
Abstract
Introduction
Osteonecrosis of the femoral head (ONFH) is a disease in which the blood supply of the femoral head is interrupted or damaged, resulting in joint dysfunction. Hypoxic environments increase the expression of EPO, VEGF, and HIF causes vascular proliferation and increases the blood supply. It also causes the organism to be in a state of hypercoagulability and increases thrombosis. Therefore, the purpose of this study was to explore the occurrence of ONFH after the use of glucocorticoids (GCs) under conditions of hypoxia tolerance for a long time.
Materials and methods
Sprague-Dawley rats were fed in a hypobaric hypoxic chamber at an altitude of 4000 m, the whole blood viscosity, and plasma viscosity were determined to analyze the blood flow and hemagglutination. Western blotting, polymerase chain reaction, and immunohistochemistry were used to detect EPO, VEGF, CD31, and osteogenesis related proteins. Femoral head angiography was used to examine the local blood supply and micro-CT scanning was used to detect the structure of the bone trabecula.
Results
Under hypoxic environments, the expression of EPO and VEGF increased, which increased the local blood supply of the femoral head, but due to more severe thrombosis, the local blood supply of the femoral head decreased.
Conclusions
Hypoxic environments can aggravate ONFH in SD rats; this aggravation may be related to the hypercoagulable state of the blood. We suggest that long-term hypoxia should be regarded as one of the risk factors of ONFH and we need to conduct a more extensive epidemiological investigation on the occurrence of ONFH in hypoxic populations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Globally, more than 100 million people inhabit the high-altitude regions, where the internal environment is deprived of oxygen, which is also a characteristic of chronic obstructive pulmonary disease (COPD), chronic heart failure (CHF), and other diseases. Hypoxia stimulation is known to exert certain effects on erythrocytes, microvessels, blood flow, thrombosis, and the production of erythropoietin (EPO) and vascular endothelial growth factor (VEGF) [1], which are involved in the occurrence and development of some diseases.
Osteonecrosis of the femoral head (ONFH) is a disease caused by the administration of high doses of glucocorticoids (GCs) and alcohol abuse [2], which often requires surgical treatment and imposes a huge burden on the patients and society [3,4,5,6]. Although the mechanisms underlying ONFH have not been fully and convincingly explained, endothelial dysfunction, thrombosis [7], and a series of pathological changes caused by them have been identified as the important causes of ONFH [8]. Several studies have shown that various physiological changes secondary to hypoxia play important roles in ONFH. Certain epidemiological studies also suggest that anoxia-related genetic variations may help in identifying ONFH susceptibility [9]. However, the effects of long-term hypoxia on ONFH have not been clarified yet.
The regulation of EPO expression by the liver and kidneys is one of the most classical physiological responses to hypoxia [10]. In addition to increasing VEGF expression and its mediated angiogenesis, EPO can also exert noteworthy protective effects against bone loss [11], by inhibiting the apoptosis of osteoblasts [12] and enhancing Runx2-mediated osteogenesis [13]. Animal experiments have shown that the simultaneous injection of EPO can partially prevent hormone-induced ONFH [14].
Additionally, VEGF is another cytokine that is upregulated following hypoxia and has a more obvious and definite preventive effect against ONFH [15]. Studies have shown that the polymorphism in the VEGF [9, 16, 17] and its promoter [18] is related to the increased risk of ONFH. Immunohistochemical staining also showed that the expression of VEGF decreased significantly after the use of GC [19] and the immune response of osteoblasts also changed correspondingly [20]. Moreover, it has been reported that the femoral head may be an anatomical site that is particularly sensitive to GC, and such sensitivity will have an obvious negative influence on the expression of VEGF [21], resulting in a series of pathological changes. Varoga et al. observed that compared with those from the periphery, osteoblasts distributed in the reactive penumbra exhibited increased immunoreactivity to VEGF. More importantly, in later-stage osteonecrosis, VEGF might accelerate the ingrowth of reparative arterioles into lesions [20]. Some researchers are of the opinion that angiogenic factors might be candidates for new therapeutic targets and diagnostic biomarkers for the treatment of diseases such as ONFH [22].
However, not all studies on the effects of hypoxia on ONFH had positive results. Jones [23] proposed the intravascular coagulation (IC) theory in 1992, pointing out that IC may be the final common pathway of ONFH caused by various factors. Although this hypothesis is not comprehensive, the view that hypercoagulability, which is characterized by thrombophilias and/or low fibrinolysis [24], is a high-risk factor for ONFH has been widely accepted [8, 25, 26], and hence, anticoagulant therapy has achieved a certain theoretical basis [27, 28]. When humans are chronically exposed to oxygen deprivation, there will be compensatory erythrocyte proliferation, increased blood viscosity, hemodynamic changes, which puts the body in a hypercoagulable state [1], increasing the risk of thrombosis [29], and thus raising the incidence rate of ONFH.
However, the relationship between hypoxia and bone cells is still unclear. Not only did an epidemiological survey show that hypoxia-inducible factor (HIF) polymorphisms have relationships with ONFH [30], but also showed a decrease in HIF expression in animal models treated with GCs [21]. It has been confirmed that transplantation of HIF-1α transgenic bone marrow mesenchymal stem cells (BM-MSCs) [31] and SDF-1α overexpression in BM-MSCs [32] can potentially promote the bone generation and the repair of the necrotic areas following corticosteroid-induced ONFH. All these findings suggest that HIF produced in local tissues may have a protective effect on ONFH, and after transfection of HIF-1α, both the proliferation and colony-forming ability of hypoxia-exposed BM-MSCs were significantly enhanced compared to those of BM-MSCs under conditions of normoxia [33]. However, in vitro experiments reported that hypoxia conditions may lead to the enhancement of the effects of GC by upregulating GC-receptor activity [34] and increasing the number of necrotic osteocytic cells through the overexpression of Dickkopf-1 (Dkk-1), an inhibitor of Wnt/β-catenin signaling [35].
These studies indicate that hypoxia may trigger a series of physiological changes that either prevent or aggravate ONFH. Therefore, in this study, we investigated the relationship between hypoxia and ONFH.
Materials and methods
Animal models and grouping
Forty Sprague-Dawley (SD) rats (Shanghai Animal Experimental Center, Shanghai, China), which were 8 weeks old and weighed 295–305 g, were divided into four groups—control, hypoxia, methylprednisolone (MP), and MP + hypoxia. Neither the rats in the control group nor the hypoxia group received any treatment; however, the control group was raised in a conventional oxygen environment, while the hypoxia group was raised in a hypoxic environment simulating an altitude of 4000 m. Rats in the (MP) group received intramuscular injection of MP (20 mg/kg/day) (Pfizer, USA) for three continuous days per week for 3 weeks (total MP 180 mg/kg), according to the method described by Xu et al. [36]. The MP + hypoxia group was firstly raised in a hypoxic environment (4000 m altitude) for 1 week, and then intramuscularly injected with methylprednisolone (same as the MP group), and was then continuously exposed to an hypoxic environment until the animals were sacrificed. All the samples were obtained 6 weeks after the first injection of MP. All experimental protocols were approved by the Animal Research Committee of Shanghai Jiaotong University School of Medicine.
Hypobaric hypoxia exposure
The rats were exposed to hypoxic experiment in a hypobaric hypoxia chamber, which was decompressed at a velocity of 10 m/min until the simulated altitude of 4000 m was achieved (O2, 12.5 kPa). Humidity in the chamber was maintained at 40–50% and the temperature ranged from 23 to 25 °C. The altitude was increased to 4000 m through the adapter module and food and water were added to the subjects daily. The altitude, temperature, and humidity of the laboratory module remained unchanged [37].
Oxygen content, complete blood count, and hemorheology
Firstly, the rats were anesthetized, and their abdominal aorta and vein were dissected; then, their abdominal aortas were punctured to extract three blood samples. One of the blood samples was isolated from the air for arterial blood gas (ABG) analysis including arterial oxygen partial pressure (PaO2) and arterial oxygen saturation (SaO2), and the rest were administered heparin for anticoagulation. Finally, the erythrocyte (RBC) count, hematocrit (HCT) values, platelet (PLT) count, and whole blood viscosity (WBV) (high shear rate, middle shear rate, low shear rate) and plasma viscosity (PV) were determined by routine laboratory assays.
Western blot (WB)
Kidney tissue was ground, homogenized, and mixed with cell lysis buffer and proteinase inhibitor. Proteins were extracted by centrifuging the samples, and their concentrations were tested with a BCA assay, and complete protein denaturation was conducted at 95 °C for 5 min. SDS-PAGE was performed on 30 µg of the protein samples, after which the proteins were transferred to polyvinylidene difluoride (PVDF) membrane. After blocking for 2 h with 5% non-fat dry milk, the membranes were incubated overnight with the primary-antibody of EPO (Abcam, Cambridge, MA, USA, 1:1000 dilution) and β-actin (CST, Danvers, MA, USA, 1:1000 dilution) at 4 °C, and then anti-rabbit IgG (CST, Danvers, MA, USA, 1:1000 dilution) labeled with horseradish peroxidase was used as a secondary antibody. The membrane was immersed with the secondary antibody for 2 h at 37 °C. The protein bands were visualized and detected with a gel image-processing system.
Quantitative real-time polymerase chain reaction analysis (qRT-PCR)
Total RNA was extracted from femoral head or kidney with TRIzol reagent (Invitrogen) after the tissue was fully ground. According to the manufacturer’s instructions, RT was performed on 1 µg of total RNA with EasyScript one-step gDNA Removal and cDNA Synthesis Supermix (TransGen Biotech, Beijing, China), and was then quantified by real-time qRT-PCR with the TransStart Tip Green qPCR SuperMix (TransGen Biotech, Beijing, China). The relative expression of mRNAs was normalized to that of the housekeeping gene glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and the primers used are listed in Table 1. The reaction conditions were 95 °C for 15 s and 60 °C for 60 s in all the 40 cycles, meanwhile, a 75–95 °C solubility curve was constructed.
Serum EPO, serum alkaline phosphatase (ALP), undercarboxylated osteocalcin (Glu-OC), and carboxylated osteocalcin (Gla-OC)
Blood samples were obtained by abdominal aortic puncture, centrifuged for 10 min at 4 °C, the serum was separated, which was firstly measured by a specific assay (Nanjing Jiancheng Biological Engineering Institute). The absorbance at 405 nm was recorded as the relative ALP levels in rats. Serum EPO levels were evaluated using the Mouse Erythropoietin Quantikine ELISA kit according to the manufacturer’s protocol (R&D Systems, California, USA). And we tested serum Glu-OC and Gla-OC with enzyme immunoassay (EIA) kits (Takara, Shiga, Japan). We analyzed the absorption of the samples at 450 nm, plotted each protein’s standard curve and found absolute concentrations from the standard curve.
Micro-CT scanning
After samples were collected from the sacrificed rats, the trabecular bone parameters of the upper outer subchondral bone of the right femoral head were estimated with a micro-CT scanner at a voxel of 9 μm. The parameters analyzed included bone mineral density (BMD), bone volume (BV), bone volume per tissue volume (BV/TV), trabecular thickness (Tb.Th), trabecular number (Tb.N) [38], and the bone structure of fractured femoral heads. The images were analyzed by CTAn software.
Angiography
After the rats were anesthetized, the abdominal aorta and vein were dissected, and the distal abdominal aorta was injected with heparin saline, 4% paraformaldehyde, and Microfil (MV-112, Flow Tech, Inc., Carver, MA) successively. Finally, micro-CT scanning was implemented as described above and 2-D images were transferred to CTVol and CTAn to reconstruct the 3-D images and calculate the vascular volume and vascular volume/total volume.
Histological and immunohistochemical analyses
After micro-CT scanning, the femoral heads were decalcified, paraffin-embedded, and sectioned at 5-μm thickness in the coronal plane. Most of them were deparaffinized, antigen retrieved, incubated with anti-OC (Abcam, Cambridge, MA, USA), anti-CD31 (Abcam, Cambridge, MA, USA), anti-Runx2 (Abcam, Cambridge, MA, USA) or anti-VEGF (Boshide, Wuhan, China) primary antibodies and the appropriate secondary antibodies successively, while the others were stained with hematoxylin and eosin (H&E) to evaluate the trabecular structure. Finally, sections were visualized with DAB and counterstained with hematoxylin. The photomicrographs were acquired using a LEICA DM 4000 (Leica Microsystems, Germany) and the images of immunohistochemical staining were analyzed with the software Image-Pro Plus. We recorded the target protein’s integrated option density (IOD) and the total area of trabecular bones, and obtained the mean density (IOD/area).
Statistical analyses
All data were analyzed by SPSS 22.0 (Microsoft, Chicago, IL, USA) and presented as the mean ± standard deviation (SD) with three independent experiments. Comparisons of data among the groups were performed using one-way analysis of variance (ANOVA) with Tukey’s post hoc test. P < 0.05 (*) and P < 0.01 (**) were considered statistically significant.
Results
Hypoxia reduced the PaO2 and SaO2
Post hypoxia exposure and GC treatment, there was no statistical difference in weight between the groups, indicating that hypoxia exposure and GC treatment had no effect on the general condition of the rats (Fig. 1a). However, ABG analysis reported that hypoxia resulted in significant reductions in both PaO2 and SaO2 (Fig. 1b, c).

Effects of hypoxia on general condition and ABG in mice. a Told us that the weight of the subjects in each group was basically the same, and the general situation did not change due to GC treatment and hypoxia. b, c Although GC did not affect ABG, hypoxia caused a significant decrease in PaO2 and SaO2 (** indicated P < 0.01)
Hypoxic exposure maintained the blood in a hypercoagulable state
Hemorheology test results showed that low oxygen levels significantly increased the PV or WBV of the blood samples with or without GC injection (Fig. 2a). The increase in WBV was not only due to the changes of PV, but also due to the RBC count and HCT increased caused by the decrease in oxygen content, while the use of hormones also increased the RBC count and HCT (Fig. 2b, c). The PLT fluctuation was not statistically significant, although it did occur due to the changes in drug administration or oxygen levels (Fig. 2d).

Hypoxia promotes the proliferation of red blood cells, and the increase of PV and WBV, makes the blood in a hypercoagulable state. a Hemorheology showed that hypoxia not only increased PV, but also significantly increased WBV in various cutting rates. b, c GC treatment increased both RBC and HCT, while hypoxia had a more significant effect on both. d The PLT of the four groups did not change. (* indicated P < 0.05; ** indicated P < 0.01)
Hypoxia increased the expression of EPO and VEGF
Hypoxia causes the kidney to overexpress EPO, while GC exposure reduces EPO expression (Fig. 3a, c). We observed from ELISA results that 1 week’s hypoxia treatment in advance can effectively prevent GC from reducing serum EPO and maintain EPO content at the same level as that in the control group (Fig. 3e). PCR showed the same trend as WB (Fig. 3c). Similar to EPO, VEGF expression increased due to hypoxia and decreased with the use of GC. Although rats pretreated with hypoxia still showed lower VEGF expression level than those in the control group due to the use of GC, it was still at a higher level than that in the experimental subjects without hypoxia (Fig. 3b). The PCR results of VEGF were similar, but the mRNA transcription level of rats treated with hypoxia and GC was higher than that of the control group (Fig. 3d).

Hypoxia stimulates the overexpression of EPO and VEGF. a WB proved that hypoxia maybe change the concentration of EPO (P < 0.05), and it is more significant between the MP and MP + hypoxia group (P < 0.01). Even after GC was used, EPO expression remained at the same level as that of the control group. b Hypoxia also increased the expression of VEGF (P < 0.01), significantly improving the expression level of VEGF after GC exposure (P < 0.01), although it was still lower than the general level (P < 0.01). The arrow represents the target protein, that is, VEGF staining. c, d The mRNA transcription level of both was consistent with the protein expression trend, but the VEGF transcription level of the MP + hypoxia group was higher than that of the control group. e ELISA confirmed that hypoxia can effectively induce the overexpression of serum EPO (P < 0.01), while the use of MP can reduce the expression (P < 0.05). (* indicated P < 0.05; ** indicated P < 0.01)
Hypoxia can aggravate the blood supply damage in ONFH
In the absence of GC, hypoxia exposure enhanced the blood supply to the femoral head, resulting in a statistically significant increase in vascular volume and vascular volume/total volume. By analyzing the 3D-reconstruction of angiography, we believe that this increase is mainly manifested in a large increase in the number of tiny vessels (Fig. 4d–f). However, in both the groups injected with GC, the hypoxia-exposed group did not exhibit the same improvement in blood supply but showed lesser vascular volume and vascular volume/total volume (Fig. 4d–f). However, there was no such divergence in CD31. We deduced from that hypoxia can increase CD31 expression, while GC can decrease it. It should be noted that there was no significant difference in the immunohistochemical density between the MP + hypoxia group and the Control group, but PCR showed that mRNA in the former group was lower than that in the latter group (Fig. 4a–c).

Effect of hypoxia on local blood supply to femoral head. a, b No matter whether GC is injected or not, hypoxia can significantly improve the expression of CD31 (P < 0.01), and CD31 still remains at the general level after GC is applied through pre-hypoxia. The arrow represents the target protein, that is, VEGF staining. The arrow points to the staining of CD31 protein in endothelial cells. c PCR showed the same results. d, e Hypoxia did significantly improve the blood vessel volume of femoral head (P < 0.01). Through 3D reconstruction, we observed that this improvement may be more caused by microvascular angiogenesis, but after GC use, the MP + hypoxia group had more serious blood supply impairment. f VV/TV support the above results (** indicated P < 0.01)
Hypoxia impairs the osteogenic differentiation of ONFH
In immunohistochemical and PCR experiments, hypoxia alone did not have a significant effect on the osteogenesis of the femoral head. Administration of GC significantly lowered the amount of protein and mRNA expression in OC and Runx2, and this change became more serious on hypoxic exposure. The changes between the groups were the same in the immunohistochemical analyses and PCR, making the results more persuasive (Fig. 5a–d). Although hypoxia impaired the OC and Runx2 expression, PCR results showed that it did not lead to a statistically significant decrease in the transcription level of ALP mRNA in the femoral head, which decreased with the use of GC (Fig. 5d). Nevertheless, this disparity was not observed in serum ALP activity, in which there was no difference among the groups (Fig. 6a).

Hypoxia aggravated the damage of osteogenic differentiation in ONFH. a–c Hypoxia itself did not affect osteocyte differentiation, but simultaneous exposure to hypoxia and GC resulted in a decrease in OC (P < 0.05),and the decrease of Runx2 was more obvious (P < 0.01). The arrows represent stained target proteins, including OC, which is mainly expressed in the cytoplasm, and Runx2, which is expressed in the nucleus. d The PCR results of OC and Runx2 showed the same trend as immunohistochemistry. (* indicated P < 0.05; ** indicated P < 0.01)

Influence of hypoxia on ALP activity, gla-oc and gla-oc. a–d Hypoxia has no obvious effect on ALP activity and Glu-OC,Gla-OC. b, c The injection of GC reduced the content of Glu-OC and Gla-OC (** indicated P < 0.01)
Effect of hypoxia on Glu-OC and Gla-OC
We expected to observe the reduction of Glu-OC and Gla-OC in the blood samples with the use of GC, as has been reported in many studies [39, 40]. However, we did not find that lower oxygen content had a significant effect on either of them, although we observed a decline (Fig. 6b–d).
Hypoxia aggravates the incidence of ONFH in the subchondral area
Although H&E staining lacks quantifiable detection indicators, histological evidences are still an important basis for judging the occurrence and phase of the ONFH. The structure and cell morphology of the femoral head in the control group and hypoxia group were normal, including epiphysis and regular trabeculae. In MP and MP + hypoxia groups, we not only found the disappearance of trabecular structure, but also observed empty lacunas and newly formed osteoid, what’s more, hypertrophic fatty cells and necrotic nuclei were observed at high magnification.
With MicroCT, both the control and hypoxia groups showed normal trabecular structure, and imaging changes were observed in 8 rats in the MP group, and 10 rats in the MP + hypoxia group. Thus, it can be stated that compared with 8 rats that showed mild necrosis in the MP group, all the 10 rats in the MP+ hypoxia group showed different degrees of necrosis (Fig. 7b). BMD, BV, and Tb.Th were also recorded and analyzed to assess the transformations in bone tissue (Fig. 7c–g). The BMD in the MP group was significantly lower than that in the control group and the damage was aggravated with the reduced oxygen in the MP + hypoxia group, and all the other parameters except trabecular count showed approximate fluctuations.

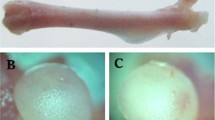
MicroCT scanning and H&E staining of the subchondral region of the femoral head. a H&E staining of the femoral head. In the control and hypoxia groups, there is the normal structure of the femoral head, including epiphysis and trabeculae. While in the two groups treated with MP, we can observe empty lacunas and newly formed osteoid. The arrows identify hypertrophic fat cells and pyknotic necrotic nuclei. b 2-D images of the coronal section of the femoral heads. c–g Morphometric analysis evaluated a series of parameters in the upper outer subchondral bone of the femoral heads (* indicated P < 0.05; ** indicated P < 0.01)
Discussion
ONFH is a debilitating disease often accompanied by osteoporosis [41] and is caused by the excessive administration of GCs. In most of the cases, it progresses to the collapse of the femoral head and degenerative arthritis [2, 5]. However, these lesions are originally formed due to the reduced capacity for bone formation and differentiation and impaired blood supply to the femoral head [8, 42]. In this series of pathological processes, the view that endothelial cell injury is a key event in ONFH is increasingly accepted and promoted [7, 17]. Hypoxia has been reported to lower the hydroxylation of HIF at different sites, enabling HIF to escape degradation and inactivation. HIF then forms active transcriptional complexes at thousands of loci across the human genome, increases the expression of EPO and VEGF above normal, promotes capillary growth and vascular volume [10, 43, 44], all of which are considered to have a protective effect on the occurrence of ONFH [12, 20]. Through HIF-1α-induced VEGF,hypoxia ameliorates the expression of Runx2 in periodontal ligament stem cells [45]. VEGF is highly correlated with ONFH and largely responsible for maintaining the fine vascular network that surrounds the highly remodeling bone [20, 46] and EPO enhances the Runx2-mediated osteogenesis, lessening bone loss in ONFH in rats [13]. However, decreased oxygen content will lead to compensated erythrocyte proliferation, increased blood viscosity, and hemodynamic changes [1, 29]. All these changes will make blood hypercoagulable, promoting the formation of thrombosis, reducing the effective vessel volume, and thus aggravating osteonecrosis [23, 47]. Hypoxia can also increase the effect of GC, which aggravates osteonecrosis by increasing the expression of Dkk-1 and up-regulating GC receptor activity [34, 35]. Collectively, hypoxia has diverse effects on ONFH and till date, there are no studies which have clearly established the relationship between hypoxia and ONFH.
In our study, we observed that the hypobaric hypoxia chamber simulated the anoxic environment efficiently, significantly increasing the expression of EPO and VEGF in the femoral head. Chen and Jin have both reported that EPO can exert noteworthy protective effects against bone loss [11], by inhibiting the apoptosis of osteoblasts [12] and enhancing the Runx2-mediated osteogenesis [13]. The effects of VEGF on ONFH have been widely reported [19, 20, 31, 46]. And before using GC, we observed that hypoxia caused a significant increase in the vascular network and the volume of blood vessels, and this increase was more manifested in the smaller blood vessels which assist in the prevention of osteonecrosis of the femoral head [48, 49]. Therefore, we can deduce that hypoxia may play a very important role in improving blood supply and preventing ONFH.
However, our results are not consistent with the above assumptions. After GC administration, angiography proved that this advantage of blood supply disappeared completely, which showed that hypoxia did not increase the volume of blood vessels, but significantly damaged the blood supply of femoral head and significantly reduced BV/TV.
Further, we also evaluated the expression of OC and Runx2 in the femoral head, which showed the same trend in the PCR and immunohistochemistry analyses. Ding H et al observed that hypoxia stimulated the HIF expression, which had a protective effect on ONFH [31], and Ciapetti et al. [33] reported that the expression of bone-related genes was significantly increased under hypoxia. Some authors also suggested that hypoxia combined with GC can increase its effect, thus aggravating ONFH [34, 35]. Our in vivo results ultimately supported the latter, with a combination of hypoxia and GC resulting in lower OC and Runx2 expression in the femoral head.
To explore the reasons, we think there are two main points. First, although hypoxia had no effect on the general condition of rats, we observed that hypoxia significantly reduced PaO2 and SaO2, which is consistent with the generally accepted consensus [1, 29], and may be a reason for the low expression of osteogenesis-related proteins OC and Runx2. Second, hypoxia increases RBC, HCT, WBV and PV, which make the blood hypercoagulable and more prone to thrombosis. We speculate that after the endothelial cell injury caused by the use of GC, the hypercoagulable state of blood leads to more extensive and severe thrombosis, which leads to more vascular loss, resulting in more severe damage of blood supply in the MP + hypoxia group than in the MP group. In addition, the interruption of local blood supply, in turn, aggravates local hypoxia and also aggravates the low expression of bone differentiation protein, not to mention that blood hypercoagulability is a recognized risk factor for ONFH [26, 28].
In general, although pathological evidence showed that ONFH will occur after MP treatment regardless of hypoxia exposure, hypoxia caused the GC-treated rats to exhibit lower BMD, lesser BV, dropped BV/TV and thinner Tb.Th. Therefore, our in vivo experiments suggested that the comprehensive effect of hypoxia on ONFH is its aggravation.
Additionally, it should be noted that the expression of the VEGF protein in the femoral head of rats exposed to both GCs and hypoxia was lower than that in case of the rats from the control group, but the PCR results showed that the VEGF mRNA expression was increased, suggesting that hypoxia may interfere with the translation process of VEGF. However, this conjecture needs to be verified in future studies. Meanwhile, our experiment is limited to macroscopic observation of the relationship between hypoxia and ONFH. We observed a decrease in bone tissue differentiation, but we were not able to determine whether it was directly caused by hypoxia or was caused by decreased blood supply, which was secondary to hypoxia. We deduced from that hypoxia can stimulate the production of HIF, EPO, VEGF and other cytokines, but how these factors regulate Runx2, OC and other osteogenic genes in bone cells. So, all these need further study and explanation.
In conclusion, hypoxia makes the blood hypercoagulable, reduces blood supply, counteracts the effects of EPO, VEGF, and other protective factors, and eventually aggravates ONFH. Hence, long-term hypoxia should be considered as one of the risk factors of ONFH and further studies need to be conducted on the epidemiological occurrence of ONFH in hypoxic populations.
References
García-Ortega A, Mañas E, López-Reyes R, Selma MJ, García-Sánchez A, Oscullo G, Jiménez D, Martínez-García MÁ (2019) Obstructive sleep apnoea and venous thromboembolism: pathophysiological links and clinical implications. Eur Respir J. https://doi.org/10.1183/13993003.00893-2018
Caplan A, Fett N, Rosenbach M, Werth VP, Micheletti RG et al (2017) Prevention and management of glucocorticoid-induced side effects: a comprehensive review: a review of glucocorticoid pharmacology and bone health. J Am Acad Dermatol 76:1–9
Uesugi Y, Sakai T, Seki T, Hayashi S, Nakamura J et al (2018) Quality of life of patients with osteonecrosis of the femoral head: a multicentre study. Int Orthop 42:1517–1525
Osawa Y, Seki T, Takegami Y, Kusano T, Makida K, Ishiguro N (2018) Cementless total hip arthroplasty for osteonecrosis and osteoarthritis produce similar results at ten years follow-up when matched for age and gender. Int Orthop 42:1683–1688
Maruyama M, Nabeshima A, Pan CC, Behn AW, Thio T, Lin T, Pajarinen J, Kawai T, Takagi M, Goodman SB, Yang YP (2018) The effects of a functionally-graded scaffold and bone marrow-derived mononuclear cells on steroid-induced femoral head osteonecrosis. Biomaterials 187:39–46
Zhao DW, Yu M, Hu K, Wang W, Yang L et al (2015) Prevalence of nontraumatic osteonecrosis of the femoral head and its associated risk factors in the Chinese population: results from a nationally representative survey. Chin Med J 128:2843–2850
Sung PH, Yang YH, Chiang HJ, Chiang JY, Chen CJ, Yip HK, Lee MS (2018) Cardiovascular and cerebrovascular events are associated with nontraumatic osteonecrosis of the femoral head. Clin Orthop Relat Res 476:865–874
Kerachian MA, Séguin C, Harvey EJ (2009) Glucocorticoids in osteonecrosis of the femoral head: a new understanding of the mechanisms of action. J Steroid Biochem Mol Biol 2009(114):121–128
Hong JM, Kim TH, Kim HJ, Park EK, Yang EK, Kim SY (2010) Genetic association of angiogenesis- and hypoxia-related gene polymorphisms with osteonecrosis of the femoral head. Exp Mol Med 42:376–385
Schödel J, Ratcliffe PJ (2019) Mechanisms of hypoxia signalling: new implications for nephrology. Nat Rev Nephrol 15:641–659
Bakhshi H, Rasouli MR, Parvizi J (2012) Can local erythropoietin administration enhance bone regeneration in osteonecrosis of femoral head? Med Hypotheses 79:154–156
Chen S, Li J, Peng H, Zhou J, Fang H (2014) Administration of erythropoietin exerts protective effects against glucocorticoid-induced osteonecrosis of the femoral head in rats. Int J Mol Med 33:840–848
Xu T, Jin H, Lao Y, Wang P, Zhang S, Ruan H, Mao Q, Zhou L, Xiao L, Tong P, Wu C (2017) Administration of erythropoietin prevents bone loss in osteonecrosis of the femoral head in mice. Mol Med Rep 16:8755–8762
Yan Y-Q, Pang Q-J, Xu R-J (2018) Effects of erythropoietin for precaution of steroid-induced femoral head necrosis in rats. BMC Musculoskelet Disord 19:282
Ma L, Hernandez MO, Zhao Y, Mehta M, Tran B, Kelly M, Rae Z, Hernandez JM, Davis JL, Martin SP, Kleiner DE, Hewitt SM, Ylaya K, Wood BJ, Greten TF, Wang XW (2019) Tumor cell biodiversity drives microenvironmental reprogramming in liver cancer. Cancer Cell 36:418.e6–430.e6
Ma W, Xin K, Chen K, Tang H, Chen H, Zhi L, Liu H (2018) Relationship of common variants in VEGFA gene with osteonecrosis of the femoral head: a Han Chinese population based association study. Sci Rep 8:16221
Chen C, Yang S, Feng Y, Wu X, Chen D, Yu Q, Wang X, Li J, Chen J (2013) Impairment of two types of circulating endothelial progenitor cells in patients with glucocorticoid-induced avascular osteonecrosis of the femoral head. Jt Bone Spine 80:70–76
Kim T, Hong JM, Lee J, Oh B, Park EK, Lee C, Bae S, Kim S (2008) Promoter polymorphisms of the vascular endothelial growth factor gene is associated with an osteonecrosis of the femoral head in the Korean population. Osteoarthr Cartil 16:287–291
Yang F, Luo P, Ding H, Zhang C, Zhu Z (2018) Collagen type V a2 (COL5A2) is decreased in steroid-induced necrosis of the femoral head. Am J Transl Res 10:2469–2479
Varoga D, Drescher W, Pufe M, Groth G, Pufe T (2009) Differential expression of vascular endothelial growth factor in glucocorticoid-related osteonecrosis of the femoral head. Clin Orthop Relat Res 467:3273–3282
Weinstein R, Hogan E, Borrelli M, Liachenko S, O’Brien C, Manolagas S (2017) The pathophysiological sequence of glucocorticoid-induced osteonecrosis of the femoral head in male mice. Endocrinology 158:3817–3831
Chim SM, Tickner J, Chow ST, Kuek V, Guo B, Zhang G, Rosen V, Erber W, Xu J (2013) Angiogenic factors in bone local environment. Cytokine Growth Factor Rev 24:297–310
Jones JP (1992) Intravascular coagulation and osteonecrosis. Clin Orthop Relat Res 277:41–53
Ferrari P, Schroeder V, Anderson S, Kocovic L, Vogt B, Schiesser D, Marti HP, Ganz R, Frey FJ, Kohler HP (2002) Association of plasminogen activator inhibitor-1 genotype with avascular osteonecrosis in steroid-treated renal allograft recipients. Transplantation 74:1147–1152
Li Y, Liu FX, Yuan C, Meng L (2017) Association between plasminogen activator inhibitor gene polymorphisms and osteonecrosis of the femoral head susceptibility: a case-control study. Medicine 96:e7047
Kang P, Shen B, Yang J, Pei F (2008) Circulating platelet-derived microparticles and endothelium-derived microparticles may be a potential cause of microthrombosis in patients with osteonecrosis of the femoral head. Thromb Res 123:367–373
Cao F, Liu G, Wang W, Wang B, Wei X, Lu F, Yang F, Kang K, Wang Y, Yang J, Qin K, Zhao D (2017) Combined treatment with an anticoagulant and a vasodilator prevents steroid-associated osteonecrosis of rabbit femoral heads by improving hypercoagulability. Biomed Res Int 2017:1624074
Wang W, Zhang N, Guo W, Gao F (2018) Combined pharmacotherapy for osteonecrosis of the femoral head after severe acute respiratory syndrome and interstitial pneumonia: two and a half to fourteen year follow-up. Int Orthop 42:1551–1556
Kicken CH, Ninivaggi M, Konings J, Moorlag M, Huskens D, Remijn JA, Bloemen S, Lancé MD, De Laat B (2018) Hypobaric hypoxia causes elevated thrombin generation mediated by FVIII that is balanced by decreased platelet activation. Thromb Haemost 118:883–892
Hong JM, Kim TH, Chae SC, Koo KH, Lee YJ, Park EK, Choi JY, Ryoo HM, Kim SY (2007) Association study of hypoxia inducible factor 1alpha (HIF1alpha) with osteonecrosis of femoral head in a Korean population. Osteoarthr Cartil 15:688–694
Ding H, Gao YS, Hu C, Wang Y, Wang CG, Yin JM, Sun Y, Zhang CQ (2013) HIF-1α transgenic bone marrow cells can promote tissue repair in cases of corticosteroid-induced osteonecrosis of the femoral head in rabbits. PLoS One 8:e63628
Yang F, Xue F, Guan J, Zhang Z, Yin J, Kang Q (2018) Stromal-cell-derived factor (SDF) 1-alpha overexpression promotes bone regeneration by osteogenesis and angiogenesis in osteonecrosis of the femoral head. Cell Physiol Biochem 46:2561–2575
Ciapetti G, Granchi D, Fotia C, Savarino L, Dallari D, Del Piccolo N, Donati DM, Baldini N (2016) Effects of hypoxia on osteogenic differentiation of mesenchymal stromal cells used as a cell therapy for avascular necrosis of the femoral head. Cytotherapy 18:1087–1099
Zou W, Yang S, Zhang T, Sun H, Wang Y, Xue H, Zhou D (2015) Hypoxia enhances glucocorticoid-induced apoptosis and cell cycle arrest via the PI3K/Akt signaling pathway in osteoblastic cells. J Bone Miner Metab 33:615–624
Ueda S, Ichiseki T, Yoshitomi Y, Yonekura H, Ueda Y, Kaneuji A, Matsumoto T (2015) Osteocytic cell necrosis is caused by a combination of glucocorticoid-induced Dickkopf-1 and hypoxia. Med Mol Morphol 48:69–75
Xu J, Gong H, Lu S, Deasey MJ, Cui Q (2018) Animal models of steroid-induced osteonecrosis of the femoral head-a comprehensive research review up to 2018. Int Orthop 42:1729–1737
Jing L, Shao J, Sun W, Lan T, Jia Z, Ma H, Wang H (2019) Protective effects of two novel nitronyl nitroxide radicals on heart failure induced by hypobaric hypoxia. Life Sci 248:116481
Ma J, He W, Zhao J, Kuang M, Bai H, Sun L, Lu B, Tian A, Wang Y, Dong B, Wang Y, Ma X (2017) Bone microarchitecture and biomechanics of the necrotic femoral head. Sci Rep 7:13345
Shiraki M, Shiraki Y, Aoki C, Miura M (2000) Vitamin K2 (menatetrenone) effectively prevents fractures and sustains lumbar bone mineral density in osteoporosis. J Bone Miner Res 15:515–521
Zhang YL, Yin JH, Ding H, Zhang W, Zhang CQ, Gao YS (2016) Vitamin K2 prevents glucocorticoid-induced osteonecrosis of the femoral head in rats. Int J Biol Sci 12:347–358
Tian L, Baek SH, Jang J, Kim SY (2018) Imbalanced bone turnover markers and low bone mineral density in patients with osteonecrosis of the femoral head. Int Orthop 42:1545–1549
Fowler TW, Acevedo C, Mazur CM, Hall-Glenn F, Fields AJ, Bale HA, Ritchie RO, Lotz JC, Vail TP, Alliston T (2017) Glucocorticoid suppression of osteocyte perilacunar remodeling is associated with subchondral bone degeneration in osteonecrosis. Sci Rep 7:44618
Gonzalez FJ, Xie C, Jiang C (2018) The role of hypoxia-inducible factors in metabolic diseases. Nat Rev Endocrinol 15:21–32
Żebrowska A, Jastrzębski D, Sadowska-Krępa E, Sikora M, Di Giulio C (2019) Comparison of the effectiveness of high-intensity interval training in hypoxia and normoxia in healthy male volunteers: a pilot study. BioMed Res Int 2019:7315714
Xu Q, Liu Z, Guo L, Liu R, Li R, Chu X, Yang J, Luo J, Chen F, Deng M (2019) Hypoxia mediates runt-related transcription factor 2 expression via induction of vascular endothelial growth factor in periodontal ligament stem cells. Mol Cells 42:763–772
Zaidi M, Sun L, Robinson LJ, Tourkova IL, Liu L, Wang Y, Zhu LL, Liu X, Li J, Peng Y, Yang G, Shi X, Levine A, Iqbal J, Yaroslavskiy BB, Isales C, Blair HC (2010) ACTH protects against glucocorticoid-induced osteonecrosis of bone. Proc Natl Acad Sci USA 107:8782–8787
Zhao L, Wu X, Wu H, Su J, Zhang W, Zhao Y, Zhang X, Zheng W (2016) Symptomatic knee osteonecrosis in patients with systemic lupus erythematosus: a case-control study. Rheumatol Int 36:1105–1111
Janke LJ, Liu C, Vogel P, Kawedia J, Boyd KL, Funk AJ, Relling MV (2013) Primary epiphyseal arteriopathy in a mouse model of steroid-induced osteonecrosis. Am J Pathol 183(1):19–25
Drescher W, Beckmann R, Kasch R, Pufe M, Knobe M, Kweider N, Hassenpflug J, Tingart M, Pufe T, Kadyrov M (2011) Nitrate patch prevents steroid-related bone necrosis. J Orthop Res 29:1517–1520
Acknowledgements
The current research was funded by the Key R&D Program of the Tibet Autonomous region (no. XZ2017ZY01). We are also indebted to the teachers of the 940th Hospital of Joint Logistics Support force of PLA for their assistance.
Author information
Authors and Affiliations
Contributions
Wei Zhang and Bo-hao Yin conceived and designed the study. Bo-hao Yin, and Hong-chi Chen performed the experiments. Qiu-ming Gao provided the hypobaric hypoxia chamber. Bo-hao Yin wrote the paper. Wei Zhang, Tan-zhu Li, and Jing-wen Liu reviewed and edited the manuscript. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interest exists.
Ethical approval
All experimental protocols were approved by the Animal Research Committee of Shanghai Jiaotong University School of Medicine.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Yin, Bh., Chen, Hc., Zhang, W. et al. Effects of hypoxia environment on osteonecrosis of the femoral head in Sprague-Dawley rats. J Bone Miner Metab 38, 780–793 (2020). https://doi.org/10.1007/s00774-020-01114-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-020-01114-0