
Abstract
Objectives
This in vivo study aimed to compare the marginal discrepancies of zirconia copings manufactured on the basis of two direct intraoral scanning systems and the indirect digitization of a conventional impression.
Materials and methods
A total of 63 teeth in 23 patients were prepared to receive full-coverage crowns. Subsequently, these teeth were intraorally scanned using CEREC AC Omnicam and Cara TRIOS and a conventional impression was taken with the scannable PVS Flexitime Fast & Scan. The conventional impression was then extraorally digitized using a D700 laboratory scanner. The zirconia copings were manufactured on the basis of the resulting datasets. Silicone replicas of the copings were produced and sectioned for the measurement of the marginal discrepancy under a digital microscope.
Results
The statistical analysis showed no significant differences between the two intraoral scanners, the CEREC AC Omnicam (86.09 μm ± 61.46 μm) and the Cara TRIOS (88.95 μm ± 54.46 μm). However, the discrepancies of the zirconia copings obtained from the laboratory scans of conventional impressions (143.29 μm ± 100.71 μm) showed significant differences. Both intraoral scanners achieved a marginal discrepancy below 100 μm, whereas the laboratory scan exhibited considerably higher values.
Conclusions
The intraoral scanners tested allow for the production of single-tooth-restorations with an adequate marginal fit, whereas the production of restorations on the basis of the scan of a conventional impression led to vast marginal gaps.
Clinical relevance
The method of digitizing a conventional impression using a laboratory scanner seemed to have reached its limits in the clinical environment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Intraoral scanning systems are increasingly gaining importance in the CAD/CAM (computer-aided design/computer-aided manufacturing) production of high-resistance all-ceramic restorations, especially regarding single-tooth restorations and short span-bridges. The high acquisition costs are further hindering clinicians from purchasing intraoral scanning systems. Therefore, conventional impression techniques are still used for the majority of impressions performed in a clinical setting. The standard procedure for achieving the implementation of the CAD/CAM method in this setting is by scanning the plaster model resulting from the conventional impression by using a laboratory scanner [1]. However, mainly due to gypsum expansion, the model casting process is highly prone to error. The direct laboratory scan of the conventional impression, which is one work-step ahead in the conventional workflow, could be an approach to eliminate the entire model casting process and may be thus promising for reducing the overall error and therefore improving the fitting accuracy of restorations.
The marginal fit of the restoration is one of the main factors that determine the longevity of the restoration and its overall success [2]. In the oral environment, an inadequate marginal fit can lead to the dissolution of the cement film [3]. Subsequent plaque accumulation [4] can facilitate the development of periodontitis and [5] secondary caries [6], as well as microleakage and, as a consequence, endodontic inflammation of the tooth [7]. McLean and Fraunhofer stated that the marginal gap of a restoration should not exceed 120 μm [8]. Although there have been other investigations demanding values below 50 μm [9], the most recent studies mainly rely on the data of McLean and Fraunhofer [10].
A variety of factors can lead to an inadequate marginal fit of a restoration. Impressions that use an elastomeric material such as vinylpolysiloxane are a standard procedure in the conventional workflow, and the literature shows that a sufficient accuracy is achievable with conventional impression techniques [11,12,13]. However, a multitude of errors can occur in the intraoral phase and during laboratory procedures due to the high level of sensitivity of the technique and its dependence on material properties [14].
Recent investigations show a higher fitting accuracy in vivo with an all-digital workflow using direct intraoral digitization systems, such as Lava COS (3 M, St. Paul, USA) [15], CEREC (Sirona, Bensheim, Germany) [16], Cara TRIOS (Heraeus, Hanau, Germany) [17], and iTero (Align Technology, Amsterdam, Netherlands) [18]. One of the major drawbacks of these systems is that they are not able to record areas that are not fully optically accessible. However, this is also true for conventional impression techniques that also require a moisture-free and accessible preparation margin for successful impression. In these situations, further methods such as surgical crown lengthening may be necessary.
To our knowledge, the accuracy of the indirect approach by scanning the elastomeric impression has only been sparsely investigated. Thus far, this method of indirect digitization has shown acceptable outcomes in vitro [19,20,21,22] that are comparable to those of direct intraoral scanning, but no in vivo investigations have been published.
The following null hypothesis was tested: There is no significant difference between the marginal fit of restorations that are manufactured on the basis scans obtained from two established intraoral scanners and those that are manufactured on the basis of a laboratory scan of a conventional impression in vivo.
Materials and methods
This study was conducted at the Department of Prosthodontics of the Justus-Liebig-University in Giessen, Germany. A total of 63 teeth in 23 patients (12 females and 11 males; ages 50 to 84 years) were included in this study. The inclusion criteria included the indication for a crown restoration (crowns, bridges, and telescopic crowns), an asymptomatic tooth, and a visible finish line. Exclusion criteria included unstoppable bleeding, an inability to keep the area dry, and an indistinguishable finish line. Additionally, all of the subjects who were included gave their written consent after being informed of the aims and the procedure of the study. The study protocol was approved by the Ethics Committee of the Justus-Liebig-University in Giessen, Germany (267/13), and was registered in the German Clinical Trial Register (DRKS00009371).
Clinical procedures
All of the patients were given local anesthesia for the preliminary treatment of the abutment teeth, which included, if necessary, excavation of caries and adhesive build-ups (Optibond FL, Kerr, Rastatt, Germany; Rebilda LC blue, Voco, Cuxhaven, Germany). A chamfer finish line was prepared with diamond burs with rounded edges and polished with a fine diamond bur according to generally accepted guidelines [23]. Afterwards, the provisional restoration preparation (Luxatemp, DMG, Englewood, USA) was made and was temporarily cemented (Temp Bond, Kerr, Rastatt, Germany).
A conventional impression and two intraoral scans were taken 7–10 days after the preparation to allow for possible injuries of the gingiva caused by the preparation to heal. To ensure a sufficient retraction of the gingiva and in order to prevent bleeding, intrapapillary anesthesia (Ultracain, Sanofi-Aventis, Frankfurt am Main, Germany) was administered and retraction cords, which were soaked in 25% alumina sulfate (Orbat sensitive, lege artis, Dettenhausen, Germany), were placed in the sulcus prior to each impression (Ultrapak, Ultradent, South Jordan, USA). The double cord technique was employed, meaning that one smaller cord was plugged deep into the sulcus beneath the finish line and one larger cord was plugged right above it. The latter was then removed for the scanning procedure, while the previous cord remained in the sulcus in order to prevent the gingiva from collapsing during the procedure. Dry tips and disposable soft tissue retractors for cheeks and lips (Optragate, Ivoclar Vivadent, Schaan, Liechtenstein) were used to keep the scanning area dry at all times. Two intraoral scans were conducted using different powder-free intraoral scanners (CEREC AC Omnicam, Sirona, Bensheim, Germany; Cara TRIOS, Heraeus Kulzer, Hanau, Germany) in a randomized order. The manufacturer’s scanning protocols were abided by at all times. Before proceeding to the conventional impression, the data that were captured were checked for artifacts. The resulting files were exported from the intraoral scanners and, if necessary, converted into stl format (CrossManager, Datakit, Lyon, France). All scans and impressions were performed by the same calibrated dentists (P.B.). Prior to the study, the operator was trained by the respective manufactures and supervised by the senior authors (P.R. and B.W.). Before starting the study it was ensured that the operator had performed a minimum of 30 scans per system.
The conventional impression was always taken after the intraoral scanning procedure was completed so that the retraction measures would not be compromised. Perforated metal stock trays were used. The handles had to be shortened by approximately 3 cm beforehand in order for the trays to fit in the laboratory scanner without disrupting the scanning process. After varnishing the metal stock trays with a tray adhesive, a two-step putty-wash technique was implemented using a scannable VPS (Flexitime Fast & Scan Putty and Light Flow, Heareus Kulzer, Hanau, Germany). The remaining retraction cord was removed just before applying the washing material so that the cord would not get impacted in the impression. The impression material was given 3:30 min to set, as recommended by the manufacturer. All of the impressions were disinfected and then sent to a dental technician laboratory.
For each tooth included in the study, three zirconia copings were manufactured, resulting in a total of 189 copings.
Laboratory procedures
In the dental technician laboratory, all of the undercuts of the conventional impressions were trimmed without harming the prepared teeth. Undercuts directly below the preparation margin are in general small feather-edges of less than a millimeter. These were not removed in order not to destroy the impression.
Thereafter, the conventional impression was digitized by a trained dental technician using an automated laboratory scanner (D700, 3Shape, Copenhagen, Denmark). The resulting files were sent back to the department, where they were converted into stl file format (CrossManager, Datakit, Lyon, France).
The conventional impression and the intraoral scans each resulted in one stl-dataset per tooth. These were sent to a dental laboratory (Dentallabor Kappert, Essen, Germany) for design and manufacturing of the zirconia copings. The design parameters were set at 65 μm for the cement gap, 600 μm for the overall layer thickness and 200 μm for the edge reinforcement (ExoCAD, Darmstadt, Germany). These parameters were identified in a laboratory conducted series of systematic pretests with different values for the cement gap, the overall layer thickness, and the edge reinforcement to deliver optimal results for the marginal fit of each impression system.
All of the copings were milled from pre-sintered zirconia blocks (Copran Zr, White Peaks, Wesel, Germany) by means of a 5-axis milling machine (DWX 50, Roland, Irvine, USA). After sintering at 1500 °C, the copings were sent back to the dental operatory for try-in.
Thereafter the conventional impression was poured with type IV plaster and further used for the production of the intended restoration for the patient. For scientific clearness, we only compared the three zirconia copings and left out the final restoration.
Replica technique
The marginal fit of the copings was determined by means of the replica technique. After removing the provisional crown, the abutment teeth were thoroughly cleaned. Before implementing the replica technique, the initial fit of the coping was checked visually. If it was not possible to seat the coping on the tooth, a low viscosity silicone (Fit Test C&B, Voco, Cuxhaven, Germany) was used as fit-checker and up to 3 adjustments using a fine diamond bur (25 μm grain size) were made. For the replica technique, the copings were filled with a low-viscosity silicone (Fit Test C&B, Voco, Cuxhaven, Germany), seated on the preparation and held in place with maximum finger pressure for 3 s, simulating the clinical cementation of the crown. After 2 min of setting time, the coping was removed from the tooth. For this purpose, it was crucial that the resulting thin layer of silicone remained adhered to the inner surface of the coping and did not tear when removed. If this was not achieved, the procedure was repeated. Afterwards, the lumen of the coping was filled with another low viscosity silicone, stabilizing the first layer and mimicking the tooth. After the silicone had set, the replica was carefully removed from the coping and sectioned. Using a sharp scalpel, one cut was made mesio-distally, and one was made buco-orally, resulting in four sections. The samples were embedded in putty-mass (Giroform Putty, Amann Girrbach, Pforzheim, Germany) on a microscope slide and adjusted horizontally with a parallel-press. The measurements were conducted using a digital microscope (Smartzoom5, Zeiss, Jena, Germany) at × 200 magnification. Image analysis software was used to measure the marginal discrepancy (the shortest distance from the margin of the coping to the abutment surface closest to the finish line), which was performed in accordance with the procedure described by Holmes et al. (Fig. 1). All of the replicas were prepared and all of the measurements were made using the same calibrated operator. The measurements were recorded in microns and exported to a spreadsheet.

Replica at × 200 magnification, (1: tooth, 2: coping, 3: cement gap, 4: marginal discrepancy)
Statistical procedures
Based on the data of Boeddinghaus et al. [24], a sample size of approximately 60 specimens was calculated for achieving a power of 80%. The statistical analysis was carried out using SPSS (22, IBM Statistics, Armonk, USA). The level of significance was set at α = 0.5%. Because of dependencies within the variables, a random-intercept model was applied. The mixed procedure was calculated with logarithmic values in order to determine estimations with approximately normally distributed residuals. The Levene test was applied to check for variance homogeneity. In the case of a significant F-test when testing the four-staged factor “type of tooth,” pairwise comparisons of the estimated margins, which were corrected for multiple testing (Sidak), were interpreted. The mean values and standard deviations were reported.
Results
In total, 63 teeth from 23 patients were examined. Thirty-three teeth were situated in the upper jaw, and 29 in the lower jaw. Altogether, 16 incisors, 22 canines, 16 premolars, and 9 M were analyzed. Only six copings initially needed adjustments. However, no visually acceptable fit could be achieved and therefore, these six copings could not be tested: one based on the data of CEREC and five based on the data of the impression scan. The mean values of all of the methods were tested and compared. The marginal discrepancies were 86.09 μm (± 64.46 μm) for CEREC AC Omnicam, 88.95 μm (± 54.46 μm) for Cara TRIOS, and 143.29 μm (± 100.71 μm) for the impression scan (Fig. 2). Significant differences could be established between the laboratory scan and the two intraoral scanners (p < 0.05). The comparison of the different types of teeth (Table 1) showed no significant differences within each acquisition method (p > 0.05). Therefore, the null hypothesis was rejected.

Boxplot diagram of the impression methods
Discussion
This study aimed at measuring and comparing the marginal fit of all-ceramic restorations fabricated from three different impression systems, two direct and one indirect. The focus of this investigation was on the indirect laboratory scan of a conventional impression. Due to various results from studies over the last few years [25, 26], which showed a greater accuracy for single-tooth restorations that were manufactured on the basis of direct intraoral scans in comparison to the conventional workflow, we decided to utilize two well-established and validated intraoral scanners (CEREC AC Omnicam; Cara TRIOS) as references. As this study analyzed the entire workflow, we optimized the production parameters prior to the study to insure an optimal result for the clinically most relevant parameter “marginal fit” for the different methods compared. We ensured that the marginal fit was not effected by axial, incisal, or occlusal discrepancies. Therefore, we omitted the further analysis of the internal fit of the copings.
All types of teeth (molars, premolars, and anteriors) were included in this study, although not in equal numbers. This is not suspected to have any influence on the differences found between the acquisition methods, as the same conditions were provided for every technique and reproduction of every type of tooth. There was no limitation concerning the position of the preparation margin, as long as it was visible. This was particularly necessary for the intraoral scanners, which operate solely with optical acquisition systems, yet it is also necessary for the application of VPS for the conventional impression to the preparation margin. The absolute marginal discrepancy according to Holmes et al. [27] was selected as the primary outcome variable as this measurement does imply the full extent of the misfit, and includes under-extension and over-extension of the restoration margins. As also most authors measure the marginal discrepancy [10], so we chose to do the same to increase the comparability of the study. Compared to an in vitro setup, where teeth and cemented restoration can easily be sectioned, the in vivo assessment of the marginal gap is rather difficult. Therefore, the well-established replica technique was applied, which allows for a non-invasive and easily performed means for assessing the adaptation of a restoration to the tooth surface [28]. The concordance of the thin outer silicone layer in the replica to the cement-space of a cemented restoration has been validated multiple times [29, 30]. Known limitations of the technique, such as its slice preparation and deep preparation margins, were excluded from the beginning and therefore did not have an effect [31].
As there are several work steps between the capturing of the intraoral situation and the completion of the actual zirconia coping, not only the acquisition method but also the whole workflow with all of its variables has to be taken into account. As all three of the systems produce digital data, from this point on, the same standardized workflow was conducted for all of the methods.
Considering the data obtained in this clinical investigation, the null hypothesis was rejected because significant differences were found for the marginal discrepancies of the copings fabricated from the direct and indirect digital impression methods. The mean marginal gap was 86.09 μm for CEREC AC Omnicam, 88.95 μm for Cara TRIOS, and 143.29 μm for the impression scan. To our knowledge, there are no in vivo investigations available in the literature that compare intraoral scanning systems with the indirect laboratory scan of a conventional impression. However, there are some studies comparing intraoral scanning systems with the laboratory scan of a gypsum cast [15, 17, 18, 24, 32] or with the entire conventional workflow [25, 26].
Berrendero et al. [17] assessed the marginal gap of full-ceramic crowns in vivo, comparing the CaraTRIOS intraoral scanner to a laboratory scan of a plaster model resulting from a conventional impression. The mean marginal discrepancy was 106.6 μm for the intraoral scan and 119.9 μm for the scan of the gypsum cast. Boeddinghaus et al. [24] investigated both intraoral scanners that were utilized in this investigation and measured a mean marginal gap of 112 μm for CaraTRIOS and a mean marginal gap of 149 μm for CEREC AC Omnicam. Additionally, they tested another intraoral scanning system, Lava True Definition, and observed a mean marginal gap of 88 μm. The study of Brawek et al. [16] compared the marginal gaps of crowns fabricated from the data captured with the Lava COS intraoral scanner to those fabricated from the data of CEREC AC in vivo and measured 51 μm for Lava COS and 83 μm for CEREC AC. Other authors also found smaller gaps with Lava COS in vivo [15, 32]. However, both 3 M scanning systems, Lava COS and Lava True Definition, operate only with the application of a scanning powder and therefore cannot be compared directly to powderless scanning systems. The slightly lower values for Cara TRIOS and CEREC AC Omnicam in the present study could have been due to the use of more recent software versions in both intraoral scanners and lower settings for the cement space. Regarding the laboratory scan of a conventional impression, in vitro investigations show considerably smaller marginal gaps compared to the in vivo outcomes of the present study [20, 33]. Lee et al. compared two indirect laboratory procedures and found mean marginal discrepancies ranging from 54 μm to 75 μm for the scan of the plaster model and from 69 μm to 118 μm for the scan of the conventional impression [21]. Shembesh et al. investigated all three methods of digitizing the intraoral situation. The best outcome was shown by the intraoral scanning system Lava True Definition, which measured a mean marginal gap of 27 μm. The laboratory scan of the gypsum model achieved a mean value of 50 μm, while the laboratory scan of a silicone impression reached the highest value of 81 μm, which still is well within the clinical parameters of acceptance [22]. It is common for studies to show higher accuracies in vitro than in vivo [34]. Clinical factors, such as limited space, patient movement, saliva, bleeding, and sulcus-fluid do not have any influence on the outcome in in vitro settings, whereas they foster errors when working in vivo. Here, digital systems appear to have an advantage over conventional impressions because they allow the user to check for inaccuracies on a magnified model on a screen after finishing the scanning procedure. Therefore, errors can be detected more easily.
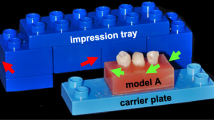
In this study, the mean marginal gaps for the different types of teeth within each acquisition method were also examined. Although none of them displayed significant differences, a tendency is recognizable within the data of the laboratory scan of the conventional impression (Table 1). Incisors and canines, which are teeth that are typically longer and more angulated when prepared for a crown, exhibit greater mean marginal gaps and greater standard deviations compared to premolars and molars. The latter show a stronger similarity to the shape of model teeth that are typically used in in-vitro settings. The major disadvantage when scanning conventional impressions appears to be the insufficient ability to capture long and deep hollow spaces and inside contours, as found in the impression of prepared incisors and canines [35, 36]. Figure 3 shows a schematic representation why the capturing process might fail to complete. The angle α remains the same for both rays of light shown. The green ray can be reflected to the sensor whereas the red ray is hindered by the border of the impression resulting in an incomplete acquisition of the same tooth. Therefore the limitations do not seem too dependent on the scanner, but on the geometry of the tooth.

Incomplete acquisition of a tooth in the scanning process of a conventional impression
Conclusion
Within the limitations of the present study, it can be concluded that the laboratory scan of a conventional impression is not comparable to that obtained using intraoral scanners regarding the marginal fit of zirconia copings manufactured on the basis of the resulting data. Only the copings that were obtained from the intraoral scanners CEREC AC Omnicam and Cara TRIOS displayed marginal gaps within the limits of clinical acceptability.
References
Fasbinder DJ (2013) Computerized technology for restorative dentistry. Am J Dent 26:115–120
Gardner FM (1982) Margins of complete crowns--literature review. J Prosthet Dent 48:396–400
Jacobs MS, Windeler AS (1991) An investigation of dental luting cement solubility as a function of the marginal gap. J Prosthet Dent 65:436–442
Ramfjord SP (1974) Periodontal aspects of restorative dentistry. J Oral Rehabil 1:107–126
Sorensen SE, Larsen IB, Jorgensen KD (1986) Gingival and alveolar bone reaction to marginal fit of subgingival crown margins. Scand J Dent Res 94:109–114
Walton JN, Gardner FM, Agar JR (1986) A survey of crown and fixed partial denture failures: length of service and reasons for replacement. J Prosthet Dent 56:416–421
Goldman M, Laosonthorn P, White RR (1992) Microleakage-full crowns and the dental pulp. J Endod 18:473–475. https://doi.org/10.1016/s0099-2399(06)81345-2
McLean JW and von Fraunhofer JA (1971) The estimation of cement film thickness by an in vivo technique. Br Dent J 131:107–111
Dreyer Jorgensen K (1956) Prüfergebnisse zahnärztlicher Gußverfahren. Dtsch Zahnärztl Z 13:461–468
Contrepois M, Soenen A, Bartala M, Laviole O (2013) Marginal adaptation of ceramic crowns: a systematic review. J Prosthet Dent 110:447–454. https://doi.org/10.1016/j.prosdent.2013.08.003
Takahashi H, Finger WJ (1994) Effects of the setting stage on the accuracy of double-mix impressions made with addition-curing silicone. J Prosthet Dent 72:78–84
Petrie CS, Walker MP, O'Mahony AM, Spencer P (2003) Dimensional accuracy and surface detail reproduction of two hydrophilic vinyl polysiloxane impression materials tested under dry, moist, and wet conditions. J Prosthet Dent 90:365–372. https://doi.org/10.1016/s0022391303005158
Luthardt RG, Koch R, Rudolph H, Walter MH (2006) Qualitative computer aided evaluation of dental impressions in vivo. Dent Mater 22:69–76. https://doi.org/10.1016/j.dental.2005.02.015
Birnbaum NS, Aaronson HB (2008) Dental impressions using 3D digital scanners: virtual becomes reality. Compend Contin Educ Dent 29 494(496):498–505
Ahrberg D, Lauer HC, Ahrberg M, Weigl P (2015) Evaluation of fit and efficiency of CAD/CAM fabricated all-ceramic restorations based on direct and indirect digitalization: a double-blinded, randomized clinical trial. Clin Oral Investig 20:291–300. https://doi.org/10.1007/s00784-015-1504-6
Brawek PK, Wolfart S, Endres L, Kirsten A, Reich S (2013) The clinical accuracy of single crowns exclusively fabricated by digital workflow--the comparison of two systems. Clin Oral Investig 17:2119–2125. https://doi.org/10.1007/s00784-013-0923-5
Berrendero S, Salido MP, Valverde A, Ferreiroa A, Pradies G (2016) Influence of conventional and digital intraoral impressions on the fit of CAD/CAM-fabricated all-ceramic crowns. Clin Oral Investig 20:2403–2410. https://doi.org/10.1007/s00784-016-1714-6
Zarauz C, Valverde A, Martinez-Rus F, Hassan B, Pradies G (2015) Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions. Clin Oral Investig 20:799–806. https://doi.org/10.1007/s00784-015-1590-5
Persson AS, Oden A, Andersson M, Sandborgh-Englund G (2009) Digitization of simulated clinical dental impressions: virtual three-dimensional analysis of exactness. Dent Mater 25:929–936. https://doi.org/10.1016/j.dental.2009.01.100
Jeon JH, Kim HY, Kim JH, Kim WC (2014) Accuracy of 3D white light scanning of abutment teeth impressions: evaluation of trueness and precision. J Adv Prosthodont 6:468–473. https://doi.org/10.4047/jap.2014.6.6.468
Lee WS, Kim WC, Kim HY, Kim WT, Kim JH (2014) Evaluation of different approaches for using a laser scanner in digitization of dental impressions. J Adv Prosthodont 6:22–29. https://doi.org/10.4047/jap.2014.6.1.22
Shembesh M, Ali A, Finkelman M, Weber HP, Zandparsa R (2017) An in vitro comparison of the marginal adaptation accuracy of CAD/CAM restorations using different impression systems. J Prosthodont 26:581–586. https://doi.org/10.1111/jopr.12446
Podhorsky A, Rehmann P, Wostmann B (2015) Tooth preparation for full-coverage restorations-a literature review. Clin Oral Investig 19:959–968. https://doi.org/10.1007/s00784-015-1439-y
Boeddinghaus M, Breloer ES, Rehmann P, Wostmann B (2015) Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clin Oral Investig 19:2027–2034. https://doi.org/10.1007/s00784-015-1430-7
An S, Kim S, Choi H, Lee JH, Moon HS (2014) Evaluating the marginal fit of zirconia copings with digital impressions with an intraoral digital scanner. J Prosthet Dent 112:1171–1175. https://doi.org/10.1016/j.prosdent.2013.12.024
Ng J, Ruse D, Wyatt C (2014) A comparison of the marginal fit of crowns fabricated with digital and conventional methods. J Prosthet Dent 112:555–560. https://doi.org/10.1016/j.prosdent.2013.12.002
Holmes JR, Bayne SC, Holland GA, Sulik WD (1989) Considerations in measurement of marginal fit. J Prosthet Dent 62:405–408
Reich S, Uhlen S, Gozdowski S, Lohbauer U (2011) Measurement of cement thickness under lithium disilicate crowns using an impression material technique. Clin Oral Investig 15:521–526. https://doi.org/10.1007/s00784-010-0414-x
Laurent M, Scheer P, Dejou J, Laborde G (2008) Clinical evaluation of the marginal fit of cast crowns-validation of the silicone replica method. J Oral Rehabil 35:116–122. https://doi.org/10.1111/j.1365-2842.2003.01203.x
Rahmé HY, Tehini GE, Adib SM, Ardo AS, Rifai KT (2008) In vitro evaluation of the "replica technique" in the measurement of the fit of Procera crowns. J Contemp Dent Pract 9:25–32
Boening KW, Wolf BH, Schmidt AE, Kastner K, Walter MH (2000) Clinical fit of Procera AllCeram crowns. J Prosthet Dent 84:419–424. https://doi.org/10.1067/mpr.2000.109125
Syrek A et al (2010) Clinical evaluation of all-ceramic crowns fabricated from intraoral digital impressions based on the principle of active wavefront sampling. J Dent 38:553–559. https://doi.org/10.1016/j.jdent.2010.03.015
Kim KB, Kim JH, Kim WC, Kim HY, Kim JH (2013) Evaluation of the marginal and internal gap of metal-ceramic crown fabricated with a selective laser sintering technology: two- and three-dimensional replica techniques. J Adv Prosthodont 5:179–186. https://doi.org/10.4047/jap.2013.5.2.179
Wöstmann B, Blosser T, Gouentenoudis M, Balkenhol M, Ferger P (2005) Influence of margin design on the fit of high-precious alloy restorations in patients. J Dent 33:611–618. https://doi.org/10.1016/j.jdent.2005.01.002
Kühmstedt P and Hintersehr J (2008) Optische 3D-Messtechnik im Dentalbereich digital_dental news 9:40–45
Hollenbeck K, Attin T and Van der Poel M (2012) Dental lab 3D scanners - how they work and what works best. 3Shape technology research, Copenhagen. http://www.3shapedental.com/restoration/education-video/cases/white-papers/dental-lab-3d-scanners/. Accessed Acces date 2015
Acknowledgments
The authors gratefully acknowledge Dr. Johannes Herrmann of Giessen, Germany, for his statistical advice.
Funding
The work was supported by the Department of Prosthetic Dentistry of the Justus Liebig University, Gießen, Germany.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standard.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Bosniac, P., Rehmann, P. & Wöstmann, B. Comparison of an indirect impression scanning system and two direct intraoral scanning systems in vivo. Clin Oral Invest 23, 2421–2427 (2019). https://doi.org/10.1007/s00784-018-2679-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2679-4