
Abstract
Purpose
To investigate whether helical blade implant systems have advantages in terms of tip apex distance (TAD) and cut-out rate in comparison to conventional lag screws for intertrochanteric fractures in a geriatric population.
Methods
Relevant articles were sourced from the MEDLINE, Embase, Ovid and Cochrane Library databases from inception through March 2015. All randomized controlled trials (RCTs) comparing outcomes between helical blade and lag screw implant systems were selected. Mean TAD values and reported cut-out complications were noted. Each author independently assessed the relevance of the enrolled studies and the quality of the extracted data. Data were analyzed using R software.
Results
Ten studies including 1831 patients were eligible for this review, seven of which were included in a combined analysis of dichotomous outcomes and five in a combined analysis of continuous outcomes. The results revealed that, compared with lag screw implantations, the use of helical blades led to a lower rate of cut-out complications (95 % CI: 0.28–0.96, P = 0.036). Patients who experienced cut-out complications had a significantly greater tip apex distance (95 % CI: 0.68–1.34, P < 0.001). However, the actual tip apex distances were similar between the screw group and blade group (95 % CI: −0.44–0.79, P = 0.58).
Conclusions
No difference in TAD values was found between blades and screws. In addition, the cut-out risk in the blade-design group was lower than that of the screw group. Therefore, TAD is not an accurate predictor of cut-out risk.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cut-out of cephalic screws from the femoral head is the most common source of fixation failure following treatment of extracapsular proximal femoral fractures [1]. Baumgaertner et al. [2] showed that optimization of the tip apex distance (TAD) to less than 25 mm is critical for preventing intertrochanteric fixation failure. There are two types of cephalic screws available, lag screws and helical blades. The dynamic hip screw (DHS), an extramedullary implant that utilizes a lag screw, has been recognized as the standard for surgical and clinical outcomes in clinical trials. The proximal femoral nail anti-rotation (PFNA) system is an intramedullary nail implant designed by the Association for Osteosynthesis/Association for the Study of Internal Fixation (AO/ASIF). As implant designs have improved, such helical blade implants have gradually become more popular and have gained acceptance among surgeons. This new design sets a helical blade rather than a lag screw into the femoral head, which has been shown to significantly reduce the incidence of cut-out [3, 4]. However, randomized controlled trials (RCTs) comparing these two methods of internal fixation have demonstrated results that differ greatly from published experimental and theoretical findings [1, 5–14].
It has been reported that the risk of cut-out is closely associated with greater TAD [15]. It is not clear, however, whether the helical blade system is truly superior to traditional screw implants in terms of cut-out rates and TAD for the treatment of intertrochanteric fractures. From a thorough review of the literature, it became clear that no available publications had compiled relevant studies into a meta-analysis or systematic review to investigate this point. The present meta-analysis combines TAD values and cut-out complications for patients who underwent implantation with a helical blade or conventional lag screw. The results of this study will clarify differences between the blade and the screw in terms of cut-out rates and optimal TAD values.
Methods
Search strategies
Relevant articles were sourced from the PubMed, Embase, Ovid and Cochrane Library databases from inception through March 22, 2015, while conference publications, special orthopaedic and sports journals, and reference lists of related articles were included if deemed to be of value. Efforts were made to include all clinical RCTs that compared mean TAD for patients with helical blade versus screw systems, compared mean TAD for patients with and without cut-out failure, or compared the incidence of cut-out for patients with TAD < 25 mm vs. TAD > 25 mm. The databases were searched using the following terms: (“hip fracture” OR “intertrochanteric fracture” OR “intertrochanteric fracture” OR “trochanteric fracture”) AND (“proximal femoral nail anti-rotation” OR “PFNA” OR “TFN” OR “trochanteric fixation nail” OR “helical blade” OR “DHS blade” OR “dynamic hip screw” OR “DHS” OR “gamma nail”).
Assessment of study eligibility
All level I, II, and III evidence studies that met the inclusion criteria were included, and case series studies, letters, comments, case reports, retrospective studies, and guidelines were excluded. We compiled articles that met three eligibility criteria:
-
1.
The target population consisted of elderly patients with intertrochanteric fractures requiring surgical fixation.
-
2.
An objective of the study was to conduct a randomized control trial (RCT) to compare helical blade devices with screw devices.
-
3.
The length of follow-up was not restricted and the publication language was English.
Additional strategies used to identify studies included consultation with experts and a review of reference lists from articles that fulfilled our eligibility criteria.
Assessment of methodological quality
Two reviewers (Li and Niu) graded the methodological quality of each of the included studies using a set of questions from the Newcastle-Ottawa Scale (NOS) for prospective randomized controlled trial reporting of adequate data [16]. A quality score was calculated on the basis of three major components: selection of the groups of study (0–4 points), quality of the adjustment for confounding (0–2 points) and ascertainment of the exposure or outcome of interest in the case–control or cohorts, respectively (0–3 points). A maximum score of nine points represented the highest methodological quality. Prior to data extraction, we determined the NOS scoring system as follows: 0–3, low quality; 4–6, moderate quality; 7–9, high quality. Disagreements were resolved by discussion to achieve consensus. Otherwise, a senior reviewer (Chang) was also available to resolve disagreements.
Data extraction and analysis
Two researchers extracted information regarding the incidence of cut-out among elderly patients with helical blade fixation versus those with screw fixation (dichotomous data) using a pre-specified data extraction form. Mean TAD was also extracted for patients who experienced cut-out failure versus those who did not (continuous data). Data including demographics, methodology, intervention details and outcomes were also extracted from each study independently by the two researchers. No subgroup analysis of associations between implant types (intramedullary devices versus extramedullary devices) was performed. Study characteristics were analyzed using descriptive statistics, and the primary outcomes were combined using a random effects or fixed effect model.
Statistical analysis
All data analysis was performed with R software. We present results for dichotomous outcomes as relative risk (RR) with 95 % confidence intervals (CI) and continuous outcomes as weighted mean difference. Heterogeneity among studies was assessed using I-square (I 2) and chi-square (χ 2) tests. If there was no statistical heterogeneity (χ 2 test P ≥ 0.1 or I 2 ≤ 50 %), a fixed effect model was used; otherwise a random effects model was adopted.
Results
Study identification
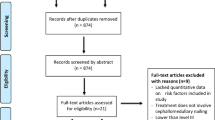
Our literature search identified 511 potentially relevant studies, among which 288 were considered for inclusion after title and abstract review. From these 288 studies, 278 were excluded after full text review. Therefore, a total of 10 RCTs were ultimately included in this review (Fig. 1). These 10 studies comprised 1831 patients, among whom there were 720 cases of implantation of a blade device, 648 cases of fixation with a screw device, and 348 cases where the specific device used could not be determined. We were able to combine results for studies as follows: six studies for the continuous outcome (mean TAD immediately after surgery for blade group versus screw group) [6, 9–11, 13, 14], nine studies for the dichotomous outcome (cut-out complication for blade group versus screw group) [5, 6, 9–14, 18] and three studies for the continuous outcome (mean TAD for cut-out versus no-cut-out groups) [1, 11, 14]. Baseline characterizations such as age and gender were all comparable between the two groups (Table 1).

Flow chart of study process for identification of studies and reasons for exclusion
Study characteristics
Details of the selected studies are shown in Table 1. These studies were conducted in China (4/10, 40 %), Spain (2/10, 20 %), Germany, the U.S., India and Switzerland. Nine of the included studies were case–control studies and one was a cohort study. We judged eight studies to be of high methodological quality and two to be of low quality (Table 2). A total of 1831 patients were included in this meta-analysis.
Outcome of TAD
We were able to extract enough data on tip apex distance (TAD) from six studies. Figure 2 shows the TAD measurements for the blade and screw groups, with a standard mean difference (SMD) of 0.17 (95 % CI −0.44–0.79; P = 0.58). Heterogeneity of the data was high (I 2 = 94 %), which may be related to different implants and TAD characteristics. A random effects model was used for this comparison.

Outcome of TAD for blade group vs. screw group
Outcome of cut-out complication
We were able to extract enough data on cut-out complications from nine studies. Figure 3 shows the incidence of cut-out for each study for both helical blade and lag screw fixation. On the basis of these data, the relative risk was 0.52 (95 % CI 0.28–0.96; P = 0.036). Heterogeneity of the data was fairly low (I 2 = 41.6 %), and a fixed effect model was used for this comparison.

Outcome of cut-out complication for blade group vs. screw group
Mean TAD for cut-out group versus no-cut-out group
We were able to determine data for the mean TAD for cut-out in three studies. Figure 4 shows the mean TAD for patients who had cut-out failure versus patients who did not. The standard mean difference was 1.01 (95 % CI 0.68–1.34; P < 0.001). Heterogeneity of the data was low (I 2 = 0 %).

Mean TAD for cut-out group vs. no-cut-out group
Discussion
Intertrochanteric fracture is one of the most common injuries among aged populations. Common treatment options include extramedullary nailing with a sliding hip screw (SHS) and intramedullary nailing with either the Gamma nail or proximal femoral nail anti-rotation (PFNA) device, both of which represent the most commonly used implants for intertrochanteric fractures. It is well known that the accuracy in positioning of the cephalic screw in the femoral head is a determinant of outcome following open reduction internal fixation, with cut-out of the implant from the femoral head the most common cause of mechanical failure, at rates of up to 12.6 % [19]. Baumgaertner et al. [2] introduced the tip apex distance (TAD) as a variable strongly correlated with cutout rate, and which was defined as the sum of the distance from the tip of the lag screw to the apex of the femoral head on the anteroposterior and lateral radiographic views. Optimization of the tip apex distance (TAD), i.e., less than 25 mm, is critical for preventing fixation failure of intertrochanteric fractures.
There are two types of cephalic screws available, lag screws and helical blades. Biomechanical tests have also demonstrated that helical blade implants have significantly higher cut-out resistance in osteoporotic bone compared to commonly used lag screw devices. However, cut-out of helical blade implants still occurs [20, 21]. From the sourced literature and related research used in the study, we found no evidence in the form of meta-analyses or systematic reviews based on published RCTs to support a connection between TAD and cut-out rates.
To the authors’ knowledge, this is the first quantitative meta-analysis of randomized controlled trials that compares cephalic helical blades to cephalic screws in terms of TAD as a predictor of implant cut-out in the treatment of intertrochanteric fractures. This meta-analysis includes ten randomized controlled trials with a total of 1831 participants. Most of these studies (8/10) were of high quality, based on NOS values, and had almost identical inclusion and exclusion criteria. No evidence of publication bias was found from the plotted funnel diagrams and Begg’s rank difference tests among the studies included in this meta-analysis.
A major strength of this meta-analysis was the rigorous inclusion of RCTs used to eliminate the possibility of selection bias and to maintain a consistent baseline in both groups. In addition, sensitivity analyses showed that many values calculated between the two groups were reliable and stable.
Rubio-Avila et al. [17] reported that patients with TAD > 25 mm had a significantly greater risk of cut-out than patients with TAD < 25 mm (RR = 12.71); patients who experienced cut-out had significantly higher TAD scores than those who did not (mean difference = 6.54 mm). A similar outcome was calculated by the meta-analysis in this study. On the basis of three studies [1, 11, 14], the standard mean difference (SMD) in TAD between groups with and without cut-out was 1.01 (95 % CI 0.68–1.34), which was statistically significant (P < 0.001) (Fig. 4). We also searched for patients with a mean TAD > 25 mm with blade and screw fixation, but could only source one study, by Stern et al. [11], on this subject. Stern claimed that there was no significant difference between blade and screw in the percentage of patients with a TAD > 25 mm (RR = 1.3, 95 % CI 0.8–2.1).
In the present study, we found that the difference in mean TAD between the blade and screw groups was not statistically significant (P = 0.58). A similar result was reported by Huang et al. [22]. However, the difference between groups in the percentage of patients suffering cut-out complications was statistically significant (P = 0.036) in our test, while Huang et al. reported a contrary outcome, showing no statistically significant difference between the blade and screw groups (P = 0.41). Our outcomes showed that the cut-out risk with blade implants was not the same as with conventional lag screws. This difference in results may be attributable to the fact that two additional RCTs were included in this study. Moreover, some papers in the literature question the concept of TAD as a reliable predictor of cut-out. Mingo-Robinet et al. [23] found no statistically significant association between sex, distraction at the fracture site, TAD or cervical angle and the risk of implant cut-out. Goffin et al. [24, 25] have suggested more than once that TAD should be adjusted depending on the size of the femoral head and that a TAD > 25 mm cannot be considered an accurate predictor of lag screw cut-out.
This meta-analysis has some potential limitations. Firstly, although little evidence of publication bias was observed, the power of the tests used was obviously limited due to the relatively small number of RCTs included. The total of ten studies involving 1831 patients was not large enough to undertake a comprehensive subgroup analysis to strengthen the validity. Secondly, different implants and evaluation systems were used in the studies analyzed, introducing the risk of selection bias in this meta-analysis. Substantial heterogeneity in terms of the cut-out rate was observed in comparing the PFNA with the DHS or Gamma nail. Finally, the follow-up durations could be considered short-term, as they were limited to 1 year, and a large number of patients withdrew before the last follow-up point. This is a common problem in studies on elderly clinical patients. However, the dropout rates were comparable between the blade and screw groups.
In conclusion, this meta-analysis, which included the most recent relevant RCTs, clarified the consequences of TAD and showed that many patients may suffer from cut-out, depending on the device implanted, whether helical blade or lag screw. No statistically significant difference was found between TAD values for blades and screws. The cut-out risk with blade designs was lower than that for the screw group in the surgical treatment of intertrochanteric fractures in an elderly population. In conclusion, TAD is not an optimum indicator for predicting the risk of cut-out.
References
Lobo-Escolar A, Joven E, Iglesias D, Herrera A. Predictive factors for cutting-out in femoral intramedullary nailing. Injury. 2010;41(12):1312–6.
Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77(7):1058–64.
Windolf M, Braunstein V, Dutoit C, Schwieger K. Is a helical shaped implant a superior alternative to the Dynamic Hip Screw for unstable femoral neck fractures? A biomechanical investigation. Clin Biomech. 2009;24(1):59–64.
Lenich A, Bachmeier S, Prantl L, Nerlich M, Hammer J, Mayr E, Al-Munajjed AA, Füchtmeier B. Is the rotation of the femoral head a potential initiation for cutting out? A theoretical and experimental approach. BMC Musculoskelet Disord. 2011;22(12):79.
Zou J, Xu Y, Yang H. A comparison of proximal femoral nail antirotation and dynamic hip screw devices in trochanteric fractures. J Int Med Res. 2009;37(4):1057–64.
Lenich A, Vester H, Nerlich M, Mayr E, Stockle U, Füchtmeier B. Clinical comparison of the second and third generation of intramedullary devices for trochanteric fractures of the hip-Blade vs screw. Injury. 2010;41(12):1292–6.
Xu YZ, Geng DC, Yang HL, Zhu GM, Wang XB. Comparative study of trochanteric fracture treated with the proximal femoral nail anti-rotation and the third generation of gamma nail. Injury. 2010;41(12):1234–8.
Liu Y, Tao R, Liu F, Wang YH, Zhou ZY, Cao Y, Wang H. Mid-term outcomes after intramedullary fixation of intertrochanteric femoral fractures using the new proximal femoral nail antirotation (PFNA). Injury. 2010;41(8):810–7.
Garg B, Marimuthu K, Kumar V, Malhotra R, Kotwal PP. Outcome of short proximal femoral nail antirotation and dynamic hip screw for fixation of unstable trochanteric fractures. A randomised prospective comparative trial. Hip Int. 2011;21(5):531–6.
Fitzpatrick DC, Sheerin DV, Wolf BR, Wuest TK. A randomized, prospective study comparing intertrochanteric hip fracture fixation with the dynamic hip screw and the dynamic helical hip system in a community practice. Iowa Orthop J. 2011;31:166–72.
Stern R, Lübbeke A, Suva D, Miozzari H, Hoffmeyer P. Prospective randomised study comparing screw versus helical blade in the treatment of low-energy trochanteric fractures. Int Orthop. 2011;35(12):1855–61.
Vaquero J, Munoz J, Prat S, Ramirez C, Aguado HJ, Moreno E, Perez MD. Proximal Femoral Nail Antirotation versus Gamma3 nail for intramedullary nailing of unstable trochanteric fractures. A randomised comparative study. Injury. 2012;43(S2):S47–54.
Zhang S, Zhang K, Jia YF, Yu B, Feng W. InterTan nail versus Proximal Femoral Nail Antirotation-Asia in the treatment of unstable trochanteric fractures. Orthopedics. 2013;36(3):e288–94.
Yang YH, Wang YR, Jiang SD, Jiang LS. Proximal femoral nail antirotation and third-generation Gamma nail: which is a better device for the treatment of intertrochanteric fractures? Singapore Med J. 2013;54(8):446–50.
De Bruijn K, den Hartog D, Tuinebreijer W, Roukema G. Reliability of predictors for screw cutout in intertrochanteric hip fractures. J Bone Joint Surg Am. 2012;94(14):1266–72.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (homepage on the internet). Ottawa Health Research Institute: Ottawa, c1996–2006 [updated 09 June 2007; cited 06 September 2007]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm.
Rubio-Avila J, Madden K, Simunovic N, Bhandari M. Tip to apex distance in femoral intertrochanteric fractures: a systematic review. J Orthop Sci. 2013;18(4):592–8.
Xu YZ, Geng, Mao HQ, Zhu XS, Yang HL. A comparison of the proximal femoral nail antirotation device and dynamic hip screw in the treatment of unstable pertrochanteric fracture. J Int Med Res. 2010;38(4):1266–75.
Nishiura T, Nozawa M, Morio H. The new technique of precise insertion of lag screw in an operative treatment of trochanteric femoral fractures with a short intramedullary nail. Injury. 2009;40(10):1077–83.
Nikoloski AN, Osbrough AL, Yates PJ. Should the tip apex distance (TAD) rule be modified for the proximal nail antirotation (PFNA)? A retrospective study. J Orthop Surg Res. 2013;17(8):35.
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2010;(9):CD000093. doi:10.1002/14651858.CD000093.pub5.
Huang X, Leung F, Liu M, Chen L, Xu Z, Xiang Z. Is helical blade superior to screw design in terms of cut-out rate for elderly trochanteric fractures? A meta-analysis of randomized controlled trials. Eur J Orthop Surg Traumatol. 2014;24(8):1461–8.
Mingo-Robinet J, Torres-Torres M, Martinez-Cervell C, Alonso JA, García-González S. Comparative study of the second and third generation of Gamma nail for trochanteric fractures: review of 218 cases. J Orthop Trauma. 2015;29(3):e85–90.
Goffin JM, Jenkins PJ, Ramaesh R, Pankaj P, Simpson AH. What is the relevance of the tip-apex distance as a predictor of lag screw cut-out? PLoS One. 2013;8(8):e71195.
Goffin JM, Pankaj P, Simpson AH. The importance of lag screw position for the stabilization of trochanteric fractures with a sliding hip screw: a subject-specific finite element study. J Orthop Res. 2013;31(4):596–600.
Acknowledgments
The authors would like to acknowledge Tienan Feng, Ming Ni and Lily Chen for their help in the methodology. We also thank Dr. Colin McClean for proofreading.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding information
The study was supported by Shanghai Municipal Science Committee (No. 14411971900), and the Young Doctor’s promotion project of the Bai-yi-deng-gao Foundation from the Yangpu District Health and Family Planning Commission (No. 20140063), Dr. Shuang Li.
About this article

Cite this article
Li, S., Chang, SM., Niu, WX. et al. Comparison of tip apex distance and cut-out complications between helical blades and lag screws in intertrochanteric fractures among the elderly: a meta-analysis. J Orthop Sci 20, 1062–1069 (2015). https://doi.org/10.1007/s00776-015-0770-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-015-0770-0