
Abstract
Trace elements within the brain are important for proper neurological function, but their imbalance has been rarely investigated in glioblastoma. This study enrolled a total of 14 patients with glioblastoma, and the tumor and peritumoral brain tissues were collected while undergoing surgery. The concentrations of Mg, Ca, Cr, Mn, Fe, Co, Cu, Zn, Se, As, Cd, Tl and Pb were determined using a well-evaluated ICP-MS method. The Cu- and Cd-binding proteomes were further analyzed using the anatomic transcriptional atlas from Ivy GAP. Histological evaluation was based on rubeanic acid staining and immunohistochemistry, respectively. The 13 trace element concentrations were obtained, and the highest were Ca, Mn, Fe, Zn and Cu, ranging from a few to dozens of ug/g. Correlation analysis suggested the existence of two intra-correlated clusters: essential metals (Cu–Ca–Zn–Mg) and heavy metals (Pb–As–Cd–Tl–Co–Cr–Mn). Compared to the tumor samples, significantly higher levels of Cu and Cd were observed in the peritumoral region. Further analysis of the Cu- and Cd-binding proteins from the anatomic view suggested that DBH and NOS1 were obviously increased in the leading edge than the central tumor region. Consistent with the above findings, histological evaluation of Cu and DBH further confirmed more copper and DBH expressions in the peritumoral area compared to the tumor core. Trace elements differ in tumor and peritumoral brain zone in glioblastoma, which may associate with tumor angiogenesis.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glioblastoma (GBM) is the most common and most lethal malignant brain tumor, with median survival under 2 years, despite surgical resection, radiation, and chemotherapy [1]. In most cases, the cause of death is tumor recurrence, occurring at the margin of surgical resection in the macroscopically normal peritumoral brain zone [2]. Tumor cells that escape complete surgical excision are the ultimate cancer cell seeds that infiltrate the brain [3]. Tumors acquire new mutations and evolve rapidly, leading to increased heterogeneity within the tumor and the development of drug resistance [4]. Besides genetic modifications, tumor cells are characterized by substantial changes in their metabolism affecting the need for macronutrients but also for micronutrients [5].
Trace elements must be in balance within certain limits in brain tissues to carry out the required functions of the central nervous system [6]. Essential elements such as calcium (Ca), magnesium (Mg), manganese (Mn), iron (Fe), cobalt (Co), copper (Cu), zinc (Zn), and selenium (Se) are required for the proper functioning and growth of the brain as they provide protection against diseases and reactive oxygen species [7]. On the flip side, excess essential elements or accumulation of toxic metals such as chromium (Cr), arsenic (As), cadmium (Cd), thallium (Tl), and lead (Pb) may induce cellular damage, resulting in a variety of abnormities [7, 8]. The balance of trace elements within the brain is regulated in a complex manner by the brain barrier system [7]. However, studies on the concentrations and anatomic variations of trace elements in brain tumors, especially GBM, are still lacking.
Therefore, in this study, we aim to determine and compare the concentrations of 13 essential and toxic trace elements including Mg, Ca, Cr, Mn, Fe, Co, Cu, Zn, Se, As, Cd, Tl, and Pb in tumor and the peritumoral brain tissues in human GBM, using a well-evaluated ICP-MS method, which would be helpful for further thorough analyses, including elucidating the pathological mechanism, or developing new therapeutic interventions or drugs.
Materials and methods
Patients and tissue samples
Approval was obtained from the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology in Wuhan, China. All the procedures involving human samples conformed to the principles outlined in the Declaration of Helsinki. Participation was voluntary and informed consent was obtained in all cases.
A total of 14 patients with glioblastoma multiforme (GBM) were included in the study. Tumor and peritumoral brain tissue samples were collected from all the cases undergoing surgery at the Department of Neurosurgery of Tongji Hospital. At the time of surgery, no patient had started chemotherapy or radiation therapy. For all the patients, GBM was diagnosed by CT/MRI, followed by histopathology for confirmation. All the GBM were isocitrate dehydrogenase 1 (IDH1) wild type (IDH1 mutation confer a favorable prognosis). The primary sites were temporal lobe (8 cases), frontal lobe (5 cases), or parietal lobe (1 case). All samples were de-identified. The detailed characteristics of all the patients are outlined in Table 1.
The tumor tissue samples were collected during tumor removal surgeries. They were sharply resected using micro-scissors from the core of the tumor to be highly representative during the histology of the lesion. The peritumoral brain tissue was resected in very small amounts from the brain area that surrounded the tumor and only from non-eloquent cerebral areas. These samples were stored in recipients with heparinized saline solution 0.9% NaCl. After gently absorbing excess solution with filter paper, samples were then flash frozen and stored in −80 °C until use.
Test set and validation set
For ICP-MS analysis, the 14 cases were randomly divided into two sets: the test set (N = 5) and the validation set 1 (N = 9). Sample preparation and ICP-MS analysis on the test set and validation set 1 were performed, respectively, on different days. In addition, the total 14 cases were also used as a whole as a new validation set 2, for an additional validation (Table 2).
Sample preparation and ICP-MS analysis
For sample preparation, a microwave-assisted acid digestion procedure was conducted using an Ethos T microwave digestion device (Milestone, Italy). A sample of 100 mg tissue was weighed and mixed with 4.0 mL of HNO3 (65–68%, w/w) and 2.0 mL of H2O2 (30%, w/w) in a Teflon pressure vessel. Then, the vessel was closed and placed into a microwave digestion device. The sample was digested at 180 °C (ramp, 10 min; hold, 15 min) with a power of 1.0 kW. After cooling, the sample solution was transferred into a Teflon beaker and heated mildly to near 2.0 mL at a relatively low temperature (about 60 °C). Finally, the resulting solution was diluted to 10.0 mL with Milli-Q water and then subjected to sample analysis.
All measurements were carried out in the Department of Laboratory Medicine of Tongji Hospital (Wuhan, China) with a quadrupole inductively coupled plasma mass spectrometer (ICP-MS) equipped with a concentric glass nebulizer and a cyclonic spray chamber ((7700× ICP-MS system, Agilent Technologies, CA, USA). Analyses were performed in standard/no-gas mode and dynamic reaction cell mode, as described in our previous reports [9,10,11]. Briefly, for Mg, Ca, Cr, Mn, Fe, Co, Cu, Zn, Se and As, the assays were run in dynamic reaction cell mode with high-purity helium (He, > 99.995%) as the reaction cell gas. For Cd, Tl and Pb, assays were run in standard/no-gas mode. Calibrating solutions were prepared every day using the Multi-element Calibration Standard (Agilent Technologies, CA, USA) and standard solutions of Cu, Zn, Ca, Fe, and Mg (O2si, USA). All the detailed ICP-MS operating conditions and calibration preparations are summarized in Table S1.
Quality assurance
Firstly, the limit of detection (LoD) and limit of quantitation (LoQ) of the method were evaluated. According to the recommendations of IUPAC and previous study [9], the LoD was determined as triple RSD (relative standard deviation) of the sample blank measurements (RSDb) (N > 10), while the LoQ were determined from LoQ = 10 RSDb C/SBR, where C is the concentration of the element in solution and SBR is the signal-to-background ratio. The LoD and LoQ are listed in Table S2. The LoD ranged from 0.02 ug/L (Cd, Tl) to 1.5 mg/L (Fe), and LoQ ranged from 0.05 ug/L (Tl) to 4.3 mg/L (Fe).
For quality assurance, two control materials: Seronorm controls (Ref:210205-10305, SERO, Billingstad, Norway) and ClinChek controls (ref.:8847-8849, RECIPE, Germany) were used, each of which had two levels (low and high level). The Seronorm controls, which were traceable to SRM from NIST (https://www.nist.gov/srm) (Table S3), were acid digested, diluted, and analyzed in the same way as the tissue samples. The ClinChek controls were only diluted and analyzed in the same way as the processed tissue samples (Table S2). When compared with target value and acceptable range, the measured values of both the Seronorm controls and ClinChek controls were mostly acceptable (Tables S2, S3), and the precision of all the elements for the ClinChek controls was less than 8.0% (Table S2).
In addition, except for the traceable control materials, to further evaluate the accuracy of the method, the recovery of standard additions was also determined. Two levels of trace element standards were added in the patient samples, and their elemental concentrations before and after addition were determined, respectively. The recovery was evaluated and both found to be in the range of 80–120%, indicating that the accuracy of the method seemed to be acceptable (Table S4).
Data analysis
According to previous studies of biological trace elements [7, 12], the ICP-MS-measured values were represented as mean ± standard deviation (SD), and Student’s two-tailed t test was used to compare the means of two groups. p < 0.05 is considered to be statistically significant. The normality of all the ICP-MS measurements was tested by Shapiro–Wilk test, and most of the trace elemental statistics showed normal distribution (data not shown). The Pearson correlation analysis and the coefficient (r) were used to assess the correlation between the different elements in the tumor samples. For statistical analysis, individual measurement below LoQ were replaced by the value of LoQ/2. All analyses were performed using SPSS (version 22.0, Chicago, USA).
Anatomic transcriptional analysis of copper-/cadmium-binding proteins
To assess the levels of the copper/cadmium in GBM and peritumoral tissues, we further performed an RNA-seq analysis of the copper-/cadmium-containing proteins using the anatomic transcriptional atlas of human glioblastoma from the Ivy Glioblastoma Atlas Project (Ivy GAP) (http://glioblastoma.alleninstitute.org/) [4]. This atlas summarized the transcriptomes in the seven anatomic features in glioblastoma, including leading edge (LE), infiltrating tumor (IT), cellular tumor (CT), pseudopalisading cells around necrosis (PAN), perinecrotic zone (PNZ), microvascular proliferation (MVP), and hyperplastic blood vessels (HBV). The LE is the outermost boundary of the tumor (peritumoral zone), where the ratio of tumor to normal cells is about 1–3/100, where the layers of the cortex are often observed.
The copper- and cadmium-binding protein lists were retrieved, respectively, from gene sets downloaded from the Molecular Signatures Database (MSigDB) (https://www.gsea-msigdb.org/gsea/msigdb). A total of 43 copper-binding proteins and 10 cadmium-binding proteins were extracted, respectively, from the copper- and cadmium-binding gene sets after removing overlapping genes (Table S5) and subjected to anatomic transcriptional analysis using normalized gene-level FPKM values from the Ivy GAP.
Copper staining and immunohistochemistry
Histological evaluation was based on the 24-h formalin-fixed tissue samples. For copper staining, sections of 3 um were subjected to routine rubeanic acid stains for copper accumulation. Immunohistochemical staining for dopamine beta-hydroxylase (DBH) was performed using the monoclonal antibody anti-DBH (EPR20385, Abcam, UK).
Results
A total of 14 patients were included in the present study. The age ranged from 38 to 70 years (mean: 55.5 years), and eight were men. All cases were IDH1 wide type (Table 1). For trace elemental analysis, to get more reliable results, the 14 cases were randomly divided into two sets: the test set (N = 5) and the validation set 1 (N = 9), and analyzed on different days, respectively. Another validation set 2, consisting of all the 14 cases, was also used for an additional validation. The concentrations of the analyzed 13 trace elements in tumor and peritumoral brain tissues of the 14 GBM patient are summarized in Table 2. Among all the trace elements, the highest concentrations in tumor were Ca (94.64 ± 44.07 ug/g), Mg (81.29 ± 28.4 ug/g), and Fe (71.9 ± 54.04 ug/g), followed by Zn (10.06 ± 3.54 ug/g) and Cu (1.55 ± 0.75 ug/g). The other essential elements such as Se (0.91 ± 0.8 ug/g), Mn (0.55 ± 0.33 ug/g), and Cr (0.14 ± 0.07 ug/g) were much lower (<1 ug/g). Toxic elements such as As, Cd, Co, Tl, and Pb are mostly at the nanogram per gram level.
Between the tumor and peritumoral brain tissues, most of the trace elements showed equivalent concentrations in the test set, while Cu and Cd were found to be lower in the tumor than in the peritumoral samples (p < 0.05). In the validation set 1, we still observed the same differences. For all the 14 cases as a whole (i.e., the validation set 2), the changes still remained the same, that is, the Cu and Cd levels in the tumor were significantly lower than those in the peritumoral samples (Cu: 1.55 ± 0.75 µg/g vs 2.93 ± 0.85 µg/g, Cd: 7.6 ± 5.72 vs 16.32 ± 11.38 ng/g) (Table 2; Fig. 1). In addition, validation set 2 showed higher levels of Se in tumors than in the peritumoral samples (0.91 ± 0.8 vs 0.51 ± 0.46 µg/g), while no such change was observed in the test set and validation set 1.

Concentrations of 13 essential and toxic trace elements in tumor and peritumoral brain tissues in glioblastoma. Student’s two-tailed t-test (p value) was used to compare the means of two groups. Results are shown as mean ± standard error. *p < 0.05. Abbreviations: Mg, magnesium; Ca, calcium; Cr, chromium; Mn, manganese; Fe, iron; Co, cobalt; Cu, copper; Zn, zinc; Se, selenium; As, arsenic; Cd, cadmium; Tl, thallium; Pb, lead
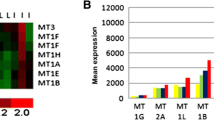
Considering that copper and cadmium in the brain may act or accumulate as binding forms in proteins or protein complexes, we further analyzed the expressions of copper- and cadmium-binding proteins in the tumor and peritumoral brain tissues of GBM patients. Using the anatomic transcriptional atlas from the Ivy GAP, we quantified the expressions of the 43 copper-binding proteins and 9 cadmium-binding proteins in the anatomic regions in GBM, and the fold changes of the six anatomic regions (leading edge (LE), infiltrating tumor (IT), pseudopalisading cells around necrosis (PAN), perinecrotic zone (PNZ), microvascular proliferation (MVP), and hyperplastic blood vessels (HBV)) when compared to the cellular tumor zone (CT), were obtained: LE vs CT, IT vs CT, PAN vs CT, PNZ vs CT, MVP vs CT, and HBV vs CT (Table S1; Fig. 2A, B). As shown in Fig. 2A, B, firstly, the hierarchical clustering of different anatomic comparisons showed LE and IT, MVP and HBV, and PAN and PNZ clustered, respectively, suggesting that these pairs of regions showed more similar patterns for copper- and cadmium-binding protein expressions.

Color map of transcriptional fold changes of copper- and cadmium-binding proteins in six anatomic structures compared to the tumor core. Transcriptional levels of copper- (A) and cadmium- (B) binding proteins in the leading edge (LE), infiltrating tumor (IT), pseudopalisading cells around necrosis (PAN), perinecrotic zone (PNZ), microvascular proliferation (MVP), and hyperplastic blood vessels (HBV) were compared to cellular tumor (CT). The expressions of copper-binding protein DBH (C) and cadmium-binding protein NOS1 (D) in the seven anatomic features are further shown as a box plot. *p < 0.05
LE and IT, especially LE, mainly represent the peritumoral brain regions, in which the tumor cells were lower in rate. For copper-binding proteins, when compared to the CT regions, it could be obviously found that several proteins were significantly increased, including DBH, MT1G, MT1E, MT1F, MT1M, SCO2, SOD1, and COX17 (Fig. 2A). Among them, the dopamine beta-hydroxylase DBH showed the highest fold increase (Log2FC > 3.5) in LE and IT than other regions (Fig. 2A, C). These results may partly explain the higher copper levels in peritumoral brain tissues than the tumor core observed in our ICP-MS analysis. For cadmium-binding proteins, SLC30A1 and NOS1 were found to be increased in LE and/or IT than in the CT regions (Fig. 2B). NOS1 was found to be only significantly increased in LE (Fig. 2B, D), and this may be associated with higher cadmium levels in peritumoral brain tissues observed in our ICP-MS analysis.
To further analyze and validate the copper variations in GBM, firstly, histological copper levels were assessed by copper staining (Fig. 3A), and more copper accumulation was observed in the peritumoral area than the tumor core (Fig. 3B). Furthermore, immunohistochemistry was also performed to evaluate the anatomic expressions of the copper-binding protein DBH (Fig. 3C), and it was shown that DBH was significantly increased in the peritumoral area compared to the tumor core (Fig. 3D). The Cu regions in the staining tended to be colocalized with DBH in immunostaining.

Copper staining and DBH expression in the tumor core and peritumoral area of the glioblastoma. A Copper stains a granular green by the rubeanic acid method (arrow) and is much more prominent in the peritumoral area than the tumor core of glioblastoma. B Quantitative integrated optical density (IOD) analysis of the copper staining. C Expressions of DBH in the peritumoral area and the tumor core of the glioblastoma were analyzed by immunohistochemistry. D Quantitative immunohistochemical staining analysis of DBH expressions (arrow). Scale bar: 20 um, *p < 0.05
For the analyzed 13 essential and toxic trace elements, considering that interactions or co-binding forms may exist, we further analyzed their correlations in the GBM tumor samples (Fig. 4). The highest correlations were mainly between the heavy metals, including Pb–As, Pb–Cd, Pb–Tl, Pb–Co, Pb–Cr, Pb–Mn, Tl–Cr, Tl–Mn, Tl–Co, Tl–As, Tl–Cd, Cd–Co, Cd–As, As–Cr, As–Co, As–Mn, Co–Mn, Co–Cr, and Cr–Mn, with the Pearson correlation coefficient (r) all > 0.6. Meanwhile, the essential metals also showed positive correlations, including Cu–Ca (r = 0.60), Cu–Zn (r = 0.64), Zn–Mg (r = 0.55), and Zn–Ca (r = 0.59) (all p < 0.05) (Fig. 4). However, between those heavy metals and essential metals, significant correlation was not observed, except that some negative correlations seemed to exist as in Cu–Cd (r = − 0.51, p = 0.09) and Pb–Se (r = − 0.50, p = 0.08). These results suggested that essential metals and heavy metals showed distinct patterns in the tumors.

Correlation matrix between the 13 trace elements in tumor samples. Pearson correlation coefficients (r, above) and p values (below, italic) for the correlation between each two of the 13 elements. Color represents correlation coefficients. Abbreviations: Mg, magnesium; Ca, calcium; Cr, chromium; Mn, manganese; Fe, iron; Co, cobalt; Cu, copper; Zn, zinc; Se, selenium; As, arsenic; Cd, cadmium; Tl, thallium; Pb, lead
Discussion
Trace elements have been implicated in cancer, since the levels differ between cancerous and noncancerous tissue, different cancer types, and different malignancy grades [8]. However, few studies have been conducted on trace element concentrations in brain tumors. Thus, in this study, we determined the concentrations of 13 toxic and essential trace elements in tumor and its adjacent tissue, respectively, from patients with GBM, using a well-established ICP-MS method. The concentrations were reported, and the highest concentrations of Ca, Mg, Fe, Zn and Cu ranged from a few to dozens of ug/g in tumor and in the adjacent tissues, which were equivalent toth previous report of human brain tissue [13]. The other essential elements such as Mn, Se, and Cr and heavy metals such as As, Cd, Co, Tl, and Pb were much lower (<1 ug/g) in concentrations, which seemed to be slightly lower when compared to previous reports [7], and it could be due to the differences in the detection method. In fact, for human brain tissues, trace element concentrations often showed wide variations from different reports because of the differences in sample weight (wet or dry weight), sample processing procedures and, more generally, detection methods (NAA, FAAS, ICP-MS, etc.) [12]. In this study, we established a method with good performance based on ICP-MS, and obtained the trace element concentrations in the tumor and peritumoral tissues, respectively, which provides a new comparable dataset for this field.
Trace elements always showed some correlations in blood [9, 14] and urine [15, 16]. In our study, the correlation network of trace elements in GBM tumor seems to form two intra-correlated clusters: the essential metals (Cu–Ca–Zn–Mg) and heavy metals (Pb–As–Cd–Tl–Co–Cr–Mn), respectively, suggesting their distinct mechanisms in brain tumors. This was much similar to those observed in human blood [14]. Essential metals always serve as enzymatic cofactors and are key components of intra- and inter-neuronal signaling, while heavy metals may interfere with specific proteins, either by forming a complex with functional side chain groups or by displacing essential metal ions in metalloproteins [17].
In glioblastoma, peritumoral brain zone or peritumor area is a region that cannot be ignored. In fact, 90% of recurrences of glioblastoma occur in the normal peritumoral brain zone, which possesses specific properties, has been less studied than the tumor core [2]. In our findings, of all the analyzed essential and toxic trace elements, most appeared to be equivalent between the tumor and peritumoral tissues, except for Cu and Cd, which were found to be lower in GBM tumor samples than the peritumoral samples. This difference was well consistent with the previous reports for Cu [8, 18, 19]. Cu is a determining factor in malignant transformation, making it possible for its levels to be higher in the normal brain tissues adjacent to the tumor. Accordingly, more copper accumulation could be observed in the peritumoral area by copper staining, as tumor growth and recurrences mainly occur in the peritumoral brain tumor zone and copper alterations are in accordance with tumor-specific alterations in the microenvironment [18]. Furthermore, Cu is the main building block in more than 30 enzymes and has a role in angiogenesis. DBH is a copper-containing, essential neurotransmitter-synthesizing enzyme that catalyzes the formation of norepinephrine from dopamine [20]. Our immunohistochemical staining showed higher levels of DBH in the peritumoral area, which may associate with the changed dopamine signaling surrounding the tumor. Dopamine could impact the pathogenesis of glioma by regulating tumor angiogenesis and vasculogenesis [21]. Therefore, an increased Cu could be due to an increasing blood supply around the tumor [19]; however, more evidence is still needed to confirm the findings in future studies.
In addition, another essential metal, Zn, is a component of >1000 proteins including several proteins involved in DNA-damage repair such as p53, which is mutated in half of human tumors, especially in GBM [22]. Zn was reported to be lower in the tumor core than the outer zone surrounding the GBM tumor [18], which, however, was not significant in our results. Se is an essential micronutrient with antioxidative and anticancer properties, which may impact on the interaction in the tumor microenvironment between tumor cells, tumor-associated cells, and immune cells [23]. Our results from the only validation set 2 show its up-regulation in the tumor core than the peritumor area, which still needed to be confirmed in future studies. In addition to the above, the other analyzed essential elements including Mg, Ca, Cr, Mn, Fe, and Co all showed no significant changes between the tumor core and peritumoral area. In the case of the essential elements, the relationship between them and cancer may not be as simple as could be assumed from the well-established requirement of essential elements for cell proliferation. Basic and pre-clinical studies indicate that deficiency of some essential elements like magnesium can have both anti- and pro-tumor effects [24]. Therefore, their possible associations and mechanisms in GBM, including cell proliferation, differentiation, angiogenesis, and apoptosis, still need be clarified in future studies.
For heavy metals, they are found in very limited concentrations in tumors and adjacent tissues, but have been successfully detected in both tumors and peritumor tissues, demonstrating that they can cross the blood–brain barrier. A previous study analyzed the heavy metal distribution in benign and malignant brain tumors and found a higher concentration of Pb and Hg and a lower concentration of Cd in the malignant tissue [25]. Consistent with this, our data suggested lower concentrations of Cd in the tumor than the peritumoral brain tissues in GBM, but changes in Pb concentrations were not observed. Cd has been known to be a transcriptional regulator, and the exposure of cancer cells to Cd may be associated with the acceleration of tumor progression [26]. Cd interacts with proteins and non-protein sulfhydryl groups, which has a wide range of effects, including damage to the vascular endothelium leading to decrease in availability of nitric oxide and endothelial dysfunction [27]. The Cd-binding protein NOS1, a nitric oxide synthase, was observed to be increased in the peritumoral area than the tumor core. NOS1 increased in multiple cancers and participates in various cancer processes such as formation, progression, and metastasis [28]. We supposed that, similar to Cu, higher levels of Cd in the peritumoral brain tissue may be associated with its potential for malignant transformation.
For other heavy metals, including As, Tl and Pb, concentrations range from a few nanograms per gram (Tl) to tens of nanograms per gram (As, Pb); however, they all showed no obvious changes between the tumor core and peritumoral area. Since still no sufficient evidence was obtained to implicate the role of these heavy metals in glioma development or progression, their effect and mechanisms on the pathologies of brain tumors need to be investigated [29].
With respect to tumor growth, which mainly occurs in the outer tumor zone, Cu and Cd alterations are in accordance with tumor-specific alterations in the microenvironment. To further clarify the Cu and Cd alterations, we analyzed their binding proteins from an anatomic view. Among the Cu-binding proteins, the DBH increased the most in the leading edge compared to the cellular tumor zone, suggesting dopamine metabolism was possibly more active in this region. Dopamine is currently regarded as an important endogenous regulator of tumor growth and may have potential roles in malignant transformation [21]. Among the Cd-binding proteins, nitric oxide synthase 1 (NOS1) was found to be only significantly increased in the leading edge compared to the cellular tumor zone. The enzyme nitric oxide synthase (NOS) is responsible for the generation of endogenous nitric oxide (NO), which has a definite role in the pathophysiology of glioblastoma. NOS promotes glioblastoma cell proliferation and invasion and increases resistance to apoptosis [30]. These results implied that the changes in Cu or Cd concentration in the outer tumor zone compared to the central tumor region may have resulted from the regulation of their binding proteins, which were supposed to have key roles for tumor cell proliferation and invasion.
Limitation
A major limitation of this study is the sample size. The concentrations of trace elements were determined based on 14 GBM patients. A training set and validation set were established and the testing method was well evaluated. However, future studies on a larger cohort may still be needed. In addition, considering the tumor heterogeneity and pathogenesis complexity, the mechanisms of trace elements, especially copper and cadmium, and their protein-binding forms, states, and proportions in GBM are unclear and still need to be further elucidated in vitro and/or animal experiments in the future.
Conclusion
This study determined and compared the concentrations of 13 essential and toxic trace elements in tumor and peritumoral brain tissues in GBM, and found significantly higher levels of copper and cadmium in the peritumoral brain region. Further analysis of the copper- and cadmium-binding proteins from an anatomic view suggested that DBH and NOS1 were obviously increased in the edges than the tumor core. These findings would be helpful for the community for further thorough analyses, including elucidating the pathological mechanism and developing new therapeutic strategies.
Availability of data and material
The data will be made available to others on reasonable request to the corresponding author after publication.
References
Ostrom QT, Price M, Neff C et al (2022) CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2015–2019. Neuro Oncol 24(Suppl 5):v1–v95. https://doi.org/10.1093/neuonc/noac202
Lemee JM, Clavreul A, Menei P (2015) Intratumoral heterogeneity in glioblastoma: don’t forget the peritumoral brain zone. Neuro Oncol 17(10):1322–1332. https://doi.org/10.1093/neuonc/nov119
Giambra M, Di Cristofori A, Valtorta S et al (2023) The peritumoral brain zone in glioblastoma: where we are and where we are going. J Neurosci Res 101(2):199–216. https://doi.org/10.1002/jnr.25134
Puchalski RB, Shah N, Miller J et al (2018) An anatomic transcriptional atlas of human glioblastoma. Science (New York, NY) 360(6389):660–663. https://doi.org/10.1126/science.aaf2666
Lossow K, Schwarz M, Kipp AP (2021) Are trace element concentrations suitable biomarkers for the diagnosis of cancer? Redox Biol 42:101900. https://doi.org/10.1016/j.redox.2021.101900
Bayir A (2015) Chapter 16 - The effects of trace element deficiencies on neurological disease and treatment with trace element support. In: Watson RR, Preedy VR (eds) Bioactive nutraceuticals and dietary supplements in neurological and brain disease. Academic Press, San Diego, pp 153–159
Grochowski C, Blicharska E, Krukow P et al (2019) Analysis of trace elements in human brain: its aim, methods, and concentration levels. Front Chem 7:115. https://doi.org/10.3389/fchem.2019.00115
Cilliers K, Muller CJF, Page BJ (2020) Trace element concentration changes in brain tumors: a review. Anat Rec 303(5):1293–1299. https://doi.org/10.1002/ar.24254
Zeng HL, Li H, Lu J, Guan Q, Cheng L (2019) Assessment of 12 metals and metalloids in blood of general populations living in Wuhan of China by ICP-MS. Biol Trace Elem Res 189(2):344–353. https://doi.org/10.1007/s12011-018-1486-8
Zeng HL, Yang Q, Yuan P, Wang X, Cheng L (2021) Associations of essential and toxic metals/metalloids in whole blood with both disease severity and mortality in patients with COVID-19. FASEB J 35(3):e21392. https://doi.org/10.1096/fj.202002346RR
Zhang B, Yang Q, Wang X, Jia B, Cheng L, Zeng H-L (2023) Association of whole blood metals/metalloids with severity in sepsis patients: a prospective, single-center, pilot study. J Trace Elem Med Biol 75:127098. https://doi.org/10.1016/j.jtemb.2022.127098
Ramos P, Pinto E, Santos A, Almeida A (2021) Reference values for trace element levels in the human brain: a systematic review of the literature. J Trace Elem Med Biol 66:126745. https://doi.org/10.1016/j.jtemb.2021.126745
Krebs N, Langkammer C, Goessler W et al (2014) Assessment of trace elements in human brain using inductively coupled plasma mass spectrometry. J Trace Elem Med Biol 28(1):1–7. https://doi.org/10.1016/j.jtemb.2013.09.006
Gong L, Yang Q, Liu CW, Wang X, Zeng HL (2021) Assessment of 12 essential and toxic elements in whole blood of pregnant and non-pregnant women living in Wuhan of China. Biol Trace Elem Res 199(6):2121–2130. https://doi.org/10.1007/s12011-020-02337-y
Zeng HL, Liu CW, Lu J, Wang X, Cheng L (2019) Analysis of urinary trace element levels in general population of Wuhan in central China. Environ Sci Pollut Res Int 26(27):27823–27831. https://doi.org/10.1007/s11356-019-05973-7
Zeng HL, Zhang B, Wang X, Yang Q, Cheng L (2021) Urinary trace elements in association with disease severity and outcome in patients with COVID-19. Environ Res 194:110670. https://doi.org/10.1016/j.envres.2020.110670
Tamás MJ, Sharma SK, Ibstedt S, Jacobson T, Christen P (2014) Heavy metals and metalloids as a cause for protein misfolding and aggregation. Biomolecules 4(1):252–267. https://doi.org/10.3390/biom4010252
Dehnhardt M, Zoriy MV, Khan Z et al (2008) Element distribution is altered in a zone surrounding human glioblastoma multiforme. J Trace Elem Med Biol 22(1):17–23. https://doi.org/10.1016/j.jtemb.2007.08.002
Gaman L, Radoi MP, Delia CE et al (2021) Concentration of heavy metals and rare earth elements in patients with brain tumours: analysis in tumour tissue, non-tumour tissue, and blood. Int J Environ Health Res 31(7):741–754. https://doi.org/10.1080/09603123.2019.1685079
Gonzalez-Lopez E, Vrana KE (2020) Dopamine beta-hydroxylase and its genetic variants in human health and disease. J Neurochem 152(2):157–181. https://doi.org/10.1111/jnc.14893
Lan YL, Wang X, Xing JS, Lou JC, Ma XC, Zhang B (2017) The potential roles of dopamine in malignant glioma. Acta Neurol Belg 117(3):613–621. https://doi.org/10.1007/s13760-016-0730-2
Ho E, Ames BN (2002) Low intracellular zinc induces oxidative DNA damage, disrupts p53, NFκB, and AP1 DNA binding, and affects DNA repair in a rat glioma cell line. Proc Natl Acad Sci USA 99(26):16770–16775. https://doi.org/10.1073/pnas.222679399
Yakubov E, Eibl T, Hammer A, Holtmannspotter M, Savaskan N, Steiner HH (2021) Therapeutic potential of selenium in glioblastoma. Front Neurosci 15:666679. https://doi.org/10.3389/fnins.2021.666679
Wolf FI, Trapani V (2012) Magnesium and its transporters in cancer: a novel paradigm in tumour development. Clin Sci (Lond) 123(7):417–427. https://doi.org/10.1042/cs20120086
Al-Saleh I, Shinwari N (2001) Levels of cadmium, lead, and mercury in human brain tumors. Biol Trace Elem Res 79(3):197–203. https://doi.org/10.1385/bter:79:3:197
Luparello C (2021) Cadmium-associated molecular signatures in cancer cell models. Cancers 13(11):2823. https://doi.org/10.3390/cancers13112823
Thevenod F, Fels J, Lee WK, Zarbock R (2019) Channels, transporters and receptors for cadmium and cadmium complexes in eukaryotic cells: myths and facts. Biometals 32(3):469–489. https://doi.org/10.1007/s10534-019-00176-6
Xu P, Ye S, Li K et al (2019) NOS1 inhibits the interferon response of cancer cells by S-nitrosylation of HDAC2. J Exp Clin Cancer Res 38(1):483. https://doi.org/10.1186/s13046-019-1448-9
Xie MY, Huang GL, Lin ZY et al (2023) Insufficient evidence to link human exposure to heavy metals with biomarkers of glioma. J Hazard Mater 447:130779. https://doi.org/10.1016/j.jhazmat.2023.130779
Fahey JM, Stancill JS, Smith BC, Girotti AW (2018) Nitric oxide antagonism to glioblastoma photodynamic therapy and mitigation thereof by BET bromodomain inhibitor JQ1. J Biol Chem 293(14):5345–5359. https://doi.org/10.1074/jbc.RA117.000443
Funding
The work was supported by the National Natural Science Foundation of China (Grant No. 31600666 to HL Zeng).
Author information
Authors and Affiliations
Contributions
HL Zeng, CX Li: conceptualization; HL Zeng, B Jia, Q Yang, F Zeng: data curation; L Zeng, B Jia, Q Yang, H Li: methodology; HL Zeng, CX Li: writing—original draft; L Cheng: writing—review and editing.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
The study was conducted in accordance with the guidelines approved by the Ethics Committees of Tongji Hospital (Wuhan, China).
Consent to participate
Informed consent for the use of the laboratory results and personal information in this study was obtained from all the patients, and all the data were analyzed anonymously.
Consent for publication
All authors have reviewed and approved the final manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zeng, HL., Jia, B., Yang, Q. et al. Assessment of 13 essential and toxic trace elements in tumor and peritumoral brain tissues from human glioblastoma. J Biol Inorg Chem 28, 699–709 (2023). https://doi.org/10.1007/s00775-023-02021-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00775-023-02021-1