
Abstract
Objectives
The aim of this study was to evaluate the clinical performance of silorane-based composite restorations applied after different surface treatments.
Materials and methods
This controlled and randomized clinical trial included 26 patients with class I restoration indications. The teeth were randomly assigned to the following treatments: control 1/G1, silorane specific self-etching adhesive (P90 self-etch primer and bond) + silorane-based composite resin (Filtek™ P90 low shrink posterior restorative); G2, 37% phosphoric acid + silorane specific self-etching adhesive + silorane-based composite resin; G3, blasting with aluminum oxide + silorane specific self-etching adhesive + silorane-based composite resin; and control 2/G4, self-etching adhesive (Adper™ SE Plus self-etch adhesive) + dimethacrylate-based composite resin (Filtek™ P60 posterior restorative). The clinical performance was evaluated at baseline and after 1 year.
Results
A total of 141 restorations were made and evaluated. For all clinical criteria evaluated, no significant difference was found between the surface treatments at baseline and after 1 year (p > 0.05). After 1 year, only the group with 37% phosphoric acid + silorane specific self-etching adhesive (G2) showed a significant reduction in marginal adaptation (p < 0.05).
Conclusion
In general, all surface treatments showed an adequate clinical performance for silorane-based composite resin in class I restorations. However, a reduction in the marginal adaptation after 1 year was found when additional phosphoric acid etching was used prior to silorane specific self-etching adhesive.
Clinical relevance
The use of phosphoric acid etching prior to specific self-etching adhesive can adversely affect the marginal adaptation of silorane-based restorations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The development of new adhesives and the improvement of the physical and chemical properties of composite resins markedly increased the demand for mercury-free, esthetic restorations in restorative dentistry [1, 2]. Because esthetics is a subjective concept, dental procedures should meet the patient’s esthetic expectations while also considering the functionality of the restoration and the characteristics of the material used [3].
Despite significant advances in adhesives technology, two features of dental resin-based esthetic restorations still require improvement: polymerization shrinkage and the development of polymerization shrinkage stress, which degrades the adhesive interface and creates cracks that compromise the quality and longevity of the restoration. Shrinkage stress can lead to marginal microleakage and adjacent caries lesions: the most common cause of failure for composite resin-based restorations [4]. Marginal defects, material and dental fractures, marginal staining, color changes, hypersensitivity, and patient dissatisfaction also cause failures that can lead to restoration replacement or repair [5,6,7,8,9].
The change from dimethacrylate (a base monomer of composite resins) to silorane has been an important strategy in reducing the effects of polymerization shrinkage. Because the polymerization of silorane occurs through a cationic ring-opening reaction, there is less shrinkage [10]. Additionally, the constant search for new adhesive strategies that improve the interfacial contact between teeth and adhesive has also provided solutions for this problem [11].
Different dental tissue treatments have also been tested to increase surface roughness, thereby improving interfacial contact between the tooth structure and adhesives [12]. As an alternative to acid etching, air abrasion with aluminum oxide has also been used for the pretreatment of enamel and dentin surfaces. This pretreatment promotes the mechanical removal of the smear layer and improves the adhesive infiltration in the demineralized dentin, resulting in substantially increased adhesive strength [13,14,15].
The clinical efficacy of air abrasion with aluminum oxide for silorane-based restorations has not been widely evaluated, particularly compared with the attention given to conventional adhesive [16]. Considering that the choice of the ideal surface treatment should be based on clinical trials results, the current study was conducted to investigate the clinical performance of silorane-based composite resin class I restorations with different surface treatments, at baseline and after 1 year. The null hypothesis tested was that different surface treatments do not affect the clinical performance of silorane-based class I restorations.
Materials and methods
Trial design
A prospective double-blind randomized and controlled clinical trial was designed. The experimental unit was the restoration, and the dependent variable was the qualitative categorical ordinal. This study was approved by the Institutional Ethics Committee (CAAE: 17810713.30000.5141) and registered and approved by the Brazilian Clinical Trials Registry (ReBec) (protocol RBR-2xbpff), being conducted according with CONSORT guidelines. Written informed consent was obtained from all participants.
Patient inclusion and exclusion criteria
This study included subjects who had premolars and molars with indications for class I restorations (active and cavitated occlusal caries lesions extending to dentin but free of proximal caries, according to bitewing radiography) and patients with class I restorations that were assessed as failed in at least one of the following clinical criteria: marginal adaptation, anatomical shape, marginal staining, surface roughness, and postoperative sensitivity or secondary caries. The included patients were older than 18 years of age and agreed to participate in all stages of the research.
Subjects with contraindications to dental treatment due to their medical histories, had xerostomia or were taking medication that substantially decreased the salivary flow, had abutment teeth for fixed or removable prostheses, and had teeth without occlusal relationship with natural dentition were excluded. Non-vital teeth and very deep cavity preparations were also excluded. Patients with visible plaque index higher than 33% were excluded. All participants received oral hygiene instructions and guidance for non-cariogenic diets.
Sample size calculation
Twenty-six patients were recruited from the Operative Dentistry Clinic at the FUNORTE Dental School, Montes Claros, Minas Gerais, Brazil. To calculate the sample size, a 50% difference between the groups was adopted, with a statistical power (1 – β) = 0.90 and error type I (α) = 0.05. The minimum number of teeth in each group should be 19. We decided to include 30 teeth in each group to compensate for patient loss to follow-up [17]. As the sampling unit was the tooth, some patients were allocated to more than one treatment group for each tooth that received a different treatment.
Randomization
The treatments were assigned to each tooth according to a sequence of random numbers generated by MS Excel software (Microsoft Corp., Redmond, WA, USA). After completing 30 random assignments to specific treatments, each group was excluded from subsequent allocations. A professional who was not involved in the intervention or clinical evaluations conducted the randomization process.
Treatment groups
To assess the effect of surface treatments on the clinical performance of silorane restorations, the following groups were tested: control 1/G1, silorane specific self-etching adhesive (P90 self-etch primer and bond) + silorane-based composite resin (Filtek™ P90 low shrink posterior restorative); G2, 37% phosphoric acid + silorane specific self-etching adhesive + silorane-based composite resin; G3, blasting with aluminum oxide + silorane specific self-etching adhesive + silorane-based composite resin; and control 2/G4, self-etching adhesive (Adper™ SE plus self-etch adhesive) + dimethacrylate-based composite resin (Filtek ™ P60 posterior restorative). Table 1 lists the chemical composition and manufacturers of the materials used in this study. Group G2 used 37% phosphoric acid prior to the silorane specific self-etching adhesive system according to the manufacturer recommendations (3M/ESPE); this protocol is optional.
Restorative procedures
Table 2 lists the clinical sequence of surface treatment and restorative procedures. To minimize operator bias, all restorative procedures were performed by only one operator, in accordance with the manufacturer’s instructions. Oblique increments (1.5 mm) of composite resins were inserted and light-cured (40 s). Coarse finishing was made using 3168 FF® diamond tips (KG Sorensen) immediately after completing the restorations, and the polishing was performed with a 9714 FF® carbide drill (KG Sorensen) and Enhance® system (Dentsply) 7 days after the restorative procedure.
Examinations
At baseline (after polishing) and after 1 year, two trained examiners (kappa ≥ 0.78) evaluated the restorations using the FDI World Dental Federation clinical criteria related to direct restorations [18]. The following parameters were evaluated: smoothness and brightness, surface staining, marginal staining, material fracture and retention, marginal adaptation, contour form and occlusal wear, patient opinion, postoperative hypersensitivity, secondary caries, and tooth integrity. For each criterion, the restorations were classified as one of the following conditions: clinically excellent; clinically good, does not need treatment; clinically satisfactory, acceptable effects; clinically unsatisfactory but repairable; and clinically bad, needs replacement.
Statistical analysis
The normality of errors and homoscedasticity of data were assessed for each response variable. Kruskal-Wallis tests compared the treatment groups for each evaluation (baseline and after 1 year), considering all listed criteria. Wilcoxon tests compared the groups among themselves, evaluating the classifications at baseline and after 1 year. The statistical tests considered all classifications in each criterion, but the restoration condition was characterized showing only the percentage of “clinically excellent” cases (the best condition). SPSS® version 20.0 (Statistical Package for the Social Sciences, IBM Company, Hong Kong, China) was used in these calculations, and a significance level of 5% was adopted.
Results
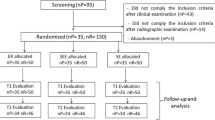
Thirty patients were invited to participate in the trial. However, after applying the inclusion and exclusion criteria, 26 patients were included in the study (18 women and 8 men). The patients were 18–62 years of age (mean = 32.15 years, standard deviation = 11.81). The number of restorations performed matched the number of restorations evaluated at baseline (141 restorations). However, 5 patients did not respond to the 1-year follow-up, and 18 sampling units were lost (Fig. 1).

A flowchart of the clinical trial
The distribution of premolars and molars included in each treatment group at baseline is shown in Table 3. Table 4 shows the clinical performance of the restorations at baseline, according the surface treatment groups for each evaluation criterion. No significant difference was observed between the treatment groups (p > 0.05). Similarly, after 1 year, no significant difference (p > 0.05) was observed between the treatment groups for all evaluated clinical criteria (Table 5).
In the comparison of the clinical performance of restorations between baseline and after 1 year, only the 37% phosphoric acid + silorane specific self-etching adhesive (G2) showed a significant reduction (p < 0.05) in marginal adaptation. No significant difference was observed in the other treatment groups and evaluation criteria (p > 0.05) (Table 6).
Discussion
In general, the different adhesion strategies tested exhibited similar clinical performance for the silorane-based composite in class I restorations, accepting the null hypothesis tested. However, a reduction in marginal adaptation was found when 37% acid phosphoric etching was used prior to the silorane specific self-etching adhesive. Approximately 50% of restorations in this group were classified as “clinically excellent.” Most restorations received clinically favorable ratings, demonstrating an acceptable clinical performance for all groups tested after 1 year. None of the restorations evaluated throughout the study required replacement, and only five needed to be repaired. Independent of the surface treatment used; these results may be due to the quality of the silorane-based composite, which exhibited good clinical performance [19].
The loss to follow-up was approximately 12%. This rate was comparable to those found in similar clinical studies, which usually recorded up to a 15% loss in 1-year recalls [20,21,22]. Even taking into account the loss to follow-up, the minimum sample size was exceeded in each group (19 restorations).
Despite advances in adhesive dentistry and improvements in the physical-chemical properties of dental composites, including an increase in the diversity of the types and brands of composites available on the market, it is necessary to determine their clinical performance. For this reason, clinical studies are the methodological gold standard for generating clinical evidence that is reliable and consistent with practice. This study demonstrated that all the surface treatments tested can be used for restorations of posterior teeth with silorane composites. After a 1-year follow-up, all treatment groups exhibited favorable clinical performance in terms of the evaluated criteria. However, a longer follow-up is required to confirm the long-term clinical performance of these treatments.
Moreover, a reduction in marginal adaptation was found for the group treated with 37% phosphoric acid prior to silorane specific self-etching adhesive. Resin composite direct restorations in posterior teeth are likely to develop cracks in the dental interface because the polymerization shrinkage of the resin and the stress generated by polymerization shrinkage promoting cuspal deflection [23, 24]. Thus, to minimize risks and avoid interpretation bias, the polymerization procedure was carefully performed. The restorations were made using the incremental layering technique, and the quality and intensity of the light emitted by the light-curing device were properly maintained. Therefore, these failures have been attributed to the polymerization shrinkage of the composite and to long-term adhesive degradation [13, 25]. Although this study is still in the initial phase, similar results have been reported by previous studies that detected imperfections in the marginal integrity and function of restorations evaluated from the first year of follow-up [20, 26]. Nevertheless, it is not plausible that the presence of dental caries related to the restoration may have affected the marginal integrity and marginal adaptation, as the short follow-up may not have been sufficient to allow the development of these lesions. Additionally, the lack of injuries can be attributed to the fact that patients with poor oral hygiene (IPV > 30%) and those with a low production of saliva were excluded from the study.
The clinical performance of dental restorations also depends on the patient behavior to maintain proper diet and hygienic habits, as well as the meticulous operative technique and professional skills that play a decisive role in the success of the restorative treatments [27]. Moreover, there is no consensus in the scientific literature regarding the criteria used to evaluate the clinical features of dental restorations or regarding the subjectivity of the process [29]. In this study, we opted to use the criteria proposed by Hickel et al. (2007) because these criteria are a consolidated tool composed of clinical and biological parameters that can be selected based on the specific objective of the study [18, 28,29,30].
Despite the satisfactory clinical results found for all clinical parameters evaluated, future studies and evaluations must be conducted in the medium and long term to affirm the effect of the surface treatments tested, primarily in deep cavity preparations. Overall, the surface treatments and the base monomers tested provided clinically acceptable resin composite restorations in posterior teeth achieving high rates of excellence. However, 37% phosphoric acid etching prior to the silorane specific self-etching adhesive can compromise the marginal adaptation.
References
Frankenberger R, Kramer N, Petachelt A (2000) Technique sensitivity of dentin bonding: effect of applications mistakes on bond strength and marginal adaptation. Oper Dent 25:324–330
Papacchini F, Magni E, Radovic I, Mazzitelli C, Monticelli F, Goracci C, Polimeni A, Ferrari M (2007) Effect of intermediate agents and pre-heating of repairing resin on composite-repair bonds. Oper Dent 32:363–371. https://doi.org/10.2341/06-105
Kelleher M (2012) Ethical issues, dilemmas and controversies in ‘cosmetic’ or aesthetic dentistry. A personal opinion. Br Dent J 212:365–367. https://doi.org/10.1038/sj.bdj.2012.317
Eick D, Kotha SP, Chappelow CC et al (2007) Properties of silorane-based dental resins and composites containing a stress-reducing monomer. Dent Mater 23:1011–1017. https://doi.org/10.1016/j.dental.2006.09.002
Van Ende A, Mine A, De Munck J, Poutevin A, Van Meerbeek B (2012) Bonding of low-shrinking composites in high C-factor cavities. J Dent 40:295–303. https://doi.org/10.1016/j.jdent.2012.01.004
Fernández E, Martin JA, Angel PA et al (2011) Survival rate of sealed, refurbished and repaired defective restorations: 4-year follow-up. Braz Dent J 22:134–139. https://doi.org/10.1590/S0103-64402011000200008
Blum I, Lynch CD, Wilson NH (2012) Teaching of direct composite restoration repair in undergraduate dental schools in the United Kingdom and Ireland. Eur J Dent Educ 16:53–58. https://doi.org/10.1111/j.1600-0579.2010.00674.x
Costa T, Serrano AM, Atman AP, Loquercio AD, Reis A (2012) Durability of composite repair using different surface treatments. J Dent 40:513–521. https://doi.org/10.1016/j.jdent.2012.03.001
Hickel R, Brushaver K, Ilie N (2013) Repair of restorations—criteria for decision making and clinical recommendations. Dent Mater 29:28–50. https://doi.org/10.1016/j.dental.2012.07.006
Popoff DAV, Santa-Rosa TTA, Ferreira RC, Magalhães SCS, Moreira AN, Mjor IA (2012) Repair of dimethacrylate-based composite restorations by a silorane-based composite: a one-year randomized clinical trial. Oper Dent 37:E1–10. https://doi.org/10.2341/11-121-C
Reis A, Loguercio AD, Schroeder M, Luque-Martinez I, Masterson D, Maia LC (2015) Does the adhesive strategy influence the postoperative sensitivity in adult patients with posterior resin composite restorations?: A systematic review and meta-analysis. Dent Mater 31:1052–1067. https://doi.org/10.1016/j.dental.2015.06.001
Coli P, Alaeddin S, Wwennerberg A, Karlsson S (1999) In vitro dentin pretreatment: surface roughness and adhesive shear bond strength. Eur J Oral Sci 107:400–413. https://doi.org/10.1046/j.0909-8836.1999.eos107512.x
França FMG, Santos AJS, Lovadino JR (2007) Influence of air abrasion and long-term storage on the bond strength of self-etching adhesives to dentin. Oper Dent 32:217–224. https://doi.org/10.2341/06-61
Los SA, Barkmeier WW (1994) Effects of dentin air abrasion with aluminium oxide and hydroxyapatite on adhesive bond strength. Oper Dent 19:169–175
Rinaudo PJ, Cochran MA, Moore BK (1997) The effect of air abrasion on shear bond strength to dentin with dental adhesives. Oper Dent 22:254–259
Baracco B, Fuentes MV, Ceballos L (2016) Five-year clinical performance of a silorane- vs a methacrylate-based composite combined with two different adhesive approaches. Clin Oral Investig 20:991–1001. https://doi.org/10.1007/s00784-015-1591-4
Escosteguy CC (1999) Tópicos metodológicos e estatísticos em ensaios clínicos controlados randomizados. Arq Bras Cardiol 72:139–143
Hickel R, Roulet JF, Bayne S et al (2007) Recommendations for conducting controlled clinical studies of dental restorative materials. Science Committee Project 2/98--FDI World Dental Federation study design (Part I) and criteria for evaluation (Part II) of direct and indirect restorations including onlays and partial crowns. J Adhes Dent 9:121–147
Mahmoud SH, Ali AK, Hegazi HA (2014) A three-year prospective randomized study of silorane- and methacrylate-based composite restorative systems in class II restorations. J Adhes Dent 16:285–292. https://doi.org/10.3290/j.jad.a31939
Schmidt M, Kirkevang LL, Hǿrsted-Bindslev P, Poulsen S (2011) Marginal adaptation of a low-shrinkage silorane-based composite: 1-year randomized clinical trial. Clin Oral Investig 15:291–295. https://doi.org/10.1007/s00784-010-0446-2
Gordan VV, Shen C, Watson RE, Mjor IA (2005) Four-year clinical evaluation of self-etching primer and resin-based restorative material. Am J Dent 18:45–49
Moncada G, Martin J, Fernández E, Hampel MC, Mjör IA, Gordan VV (2009) Sealing, refurbishment and repair of class I and class II defective restorations: a three-year clinical trial. J Am Dent Assoc 140:425–432
Baratieri LN, Ritter AV (2001) Four-year clinical evaluation of posterior resin-based composite restorations placed using the total-etch technique. J Esthet Restor Dent 13:50–57. https://doi.org/10.1111/j.1708-8240.2001.tb00251.x
Campos EA, Andrade MF, Porto-Neto ST et al (2009) Cuspal movement related to different bonding techniques using etch-and-rinse and self-etch adhesive systems. Eur J Dent 3:213–218
Moura FRR, Romano AR, Lund RG, Piva E, Rodrigues-Junior AS, Demarco FF (2011) Three-year clinical performance of composite restorations placed by undergraduate dental students. Braz Dent J 22:111–116. https://doi.org/10.1590/S0103-64402011000200004
Lima FG, Romano AR, Correa MB, Demarco FF (2009) Influence of microleakage, surface roughness and biofilm control on secondary caries formation around composite resin restorations: an in situ evaluation. J Appl Oral Sci 17:61–65. https://doi.org/10.1590/S1678-77572009000100012
Park J, Chang J, Ferracane J, Lee IB (2008) How should composite be layered to reduce shrinkage stress: incremental or bulk filling? Dent Mater 24:1501–1505. https://doi.org/10.1016/j.dental.2008.03.013
Hickel R, Roulet JF, Bayne S, Heintze SD, Mjör IA, Peters M, Rousson V, Randall R, Schmalz G, Tyas M, Vanherle G (2007) Recommendations for conducting controlled clinical studies of dental restorative materials. Clin Oral Investig 11:5–33. https://doi.org/10.1007/s00784-006-0095-7
Opdam NJ, Bronkhorst EM, Roeters JM, Loomans BAA (2007) A retrospective clinical study on longevity of posterior composite and amalgam restorations. Dent Mater 23:2–8. https://doi.org/10.1016/j.dental.2005.11.036
Rosa Rodolpho PA, Donassollo TA, Cenci MS et al (2011) 22-year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater 27:955–963. https://doi.org/10.1016/j.dental.2011.06.001
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the National Research Committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all study participants.
Rights and permissions
About this article

Cite this article
Marques, I.P., de Oliveira, F.B.S., Souza, J.G.S. et al. Influence of surface treatment on the performance of silorane-based composite resin in class I restorations: a randomized clinical trial. Clin Oral Invest 22, 2989–2996 (2018). https://doi.org/10.1007/s00784-018-2390-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2390-5