
Abstract
Objective
The objective of this study was to investigate the effects of cavity configuration on the shrinkage vectors of a flowable resin-based composite (RBC) placed in occlusal cavities.
Materials and methods
Twenty-seven human molars were divided into three groups (n = 9) according to cavity configuration: “adhesive,” “diverging,” and “cylindrical.” The “adhesive” cavity represented beveled enamel margins and occlusally converging walls, the “diverging” cavity had occlusally diverging walls, and the “cylindrical” cavity had parallel walls (diameter = 6 mm); all cavities were 3 mm deep. Each prepared cavity was treated with a self-etch adhesive (Adper Easy Bond, 3 M ESPE) and filled with a flowable RBC (Tetric EvoFlow, Ivoclar Vivadent) to which had been added 2 wt% traceable glass beads. Two micro-CT scans were performed on each sample (uncured and cured). The scans were then subjected to medical image registration for shrinkage vector calculation. Shrinkage vectors were evaluated three-dimensionally (3D) and in the axial direction.
Results
The “adhesive” group had the greatest mean 3D shrinkage vector lengths and upward movement (31.1 ± 10.9 μm; − 13.7 ± 12.1 μm), followed by the “diverging” (27.4 ± 12.1 μm; − 5.7 ± 17.2 μm) and “cylindrical” groups (23.3 ± 11.1 μm; − 3.7 ± 13.6 μm); all groups differed significantly (p < 0.001 for each comparison, one-way ANOVA, Tamhane’s T2).
Conclusion
The values and direction of the shrinkage vectors as well as interfacial debonding varied according to the cavity configuration.
Clinical relevance
Cavity configuration in terms of wall orientation and beveling of enamel margin influences the shrinkage pattern of composites.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Shrinkage vectors represent the amount and direction of resin-based composite (RBC) mass movement due to polymerization shrinkage [1]. Polymerization shrinkage of light-cured RBC depends on the chemical composition, degree of conversion of RBC, and the curing light energy [2, 3]. Furthermore, boundary conditions such as cavity configuration and bonding conditions have varying influences on restricting shrinkage by adhesive attachment of the composite to the surrounding constraints [4,5,6]. The adverse consequences of shrinkage are studied by testing marginal adaptation and microleakage, interfacial gaps, and bond strength [7,8,9,10,11].
Volumetric or linear shrinkage measurements of RBCs can be performed for a mass of RBC [1, 12, 13] or by assessing the linear cuspal deflection, which indicates the shrinkage of an RBC placed in a cavity [14, 15]. With the increased use of radiological images in medical research, medical image registration has evolved [16]. Recently, micro-CT scans of RBCs were used for measuring volume loss upon polymerization either in molds or in cavities prepared in teeth [17,18,19,20,21,22]. This method can also display areas of debonding and leakage around restorations [17, 18, 20, 23,24,25,26].
Chiang et al. and Rösch et al. developed a method for visualizing two-dimensional (2D) and three-dimensional (3D) shrinkage vectors of RBC restorations upon image registration. They traced radiolucent glass beads embedded in a commercial RBC in micro-CT scans before and after light curing, thus displaying the shrinkage vectors upon polymerization and the internal movements in relation to the tooth structure. The 2D analysis was based on an evaluation of B-splines, and the 3D analysis was based on the block-matching algorithm [27,28,29].
The visualization of shrinkage vectors can be achieved by various methods, each of which is based on a specific mathematical principle [30]. Cho et al. traced radiopaque zirconia fillers added to an RBC using a cluster-labeling algorithm to extract the fillers and perform the pairing procedure [31]. Takemura et al. incorporated air bubbles into the RBC and traced these via regression analysis to obtain shrinkage vectors [32], while van Ende et al. traced inherently present particles by implementing a B-spline evaluation [33].
The cavity configuration proposed for adhesive restorations features beveled enamel margins and rounded dentin walls [34, 35]. The polymerization shrinkage of an adhesive restoration was reported to be directed toward the curing light [34, 36]. Versluis et al. conducted a finite element analysis (FEA) and claimed that shrinkage was not necessarily directed toward the curing light but was rather affected by the bonding of the restoration and free surfaces, in other words, by the boundary conditions [6]. On the other hand, cavities in previous studies investigating shrinkage vectors were either cylindrical [27, 28, 33] or cubic [31] in either teeth [22, 27, 28] or artificial cavity models [31,32,33].
The aim of this study was to analyze the effects of occlusal cavity configuration on the direction of the shrinkage vectors of a light-cured RBC both three-dimensionally and in the axial direction in relation to the curing light. To clarify whether the cavity configuration of an adhesive restoration influences the shrinkage direction, two other cavity configurations were proposed: a “diverging” cavity (cone trunk shaped) that allows for unimpeded upward movement and a “cylindrical” cavity that is neutral to any shrinkage direction. The null hypothesis was that there would be no effect of cavity configuration on the shrinkage vectors.
Materials and methods
The materials used are listed in Table 1. The extracted teeth were collected and stored in sodium azide in the dark. The experimental procedures were approved by the ethics committee of the medical faculty.
Sample preparation
Twenty-seven freshly extracted sound human molars were divided into three groups (n = 9) according to cavity configuration: “adhesive,” “diverging,” and “cylindrical.” The occlusal cusps of the teeth were slightly flattened for standardizing the light-curing procedure and for easier perpendicular light application without contacting the cavity margin. The roots of the teeth were embedded in an acrylic resin (Technovit 4000, Heraeus Kulzer GmbH, Hanau, Germany). The depth of all prepared cavities of different configurations was 3 mm, and cavities were prepared by one investigator at high speed with adequate coolant.
The “adhesive” cavity configuration, as proposed for adhesive restorations, displayed beveled enamel margins and rounded geometric cavity walls [34, 36]. A cylindrical cavity 5 mm in diameter was prepared with a diamond wheel, which was used to cut laterally into the dentin at full depth to prepare the rounded walls. A circumferential bevel of 1 mm at the enamel margin of the cavity was prepared with a fine cylindrical diamond to create a greater surface area for bonding to enamel.
The “diverging” cavity configuration had occlusally diverging walls, with an outer cavity margin in enamel 7 mm in diameter and a cavity floor 5 mm in diameter. A cylindrical cavity was prepared with a diamond wheel, and occlusally diverging walls were prepared with a fine cylindrical diamond. This cavity configuration was included to allow for unimpeded upward movement of the RBC in case it would shrink toward the curing light.
The “cylindrical” cavity configuration was prepared with a diamond wheel according to Chiang et al. and Versluis et al., with parallel walls that were neutral to any direction of shrinkage [6, 27, 28]. The samples were fixed to the sample holder with RBC to prevent any movement during the scanning procedure.
The volumes of the cavity configurations were 85.6 mm3 for the “adhesive,” 85.6 mm3 for the “diverging,” and 84.8 mm3 for the “cylindrical.” The C-factor of the “adhesive” cavity configuration was 2.6, that of the “diverging” was 2.1, and that of the “cylindrical” was 3.
Adper Easy Bond (3 M ESPE, Seefeld, Germany), a self-etch one-step adhesive, was applied for 20 s, air thinned for 5 s, and light cured for 20 s using the light-curing unit Elipar FreeLight2 (3 M ESPE, Seefeld, Germany) with a light intensity of 1200 mW/cm2 according to the manufacturer, which was checked for constant light intensity once/week with a dental radiometer (Bluephase Meter, Schaan, Ivoclar Vivadent).
Preparation of the traceable RBC
A flowable RBC (Tetric EvoFlow, Ivoclar Vivadent, Schaan Liechtenstein) was used to which had been added 2 wt% silanized radiolucent glass beads of average particle size of 40–70 μm (Sigmund Lindner GmbH, Warmensteinach, Germany) [27, 28, 37, 38]. Silanization of the glass beads offered chemical bonding of the beads to the resin matrix [39], and the protocol for the glass bead silanization was previously described in detail [37]. The RBC was inserted into the prepared cavity in bulk and remained uncured during the first scanning.
X-ray micro-computed tomography measurements
The samples were scanned in a high-resolution micro-computed tomography apparatus (Micro-CT 40, Scanco Medical AG, Switzerland) with the following settings: acceleration voltage 70 kVp and cathode current 114 μA. The samples were scanned with high resolution (8 μm voxel size) using an integration time of 600 ms. Water was added to the sample holder to prevent the dehydration and subsequent cracking of the tooth during tooth scanning. The sample holder was covered with a radiolucent and dark cap to avoid premature polymerization of the uncured RBC during the scanning procedure and was placed inside the micro-CT machine for the first micro-CT scan [27, 28, 37, 38].
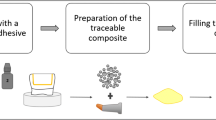
The RBC was light cured for 40 s, and the sample was scanned again using the same parameters as before. During the entire process, the sample remained in the sample holder to avoid the gross displacement of the tooth to facilitate and accelerate the subsequent registration of the data sets. The raw micro-CT scans were reconstructed and saved as 16-bit data sets of the attenuation coefficient per voxel and each data set was approximately 3.9 GB in size; details of the workflow are presented in Fig. 1 [27, 28, 37, 38].

Workflow for obtaining the digital 3D data sets from the micro-CT scanner
Data processing
The aim was identifying each individual embedded glass bead presented in the scan as a sphere and to follow the position change of the spheres due to polymerization shrinkage. Data processing started with rigid registration [40] in order to align the scans through the enamel and the dentinoenamel junction, followed by sphere segmentation and sphere registration of each individual sphere based on a block-matching algorithm that was previously described in details [27,28,29, 37, 38, 41].
Qualitative evaluation of polymerization shrinkage: visualization of shrinkage vectors
The shrinkage vector fields were visualized three-dimensionally using VTK (www.vtk.org), where each shrinkage vector was represented graphically in the form of a glyph (arrow) that pointed in the direction of shrinkage and all shrinkage vectors together formed the shrinkage vector field. For better visibility, the shrinkage vectors were scaled by a factor of 5 and the shrinkage vector fields were visually analyzed for shrinkage patterns [27, 28, 37, 38].
Quantitative evaluation of polymerization shrinkage: values of shrinkage vectors
The result of the registration process was presented in a text file that listed the x-, y-, and z-coordinates of each identified sphere, in both the pre-polymerization and post-polymerization scans. Absolute values of the 3D shrinkage vectors were calculated as the Euclidean distance of the centers of gravity of each segmented individual sphere before and after curing [27, 28, 37, 38]. Additionally, the shrinkage relative to the curing light was analyzed by examining only the z-component of the shrinkage vectors that denotes the filler movement along the z-axis [37, 38].
Statistical analysis
The mean vector lengths and glass bead movement in the z-direction were computed, and each was subjected to one-way ANOVA with post hoc pairwise comparisons using Tamhane’s T2 at p < 0.05 (with IBM SPSS Statistics 20) [37, 38].
Scanning electron microscopy
One sample per group was critically point dried, sectioned longitudinally, and examined for internal adaptation with a scanning electron microscope (ZEISS GEMINI® FESEM, SUPRA™ 55VP, Carl Zeiss SMT AG, Oberkochen, Germany) at × 200 magnification [28, 37, 38].
Results
Qualitative evaluation of polymerization shrinkage: visualization of shrinkage vectors
The glass beads were identified, labeled, and extracted from the matrix by sphere segmentation. Then, the segmented spheres were registered and shrinkage vectors were computed (Fig. 2). All shrinkage vectors of one restoration formed the shrinkage vector field. The shrinkage vector field in the “adhesive” group showed, for all samples, extensive upward movement in the lower part of the restoration with predominantly large vectors, while the upper part exhibited fewer shrinkage vectors with minimal downward shrinkage (Fig. 3a). The SEM images of the arbitrarily selected sample showed a defective bond at the floor, while an intact bond at the enamel margin was observed (Fig. 3b).

Sphere segmentation and sphere registration. Sphere segmentation: the set of all identified and extracted glass beads in one sample (a). Sphere registration: both scans of one sample were superimposed (b). In the first scan, the identified glass beads were radiolucent and colorless, while in the second scan, the corresponding glass beads were superimposed and color coded. Sphere registration was performed based on a block-matching algorithm to determine the displacement of the segmented spheres due to polymerization shrinkage

The shrinkage vector fields with the radiographic planes of the micro-CT scans in the background and SEM images of representative samples of the three cavity configurations. The shrinkage vectors, represented as glyphs (arrows), were scaled by a factor of 5 to enhance visibility. In the “adhesive” cavity configuration (a), the shrinkage vectors point upward, but only minute downward movement is observed at the free surface. SEM images (× 200) of the “adhesive” cavity configuration (b) show an intact bond at the enamel margin and a defective bond at the floor of the restoration (arrows). The star indicates one traceable glass bead. In the “diverging” cavity configuration (c), large shrinkage vectors point downward near the free surface, and small ones point upward from the restoration floor. SEM images (× 200) of the “diverging” cavity configuration (d) display a defective bond at the enamel margin (arrows) and an intact bond at the restoration floor. The shrinkage vector field in the “cylindrical” cavity configuration displays shrinkage pattern-1 (e), where more shrinkage vectors are located in the lower part, while shrinkage pattern-2 (f) additionally exhibits large vectors in the upper restoration part. SEM images (× 200) of the “cylindrical” restoration (g) showing an intact bond at the enamel margin on one side and a defective bond at the floor of the restoration (arrows)
In the “diverging” group, the shrinkage vector field showed, in the upper part of the restoration, large shrinkage vectors with great downward shrinkage, while the lower part of the restoration had many small vectors with upward shrinkage (Fig. 3c). The SEM images displayed a defective bond at the enamel margin and an intact bond at the floor (Fig. 3d).
All the teeth in the “cylindrical” group showed a considerable number of shrinkage vectors in the lower third of the cavity, which pointed upward. In contrast to this uniform appearance of the lower cavity part, the upper part of the cavity had fewer vectors pointing downward in the upper third of the cavity for six teeth (Fig. 3e), termed shrinkage pattern-1. Three teeth exhibited more shrinkage vectors in the upper third of the cavity pointing downward (Fig. 3f), termed shrinkage pattern-2. The density of the identified vectors was the same in both groups. The vector density in the lower third was greater than in the upper third. SEM images showed an intact bond at the enamel margin on one side only and a defective bond at the floor (Fig. 3g).
The thickness of the adhesive layer varied in the different cavity configurations at different locations: in the “adhesive” cavity configuration, it was thickest below the enamel margin, while in the “diverging,” it was thickest at the enamel margin. None of these variations in thickness were observed in the “cylindrical” cavity configuration.
Quantitative evaluation of polymerization shrinkage: values of shrinkage vectors
Quantitative non-directional analysis
The results of the mean vector lengths are summarized in Table 2. The “adhesive” cavity configuration had the highest vector length values, followed by the “diverging”; the smallest were in the “cylindrical” cavity configuration. One-way ANOVA revealed significant differences (F = 179.848; Df = 2,4370; p < 0.001), and the post hoc pairwise comparison using Tamhane’s T2 test showed significant differences between all the groups.
Quantitative directional analysis
An analysis of the shrinkage in relation to the curing light was performed by examining only the z-component of the 3D shrinkage vectors, which denoted the bead movement along the z-axis. Negative values denoted upward shrinkage movement toward the curing light, while positive ones exhibited downward shrinkage away from the light. The greatest mean glass bead movement toward the light was in the “adhesive” cavity configuration, followed by the “diverging” cavity configuration, while the “cylindrical” cavity configuration showed the least mean bead movement toward the curing light (Table 2). The one-way ANOVA revealed significant differences (F = 216.839; Df = 2,4380; p < 0.001), and the post hoc pairwise comparison with Tamhane’s T2 showed statistically significant differences between all the groups.
Discussion
In light of the results, the null hypothesis was rejected because the shrinkage vectors differed significantly in magnitude and direction in the different cavity configurations.
The literature shows that “free shrinkage” occurs when the RBC is not restricted in shrinkage by cavity walls, and it will tend to shrink toward the center [42]. Once the RBC is bonded to an enclosing cavity wall, the shrinkage will be directed toward the cavity wall until the bond strength is exceeded by the developing shrinkage stresses [42,43,44]. Whenever RBCs are bonded, their shrinkage movement is governed by their boundary conditions, such as the cavity configuration, the C-factor, the bonding condition, and the bonding substrate [6, 22, 27, 32, 33, 45, 46]. Accordingly, this shrinkage is termed the “effective shrinkage” [42, 47].
We observed downward shrinkage in the upper parts of the restorations regardless of the cavity configuration. Nonetheless, the downward movement that was related to the free surface was reversed at a deeper part of the restoration. Similar observations were made by Versluis et al. in their FEA of a case presenting a perfect bond to enamel and no bond to dentin [6] and by Cho et al. in a bonded restoration showing downward shrinkage in the upper part while the fillers in the remaining part of the restoration moved upward [31]. Moreover, van Ende et al. detected a comparable shrinkage pattern in large restorations [33].
Therefore, we termed the area where downward and upward shrinkage met as the “fictional zero-line” where almost no axial shrinkage was observed. The fictional zero-line was located close to the surface in the “adhesive” cavity configuration, almost in the middle in the “cylindrical” cavity configuration, and at the junction between the middle and lower thirds in the “diverging” cavity configuration. An RBC has a tendency to shrink toward the center, which is limited by a strong bond to the tooth structure [42]. The apparent strong bonding of the RBC to the beveled enamel in the “adhesive” cavity configuration hindered the downward movement, while the large free surface in the “diverging” cavity configuration enabled downward shrinkage and debonding from the enamel margin. The debonding, in turn, allowed for even more downward shrinkage, which resulted in the fictional zero-line at a lower level.
The bonding condition in the current study was maintained constant by using only one type of self-etch adhesive, which is in contrast to studies that reported the effects of bonded versus unbonded conditions [22, 31, 32]. Self-etch adhesives usually have lower bond strength values than total etch adhesives; thus, debonding from the cavity walls is expected at lower stress levels [48]. This is supported by findings of unbonded restorations that showed greater shrinkage vectors and greater percentage shrinkage [22, 31, 32].
Previous studies of beam profile analysis showed that the light intensity is not homogeneous throughout the diameter of the light tip, which could affect the degree of cure [49, 50]. In the current study, the RBC was cured at the closest possible distance (< 1 mm) for an extended curing time (40 s) to ensure optimal polymerization [22, 27, 28, 31, 32].
For easier visualization of the curing light in relation to the different cavity configurations, a schematic drawing is presented in Fig. 4a–c. The cross-sectional view of the “adhesive cavity” elucidated that light could not directly reach the RBC below the enamel margin in proximity to the dentin walls. This could have affected the polymerization process and might have left the RBC less optimally cured in that area. Stronger bonding to enamel, anchoring along the enamel bevel, and more optimally cured RBC near the surface might be reasons for the greater shrinkage observed in the lower cavity part.

The curing light in relation to the “adhesive” (a), “diverging” (b), and “cylindrical” (c) cavity configurations. In the “adhesive” cavity configuration, light did not directly reach the RBC below the enamel margin. In the “diverging” and “cylindrical” cavity configurations, there was no configurational impedance to the curing light. The light focus of Elipar FreeLight2 (3 M ESPE) in relation to the “cylindrical” cavity configuration (d)
Light emission is not homogeneously distributed throughout the light beam as the light focus differs from one curing light to another. The light focus of the used curing light, Elipar FreeLight2, in relation to the cylindrical cavity is presented in Fig. 4d. It shows more intense light in the center and less intense light at the periphery.
Axial shrinkage constituted only part of the overall 3D shrinkage and should not be taken as the sole measure. Shrinkage in the horizontal direction would provide more information on movements along the cavity walls and floor. Investigating the shrinkage vectors near the bonded surfaces would require the extraction of data in close proximity to the cavity boundaries from the overall data, which was not within the scope of our study.
Shrinkage vectors were visualized three-dimensionally and were quantified regardless of their direction, giving us the absolute values of the shrinkage vectors. In the “adhesive” cavity configuration, numerous shrinkage vectors were located at the rounded area between the floor and walls, reflecting deformation in the undercut area, where light was not directly accessible and its intensity was more attenuated than in other areas. The shrinkage vector field of the “cylindrical” cavity configuration differed from previous findings of Chiang et al. but was in agreement with the bonded restoration by Cho et al. and observations by Sampaio et al. [27, 28, 31, 51].
Shrinkage patterns could be associated with regional volumetric variations in the RBC at different cavity levels within each cavity configuration, as greater shrinkage occurred at the area of greater RBC volume in each group. The “cylindrical” cavity configuration had no regional volumetric variation within the cavity; nonetheless, debonding occurred at one side of the enamel margin and may indicate where the debonding initiated [27, 28]. The absolute vector length values indicate the internal movements within the restoration in relation to the cavity configuration and bonding substrates. In our study, we could relate larger shrinkage vectors to regions of larger volume. Clinicians are advised to minimize variations in volume if possible.
Our results are in line with those of others who observed that shrinkage due to polymerization was not equal in all directions [42]. On the other hand, Zeiger et al. claimed that neither overall shrinkage nor its spatial distribution was affected by cavity geometry or C-factor [20]. This variation might be due to differences in testing methods and study design. Zeiger et al. performed a volumetric evaluation of polymerization shrinkage and a leakage evaluation of non-bonded RBC restorations in human teeth. A volumetric evaluation gives an account of the percentage of shrinkage but not of the internal movements. Nevertheless, the leakage evaluation displayed the areas of debonding from the cavity walls. Their cavities were markedly smaller in size than ours. Upon investigating the shrinkage vectors in small and large cavities, van Ende et al. found that the cavity size played a significant role in the pattern of shrinkage vectors. It is recommended that future studies investigate the effect of C-factor on the shrinkage vectors.
A specific shrinkage pattern could be identified and related to each cavity configuration. The sample size was sufficiently large to report this observation as the resultant shrinkage pattern. Previous studies reported that thick enamel margins promoted a better bond, while thin enamel margins favored debonding and gap formation. The findings of Chiang et al. could not be confirmed in our study because investigating variation in the enamel thickness was not part of our study design, and we did not randomly observe any discrepancies in enamel thickness related to anatomic variation in teeth [27, 28].
A radiolucent area between the tooth and restoration was observed in some samples of the “adhesive” and “diverging” cavity configurations, which could represent either a gap or a relatively thick layer of adhesive. Such areas were observed in both pre- and post-polymerization scans and consequently were assumed to be pooling of the adhesive, as confirmed by SEM. The adhesive thickness varied between the different cavity configurations at different locations.
A flowable RBC was chosen over a conventional RBC because it facilitated incorporation of the glass beads used for tracing. Additionally, flowable RBCs exhibit a greater degree of shrinkage than do their conventional counterparts [51]. Thus, greater shrinkage vector values and easier visualization were expected. Silanization of the glass beads offered chemical bonding and movement with the resinous mass upon polymerization. Being radiolucent, the reconstruction artifacts that might occur with zirconium dioxide fillers could be avoided in the micro-CT scans [27, 28]. The number of embedded glass beads was sufficient to trace the material’s movement throughout the restoration because the average number of identified spheres and resultant shrinkage vectors per restoration was approximately 900. The original Tetric EvoFlow contains 41 wt% fillers, while the hybrid RBC Tetric EvoCeram contains 48.5 wt% fillers; thus, we concluded that the addition of 2 wt% would affect the polymerization to a negligible degree. Although the addition of glass beads or the entrapment of air bubbles might influence the shrinkage behavior of the RBC, only one study has reported tracing inherently present fillers of an RBC [33]. Voids and porosity were not quantified in this study, but they have been reported to expand upon polymerization of the RBC, compensating for the surrounding shrinkage [33].
However, the flowable RBC is not comparable to a hybrid RBC regarding the application in posterior teeth because it has a lower modulus of elasticity. Thus, the shrinkage pattern of a hybrid RBC might differ from the results presented here. Tetric EvoFlow should not be used in increments greater than 2 mm per the manufacturer’s instructions, although a depth of cure of 3 mm was previously confirmed [52]. The incremental application of RBC restorations is a standard technique to compensate for the volumetric shrinkage. Moreover, bulk-fill materials have certain additions to their matrix that enable them to be cured in thicknesses up to 5 mm, but the shrinkage vectors have not yet been evaluated in either incrementally applied RBCs or bulk-fill materials. Therefore, further investigations are needed with bulk-fill materials in deeper cavities and with incrementally applied RBCs.
The computation of shrinkage vectors of dental RBCs upon polymerization is a relatively recent method. The current study implemented the analysis of 3D shrinkage vectors of Chiang et al. and Rösch et al., which is based on a block-matching method [27,28,29]. Registration of the individual spheres was performed to determine the segmented spheres’ displacement during the polymerization process. Accordingly, each identifiable pair of spheres before and after curing was represented by a shrinkage vector, which presented the actual movement and was the method’s main advantage. The approach of matching pairs of spheres is in agreement with others [31, 32].
Some of the limitations of the current study include possible variations in the volumes of the different cavity configurations despite efforts to standardize them, in addition to such unstandardizable variables as the degree of mineralization and structural features of teeth. On the other hand, using human teeth can provide a more clinically relevant outcome compared to using artificial molds of standardized sizes, as was the case in previous studies [31,32,33].
Conclusion
Under the circumstances of this investigation and considering all limitations, it could be concluded that the values and direction of the shrinkage vectors varied according to the cavity configuration and in different regions within a given cavity. Areas of greater restoration volume in a cavity exhibited greater interfacial debonding, where the cylindrical cavity configuration produced the most favorable shrinkage pattern. More research is required to determine the best RBC application protocol to avoid unfavorable shrinkage patterns and interfacial gaps at different cavity parts with variable types of RBCs.
References
Watts DC, Cash AJ (1991) Determination of polymerization shrinkage kinetics in visible-light-cured materials: methods development. Dent Mater 7(4):281–287. https://doi.org/10.1016/S0109-5641(05)80030-2
Price RB, Felix CA, Andreou P (2004) Effects of resin composite composition and irradiation distance on the performance of curing lights. Biomaterials 25(18):4465–4477. https://doi.org/10.1016/j.biomaterials.2003.11.032
Price RB, Felix CM, Whalen JM (2010) Factors affecting the energy delivered to simulated class I and class v preparations. J Can Dent Assoc 76:a94
Braga RR, Ferracane JL (2002) Contraction stress related to degree of conversion and reaction kinetics. J Dent Res 81(2):114–118. https://doi.org/10.1177/0810114
Ferracane JL (2008) Buonocore Lecture. Placing dental composites—a stressful experience. Oper Dent 33(3):247–257. https://doi.org/10.2341/07-BL2
Versluis A, Tantbirojn D, Douglas WH (1998) Do dental composites always shrink toward the light? J Dent Res 77(6):1435–1445. https://doi.org/10.1177/00220345980770060801
Roulet JF, Salchow B, Wald M (1991) Margin analysis of posterior composites in vivo. Dent Mater 7(1):44–49. https://doi.org/10.1016/0109-5641(91)90026-U
Braga RR, Meira JB, Boaro LC, Xavier TA (2010) Adhesion to tooth structure: a critical review of “macro” test methods. Dent Mater 26(2):e38–e49. https://doi.org/10.1016/j.dental.2009.11.150
Armstrong S, Geraldeli S, Maia R, Raposo LH, Soares CJ, Yamagawa J (2010) Adhesion to tooth structure: a critical review of “micro” bond strength test methods. Dent Mater 26(2):e50–e62. https://doi.org/10.1016/j.dental.2009.11.155
Al-Harbi F, Kaisarly D, Bader D, El Gezawi M (2016) Marginal integrity of bulk versus incremental fill class II composite restorations. Oper Dent 41(2):146–156. https://doi.org/10.2341/14-306-L
Al-Harbi F, Kaisarly D, Michna A, ArRejaie A, Bader D, El Gezawi M (2015) Cervical interfacial bonding effectiveness of class II bulk versus incremental fill resin composite restorations. Oper Dent 40(6):622–635. https://doi.org/10.2341/14-152-L
Watts DC, Marouf AS (2000) Optimal specimen geometry in bonded-disk shrinkage-strain measurements on light-cured biomaterials. Dent Mater 16(6):447–451. https://doi.org/10.1016/S0109-5641(00)00043-9
Bekkedahl N (1949) Volume dilatometry. J Res Natl Bur Stand (1934) 43(2):145–156. https://doi.org/10.6028/jres.043.017
Morin DL, Douglas WH, Cross M, DeLong R (1988) Biophysical stress analysis of restored teeth: experimental strain measurement. Dent Mater 4(1):41–48. https://doi.org/10.1016/S0109-5641(88)80087-3
Moorthy A, Hogg CH, Dowling AH, Grufferty BF, Benetti AR, Fleming GJ (2012) Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J Dent 40(6):500–505. https://doi.org/10.1016/j.jdent.2012.02.015
Hill DL, Batchelor PG, Holden M, Hawkes DJ (2001) Medical image registration. Phys Med Biol 46(3):R1–45. https://doi.org/10.1088/0031-9155/46/3/201
Sun J, Fang R, Lin N, Eidelman N, Lin-Gibson S (2009) Nondestructive quantification of leakage at the tooth-composite interface and its correlation with material performance parameters. Biomaterials 30(27):4457–4462. https://doi.org/10.1016/j.biomaterials.2009.05.016
Sun J, Eidelman N, Lin-Gibson S (2009) 3D mapping of polymerization shrinkage using X-ray micro-computed tomography to predict microleakage. Dent Mater 25(3):314–320. https://doi.org/10.1016/j.dental.2008.07.010
Sun J, Lin-Gibson S (2008) X-ray microcomputed tomography for measuring polymerization shrinkage of polymeric dental composites. Dent Mater 24(2):228–234. https://doi.org/10.1016/j.dental.2007.05.001
Zeiger DN, Sun J, Schumacher GE, Lin-Gibson S (2009) Evaluation of dental composite shrinkage and leakage in extracted teeth using X-ray microcomputed tomography. Dent Mater 25(10):1213–1220. https://doi.org/10.1016/j.dental.2009.04.007
Carrera CA, Lan C, Escobar-Sanabria D, Li Y, Rudney J, Aparicio C, Fok A (2015) The use of micro-CT with image segmentation to quantify leakage in dental restorations. Dent Mater 31(4):382–390. https://doi.org/10.1016/j.dental.2015.01.002
Hirata R, Clozza E, Giannini M, Farrokhmanesh E, Janal M, Tovar N, Bonfante EA, Coelho PG (2015) Shrinkage assessment of low shrinkage composites using micro-computed tomography. J Biomed Mater Res B Appl Biomater 103(4):798–806. https://doi.org/10.1002/jbm.b.33258
Kim HJ, Park SH (2014) Measurement of the internal adaptation of resin composites using micro-CT and its correlation with polymerization shrinkage. Oper Dent 39(2):E57–E70. https://doi.org/10.2341/12-378-L
Neves AA, Jaecques S, Van Ende A, Cardoso MV, Coutinho E, Luhrs AK, Zicari F, Van Meerbeek B (2014) 3D-microleakage assessment of adhesive interfaces: exploratory findings by muCT. Dent Mater 30(8):799–807. https://doi.org/10.1016/j.dental.2014.05.003
Han SH, Park SH (2014) Micro-CT evaluation of internal adaptation in resin fillings with different dentin adhesives. Restor Dent Endod 39(1):24–31. https://doi.org/10.5395/rde.2014.39.1.24
Han SH, Sadr A, Tagami J, Park SH (2016) Non-destructive evaluation of an internal adaptation of resin composite restoration with swept-source optical coherence tomography and micro-CT. Dent Mater 32(1):e1–e7. https://doi.org/10.1016/j.dental.2015.10.009
Chiang YC, Rösch P, Dabanoglu A, Lin CP, Hickel R, Kunzelmann KH (2010) Polymerization composite shrinkage evaluation with 3D deformation analysis from microCT images. Dent Mater 26(3):223–231. https://doi.org/10.1016/j.dental.2009.09.013
Chiang YC (2009) Polymerization shrinkage with light-initiated dental composites. PhD thesis, Ludwig-Maximilians-University Munich, Germany
Rösch P, Chiang YC, Kunzelmann K (2009) Quantification of local polymerisation shrinkage from 3D micro CT images of dental composites. Int J Comput Assist Radiol Surg 4(Suppl. 1):200–201
Kaisarly D, Gezawi ME (2016) Polymerization shrinkage assessment of dental resin composites: a literature review. Odontology 104(3):257–270. https://doi.org/10.1007/s10266-016-0264-3
Cho E, Sadr A, Inai N, Tagami J (2011) Evaluation of resin composite polymerization by three dimensional micro-CT imaging and nanoindentation. Dent Mater 27(11):1070–1078. https://doi.org/10.1016/j.dental.2011.07.008
Takemura Y, Hanaoka K, Kawamata R, Sakurai T, Teranaka T (2014) Three-dimensional X-ray micro-computed tomography analysis of polymerization shrinkage vectors in flowable composite. Dent Mater J 33(4):476–483. https://doi.org/10.4012/dmj.2013-288
Van Ende A, Van de Casteele E, Depypere M, De Munck J, Li X, Maes F, Wevers M, Van Meerbeek B (2015) 3D volumetric displacement and strain analysis of composite polymerization. Dent Mater 31(4):453–461. https://doi.org/10.1016/j.dental.2015.01.018
Lutz F, Luescher B, Ochsenbein H, Muehlemann HR (1976) Adhaesive Zahnheilkunde. Juris Druck und Verlag, Zurich
Hellwig E, Klimek J, Attin T (2003) Restorations with plastic filling materials “Restaurationen mit plastischen Fuellungsmaterialien”. In: Einführung in die Zahnerhaltung. 3rd edition edn. Urban & Fischer, Munich, Germany, pp 145-216
Porte A, Lutz F, Lund MR, Swartz ML, Cochran MA (1984) Cavity designs for composite resins. Oper Dent 9(2):50–56
Kaisarly D (2014) The effect of boundary conditions on the polymerization shrinkage vectors of light-cured dental resin composites. PhD thesis, Ludwig-Maximilians-University Munich, Germany
Kaisarly D, El Gezawi M, Xu X, Rösch P, Kunzelmann K-H (2018) Shrinkage vectors of a flowable composite in artificial cavity models with different boundary conditions: Ceramic and Teflon. J Mech Behav Biomed Mater 77(Supplement C):414–421
Liu Q, Ding J, Chambers DE, Debnath S, Wunder SL, Baran GR (2001) Filler-coupling agent-matrix interactions in silica/polymethylmethacrylate composites. J Biomed Mater Res 57(3):384–393. https://doi.org/10.1002/1097-4636(20011205)57:3<384::AID-JBM1181>3.0.CO;2-F
Rösch P, Blaffert T, Weese J (1999) Multi-modality image registration using local correlation. CARS'99:228-232
Chiang YC, Rösch P, Lin CL, Hickel R, Kunzelmann K (2008) Deformation analysis of composite polymerization shrinkage from μCT images. Annual Meeting of the Academy of Dental Materials
Asmussen E, Jorgensen KD (1972) A microscopic investigation of the adaptation of some plastic filling materials to dental cavity walls. Acta Odontol Scand 30(1):3–21. https://doi.org/10.3109/00016357209004588
Asmussen E, Peutzfeldt A (1999) Direction of shrinkage of light-curing resin composites. Acta Odontol Scand 57(6):310–315. https://doi.org/10.1080/000163599428535
Braga RR, Koplin C, Yamamoto T, Tyler K, Ferracane JL, Swain MV (2013) Composite polymerization stress as a function of specimen configuration assessed by crack analysis and finite element analysis. Dent Mater 29(10):1026–1033. https://doi.org/10.1016/j.dental.2013.07.012
Swanson TK, Feigal RJ, Tantbirojn D, Hodges JS (2008) Effect of adhesive systems and bevel on enamel margin integrity in primary and permanent teeth. Pediatr Dent 30(2):134–140
Choi KK, Ryu GJ, Choi SM, Lee MJ, Park SJ, Ferracane JL (2004) Effects of cavity configuration on composite restoration. Oper Dent 29(4):462–469
Hansen EK (1982) Visible light-cured composite resins: polymerization contraction, contraction pattern and hygroscopic expansion. Scand J Dent Res 90(4):329–335
Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, Vijay P, Van Landuyt K, Lambrechts P, Vanherle G (2003) Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent 28(3):215–235
Price RB, Labrie D, Whalen JM, Felix CM (2011) Effect of distance on irradiance and beam homogeneity from 4 light-emitting diode curing units. J Can Dent Assoc 77:b9
Price RB, Rueggeberg FA, Labrie D, Felix CM (2010) Irradiance uniformity and distribution from dental light curing units. J Esthet Restor Dent 22(2):86–101. https://doi.org/10.1111/j.1708-8240.2010.00318.x
Sampaio CS, Chiu KJ, Farrokhmanesh E, Janal M, Puppin-Rontani RM, Giannini M, Bonfante EA, Coelho PG, Hirata R (2017) Microcomputed tomography evaluation of polymerization shrinkage of class I flowable resin composite restorations. Oper Dent 42(1):E16–e23. https://doi.org/10.2341/15-296-L
Lindberg A, Peutzfeldt A, van Dijken JW (2004) Curing depths of a universal hybrid and a flowable resin composite cured with quartz tungsten halogen and light-emitting diode units. Acta Odontol Scand 62(2):97–101. https://doi.org/10.1080/00016350410006905
Acknowledgements
The authors would like to thank Mr. T. Obermeier for providing technical support and Mrs. G. Dachs and Mrs. E. Koebele for technical support with the micro-CT and SEM images.
Funding
This work was supported by the Department of Conservative Dentistry and Periodontology, Ludwig-Maximilians-University of Munich, Germany.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. The research ethics committee of the medical faculty of Ludwig-Maximilians-University of Munich, Germany, approved the use of extracted human teeth in anonymized form (#078-14).
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Kaisarly, D., El Gezawi, M., Lai, G. et al. Effects of occlusal cavity configuration on 3D shrinkage vectors in a flowable composite. Clin Oral Invest 22, 2047–2056 (2018). https://doi.org/10.1007/s00784-017-2304-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-017-2304-y