
Abstract
Objectives
This study focused on the clinical investigation of the internal and marginal fit of CAD/CAM-fabricated zirconia single crowns produced via conventional and digital impression techniques.
Materials and methods
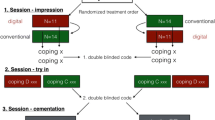
In a private practice, 20 molar teeth, one from each of 20 patients, were prepared with a circumferential 1.0-mm deep chamfer and an occlusal reduction of 1.5 mm. Conventional impression (CI) taking with a polyvinylsiloxane material (Aquasil Monophase + Aquasil XLV; Dentsply, Konstanz, Germany) and intraoral scanning (IS) (Cara TRIOS; Heraeus, Hanau, Germany) of each of the preparations was performed, and then two respective zirconia copings per tooth were produced (20 crowns per group). The marginal and internal fit of the restorations was evaluated employing a replica technique. For statistical analysis, a pairwise comparison (Wilcoxon rank test) was performed.
Results
Zirconia single crowns produced with the IS technique revealed a statistically significant better precision of internal fit only in specific areas (chamfer area/occlusal area). The evaluation of marginal fit showed no significant differences between the two groups. All restorations of both groups offered internal and marginal gaps within the postulated clinical tolerance ranges.
Conclusions
CAD/CAM-fabricated zirconia single crowns produced with CI and IS techniques offer adequate marginal and internal precision. However, the IS technique provides lower internal gaps in some specific areas.
Clinical relevance
The clinical precision of fit of restorations produced with a CI and an IS technique appeared to be equivalent. Therefore, the IS technique can be rated as a suitable alternative for the manufacturing of single crowns.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Conventional impression (CI) taking with reversible or irreversible elastic impression materials is still the common method for generating an exact replica of the intraoral situation and transferring this information to the dental laboratory as the basis for the fabrication of indirect dental restorations [1]. Alternatively, for the computer-assisted design/computer-assisted manufacturing (CAD/CAM) of dental restorations, various intraoral scanning (IS) systems were developed and are in use today [2]. Currently, most of the systems allow for the digitizing of whole quadrants and jaws and additional scanning and correlation of antagonistic teeth [2–4]. The potential benefits of the IS process are an improved patient- and operator-acceptance and potential cost- and time-effectiveness [1, 5, 6].
Nevertheless, the marginal and internal fitting accuracy of dental restorations fabricated in a fully digital workflow is a crucial factor determining the clinical long-term success. An insufficient marginal fit can lead to plaque retention and washout of the luting agent, causing secondary caries, periodontal, and pulpal inflammation or retention loss of the restoration [7–10]. As possible consequences of an insufficient internal fit, loss of axial retention, missing rotation stability, and reduced fracture toughness have to be considered [2, 11].
The fitting accuracy of dental restorations manufactured in a fully digitized workflow with the help of IS and CAD/CAM systems has been evaluated in both in vitro and in vivo conditions. Under in vitro conditions, the results appeared to be superior to conventional impression techniques due to the avoidance of conventional error sources (e.g., the deformation of the impression material or the dimensional change of the model materials) [12–17]. In clinical studies, IS systems were evaluated for fitting accuracy, time efficiency, and patient comfort [1, 18–21]. For the evaluation of IS systems, data on the fitting accuracy of dental restorations under clinical conditions were essential, especially if their design allowed a direct comparison with conventional impressions by applying generally accepted measurement criteria and well-established methods of evaluation [7–10, 22, 23]. For the clinical evaluation of the marginal and internal accuracy of restorations, the replica technique combined with light microscopy has been shown to be a practical and established method [24], offering the possibility of saving time for in vivo analysis of internal and marginal gaps [8, 11, 25–29]. Although there is some controversy regarding the clinically acceptable marginal gap, most authors have accepted a maximum marginal gap of 120 μm as defined by McLean and von Frauenhofer (1971) [7, 8, 11, 25–31]. Clinical studies using the replica technique to evaluate the precision of restorations produced by digital impressions compared with conventional impressions demonstrated equal, or even better, results in the accuracy of digital impressions [18, 28–31]. Despite these positive initial findings, some special aspects of IS devices need to be evaluated. The first generation of IS systems required the application of a scanning powder. More recently introduced technologies based on confocal imaging do not require the application of a scanning powder. This simplifies the clinical handling and might affect the accuracy of the scanning results as the powder layer is omitted. Clinical data on these “powder free” intraoral scanners are still sparse [29, 31]. Moreover, the precision of a IS can be influenced by several factors, including the finishing line location, moisture control, and patient compliance or scanning strategies [31, 32]. Intraoral scans, especially in the molar area where only limited space is available, are challenging. In these areas, the oral cavity limits the handling of the so-called scanning wand. Furthermore, moisture control in these areas is more challenging than in the anterior region [29]. As all IS systems can only scan visible and dry areas, this is of high practical relevance because it can affect the scanning accuracy. To the authors’ best knowledge, clinical studies evaluating the accuracy of powder-free digital impressions solely for molar restorations in comparison with conventional impression are not yet available.
In the present prospective clinical study, the marginal and internal fit of zirconia molar crown copings manufactured with conventional and intraoral digital impression techniques were evaluated by using a replica technique. The null hypothesis was that the zirconia copings based on digital impression taking would offer statistically significant better marginal and internal accuracy than copings produced via conventional impression taking.
Materials and methods
Patients
This study was performed in a private practice in Hanau, Germany. After giving informed consent, 20 patients with treatment plans for single molar crowns were included in the study. Patients had to be of legal age and in need of at least one single crown in the molar region. Inclusion criteria were a tooth free from clinical symptoms, either vital or with a sufficient endodontic treatment Furthermore, a visible finishing line not more than 1 mm below the gingival margin and an adequate level of oral hygiene expressed by the absence of bleeding on probing and a periodontal pocket probing depth of <4 mm were required. Two restorations in each patient per abutment were manufactured—one coping via conventional impression (CI) and one via digital intraoral scanning (IS). All patients received a fitting of copings with the assessment of internal and marginal fit using a replica technique. Thus, 20 specimens per group were evaluated. After the evaluation of clinical fit, the framework that offered the best accuracy was veneered and inserted. This study was approved by the ethics committee of the Georg-August-University, Goettingen, Germany (application no. 5/11/11), and all patients gave written informed consent.
Tooth preparation
All abutment teeth received an adhesive core built-up with a self-curing (CoreUp, Kaniedenta, Herford, Germany) using an adhesive system (OptiBond FL, Kerr GmbH, Rastatt, Germany). The preparation was performed under local anesthesia with the objective of getting a 90° chamfer finish line with a circumferential reduction of 1.0 mm and an occlusal reduction of 1.5 mm. The convergence angle was set at approximately 6°–10°, and all edges were rounded. After preparation, the teeth received a provisional restoration fabricated from an auto-curing resin-based material (Luxatemp, DMG, Hamburg, Germany). Impressions were taken after a minimum waiting time of 7 days to allow complete healing of the soft tissues. Before taking digital and conventional impressions, retraction cords (Ultra Clean Cut, Ultradent, Cologne, Germany) were applied using the double-cord technique for rendering of the finish line (Fig. 1). A flexible aid for full mouth access (Optragate, Ivoclar Vivadent, Schaan, Liechtenstein) and absorbent pads (Dry Tips, Microbrush International, Crafton, USA.) were used for moisture control in the working field.

Prepared tooth 26 with retraction cords applied using the double-cord technique prior to intraoral scanning
Intraoral scan
Prior to the conventional impression taking, the digital intraoral scan using the cara TRIOS system (Heraeus Kulzer, Hanau, Germany) was performed. The scanner was calibrated before scanning each patient, and scanning was performed according to the manufacturer’s instructions to capture each quadrant separately. The quadrant with the prepared tooth was scanned first, followed by a quadrant-scan of the opposing teeth. The interocclusal registration was performed by a buccal scan with teeth in maximal intercuspidation. No powder application was required for this system. The resulting digital data set was directly transferred to a CAD software (Dentaldesigner 2014, 3Shape a/S, Copenhagen, Denmark) digital design (CAD) of the zirconia copings. Additionally, a working model based on this data set was printed by scan LED technology using a light-curing resin (FotoDent LED.A, Dreve Dentamid, Unna, Germany) in a centralized production facility. According to the manufacturers’ information, the models were fabricated with a layer thickness of 50 μm and a lateral resolution (edge length of a pixel) of 32 μm. This model was used for the manual adjustments of the copings before the clinical fitting.
All scans and impressions were taken by the same dentist (S.R.) who was trained by the manufacturer. Twenty restorations were scanned and manufactured before the study began.
Conventional impression technique
For conventional impressions, a one-step putty-wash technique with a polyvinylsiloxane material (Aquasil Monophase + Aquasil XLV, Dentsply DeTrey, Konstanz, Germany) was used according to the manufacturer’s instructions. To improve the accuracy of the impression, custom impression trays based on study models were implemented. The antagonist arch impression was taken using an alginate material (Blueprint Crème, Dentsply DeTrey GmbH, Konstanz, Germany). The occlusal relationship was recorded in maximal intercuspidation using an auto-curing polyvinylsiloxane material (Futar D, Kettenbach GmbH, Eschenburg, Germany). The impressions were disinfected prior to forwarding them to the dental technician. To create a data set for the digital design (CAD) of the zirconia copings, the impressions were used to fabricate stone models (Sherapure, SHERA, Lemfoerde, Germany) for indirect digitalization via a model scanner (3shape D700, cara TRIOS, Heraeus Kulzer, Hanau, Germany).
Manufacturing of the copings
All copings for both groups (CI and IS) were designed by the same experienced dental master technician using the same software (Dental Designer 2014, 3Shape a/S, Copenhagen, Denmark). All restorations were designed and manufactured using the same settings and following the manufacturer’s recommendations (cement spacer, 40 μm, minimum wall thickness, 500 μm, edge reinforcement, 200 μm). For producing the frameworks, pre-sintered Yttria-stabilized zirconia blanks were milled on a five-axis milling unit (Side Hawk 550, Ops-Ingersoll GmbH, Burbach Germany) under dry conditions and sintered to full density in a centralized production center (Cara, Heraeus Kulzer, Hanau, Germany). Then, all copings were adjusted with a maximum adjustment time of 5 min (CI group: on stone models; IS group: on printed models).
Clinical recording of fit
To assess the clinical accuracy of the copings regarding marginal and internal fit, the inner surfaces of the copings were coated with a white-colored low-viscosity silicone (Coltex extrafine, Coltène/Whaledent, Langenau, Germany) before seating it on the respective abutment with maximum finger pressure for 10 s. After 4 min, the copings were carefully removed, and to stabilize the adherent white thin silicone film, the crowns were filled with a more rigid orange-colored silicone (Aquasil Ultra XLV, Dentsply DeTrey, Konstanz, Germany) to obtain a good contrast for the discrimination of the different layers. Then, the silicone replica was carefully removed from the coping for further processing (Fig. 2).

Silicone replica undercoated with an orange-colored silicone after removal of the coping
Replica specimen preparation
In addition to the undercoating of the white silicone layer representing the marginal and internal gap with the orange silicone (replacing the abutment), a custom-made box was used to cover the replica specimens with a blue-colored silicone (Aquasil Ultra LV, Dentsply DeTrey, Konstanz, Germany), thus replacing the framework. This box was designed to ensure that the position of all specimens was exactly centralized in the encasing blue (opaque) silicone layer, with all specimens having the same mesio-distal orientation. This allowed for sectioning into four pieces (respectively the measurement locations) of each specimen in the mesio-distal and bucco-oral direction in a reproducible and comparable manner (Fig. 3). Sectioning was carried out with razor blades (Wilkinson Sword Classic, Wilkinson, Solingen, Germany) that were used for only one cut each to avoid wearing effects.

Custom-made box for covering and sectioning the three-layered replica specimens
Measurements of internal and marginal fit
The four sections of each specimen were used for measuring the internal and marginal gaps by one calibrated examiner. Two sides of each section (mesio-distal and bucco-oral) were evaluated at 6 points for internal gap (ca = chamfer area, aw = axial wall, aw min = axial wall minimum discrepancy, aw max = axial wall maximum discrepancy, aot = axio-occlusal transition area, oa = occlusal area) and at 2 points for marginal gap (mg = marginal gap, absol mg = absolute marginal gap according to Holmes et al. (1989) [22], (Fig. 4). Replica film thickness was measured on digital photographs captured by the integrated camera of a light microscope with a magnification factor of ×35 (Leica EZ4D, Leica Mikrosysteme, Wetzlar, Germany) and a special measuring software (Axio Vision LE 4.8, Carl Zeiss Microscopy GmbH, Jena, Germany) after calibration.

Three-layered silicone replica (blue = restoration, white = marginal/internal gap, orange = abutment) with all measuring points: absol mg absolute marginal gap according to Holmes et al. (1989), mg marginal gap, ca chamfer area, aw axial wall (with minimum and maximum), aot axio-occlusal transition area, oa occlusal area
Statistical analysis
For statistical analysis, values were exported to a spreadsheet (Microsoft Excel, Microsoft Corp, Redmond, WA, USA). The Shapiro-Wilk test (p ≤ 0.05) was used to test for a normal distribution. Levene’s test was used to assess for homogeneity of variance. The Wilcoxon rank test for pairwise comparisons was performed to evaluate significant differences between the CI and the IS technique and to compare within the two series regarding specific locations. Analysis was carried out using the software MATLAB (The Mathworks Incorp., Natick, MA, USA). The significance level was set p ≤ 0.05. Mean values were reported in descriptive statistics, in addition to medians and interquartile ranges, to guarantee a good understanding of the data and to enable a comparison with other studies, even though they give only limited information on the distribution of the data.
Results
The Shapiro-Wilk test displayed a non-normal data distribution, and Levene’s test displayed no significant differences between the two groups regarding equality of variances. Thus, a non-parametric testing procedure (Wilcoxon rank test) for pairwise comparisons was used to evaluate significant differences between the CI and the IS copings regarding internal or marginal fit.
Statistical pre-tests regarding the influence of the sectioning direction (mesio-distal, bucco-oral) for internal and marginal adaptation of the copings revealed only one location (“aot”) within the IS group that showed significantly different values (206.13 ± 76.49 μm for bucco-oral sectioning direction vs. 167.72 ± 74.22 μm for mesio-distal direction). Therefore, for further statistical analysis, the directions of sectioning were pooled within both groups.
When comparing both groups (CI vs. IS), only two locations revealed significantly better internal accuracy for IS: “chamfer area” (ca) (117.94 ± 74.21 μm vs. 147.88 ± 63.88 μm) and “occlusal area” (oa) (164.22 ± 73.17 μm vs. 207.60 ± 69.99 μm) (p ≤ 0.05) (Figs. 5 and 6). All values for internal fit of the CI and the IS group are shown in Table 1. The lowest values for internal accuracy in both groups was found at the axial wall (aw min) (CI 43.36 ± 36.98 μm, IS 34.79 ± 28.67 μm), whereas the poorest fit could be found in the “occlusal area” (oa) for the CI group (207.60 ± 69.99 μm) and in the “axio-occlusal transition area” (aot) for the IS group (187.17 ± 77.35 μm).

Box plot diagram showing mean internal gaps in the “chamfer area” for the CI and the IS group. Zirconia copings produced by intraoral scanning revealed significantly lower values for the internal gap (p = 0.0002). Asterisks represent extreme values >1.5X interquartile range

Box plot diagram showing mean internal gaps in the “occlusal area” for the CI and the IS group. Zirconia copings produced with the intraoral scanning revealed significantly lower values for the internal gap (p = 0.00004). Asterisks represent extreme values >1.5X interquartile range
When comparing the values of the CI group and IS group, no significant differences could be demonstrated regarding marginal accuracy (CI 82.17 ± 75.17/IS: 87.4 ± 91.2). All values for marginal fit for both groups are shown in Table 2.
Discussion
In this study, the internal and marginal fitting accuracy of zirconia single copings produced with one CAD/CAM system (cara TRIOS, Heraeus Kulzer, Hanau, Germany) on the basis of conventional and digital impression techniques were comparatively evaluated.
The results of this study reveal that zirconia copings produced via intraoral scanning offered an equivalent marginal fitting quality (CI, 82.17 ± 75.17/IS: 87.4 ± 91.2). A better internal accuracy was only determined for two out of six locations (chamfer area, occlusal area) in relation to the copings manufactured with conventional impressions. Therefore, the null hypothesis that zirconia copings on the basis of digital impression taking would offer statistically significant better marginal and internal accuracy than copings produced by conventional impression taking has to be partially rejected.
For the interpretation of the results of the present study, it is important to consider the limitation of in vivo measurements regarding fitting accuracy. An in vivo measurement of the marginal and internal fitting accuracy is challenging, as a direct evaluation (requiring a removal of the cemented restoration from the oral cavity) is not possible. Therefore, a validated and commonly accepted measuring technique is the prerequisite for a comparison of the findings with other studies. For the in vivo assessment of the clinical fit of the copings, the silicone replica technique is a reliable, non-invasive, well-established [8, 24], and recently multiply used method [19, 27–31]. Especially in the setting of the present study with a visible preparation limit and only slight subgingival margins, the most foreseeable limitations of this technique (inaccessible marginal areas) could be eliminated. Moreover, in the present study, some methodical steps were modified to overcome the inherent limitations of this technique. The white silicone film (Coltex extrafine, Coltène/Whaledent, Langenau, Germany) representing the internal and marginal gaps was undercoated with a rigid orange-colored silicone (Aquasil Ultra XLV, Dentsply DeTrey, Konstanz, Germany) and additionally covered with blue silicone (Aquasil Ultra LV, Dentsply DeTrey, Konstanz, Germany), thus improving the contrast and visibility, especially in areas where the gaps in the silicone film were very thin. In earlier studies, especially, the analysis of the marginal area was rated critical [24, 27, 29]. The three-layer silicone technique used in the present study in combination with a special box for covering and sectioning the specimens ensured a reproducible position (Fig. 3), i.e., a perpendicular axis during the measurement with the light microscope (Leica EZ4D, Leica Mikrosysteme, Wetzlar, Germany) and improved the accessibility for measurements in such critical areas. Measuring points (Fig. 4) were set according to the literature to provide comparability with earlier studies [29, 31].
Before intraoral scanning and conventional impression taking, retraction cords (Ultra Clean Cut, Ultradent, Cologne, Germany) were applied using the double-cord technique. First, the intraoral scan was performed with both retraction cords remaining in the sulcus. Then, the upper cord was removed, and the conventional impression was applied. Thus, randomization was not necessary because both impression techniques were realized in one operation.
A specific aspect of the present study is the fact that only molar teeth were included. Thus, potential influencing factors related to handling of the scanning wand in different areas of the oral cavity (anterior area is easier to access than the posterior region) were eliminated.
In the present study, the marginal and internal fitting accuracy of zirconia copings produced by two different fabrication procedures was evaluated. The marginal and internal fit is influenced by the type of impression technique, as well as by the fabrication technique [33]. Therefore, the conventional impression was used to fabricate a master model that was scanned with a laboratory scanner to generate a comparable data set similar to that produced by intraoral scanning. To avoid any bias of the fabrication process for both impression techniques, the same CAD software, the same zirconia material, and an identical milling technique were used. Nevertheless, it must be considered that the present study evaluates the accuracy of the entire process chain, i.e., impression taking, model accuracy, milling process, and manual adaption. Therefore, it is difficult to credit the achievable clinical fitting accuracy to just a single factor only, e.g., accuracy of the scanning device. To avoid a potential bias during analysis, the calibrated examiner was not the same as the one who performed the clinical procedures.
However, there are limitations regarding the methods in this study. To simulate the best the clinically achievable fit, all restorations were manually adapted to the respective working models. Although a manual adaptation is routine in clinical procedures, it should be considered that this step can level potential effects of the fabrication technique on the achievable fitting accuracy. Above all, the precision of the working models is important for the digital workflow. In the present study, an additive fabrication technique was applied (manufacturers’ recommended layer thickness, 50 μm with a lateral resolution of 32 μm). The restorations were evaluated regarding internal and marginal fit without cementation on the respective abutment teeth. Increases in marginal gaps due to the cementation process might occur. However, the silicone used for the fixation of the copings during the fitting procedure might act as a substitute for the luting agent, thus simulating a cementation process [11, 24, 26, 27]. Furthermore, in the present study, non-veneered copings were used for clinical assessment of the marginal and internal fit, and this procedure avoided an incomplete seating of the restoration due to too strong proximal contacts. On the other hand, significant changes may occur during veneering [28, 34]. Furthermore, another limitation was inherent to the replica technique itself due to its two-dimensional exposition, which prevented circumferential analysis [24, 26–29].
The discussion of whether restorations produced via intraoral scanning offer a comparable or even superior precision of fit than restorations based on conventional impressions is still in progress [2–4, 32]. Concerning the marginal fit of CAD/CAM-generated restorations based on intraoral scanning, some in vitro studies demonstrated better marginal precision than restorations produced with conventional impressions [12–17]. This is supported by the findings of several in vivo studies [18, 28–31]. In contrast, there are also in vitro studies [12, 13, 16] that show no significant differences regarding marginal accuracy when IS and CI groups of restorations were compared. At least one clinical study [29] comparing three different intraoral scanning devices demonstrated significant differences in marginal and internal accuracy within the three tested IS systems, thus revealing a significant influence of the IS system used.
The results of the present study should preferably be discussed in the context of the results of other clinical studies using a replica technique and a comparable measuring technique for comparing CI and IS.
The overall dimensions of the values regarding marginal and internal integrity that were evaluated in the present study are in good accordance with recently performed clinical investigations [29–31]. In the present study, a mean marginal gap of 87.4 ± 91.2 μm was reported for crowns fabricated on the basis of IS. This is in good accordance with the results of other comparative clinical trials with posterior teeth. Pradies et al. (2015) [30] reported a mean marginal gap of 76.3 ± 65.3, and in another clinical study, a mean marginal gap for crowns fabricated by IS of 80.3 ± 26.4 μm was detected [31]. However, mean values for marginal and lS gaps for restorations based on digital impressions using active wave front sampling in two clinical studies [18, 28] appeared to be in a lower dimension with mean values ranging from 50 to 60 μm. There is only one comparative study using the same intraoral scanning device as in the present study (Cara Trios) [29]. In this study, a mean marginal gap of 112 μm was detected. It was not significantly different from the values found for CI (113 μm) [29]. These values are somewhat higher than in the present study (CI, 82.17 ± 75.17/IS, 87.4 ± 91.2). A possible explanation can be found in the different design parameters. In the present study, the cement gap was set to 40 μm, while in the study by Boeddinghaus et al. (2015), a cement gap of 90 μm was used [29]. Both studies found no statistically significant differences in the marginal gap size for crowns fabricated by IS (Heraeus cara Trios) and crowns fabricated by CI. Therefore, the findings of Boeddinghaus et al. (2015) confirm the results of the present study [29].
The findings for the internal fit can only be compared with the results from comparative clinical trials using another IS system as in the present study. In the present study, the best internal fitting quality for both fabrication techniques was detected at the measuring point at the axial wall (CI, 73.9 ± 40/IS, 74.68 ± 42.43) This is in good accordance with the values reported by Ahrberg et al. (2015) [28]. For identical measuring points, they reported a mean internal gap of 88.27 ± 24.77 μm for IS using an active wavefront sampling technique (Lava C.O.S, 3 M Espe, Seefeld, Germany) and 92.13 ± 49.87 for CI.
In the present study, the highest mean values for internal gaps were found in the occlusal area (IS, 167.22 ± 73.17/CI, 207.6 ± 69.99). Again, this is in good accordance with the findings of other recently published clinical trials, revealing the highest internal gaps in the occlusal area [19, 20, 28, 31] In these studies, the mean values for the internal gap in the occlusal area ranged from 155 to 297 μm. Therefore, the findings of the present study are in the lower range of the published values.
In an in vivo study using a comparable method, a better internal accuracy for IS was location-dependent (for chamfer and occlusal area only) [28]. This is in good accordance with the methods and findings of the present study.
To the authors’ knowledge, only one clinical study [28] using the replica technique is available that evaluated the “absolute marginal gap” (“absol mg”) according to the criteria of Holmes et al. (1989) [22]. This criterion appeared to be clinically relevant because it considers horizontal discrepancy (in means of over- or under-extended) margins. Therefore, it was additionally evaluated in the present study, revealing distinctively wider gaps for “absol mg” than for “mg” (138.17 ± 99.50 μm vs. 82.17 ± 75.17 μm for the CI group; 151.68 ± 113.37 μm vs. 87.40 ± 91.21 μm for the IS group).
Summarizing the available results from clinical studies comparing IS and CI, it can be stated that all studies demonstrated sufficient values for marginal gaps below the postulated threshold of 120 μm defined by McLean and von Fraunhofer (1971) [25]. Most of the studies revealed a marginal and internal fitting accuracy equivalent or better than restorations fabricated by CI. Nevertheless, for both fabrication techniques, a reduced internal fitting quality has to be expected in the occlusal areas.
Many authors concluded that intraoral scanning is a suitable alternative for the processing of dental prosthetic restorations [2–4, 13, 15–18, 20, 28–31] However, some clinical limitations regarding the indication of intraoral scanning still have to be mentioned, e.g., deep subgingival preparations, combined fixed/removable prostheses, or implant restorations. Moreover, relatively high investment costs and an initially flat learning curve have to be considered [2–4, 32]. Furthermore, the accuracy could be influenced depending on the type of intraoral scanning scope. For the TRIOS system tested in the present study, it has been demonstrated that the accuracy of the respective restorations was acceptable up to a scanning scope of half an arch, whereas the resulting precision on the basis of lab-side scanning in any scope was acceptable [35].
Conclusion
Within the imitations of the study, CAD/CAM-fabricated single tooth restorations in the posterior region produced by an intraoral scanning system using confocal imaging offer a comparable, or even better, precision of marginal and internal fitting accuracy than restorations based on conventional impressions in combination with the laboratory scanning technique. Therefore, the complete digital workflow including a digital impression technique can be rated a suitable alternative for conventional impressions, followed by a lab-side digitization, and a CAD/CAM manufacturing process in indications where the preparation limit is visible and only slightly subgingival.
References
Gjelvold B, Chrcanovic BR, Korduner EK, Collin-Bagewitz I, Kisch J (2015) Intraoral digital impression technique compared to conventional impression technique. A randomized clinical trial. J Prosthodont. doi:10.1111/jopr.12410 [Epub ahead of print]
Reich S, Vollborn T, Mehl A, Zimmermann M (2013) Intraoral optical impression system: an overview. Int J Comput Dent 16:143–162
Ting-Shu S, Jian S (2015) Intraoral digital impression technique: a review. J Prosthodont 24:313–321
Zimmermann M, Mehl A, Mörmann WH, Reich S (2015) Intraoral scanning systems—a current overview. Int J Comput Dent 18:101–129
Lee SJ, Macarthur RX 4th, Gallucci GO (2013) An evaluation of student and clinician perception of digital and conventional implant impressions. J Prosthet Dent 110(5):420–423
Yuzbasioglu E, Kurt H, Turunc R, Bilir H (2014) Comparison of digital and conventional impression techniques: evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 14:10–17
Hunter AJ, Hunter AR (1990) Gingival margins for crowns: a review and discussion. Part II: discrepancies and configurations. J Prosthet Dent 64:636–642
Karlsson S (1993) The fit of Procera titanium crowns. An in vitro and clinical study. Acta Odontol Scand 51:129–134
Contrepois M, Soenen A, Bartala M, Laviole O (2013) Marginal adaptation of ceramic crowns: a systematic review. J Prosthet Dent 110:447–454
Boitelle P, Mawussi B, Tapie L, Fromentin O (2014) A systematic review of CAD/CAM fit restoration evaluations. J Oral Rehabil 41:853–874
Wettstein F, Sailer I, Roos M, Hämmerle CH (2008) Clinical study of the internal gaps of zirconia and metal frameworks for fixed partial dentures. Eur J Oral Sci 116(3):272–279
Seelbach P, Brueckel C, Wostmann B (2013) Accuracy of digital and conventional impression techniques and workflow. Clin Oral Investig 17:1759–1764
Almeida e Silva JS, Erdelt K, Edelhoff D, Araújo É, Stimmelmayr M, Vieira LC, Guth J (2014) Marginal and internal fit of four-unit zirconia fixed dental prostheses based on digital and conventional impression techniques. Clin Oral Investig 18:515–523
Keul C, Stawarczyk B, Erdelt KJ, Beuer F, Edelhoff D, Güth JF (2014) Fit of 4-unit FDPs made of zirconia and CoCr-alloy after chairside and labside digitalization—a laboratory study. Dent Mater 30(4):400–407
Tidehag P, Ottosson K, Sjögren G (2014) Accuracy of ceramic restorations made using an in-office optical scanning technique: an in vitro study. Oper Dent 39(3):308–316
Abdel-Azim T, Rogers K, Elathamna E, Zandinejad A, Metz M, Morton D (2015) Comparison of the marginal fit of lithium disilicate crowns fabricated with CAD/CAM technology by using conventional impressions and two intraoral digital scanners. J Prosthet Dent 114(4):554–559
Ueda K, Beuer F, Stimmelmayr M, Erdelt K, Keul C, Güth F (2015) Fit of 4-unit FDPs from CoCr and zirconia after conventional and digital impressions. Clin Oral Investig. doi:10.1007/s00784-015-1513-5 [Epub ahead of print]
Syrek A, Reich G, Ranftl D, Klein C, Cerny B, Brodesser J (2010) Clinical evaluation of all-ceramic crowns fabricated from intraoral digital impressions based on the principle of active wavefront sampling. J Dent 38:553–559
Brawek PK, Wolfart S, Endres L, Kirsten A, Reich S (2013) The clinical accuracy of single crowns exclusively fabricated by digital workflow--the comparison of two systems. Clin Oral Investig 17(9):2119–2125
Tamim H, Skjerven H, Ekfeldt A, Rønold HJ (2014) Clinical evaluation of CAD/CAM metal-ceramic posterior crowns fabricated from intraoral digital impressions. Int J Prosthodont 27(4):331–337
Selz CF, Bogler J, Vach K, Strub JR, Guess PC (2015) Veneered anatomically designed zirconia FDPs resulting from digital intraoral scans: preliminary results of a prospective clinical study. J Dent 43(12):1428–1435
Holmes JR, Bayne SC, Holland GA, Sulik WD (1989) Considerations in measurement of marginal fit. J Prosthet Dent 62:405–408
Abduo J, Lyons K, Swain M (2010) Fit of zirconia fixed partial denture: a systematic review. J Oral Rehabil 37:866–876
Laurent M, Scheer P, Dejou J, Laborde G (2008) Clinical evaluation of the marginal fit of cast crowns—validation of the silicone replica method. J Oral Rehabil 35:116–122
McLean JW, von Fraunhofer JA (1971) The estimation of cement film thickness by an in vivo technique. Br Dent J 131:107–111
Fransson B, Oilo G, Gjeitanger R (1985) The fit of metal-ceramic crowns, a clinical study. Dent Mater 1:197–199
Reich S, Uhlen S, Gozdowski S, Lohbauer U (2011) Measurement of cement thickness under lithium disilicate crowns using an impression material technique. Clin Oral Investig 15:521–526
Ahrberg D, Lauer CL, Ahrberg M, Weigl P (2015) Evaluation of fit and efficiency of CAD/CAM fabricated all-ceramic restorations based on direct and indirect digitalization: a double-blinded, randomized clinical trial. Clin Oral Investig. doi:10.1007/s00784-015-1504-6 [Epub ahead of print]
Boeddinghaus M, Breloer ES, Rehmann P, Wöstmann B (2015) Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clin Oral Investig 19:2027–2034
Pradíes G, Zarauz C, Valverde A, Ferreiroa A, Martínez-Rus F (2015) Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions based on wavefront sampling technology. J Dent 43(2):201–208
Zarauz C, Valverde A, Martinez-Rus F, Hassan B, Pradies G (2015) Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions. Clin Oral Investig. doi:10.1007/s00784-015-1590-5 [Epub ahead of print]
Ender A, Mehl A (2013) Influence of the scanning strategies on the accuracy of digital intraoral scanning systems. Int J Comput Dent 16:11–21
Rinke S, Fornefett D, Gersdorff N, Lange K, Roediger M (2012) Multifactorial analysis of the impact of different manufacturing processes on the marginal fit of zirconia copings. Dent Mater J 31(4):601–609
Pak HS, Han JS, Lee JB, Kim SH, Yang JH (2010) Influence of porcelain veneering on the marginal fit of Digident and Lava CAD/CAM zirconia ceramic crowns. J Adv Prosthodont 2:33–38
Su TS, Sun J (2015) Comparison of repeatability between intraoral digital scanner and extraoral digital scanner: an in vitro study. J Prosthodont Res 59:236–242
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This study was financially supported by Heraeus Kulzer GmbH, Hanau, Germany.
Ethical approval
This study was approved by the ethics committee of the Georg-August-University, Goettingen, Germany (application no. 5/11/11).
Informed consent
All patients included in this study gave written informed consent.
Rights and permissions
About this article

Cite this article
Rödiger, M., Heinitz, A., Bürgers, R. et al. Fitting accuracy of zirconia single crowns produced via digital and conventional impressions—a clinical comparative study. Clin Oral Invest 21, 579–587 (2017). https://doi.org/10.1007/s00784-016-1924-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-016-1924-y