
Abstract
Objective
This study aims to clinically evaluate the treatment of mandibular class II furcation defects with enamel matrix derivative (EMD) and/or a bone substitute graft made of β-tricalcium phosphate/hydroxyapatite (βTCP/HA).
Materials and methods
Forty-one patients, presenting a mandibular class II buccal furcation defect, probing pocket depth (PPD) ≥4 mm and bleeding on probing, were included. They were randomly assigned to the groups: 1—EMD (n = 13); 2—βTCP/HA (n = 14); 3—EMD + βTCP/HA (n = 14). Plaque index (PI), gingival index (GI), relative gingival margin position (RGMP), relative vertical and horizontal attachment level (RVCAL and RHCAL), and PPD were evaluated at baseline and 6 and 12 months. The mean horizontal clinical attachment level gain was considered the primary outcome variable.
Results
No significant intragroup differences were observed for RGMP, but significant changes were observed for RVCAL, RHCAL, and PPD for all groups (p < 0.05). After 12 months, the mean horizontal clinical attachment level gain was 2.77 ± 0.93 mm for EMD, 2.64 ± 0.93 mm for βTCP/HA, and 2.93 ± 0.83 mm for EMD + βTCP/HA, with no significant differences among the groups. At the end of the study, 85.3 % of the sites were partially closed; however, no complete closure was observed.
Conclusion
EMD + βTCP/HA does not provide a significant advantage when compared to the isolated approaches. All three tested treatments promote significant improvements and partial closure of class II buccal furcation defects. Based on its potential to induce periodontal regeneration, EMD may be considered an attractive option for this type of defect, but complete closure remains an unrealistic goal.
Clinical relevance
The partial closure of buccal furcation defects can be achieved after the three tested approaches. However, the combined treatment does not provide a significant benefit when compared to the isolated approaches.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Several methods have been used to treat furcation defects, such as non-surgical scaling and root planing with manual and power-driven scalers, open flap debridement, resective treatment, and regenerative approaches [1]. Previous studies have reported good results when guided tissue regeneration (GTR) was used to treat mandibular class II furcation defects, achieving statistically greater clinical improvement when compared with non-regenerative procedures [2–4].
Enamel matrix derivative proteins (EMD) have been clinically used as an attempt to reproduce the events that occur during cementogenesis, in which amelogenin, secreted by Hertwig’s epithelial root sheath (HERS), induces the formation of acellular extrinsic fiber cementum, periodontal ligament, and alveolar bone. It may promote periodontal ligament cell proliferation and increased protein synthesis and mineral nodule formation by the cells. Another interesting effect of EMD would be the reduction in the local pathogenic flora, creating a more favorable environment for periodontal regeneration [5–10].
Considering the treatment of furcation defects, the results obtained with EMD application may be comparable to those achieved with GTR [11, 12] and superior to what have been reported with open-flap debridement [13] for clinical attachment level, vertical and horizontal bone levels, and resolution of the furcation defect [14]. However, the complete closure of furcation defects does not seem to be a commonly attainable outcome with the present treatment options. Jepsen [11] showed that complete closure of mandibular furcation treated with EMD was observed in 17 % of the sites compared to 8 % with GTR.
Bone replacement grafts (bone grafts and bone graft substitutes) may provide the structural framework for clot stabilization, maturation, and remodeling that supports bone formation in osseous defects [15]. Both hydroxyapatite (HA) and β-tricalcium phosphate (βTCP) are widely employed materials in dental and periodontal surgery. They are known to be osteoconductive and to enhance bone filling in periodontal defects [16, 17].
It can be hypothesized that the association of EMD with a bone substitute might improve the clinical results in furcation lesions. Thus, the aim of this clinical trial is to evaluate the treatment of mandibular class II furcation defects with the association of enamel matrix derivative (EMD) and a bone substitute graft made of β-tricalcium phosphate/hydroxyapatite (βTCP/HA) when compared to the isolated use of each material.
Materials and methods
Study design
This is a randomized, parallel, blinded, clinical trial designed to evaluate the treatment of mandibular class II furcation defects with enamel matrix derivative (EMD) along with a bone substitute graft (βTCP/HA) when compared to the isolated therapies. The study protocol has been approved by the Ethics Committee of the Piracicaba Dental School, State University of Campinas—UNICAMP (#035/2007). All patients received a detailed description of the proposed treatment and gave their written informed consent.
The patients were randomly assigned to the following treatment groups:
-
Group 1:
During flap access surgery, the granulation tissue was removed and the root surfaces were carefully instrumented with ultrasonic and hand instruments. The furcation defects in this group received the application of enamel matrix derivative (EMD—Emdogain®; Straumann, Basel, Switzerland).
-
Group 2:
During flap access surgery, the granulation tissue was removed and the root surfaces were carefully instrumented with ultrasonic and hand instruments. The furcation was filled with a bone substitute consisting of β-tricalcium phosphate/hydroxyapatite (βTCP/HA—Bone Ceramic®; Straumann, Basel, Switzerland)
-
Group 3:
During flap access surgery, the granulation tissue was removed and the root surfaces were carefully instrumented with ultrasonic and hand instruments. The furcation was filled with a mixture of enamel matrix derivative proteins (EMD) (Emdogain®; Straumann, Basel, Switzerland) and bone substitute consisting of βTCP/HA (Bone Ceramic®; Straumann, Basel, Switzerland). Immediately after debridement, EMD was applied on the root surfaces. The remaining part of the material in the syringe was then mixed with the bone substitute on a sterile dappen. This mixture was used to completely fill the defect (EMD + βTCP/HA).
Randomization and allocation concealment
The treatment for each buccal furcation defect was determined during the surgical procedure (after flap elevation and root/defect debridement) using a previously made computer-generated list and opaque envelopes. The allocation concealment was conducted by a researcher (MPS) not involved in the examinations and surgical procedures. The randomization code was not broken until all data had been collected and fully statistically analyzed. Therefore, the patient, the clinical examiner, and the statistician were not aware about the treatment group during the study procedures.
Population screening
Potential patients were selected from those referred to the Graduate Clinic of the Piracicaba Dental School. All patients received a complete periodontal examination, including anamnesis, a full-mouth periodontal probing, and radiographic examination. One furcation defect per patient was chosen. The furcation defects were classified on a three-stage scale [18] using a Nabers Probe (Hu-Friedy). The study inclusion criteria were (1) males and females, age ≥35 years and with the diagnosis of moderated chronic periodontitis [19]; (2) presence of a mandibular molar with buccal class II furcation defect, presenting horizontal PD ≥4 mm, bleeding on probing (BOP), minimum (<1 mm) or no gingival recession after non-surgical therapy; (3) good general health; (4) at least 2 mm of keratinized tissue; and (5) minimum interproximal bone loss (<2 mm). The patients who presented the following conditions were excluded from the study: (1) were pregnant or lactating; (2) required antibiotic pre-medication for the performance of periodontal examination and treatment; (3) suffered from any other systemic diseases (cardiovascular, pulmonary, liver, cerebral, diseases, or diabetes); (4) had received antibiotic treatment in the previous 3 months; (5) were taking long-term anti-inflammatory drugs; (6) had received a course of periodontal treatment within the last 6 months; (7) with non-vital/endodontically treated experimental tooth; and (8) were smokers.
Non-surgical treatment
All the subjects received a full-mouth periodontal treatment before the surgical procedure. The same operator performed the treatment at the furcation sites with an ultrasonic device (Cavitron; Dentsply, NY, USA) and specific tips for furcation debridement (PQ2N7; Hu-Friedy, Chicago, IL, USA). The subjects underwent motivation sessions, during which oral hygiene instructions were given to ensure proper level of oral hygiene before the surgical procedure. These sessions were repeated as needed, with special attention for the furcation areas, until subjects showed the ability to maintain good plaque control, as evidenced by pre-treatment plaque and bleeding scores of 20 % or less.
Clinical parameters
The following clinical parameters were assessed immediately before the surgical procedure. Full-mouth plaque score (FMPS) and full-mouth bleeding score (FMBS) were calculated after assessing dichotomously the presence of plaque and BOP (from the bottom of the pocket when probing with a manual probe) and calculating the percentage of positive sites. The presence of plaque and BOP was also dichotomously evaluated at the buccal furcation site included in the study. Probing depth (PD), relative gingival margin position (RGMP), and relative vertical clinical attachment level (RVCAL) were evaluated using a PCP-15 periodontal Probe (Hu-Friedy, Chicago, IL, USA). The relative horizontal clinical attachment level (RHCAL) was measured with the same type of probe (PCP-15 Periodontal Probe; Hu-Friedy, Chicago, IL, USA) as the distance between the deepest point reached by the probe when introduced horizontally into the furcation and the lower border of the stent. All these parameters were evaluated at one specific site at the buccal furcation entrance, determined by a groove made on an individually manufactured acrylic stent and recorded to the nearest 0.5 mm. The assessments of RGMP, PD, RVCAL, and RHCAL were performed at baseline and 6 and 12 months after the surgical procedure by one blinded trained examiner (L.A.Q.).
Investigator calibration
Initially, a total of 15 non-study subjects presenting buccal class II furcations were selected. The designated examiner measured the RVCAL and RHCAL of all patients, twice, within a period of 24 h (observing an interval of more than 1 h between examinations). The examiner was judged to be reproducible after fulfilling the pre-determined success criteria (the percentage of agreement within ±1 mm between repeated measurements had to be at least 90 %). The intra-class correlation was calculated to each parameter, resulting in 90 % reproducibility for RVCAL and 91 % for RHCAL.
Surgical procedures
All the surgical procedures were performed by the same experienced surgeon (E.A.S.). Before surgery, intraoral antisepsis was performed with 0.12 % chlorhexidine rinse solution and extraoral antisepsis was carried out with iodine solution. Following local anesthesia, sulcular incisions were made, and full-thickness flaps were raised at the buccal surface of the experimental sites, extending to the two adjacent teeth (or ridge, if the adjacent tooth was absent). Granulation tissue as well as the visible calculus on the root surface (if present) was removed with hand curettes (Gracey; Hu-Friedy) and with an ultrasonic device (Cavitron; Dentsply, Tulsa, OK, USA) with specific tips for furcation instrumentation (UI25KFPset; Hu-Friedy). The diagnosis of the class II furcation defect was then confirmed using a Nabers probe (Hu-Friedy). At this point, the opaque envelope was open and the defect could be assigned to one of the following procedures: EMD (Emdogain®; Straumann, Basel, Switzerland) application on the root surfaces (group 1); βTCP/HA graft (Bone Ceramic®; Straumann, Basel, Switzerland) was used to fill the furcation defect (group 2); EMD (Emdogain®; Straumann, Basel, Switzerland) along with βTCP/HA (Bone Ceramic®; Straumann, Basel, Switzerland) was used following the protocol: EMD was applied on the root surfaces, then a few drops of EMD were mixed with βTCP/HA, and the combination of the two materials filled the entire defect (group 3). The surgical flaps were positioned slightly coronally and sutured using modified mattress sutures (5.0 polygalactin-A, Vicryl; Johnson & Johnson, São José dos Campos, Brazil) in order to completely cover the defects (Figs. 4, 5, and 6). No side effects were seen in any of the three groups.
Postoperative care
Patients were instructed to take analgesics (500 mg of dipyrone, four times a day) for 3 days and to discontinue tooth brushing around the surgical sites for 10 days after surgery. They were instructed to gently rinse with 0.12 % chlorhexidine, twice a day for a month. The sutures were removed at 10 days post-surgery, and the clinical parameters analyzed after 6 and 12 months. Patients were enrolled in a periodontal maintenance program during the study period. The maintenance visits occurred once a month at the first 6 months and every 3 months until the end of the study.
Primary and secondary outcome measures
The primary outcome measurement of the study was considered to be the mean horizontal clinical attachment level gain (difference between RHCAL at baseline and the values observed at 6 and 12 months). Secondary outcomes included (1) PD, (2) RVCAL, (3) RPGM, (4) complete furcation closure at 12 months, (5) plaque and BOP at surgical site, and (6) full-mouth plaque index (PI) and full-mouth gingival index (GI).
Power calculation
The sample size was calculated using the software package Biostat 5.0 with parameters set to detect a difference of 2 mm between treatments and α = 5 %. The 2-mm difference value was adopted in order to detect clinically significant changes on the studied variables, minimizing the chance of detecting differences that could be related to probing variations instead of actual gains in clinical attachment levels [20–26]. The estimated standard deviation was 1 mm and the size of the sample was determined to require at least 13 patients in each group [27].
Data management and statistical analysis
Homogeneity of treatment groups at baseline was assessed. Repeated-measures analysis of variance (ANOVA) was used to detect intra- and inter-group differences in the clinical parameters (RGMP, PD, RVCAL, RHCAL, and respective changes/gains). When a statistical difference was found, analysis of the difference was determined using the method of Tukey. The presence of BOP or plaque at furcation sites, as well as furcation re-classification at 6 months [18], was analyzed using Fisher’s exact test. The level of significance was set at 5 % (SAS Institute Inc., Cary, NC, USA, release 9.1, 2003).
Results
Subject accountability
Four hundred eighty patients were examined during the screening period. Fifty-three had an initial diagnosis of buccal class II furcation defects in at least one molar, being thus eligible for the study. After hygienic therapy, three patients were excluded (did not present PPD ≥4 mm and BOP at the site). Nine of 50 patients were excluded, eight during the surgical procedure (diagnosis of class II was not confirmed) and one because of pregnancy (Fig. 1).

Study flowchart. HA hydroxyapatite, β-TCP β-tricalcium phosphate, EMD enamel matrix derivative
Study schedule
Subject recruitment started in March 2009 and was completed by December 2012. The last surgical procedure was carried out in April 2013. Data entry/statistical analyses were performed by the end of 2014.
Patient characteristics at baseline
Patients’ characteristics at baseline were not significantly different among groups. Forty-one patients contributed with 41 furcation lesions. The mean PPD and RHCAL at furcation site were not statistically different among groups at baseline (Table 1).
Plaque and bleeding on probing
Acceptable oral hygiene was achieved at baseline and during the study since FMPS and FMBS remained below 15 % (Table 2). At baseline, all the treated furcations presented BOP while approximately half of the defects showed some detectable plaque. A decrease in the number of experimental sites with plaque/BOP was observed for the three groups during the study (Figs. 2 and 3). However, group 1 (EMD) showed less experimental sites with BOP after 12 months (2 out of 13) when compared with group 2 (βTCP/HA) (6 out of 14) and group 3 (EMD + βTCP/HA) (5 out of 14) (Figs. 4, 5, and 6).

Number of experimental furcation sites with detectable plaque during the study for each treatment group. No significant difference (Fisher’s exact test, p > 0.05)

Number of experimental furcation sites with bleeding on probing during the study for each treatment group. No significant difference (Fisher’s exact test, p > 0.05)

a Initial image—group 1 (EMD). b Application of EMD at furcation site. c Flaps repositioned and sutured. d 12-month clinical view of surgical site

a Initial image—group 2 (βTCP/HA). b Application of βTCP/HA at furcation site. c Flaps repositioned and sutured. d 12-month clinical view of surgical site

a Initial image—group 3 (EMD + βTCP/HA). b Application of EMD at furcation site. c Mixed EMD + βTCP/HA filling the entire defect. d Flaps repositioned and sutured. e 12-month clinical view of surgical site
Clinical parameters (RGMP, RVCAL, RHCAL, and PPD)
The results for the clinical parameters are shown in Table 3. The comparison between baseline and 12 months values for RGMP revealed that there was no significant increase in gingival recession in any of the groups (p > 0.05). On the other hand, a significant reduction for PPD (p < 0.05) was observed for the three treatments. After 12 months, the PPD reductions was 2.54 ± 0.78 mm for group 1 (EMD), 2.36 ± 1.01 for group 2 (βTCP/HA), and 2.43 ± 1.02 for group 3 (EMD + βTCP/HA), with no differences among the groups. Regarding RVCAL and RHCAL, all three treatments provided statistically significant gains after 6 and 12 months. The difference between baseline and the values observed after 12 months for RVCAL (mean vertical attachment level gain) was 2.08 ± 1.61 for group 1 (EMD), 2.29 ± 1.27 for group 2 (βTCP/HA), and 2.14 ± 1.29 for group 3 (EMD + βTCP/HA), with no significant differences among the groups. The mean reduction in the horizontal component of the furcation lesion, as calculated by the difference between the RHCAL values observed at baseline and after 12 months, amounted 2.77 ± 0.93 mm for group 1 (EMD), 2.64 ± 0.93 mm for group 2 (βTCP/HA), and 2.93 ± 0.83 mm for group 3 (EMD + βTCP/HA), with no significant differences among the groups.
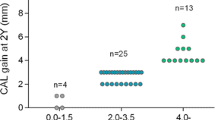
Furcation closure
Six months and 12 months after the surgeries, the furcation lesions were again evaluated according to Hamp et al.’s [18] classification (Table 4). Partial closure of the defects was observed in 33 cases, meaning that the furcations were now classified as class I, as follows: 13 furcations in group 1 (EMD), 9 furcations in group 2 (βTCP/HA group), and 11 furcations in group 3 (βTCP/HA + EMD), after 6 months of evaluation (p > 0.05). After 12 months, two furcations improved their diagnoses to class I, one in the βTCP/HA group and another in the βTCP/HA + EMD group. Complete furcation closure was not detectable during the study period.
Discussion
The progression of periodontal disease can reach the furcation area, leading to tissue destruction and creating a formidable challenge in the treatment of this chronic disease [19]. The presence of furcation defects makes the posterior teeth more vulnerable to loss than the anterior teeth [28, 29]. Therefore, new therapeutic approaches should be continuously investigated for these areas.
Enamel matrix derivative (EMD) has been used in periodontal regenerative procedures based on its fundamental role in cementum development. Histological studies have shown the potential of this material to induce periodontal regeneration [30–32]. Clinical studies showed horizontal clinical attachment level gain, PD reduction, and the possibility of complete furcation closure after EMD treatment [1, 11, 13, 33]. The synthetic bone substitute made of HA and βTCP may integrate into bone tissue, allowing osteoconductivity [34]. The combined use of different materials has been evaluated in order to find predictable approaches for periodontal regeneration in different clinical situations [35, 36]. Aiming to combine the osteoconductive and space-maintaining properties of a bone substitute with the biological properties of EMD, this study has been designed to evaluate the use of EMD + βTCP/HA. A decision was made to focus on the comparison of EMD + βTCP/HA to the isolated therapies (EMD + βTCP/HA versus βTCP/HA or EMD). Therefore, these three approaches were not compared to open flap debridement alone (OFD) or GTR in the present study. Besides the difficulties involved in finding the increased number of patients (following the inclusion/exclusion criteria) needed to conduct a study with several groups, this option was justified by the availability of historical controls, showing that both EMD [14, 37] and bone substitutes [38, 39] may provide superior clinical results to OFD and comparable results to those achieved with GTR [11, 12, 40–45].
Previous histologic studies (animal models) showed that root conditioning with EDTA may significantly enhance periodontal wound healing compared to other conditioning agents such as phosphoric acid or citric acid [46–48]. The migration of PDL fibroblasts toward the root surface may be enhanced compared to control (no root conditioning) or to other conditioning agents [47]. On the other hand, results from controlled clinical studies have failed to show statistically significant differences in the treatment outcome, when comparing open flap debridement with EDTA root conditioning to a control without EDTA [49–52]. Therefore, based on the available clinical information, EDTA root conditioning was not performed in the present study.
The three tested treatments produced favorable clinical changes characterized by a significant reduction of PPD and horizontal component of the furcation defects. Specifically concerning furcation defects, the horizontal parameter is directly related to the tooth prognosis [53]. Previous studies, using EMD alone in furcations, reported that it may result in PD reduction and RVCAL and RHCAL gains [30, 54–56]. A comparison of EMD + βTCP/HA to βTCP/HA alone was performed in patients with proximal furcation defects [57]. They reported a mean gain for RHCAL after 6 months of 1.47 mm for bone graft alone and 1.57 mm for the association of bone graft plus EMD, with no statistical differences between groups. This is in accordance with the results observed in the present study, showing no significant differences on mean RHCAL gain after treating the furcation with the isolated approaches when compared to the combined treatment. After 12 months, the mean RHCAL was 2.7 ± 0.9 for group 1 (EMD), 2.6 ± 0.9 for group 2 (βTCP/HA), and 2.9 ± 0.8 for the combined treatment (EMD + βTCP/HA). The RHCAL reduction amounted 54.5 % (EMD), 46.8 % (βTCP/HA), and 53.3 % (EMD + βTCP/HA) of the baseline value. The consequence of this reduction was that 85.3 % of all treated defects changed their diagnosis to class I after 1 year. However, no complete furcation closure could be observed during the study. This is in accordance with a previous study [13] evaluating the effects of EMD on the treatment of class II furcation defects where reduction of horizontal probing attachment level was observed after 36 months but with no complete closure of the defects. Other reports also evaluating EMD on the treatment of class II furcation showed only one site with complete closure [14]. Jepsen et al., showed complete closure of mandibular class II furcations in approximately 17 and 8 % of cases treated by EMD or GTR, respectively. Therefore, in spite of the evident reduction on the horizontal component of the furcation after treatment with current regenerative approaches, it seems also evident that the ideal outcome of complete furcation closure is not a frequent result.
In spite of the positive clinical outcomes observed when bone substitutes are used [14, 47], the results of the present study indicated that the association of βTCP/HA with EMD failed to provide a significant benefit. One point that should be considered is the difference in the histological healing pattern that may be present when comparing sites treated with EMD to sites treated exclusively with bone substitutes or the associated therapy (EMD + bone substitute). In a study conducted with the combination of EMD with biphasic calcium phosphate (BCP), in one or two wall intrabony defects around teeth schedule for extraction, it was observed that there is formation of cementum with inserting collagen fibers to a varying extent. Also, graft particles were still present and were mostly encapsulated in connective tissue, whereas formation of bone around the graft particles was observed only occasionally. Direct contact between the graft particles and the root surface (cementum or dentin) was not observed. This finding led to the conclusion that EMD may promote the formation of new cementum with an associated periodontal ligament, but there is the possibility that the presence of graft particles may interfere with the healing process, resulting in limited bone formation [58].
In conclusion, the association of the bone substitute to EMD did not provide a better clinical outcome when compared to the isolated therapies. Considering that the possibility of achieving periodontal regeneration might be increased with the use of EMD, according to previous histological studies [30–32], it seems reasonable to consider that this approach (isolated use of EMD) would be an adequate option for the treatment of class II furcation defects, similar to the ones treated in the present study. The interesting observation that bleeding at the furcation site was numerically lower in the EMD group (but not statistically significant) may suggest other properties of this material (microbiological effect?) [9], but this remains to be further evaluated. It must be recognized that there is a need for new developments in the regenerative treatments to improve the chance to promote complete closure of the defects and promote a greater positive impact on tooth prognosis.
Conclusion
EMD + βTCP/HA does not provide a significant advantage when compared to the isolated approaches. All three tested treatments promote significant improvements and partial closure of class II furcations. Based on its potential to induce periodontal regeneration, EMD may be considered an attractive option for this type of defect, but complete closure remains an unrealistic goal.
References
Cattabriga M, Pedrazzoli V, Wilson TG (2000) The conservative approach in the treatment of furcation lesions. Periodontol 2000 22:133–153
Pontoriero R, Lindhe J (1995) Guided tissue regeneration in the treatment of degree II furcations in maxillary molars. J Clin Periodontol 22(10):756–763
Becker W, Becker BE, Mellonig J, Caffesse RG, Warrer K, Caton JG et al (1996) A prospective multi-center study evaluating periodontal regeneration for class II furcation invasions and intrabony defects after treatment with a bioabsorbable barrier membrane: 1-year results. J Periodontol 67(7):641–649
Mellonig JT (1999) Enamel matrix derivative for periodontal reconstructive surgery: technique and clinical and histologic case report. Int J Periodontics Restorative Dent 19(1):8–19
Haase HR, Bartold PM (2001) Enamel matrix derivative induces matrix synthesis by cultured human periodontal fibroblast cells. J Periodontol 72(3):341–348
Sculean A, Windisch P, Gc C, Donos N, Brecx M, Treatment RE et al (2001) Treatment of intrabony defects with enamel matrix proteins and guided tissue regeneration. J Clin Periodontol 28(5):397–403
Galli C, Macaluso GM, Guizzardi S, Vescovini R, Passeri M, Passeri G (2006) Osteoprotegerin and receptor activator of nuclear factor-kappa B ligand modulation by enamel matrix derivative in human alveolar osteoblasts. J Periodontol 77(7):1223–1228
Walter C, Jawor P, Bernimoulin J (2006) Moderate effect of enamel matrix derivative (Emdogain W Gel) on Porphyromonas gingivalis growth in vitro. J Dent Res 171–176
Arweiler NB, Auschill TM, Donos N, Sculean A (2002) Antibacterial effect of an enamel matrix protein derivative on in vivo dental biofilm vitality. Clin Oral Investig 6(4):205–209
Keila S, Nemcovsky CE, Moses O, Artzi Z, Weinreb M (2004) In vitro effects of enamel matrix proteins on rat bone marrow cells and gingival fibroblasts. J Dent Res 83(2):134–138
Jepsen S, Heinz B, Jepsen K, Arjomand M, Hoffmann T, Richter S et al (2004) A randomized clinical trial comparing enamel matrix derivative and membrane treatment of buccal class II furcation involvement in mandibular molars. Part I: study design and results for primary outcomes. J Periodontol 75(8):1150–1160
Meyle J, Gonzales JR, Bödeker RH, Hoffmann T, Richter S, Heinz B et al (2004) Part II: secondary outcomes. 75(9)
Donos N, Glavind L, Karring T, Sculean A (2003) Clinical evaluation of an enamel matrix derivative in the treatment of mandibular degree II furcation involvement: a 36-month case series. Int J Periodontics Restorative Dent 23(5):507–512
Chitsazi MT, Mostofi Zadeh Farahani R, Pourabbas M, Bahaeddin N (2007) Efficacy of open flap debridement with and without enamel matrix derivatives in the treatment of mandibular degree II furcation involvement. Clin Oral Investig 11(4):385–389
Reynolds MA, Aichelmann-Reidy ME, Branch-Mays GL (2010) Regeneration of periodontal tissue: bone replacement grafts. Dent Clin N Am 54(1):55–71
Stahl SS, Froum SJ (1987) Histologic and clinical responses to porous hydroxylapatite implants in human periodontal defects. Three to twelve months postimplantation. J Periodontol 58(10):689–695
Hashimoto-Uoshima M, Ishikawa I, Kinoshita A, Weng HT, Oda S (1995) Clinical and histologic observation of replacement of biphasic calcium phosphate by bone tissue in monkeys. Int J Periodontics Restorative Dent 15(2):205–213
Hamp SE, Almfeldt I, Millinger PA (1975) Programmed continuing education in periodontics. Tandlakartidningen 67(22):1293–1298
Armitage GC (1999) Development of a classification system for periodontal diseases and conditions. Ann Periodontol 4(1):1–6
Listgarten MA, Mao R, Robinson PJ (1976) Periodontal probing and the relationship of the probe tip to periodontal tissues. J Periodontol 47(9):511–513
Armitage GC, Svanberg GK, Löe H (1977) Microscopic evaluation of clinical measurements of connective tissue attachment levels. J Clin Periodontol 4(3):173–190
Garnick JJ, Spray JR, Vernino DM, Klawitter JJ (1980) Demonstration of probes in human periodontal pockets. J Periodontol 51(10):563–570
Garnick JJ, Keagle JG, Searle JR, King GE, Thompson WO (1989) Gingival resistance to probing forces. II. The effect of inflammation and pressure on probe displacement in beagle dog gingivitis. J Periodontol 60(9):498–505
Magnusson I, Listgarten MA (1980) Histological evaluation of probing depth following periodontal treatment. J Clin Periodontol 7(1):26–31
Isidor F, Karring T, Attström R (1984) Reproducibility of pocket depth and attachment level measurements when using a flexible splint. J Clin Periodontol 11(10):662–668
Aguero A, Garnick JJ, Keagle J, Steflik DE, Thompson WO (1995) Histological location of a standardized periodontal probe in man. J Periodontol 66(3):184–190
Jeffcoat M (2002) What is clinical significance? J Clin Periodontol 29(Suppl 2):30–32
Harris RJ (2003) Case series untreated periodontal disease: a follow-up on 30 cases case series. J Periodontol 74(5):672–678
Papapanou PN (1989) Patterns of alveolar bone loss in the assessment of periodontal treatment priorities. Swed Dent J Suppl 66:1–45
Mardas N, Kraehenmann M, Dard M (2012) Regenerative wound healing in acute degree III mandibular defects in dogs. Quintessence Int 43(5):e48–e59
Araújo MG, Lindhe J (1998) GTR treatment of degree III furcation defects following application of enamel matrix proteins. An experimental study in dogs. J Clin Periodontol 25(6):524–530
Sallum EA, Pimentel SP, Saldanha JB, Nogueira-filho GR, Casati MZ, Jr FHN et al (2004) Enamel matrix derivative and guided tissue regeneration in the treatment of dehiscence-type defects: a histomorphometric study in dogs. Image (Rochester, NY) 1357–1363
Casarin RCV, Ribeiro EDP, Nociti FH, Sallum AW, Ambrosano GMB, Sallum EA et al (2010) Enamel matrix derivative proteins for the treatment of proximal class II furcation involvements: a prospective 24-month randomized clinical trial. J Clin Periodontol 37(12):1100–1109
Allograft FB, Gurinsky BS, Mills MP, Mellonig JT (2004) Clinical evaluation of demineralized derivative alone for the treatment of periodontal osseous defects in humans. Matrix 1309–1318
Itoh N, Kasai H, Ariyoshi W, Harada E, Yokota M, Mechanisms NT (2006) Mechanisms involved in the enhancement of osteoclast formation by enamel matrix derivative. J Periodontal Res
Schwartz Z, Carnes DL, Pulliam R, Lohmann CH, Sylvia VL, Liu Y et al (2000) Porcine fetal enamel matrix derivative stimulates proliferation but not differentiation of pre-osteoblastic 2T9 cells, inhibits proliferation and stimulates differentiation of osteoblast-like MG63 cells, and increases proliferation and differentiation of normal human osteoblast NHOst cells. J Periodontol 71(8):1287–1296
Koop R, Merheb J, Quirynen M (2012) Periodontal regeneration with enamel matrix derivative in reconstructive periodontal therapy: a systematic review. J Periodontol 83(6):707–720
Houser BE, Mellonig JT, Brunsvold MA, Cochran DL, Meffert RM, Alder ME (2001) Clinical evaluation of anorganic bovine bone xenograft with a bioabsorbable collagen barrier in the treatment of molar furcation defects. Int J Periodontics Restorative Dent 21(2):161–169
Tsao Y-P, Neiva R, Al-Shammari K, Oh T-J, Wang H-L (2006) Effects of a mineralized human cancellous bone allograft in regeneration of mandibular class II furcation defects. J Periodontol 77(3):416–425
Lekovic V, Kenney EB, Carranza FA, Danilovic V (1990) Treatment of class II furcation defects using porous hydroxylapatite in conjunction with a polytetrafluoroethylene membrane. J Periodontol 61(9):575–578
Carranza FA, Jolkovsky DL (1991) Current status of periodontal therapy for furcation involvements. Dent Clin N Am 35(3):555–570
Anderegg CR, Alexander DC, Freidman M (1999) A bioactive glass particulate in the treatment of molar furcation invasions. J Periodontol 70(4):384–387
Bowers GM, Schallhorn RG, McClain PK, Morrison GM, Morgan R, Reynolds MA (2003) Factors influencing the outcome of regenerative therapy in mandibular class II furcations: part I. J Periodontol 74(9):1255–1268
Trombelli L (2005) Which reconstructive procedures are effective for treating the periodontal intraosseous defect? Periodontol 2000 37:88–105
Reynolds MA, Aichelmann-Reidy ME, Branch-Mays GL, Gunsolley JC (2003) The efficacy of bone replacement grafts in the treatment of periodontal osseous defects. A systematic review. Ann Periodontol 8(1):227–265
Blomlöf J, Lindskog S (1995) Periodontal tissue-vitality after different etching modalities. J Clin Periodontol 22(6):464–468
Blomlöf J, Jansson L, Blomlöf L, Lindskog S (1995) Long-time etching at low pH jeopardizes periodontal healing. J Clin Periodontol 22(6):459–463
Blomlöf J, Jansson L, Blomlöf L, Lindskog S (1996) Root surface etching at neutral pH promotes periodontal healing. J Clin Periodontol 23(1):50–55
Mayfield L, Söderholm G, Norderyd O, Attström R (1998) Root conditioning using EDTA gel as an adjunct to surgical therapy for the treatment of intraosseous periodontal defects. J Clin Periodontol 25(9):707–714
Blomlöf L, Jonsson B, Blomlöf J, Lindskog S (2000) A clinical study of root surface conditioning with an EDTA gel. II. Surgical periodontal treatment. Int J Periodontics Restorative Dent 20(6):566–573
Sculean A, Berakdar M, Willershausen B, Arweiler NB (2006) Effect of EDTA root conditioning on the healing of intrabony defects treated with an enamel matrix protein derivative. Therapy 1167–1172
Bittencourt S, Ribeiro EDP, Sallum EA, Sallum AW, Nociti FH, Casati MZ (2007) Root surface biomodification with EDTA for the treatment of gingival recession with a semilunar coronally repositioned flap. J Periodontol 78(9):1695–1701
Harrel SK, Nunn ME (2001) Longitudinal comparison of the periodontal status of patients with moderate to severe periodontal disease receiving no treatment, non-surgical treatment, and surgical treatment utilizing individual sites for analysis. J Periodontol 72(11):1509–1519
Hak DJ (2007) The use of osteoconductive bone graft substitutes in orthopaedic trauma. J Am Acad Orthop Surg 15(9):525–536
AlGhamdi AS, Shibly O, Ciancio SG (2010) Osseous grafting part I: autografts and allografts for periodontal regeneration—a literature review. J Int Acad Periodontol 12(2):34–38
AlGhamdi AS, Shibly O, Ciancio SG (2010) Osseous grafting part II: xenografts and alloplasts for periodontal regeneration—a literature review. J Int Acad Periodontol 12(2):39–44
Peres MFS, Ribeiro EDP, Casarin RCV, Ruiz KGS, Junior FHN, Sallum EA et al (2013) Hydroxyapatite/β-tricalcium phosphate and enamel matrix derivative for treatment of proximal class II furcation defects: a randomized clinical trial. J Clin Periodontol 40(3):252–259
Pietruska M, Pietruski J, Nagy K, Brecx M, Arweiler NB, Sculean A (2012) Four-year results following treatment of intrabony periodontal defects with an enamel matrix derivative alone or combined with a biphasic calcium phosphate. Clin Oral Investig 16(4):1191–1197
Acknowledgments
The authors thank Dr. Joao Sangiorgio and Dr. Renato Casarin for the assistance with the statistical analysis and suggestions to the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Research involving human participants
All procedures performed in this study were in accordance with the ethical standards of the Ethical Committee of the Piracicaba Dental School—University of Campinas—UNICAMP and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Rights and permissions
About this article

Cite this article
Queiroz, L.A., Santamaria, M.P., Casati, M.Z. et al. Enamel matrix protein derivative and/or synthetic bone substitute for the treatment of mandibular class II buccal furcation defects. A 12-month randomized clinical trial. Clin Oral Invest 20, 1597–1606 (2016). https://doi.org/10.1007/s00784-015-1642-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-015-1642-x