Antoun JS, Fowler PV, Jack HC, Farella M (2015) Oral health-related quality of life changes in standard, cleft, and surgery patients after orthodontic treatment. Am J Orthod Dentofacial Orthop 148(4):568–575. https://doi.org/10.1016/j.ajodo.2017.06.018
Huang S, Chen W, Ni Z, Zhou Y (2016) The changes of oral health-related quality of life and satisfaction after surgery-first orthognathic approach: a longitudinal prospective study. Head Face Med 5(12):2. https://doi.org/10.1186/s13005-015-0098-1
Silvola AS, Rusanen J, Tolvanen M, Pirttiniemi P, Lahti S (2012) Occlusal characteristics and quality of life before and after treatment of severe malocclusion. Eur J Orthod 34(6):704–709. https://doi.org/10.1093/ejo/cjr085
Wang J, Chen W, Ni Z, Zheng M, Liang X, Zheng Y, Zhou Y (2017) Timing of orthognathic surgery on the changes of oral health-related quality of life in Chinese orthognathic surgery patients. Am J Orthod Dentofacial Orthop 151(3):565–571. https://doi.org/10.1016/j.ajodo.2016.06.050
Cunningham SJ, Gilthorpe MS, Hunt NP (2001) Are pre-treatment psychological characteristics influenced by pre-surgical orthodontics? Eur J Orthod 23(6):751–758. https://doi.org/10.1093/ejo/23.6.751
Lee S, McGrath C, Samman N (2007) Quality of life in patients with dentofacial deformity: a comparison of measurement approaches. Int J Oral Maxillofac Surg 36(6):488–492. https://doi.org/10.1016/j.ijom.2007.01.011
Peiró-Guijarro MA, Guijarro-Martínez R, Hernández-Alfaro F (2016) Surgery first in orthognathic surgery: A systematic review of the literature. Am J Orthod Dentofacial Orthop 149(4):448–462. https://doi.org/10.1016/j.ajodo.2015.09.022
Kettle J, Marshman Z, Benson PE et al (2017) How do patients perceive the British orthodontic society online information resource about orthognathic treatment? A qualitative study J Orthod 44(3):174–182. https://doi.org/10.1080/14653125.2017.1349057
Bergkulla N, Hänninen H, Alanko O et al (2017) Introduction and assessment of orthognathic information clinic. Eur J Orthod 39(6):660–664. https://doi.org/10.1093/ejo/cjx025
Author information
Authors and Affiliations
Contributions
V.E.H.W. Brouns contributed to the study design, data acquisition, analysis, interpretation, and drafting the manuscript. A.M.L. de Waal contributed to data acquisition, interpretation, and drafting the manuscript. E.M. Bronkhorst contributed to the study design, statistical analysis, data interpretation, and drafting the manuscript. A.M. Kuijpers-Jagtman contributed to data interpretation and drafting the manuscript. E.M. Ongkosuwito contributed to the study conception, design, data interpretation, and drafting the manuscript. All authors critically revised the manuscript and gave final approval and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Brouns, V.E.H.W., de Waal, AL.M.L., Bronkhorst, E.M. et al. Oral health-related quality of life before, during, and after orthodontic-orthognathic treatment: a systematic review and meta-analysis. Clin Oral Invest 26, 2223–2235 (2022). https://doi.org/10.1007/s00784-021-04288-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-021-04288-7