
Abstract
The postpartum period may be a particular window of vulnerability for eating disorder symptoms given changes to body shape and weight that women experience. However, no quantitative studies have identified risk factors for postpartum eating disorder symptoms, and current psychosocial frameworks of risk may be missing key elements unique to this period. This manuscript reviews existing quantitative and qualitative literature regarding the developmental trajectory of eating disorder symptoms during the perinatal period and proposes an application of three psychosocial models of eating disorder risk (objectification theory, the tripartite influence model of body image and eating disturbances, and social comparison theory) to the postpartum period. Drawing on quantitative and qualitative literature, this paper identifies novel postpartum-specific factors that should be included for consideration in psychosocial models (e.g., self-oriented body comparison and pressure to achieve a prepregnancy weight and shape). This review is the first to theorize potential postpartum-specific risk factors for postpartum eating disorder symptoms. Prior models of eating disorder risk omit key psychosocial factors that are unique to the postpartum period. Other limitations of prior research relate to measurement and methodology. This critical window of vulnerability has been largely ignored in the quantitative literature and necessitates further research.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Researchers have long understood the importance of psychosocial frameworks for understanding the development and maintenance of eating disorder symptoms (see Fitzsimmons-Craft 2011 for review). These models have been helpful in understanding risk for periods during which females experience an increase in eating disorder symptoms—for example, puberty and adolescence (Rodgers et al. 2014). One period during which females seem to be vulnerable to increased eating disorder symptoms that has not been conceptualized within psychosocial frameworks is the postpartum period. Although previously known risk factors of eating disorder symptoms may be relevant to women during the postpartum period, this paper applies three different psychosocial frameworks (objectification theory, the tripartite model of influence for body image and eating disturbances, and social comparison theory) to the postpartum period by proposing potential postpartum-specific factors that may be unique to women during this developmental period that have not been previously considered.
This paper will (1) review existing literature regarding the developmental trajectory of eating disorder symptoms during pregnancy and the postpartum period, (2) discuss an application of three psychosocial models of eating disorder risk to the postpartum period by identifying unique postpartum-specific factors to consider, and (3) highlight limitations of the current literature and propose new directions for future research (4) and implications for prevention and treatment.
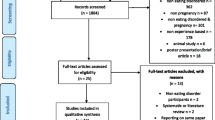
Research studies (both qualitative and quantitative) related to eating disorder symptoms in the perinatal period were retrieved by December 2019 using computer-based searches from the following databases which were available to the author’s institution: PubMed, PsycINFO, and Google Scholar using relevant keywords (e.g., body image, disordered eating, pregnancy, postpartum, perinatal). These databases yielded search results of approximately 120 articles.
Eating disorder symptoms during the postpartum period
The perinatal period is a time women may be particularly vulnerable to eating disorder symptoms given the dramatic changes to their body weight and shape that can occur. Epidemiological data found gestational weight gain exceeded the recommended guidelines in 58% of pregnancies, and approximately 15% of women experienced a postpartum weight retention of at least 10 pounds for 12 months following birth (Ashley-Martin and Woolcott 2014) indicating that many women gain more weight than medically recommended and retain excess weight for months after birth.
In addition to these fluctuations in weight, women may experience changes to their body shape including increased breast size, thickening of waist, and widening of hips (Heinberg and Guarda 2002). Women describe fluid retention, larger and leaking breasts, transformations of nipple color, dry skin, acne, loss of muscle tone, rashes, and varicose veins as objectionable pregnancy-related changes to their body shape and appearance (Clark et al. 2009a). Despite these changes being developmentally normal, and some of them healthy for the viability of the fetus (Institute of Medicine 2007), they are in direct contrast to Western culture’s thin beauty ideal, and many women report feeling negative about their postpartum bodies (Walker 1998). Considering how dynamically the human body changes during pregnancy and the postpartum period, it is important to understand how eating disorder symptoms change during these times.
Hawkins and Gottlieb (2013) theorize there are three distinct phases of increased risk for eating disorder symptoms during the perinatal period: (1) immediately following the diagnosis of pregnancy, (2) beginning of the second trimester when mothers begin to appear pregnant, and (3) the postpartum period.
Regarding the first two proposed phases, prior research of eating disorder symptoms during pregnancy has yielded mixed results. Some evidence suggests that pregnancy may protect against increased eating disorder symptoms. For example, women with bulimia nervosa reported a reduced number of binge episodes per week while pregnant (Lacey and Smith 1987; Morgan et al. 1999), and women with anorexia nervosa or bulimia nervosa experienced a reduction in overall eating disorder symptoms (Bonne et al. 1996) including dietary restriction, body dissatisfaction, and frequencies of both binge eating and purging episodes (Crow et al. 2008).
Conversely, other evidence suggests women with eating disorders may experience no changes in symptoms during pregnancy (e.g., dietary restriction; Blais et al. 2000). Coker et al. (2013) found that women with an eating disorder during their pregnancy remained stable and experienced no recovery of their symptoms during this period.
In contrast to the discrepant results regarding the trajectory of eating disorder symptoms during pregnancy, the literature is more consistent regarding Hawkins and Gottleib’s (2013) proposed third period of heightened risk for eating disorder symptoms: the postpartum period. A population-based Swedish study found that approximately 11% of women experienced an eating disorder postpartum (Larsson and Andersson-Ellström 2003). Prevalence rates for postpartum eating disorders (assessed 18 months postpartum) are roughly 0.2% for anorexia nervosa (compared with 0.1% prepregnancy), and 0.7% for bulimia nervosa (compared with 0.9% prepregnancy and 0.2% during pregnancy) suggesting that the transition from pregnancy to the postpartum period may increase one’s risk of developing anorexia nervosa or bulimia nervosa (Knoph et al. 2013). Data found that although more than 50% of treatment-seeking women with anorexia nervosa or bulimia nervosa achieved full remission of symptoms during pregnancy, only approximately 20% of them remained symptom-free within the first 12 months postpartum indicating a resurgence of symptoms for some women after giving birth (Lemberg and Phillips 1989). Nonclinical data suggest the percent of women with suspected eating disorders nearly triples from pregnancy to the postpartum period (5.3% during pregnancy compared with 12.8% postpartum; Pettersson et al. 2016).
Only three clinical studies have examined specific eating disorder symptoms during the postpartum period. All three were longitudinal studies that found binge eating and purging behaviors, dietary restriction, and weight and shape concerns decreased during pregnancy for women diagnosed with an eating disorder, yet returned during the postpartum period to a severity that was equal to or greater than they experienced prior to conception (Lacey and Smith 1987; Morgan et al. 1999; Crow et al. 2008).
Among community samples, evidence suggests 48% of women report feeling dissatisfied with their weight during the postpartum period (Walker 1998). Body dissatisfaction has been shown to increase (Coker and Abraham 2015; Shloim et al. 2015) and in some cases greater than prepregnancy dissatisfaction (Rallis et al. 2007). Body satisfaction has been shown to decrease and dietary restriction to increase during the postpartum period compared with during pregnancy (Baker et al. 1999). In general, postpartum women report an ideal weight that is an average of 6 pounds thinner than their prepregnancy ideal weight (Shrewsbury et al. 2009) suggesting there may be a different, thinner, postpartum body ideal compared with the prepregnancy body ideal. Nunes et al. (2014) found that 60% more women reported shape and weight concerns at 4–5 months postpartum compared with prepregnancy and disordered eating behaviors (e.g., dietary restriction, binge eating, purging, and laxative and diuretic use) increased during the postpartum period but did not return to the same levels as during prepregnancy.
In addition to quantitative evaluations of specific disordered eating behaviors and cognitions during the postpartum period, qualitative data have examined women’s postpartum body experiences. A common theme that emerges from the qualitative literature is the idea that women believe they do not have an excuse for retaining their pregnancy weight and shape once they are no longer pregnant—often referred to as “bouncing” back to their prepregnancy body (Earle 2003; Patel et al. 2005; Clark et al. 2009a). The majority of women described their struggle to return to their prepregnancy weight as more negative than they expected (Clark et al. 2009a). For some women, this distress was exacerbated by the fact that they no longer seemed outwardly pregnant to observers, which led to body dissatisfaction (Clark et al. 2009a; Mills et al. 2013). Feelings of loss and hopelessness surrounding the idea that they lost their prepregnant bodies and would never regain that shape or weight were strong in some women (Patel et al. 2005). Other women began planning how they would return to their prepregnancy weight after giving birth while they were still pregnant (Earle 2003) which led to feelings of anticipatory anxiety (Harper and Rail 2011).
Although pregnant women seem more tolerant of their body changes because of the understanding that their body is serving the function of growing their child (Clark et al. 2009a), postpartum women do not appear to be as accepting of body changes. Soon after giving birth, women returned to their prepregnancy beliefs about their appearance and began prioritizing the esthetics of their body over the function (Watson et al. 2015). Additionally, quantitative data indicate the importance of shape and weight increases for women during the postpartum period (Clark et al. 2009b) and that women have unrealistic expectations about their weight following birth (participants under-predicted how much weight they would retain postnatally; Jenkin and Tiggemann 1997).
Psychosocial frameworks for postpartum-specific factors associated with eating disorder symptoms
Taken together, quantitative and qualitative data suggest there may be some postpartum-specific factors to consider when applying psychosocial frameworks to eating disorder risk during this period (e.g., objectification of a woman’s postpartum body esthetic as more important than her postpartum body function, sociocultural pressure to “bounce back” and lose pregnancy weight, and self-oriented body comparison towards one’s prepregnant self).
Objectification theory
Objectification theory posits that women are socialized to view their body as a sexual item to be objectified by outside observers (Fredrickson and Roberts 1997). Fredrickson and Roberts (1997) argue that this socialization teaches women to prioritize the appearance of their body over its functionality and leads to an array of mental health concerns including depression, anxiety, and eating disorders. However, the perinatal period is a time during which women struggle with this hierarchy because the function of their body being pregnant contravenes the thin ideal beauty standard (Watson et al. 2016). Qualitative literature indicate that some women recognize their body changes are a result of the pregnancy and may be more tolerant of these changes or have more self-compassion during this time, because they believe it is more important for their body to serve its function during pregnancy than to focus on esthetics (Earle 2003; Clark et al. 2009a; Harper and Rail 2011; Nash 2012). According to Lemberg and Phillips (1989), women with anorexia nervosa or bulimia nervosa experienced remission of their eating disorder symptoms because women reported feeling they had an “excuse” to eat and take care of their bodies due to the pregnancy. However, this belief appears to change during the postpartum period when women describe their concerns that they do not have an excuse for retaining their pregnancy weight and shape once they are no longer pregnant (Earle 2003; Patel et al. 2005; Clark et al. 2009a). Although it has not been evaluated quantitatively, it is possible that this inversion of the esthetic-function hierarchy during pregnancy, followed by the adoption of the esthetic over function belief during the postpartum period (see Fig. 1), may help explain why some women experience a reduction of eating disorder symptoms when pregnant, followed by an increase in symptoms during the postpartum period.

Proposed hierarchy of importance of women’s bodies during the perinatal period adapted from Objectification Theory (Fredrickson and Roberts 1997). During pregnancy, women prioritize the function of their body over the esthetic of their body which may serve as a buffer to reduce eating disorder symptoms. However, the hierarchy reverses during the postpartum period when women instead prioritize the esthetic of their body which may help explain the resurgence of eating disorder symptoms women experience during the postpartum period
The tripartite model of body image and eating disturbance
The tripartite influence model of body image and eating disturbances (Thompson et al. 1999) theorizes that body image and disordered eating are influenced by three primary sociocultural factors (the media, peers, and family) and that these associations are mediated by two psychological factors (thin ideal internalization and social comparison). Support for this model has been evaluated across diverse populations and during different developmental periods (Huxley et al. 2015; Papp et al. 2013; Rodgers et al. 2011; Yamamiya et al. 2008); however no data have examined it among women during the postpartum period (see Fig. 2).

Tripartite Model of Body Image and Eating Disturbance (a) as depicted Keery et al. (2004) and (b) adapted to include postpartum-specific factors including pressure to “bounce back” to pre-pregnancy body shape and weight, and self-oriented body comparison
Thin ideal internalization refers to the degree to which an individual ascribes to certain sociocultural standards of beauty and thinness (Schaefer et al. 2015). Western culture upholds a thin or slender body shape with minimal body fat as the ideal body standard for women (Ahern et al. 2008). Prospective studies consistently find thin ideal internalization predicts increases in body dissatisfaction, dietary restriction, and negative affect over time (see Stice 2002 for review).
Both qualitative and quantitative studies show some women ascribe less stringently to these ideals during pregnancy compared with prepregnancy (Rallis et al. 2007; Watson et al. 2015); however qualitative studies suggest women are quick to switch back to their prepregnancy ideals of beauty standards during the postpartum period (Earle 2003; Clark et al. 2009a). To date, no studies have evaluated thin ideal internalization during the postpartum period; what little is known comes from qualitative interviews about women’s perceptions of their ideal body. Given the robust research supporting thin ideal internalization as a salient risk factor for disordered eating and body image concerns (Stice 2002; Schaefer et al. 2015) and the pattern of distress from internalizing changing beauty ideals during the postpartum period from qualitative data (Earle 2003; Clark et al. 2009a; Harper and Rail 2011), it is clear that thin ideal internalization is a risk factor for eating disorder symptoms during the postpartum period that necessitates quantitative evaluation.
According to the tripartite influence model, three primary sociocultural sources (peers, family, and the media) can influence body image and disordered eating by acting as a source of (primarily appearance-related) pressure (Thompson et al. 1999). No data exist identifying specific sources of appearance-related pressures among postpartum women; however a content analysis of images of pregnant and postpartum celebrities in magazines found that pregnancy-related weight gain was more than three times as likely to be described as negative compared with positive (Gow 2012). More than 40% of postpartum celebrities discussed meeting their goal weight loss after having their baby, only 6% of postpartum celebrities admitted to being dissatisfied with their postpartum bodies, and more than 94% of postpartum celebrities expressed positive affect towards their body changes (Gow 2012). These media-controlled experiences are in contrast to the approximately 48% of community-sampled women who report feeling dissatisfied and distressed about their postpartum body (Walker 1998). A theme of the qualitative literature is the surprise and frustration postpartum women describe when they do not lose weight like they expected they would (see Watson et al. 2015 review), yet it is still unknown (1) if women are aware of these media messages and (2) if the messages affect women’s expectancies or eating disorder symptoms. Understanding the impact of the discrepancy between the messages in the media about postpartum weight loss and the experiences of women is a gap in the current literature. It is likely the media is a potent source of influence for many postpartum women.
Family, particularly one’s significant other, may be another influential source of pressure for women during the postpartum period. Nearly one-third of women who experience an eating disorder after their pregnancy report that criticism about their postpartum weight or shape from their significant other contributed to their eating disorder (Tiller and Treasure 1998). For example, one woman described how her husband patted her stomach after she gave birth and told her “now you can get rid of this” in reference to her pregnant weight and shape (Tiller and Treasure 1998, p. 182). Therefore, it is possible a woman’s significant other could be another influential source of pressure during the postpartum period.
In general, two of the more frequently studied types of appearance-related pressures are pressure to be thin or lose weight (Cashel et al. 2003; Stice 2002; Thompson et al. 2017; van den Berg et al. 2007) and weight-related teasing (Benas et al. 2010; Eisenberg et al. 2012, 2006; Goldschmidt et al. 2015; Neumark-Sztainer et al. 2002). Qualitative data suggest postpartum women experience pressures to lose their pregnancy weight (Clark et al. 2009a), yet no quantitative evaluations have studied it or weight-related teasing.
Further missing from consideration are pressures that may be unique to women who have recently given birth. For example, qualitative interviews suggest women may feel pressure that they are responsible for controlling their body weight postpartum (Upton and Han 2003; Clark et al. 2009a; Carter 2010) or that they should lose weight quickly (Clark et al. 2009a; Hodgkinson et al. 2014). Other appearance-related pressures that may be unique to the postpartum period could include pressure to breastfeed and to hide or decrease stretch marks or pressure to exercise (despite being advised against it during the immediate period following birth). Research is needed to identify these pressures and to understand how they may be linked to eating disorder symptoms.
Social comparison theory
Social comparison theory posits that individuals make judgments about their own attributes by comparing themselves to others (Festinger 1954). Evidence suggests that one type of social comparison that is particularly salient among individuals with eating disorder symptoms is body comparison—comparing perceptions about one’s body and physical appearance to others (van den Berg et al. 2007). Body comparison is associated with body dissatisfaction in cross-sectional (Trottier et al. 2007; Fitzsimmons-Craft et al. 2012), longitudinal (Fitzsimmons-Craft and Bardone-Cone 2014), and experimental (Lin and Kulik 2002; Krones et al. 2005) studies. Additionally, body comparison has also been linked with other eating disorder symptoms including dietary restriction and a drive for thinness (Lin and Soby 2016).
Traditional measures of body comparison orient the reader to compare themselves to a source that is external to themselves, most commonly to their peers, celebrities, or figures in the media (Thompson et al. 2004; Fitzsimmons-Craft et al. 2012; Schaefer and Thompson 2014). However, given women’s focus on their prepregnancy bodies during the postpartum period (Upton and Han 2003; Hodgkinson et al. 2014), it is possible that women make comparisons to their own prepregnancy body. In addition to judging their body in comparison with external sources, perhaps postpartum women judge their body in comparison with their younger selves before they conceived. No existing measures consider this idea of self-oriented body comparison, particularly during the postpartum period, which presents a void in the literature. To date, only one study has evaluated body comparison among postpartum women and found that body comparison at 6 weeks postpartum was associated with body dissatisfaction and feeling fat at 12 months postpartum (Rallis et al. 2007); however, these results were correlational and did not assess the type of comparison made (to self, peers, media, family, etc.). Considering the postpartum period presents unique psychological challenges for mothers (Wisner et al. 2008), research should consider psychological risk factors for eating disorder symptoms (like self-oriented body comparison; see Fig. 2) that may be distinctive to this period.
Limitations of current research and future directions
There are several broad limitations of the current literature that warrant discussion. First, measures used for assessing eating disorder symptoms during the postpartum period are not validated for use within this population (Walker et al. 2015). Only one measure of disordered eating behaviors has been validated for postpartum women in the USA—the Eating Stimulus Index (ESI; Cahill et al. 2009). Some studies create their own measures using a single item (Baker et al. 1999; Berg et al. 2011), while others use traditional measures that are validated for other samples, yet may not be appropriate for pregnant or postpartum women (Cashel et al. 2003; Birkeland et al. 2005; Rallis et al. 2007; Clark et al. 2009b; Easter et al. 2015).
An exploratory factor analysis of items from the Eating Disorder Examination Questionnaire (EDE-Q), a commonly used measure of eating disorder symptoms including weight and shape concern, dietary restriction, and binge eating (Luce and Crowther 1999), found an optimized version of the measure removed several items (e.g., questions concerning a flat stomach, fear of weight gain, desire for an empty stomach, and the importance of weight) for use among postpartum samples (Pettersson et al. 2016).
Similarly, the Body Attitudes Questionnaire (BAQ; Ben-Tovim and Walker 1991), which measures feeling fat, strength and fitness, salience of weight and shape, and attractiveness, has been used within community samples of pregnant or postpartum women (Rallis et al. 2007; Clark et al. 2009b). However, analyses reveal differential measurement biases between pregnant and nonpregnant women when using this measure (Fuller-Tyszkiewicz et al. 2012). Measurement invariance tests revealed that pregnant women reported more extreme responses compared with nonpregnant women for some items, while for other items nonpregnant women reported more extreme responses compared with pregnant women. Currently, no body image scale has been validated for use with pregnant or postpartum women. The implications that existing measures and items may not appropriately capture the postpartum disordered eating experience is an important constraint that must be addressed to best understand this population.
A second general limitation of the current literature regarding psychosocial risk factors of postpartum eating disorder symptoms is the absence of quantitative data evaluating findings based on qualitative research. To date, only one quantitative study has explored psychosocial risk factors (e.g., desired weight loss and body surveillance; Rodgers et al. 2018a, b) for eating disorder symptoms during the postpartum period; all other studies exploring psychosocial risk factors during the postpartum period are of qualitative design only (Earle 2003; Clark et al. 2009a; Nash 2012; Watson et al. 2015). The qualitative literature has been instrumental in conceptualizing new frameworks of psychosocial risk factors for disordered eating behaviors and cognitions during the postpartum period. Yet, findings from the existing literature cannot be generalized to broader populations with the same confidence as conclusions from quantitative evaluations of specific hypotheses (Atieno 2009). Quantitative methods are needed to progress the field forward and better our understanding of risk factors for disordered eating behaviors and cognitions that may be unique to the postpartum period.
Implications for prevention and treatment
Despite the limitations in current research, several implications for prevention and treatment are worth noting. Healthcare providers including obstetricians/gynecologists, nurses, pediatricians, and general practitioners are vital for screening and identifying eating disorder symptoms during the postpartum period. Considering postpartum women have more contact with medical physicians than mental health providers (Astrachan-Fletcher et al. 2008), training medical health providers on how to screen and to identify eating disorder symptoms and potential postpartum-specific risk factors, in addition to how to provide appropriate referrals when necessary, is the first step towards prevention and treatment.
Given the pattern of research indicating an increase in eating disorder symptoms during the postpartum period, and the serious mental health consequences of postpartum eating disorder symptoms including postpartum depression (Green et al. 2006; Hartley et al. 2018), screening for disordered eating behaviors and cognitions should be routine in postpartum health clinics. Validated assessments should assess for a variety of disordered eating behaviors (e.g., binge eating, restrictive dieting, emotional eating) and eating disorder cognitions (e.g., body image, weight and shape concern, importance of weight and shape to self-valuation).
It is important to note that prevention interventions targeting the potential resurgence of postpartum eating disorder symptoms may be particularly important to develop during pregnancy, given evidence that eating disorder symptoms may decline during pregnancy (Lacey and Smith 1987; Bonne et al. 1996; Morgan et al. 1999; Crow et al. 2008). Pregnancy could present a key window in which clinicians may be able to intervene to prevent the resurgence of these symptoms postpartum. Although further quantitative research is needed, early qualitative research suggests that prevention programs that emphasize psychoeducation about types and expected duration of body changes and their function in the postpartum period may be effective (Earle 2003; Clark et al. 2009a). To date, no existing prevention programs currently target postpartum eating disorder symptoms; however, acceptance and commitment-based programs like BodiMojo, which emphasize mindfulness, self-compassion, and media literacy, (sociocultural pressures and beauty ideals) may be effective in preventing body image and disordered eating if adapted for perinatal women (Rodgers et al. 2018a).
Conclusions
In conclusion, the purpose of this review was to (1) review existing literature regarding the developmental trajectory of eating disorder symptoms during pregnancy and the postpartum period, (2) discuss an application of three psychosocial models of eating disorder risk to the postpartum period by identifying unique postpartum-specific factors to consider, and (3) highlight limitations of the current literature and propose new directions for future research. This is the first review to apply psychosocial models of eating disorder risk to the postpartum period and to discuss novel postpartum-specific factors that have not been previously studied. Findings from prior data indicate that many commonly used measures of eating disorder symptoms may not be psychometrically valid for use during the postpartum period. Future research is needed to quantitatively evaluate the validity and reliability of assessments for the postpartum period, as well as potential postpartum-specific psychosocial factors associated with eating disorder symptoms, in order to better understand this understudied and vulnerable period.
References
Ahern AL, Bennet KM, Hetherington MM (2008) Internalization of the ultra-thin ideal: positive implicit associations with underweight fashion models are associated with drive for thinness in young women. Eat Disord 16:294–307. https://doi.org/10.1080/10640260802115852
Ashley-Martin J, Woolcott C (2014) Gestational weight gain and postpartum weight retention in a cohort of Nova Scotian women. Matern Child Health J 18:1927–1935. https://doi.org/10.1007/s10995-014-1438-7
Astrachan-Fletcher E, Veldhuis C, Lively N, Fowler C, Marcks B (2008) The reciprocal effects of eating disorders and the postpartum period: a review of the literature and recommendations for clinical care. J Women's Health 17:227–239. https://doi.org/10.1089/jwh.2007.0550
Atieno OP (2009) An analysis of the strengths and limitation of qualitative and quantitative research paradigms. Probl Educ 21st Century 13:13–18
Baker CW, Carter AS, Cohen LR, Brownell KD (1999) Eating attitudes and behaviors in pregnancy and postpartum: global stability versus specific transitions. Ann Behav Med 21:143–148. https://doi.org/10.1007/BF02908295
Benas JS, Uhrlass DJ, Gibb BE (2010) Body dissatisfaction and weight-related teasing: a model of cognitive vulnerability to depression among women. J Behav Ther Exp Psychiatry 41:352–356. https://doi.org/10.1016/j.jbtep.2010.03.006
Ben-Tovim DI, Walker MK (1991) The development of the Ben-Tovim Walker body attitudes questionnaire (BAQ), a new measure of women’s attitudes towards their own bodies. Psychol Med 21:775–784. https://doi.org/10.1017/S0033291700022406
Berg CK, Torgersen L, Von Holle A et al (2011) Factors associated with binge eating disorder in pregnancy. Int J Eat Disord 44:124–133
Birkeland R, Thompson JK, Phares V (2005) Adolescent motherhood and postpartum depression. J Clin Child Adolesc Psychol 53(34):292–300. https://doi.org/10.1207/s15374424jccp3402_8
Blais MA, Becker AE, Burwell RA, Flores AT, Nussbaum KM, Greenwood DN, Ekeblad ER, Herzog DB (2000) Pregnancy: outcome and impact on symptomatology in a cohort of eating-disordered women. Int J Eat Disord 27:140–149. https://doi.org/10.1002/(SICI)1098-108X(200003)27:2<140::AID-EAT2>3.0.CO;2-E
Bonne OB, Rubinoff B, Berry EM (1996) Delayed detection of pregnancy in patients with anorexia nervosa: two case reports. Int J Eat Disord 20:423–425. https://doi.org/10.1002/(SICI)1098-108X(199612)20:4<423::AID-EAT10>3.0.CO;2-Z
Cahill JM, Freeland-Graves JH, Shah BS, Lu H, Klohe-Lehman DM (2009) Development and validation of the eating stimulus index in low-income, minority women in early postpartum. J Am Diet Assoc 109:1593–1598. https://doi.org/10.1016/j.jada.2009.06.364
Carter SK (2010) Beyond control: body and self in women’s childbearing narratives. Sociol Health Illn 32:993–1009. https://doi.org/10.1111/j.1467-9566.2010.01261.x
Cashel ML, Cunningham D, Landeros C, Cokley KO, Muhammad G (2003) Sociocultural attitudes and symptoms of bulimia: evaluating the SATAQ with diverse college groups. J Couns Psychol 50:287–296. https://doi.org/10.1037/0022-0167.50.3.287
Clark A, Skouteris H, Wertheim EH, Paxton SJ, Milgrom J (2009a) My baby body: a qualitative insight into women’s body-related experiences and mood during pregnancy and the postpartum. J Reprod Infant Psychol 27:330–345. https://doi.org/10.1080/02646830903190904
Clark A, Skouteris H, Wertheim EH, Paxton SJ, Milgrom J (2009b) The relationship between depression and body dissatisfaction across pregnancy and the postpartum: a prospective study. J Health Psychol 14:27–35. https://doi.org/10.1177/1359105308097940
Coker EL, Abraham S (2015) Body weight dissatisfaction before, during and after pregnancy: a comparison of women with and without eating disorders. Eat Weight Disord 20:71–79. https://doi.org/10.1007/s40519-014-0133-4
Coker EL, Mitchell-Wong LA, Abraham SF (2013) Is pregnancy a trigger for recovery from an eating disorder? Acta Obstet Gynecol Scand 92:1407–1413. https://doi.org/10.1111/aogs.12256
Crow SJ, Agras WS, Crosby R, Halmi K, Mitchell JE (2008) Eating disorder symptoms in pregnancy: a prospective study. Int J Eat Disord 41:277–279. https://doi.org/10.1002/eat.20496
Earle S (2003) “Bumps and boobs”: fatness and women’s experiences of pregnancy. Womens Stud Int Forum 26:245–252. https://doi.org/10.1016/S0277-5395(03)00054-2
Easter A, Solmi F, Bye A, Taborelli E, Corfield F, Schmidt U, Treasure J, Micali N (2015) Antenatal and postnatal psychopathology among women with current and past eating disorders: longitudinal patterns. Eur Eat Disord Rev 23:19–27. https://doi.org/10.1002/erv.2328
Eisenberg ME, Neumark-Sztainer D, Haines J, Wall M (2006) Weight-teasing and emotional well-being in adolescents: longitudinal findings from project EAT. J Adolesc Health 38:675–683. https://doi.org/10.1016/j.jadohealth.2005.07.002
Eisenberg M, Berge JM, Neumark-Sztainer D (2012) Associations between hurtful weight-related comments by family and significant other and the development of disordered eating behaviors in young adults. J Behav Med 35:500–508. https://doi.org/10.1007/s10865-011-9378-9
Festinger L (1954) A theory of social comparison processes. Hum Relat 7:117–140. https://doi.org/10.1177/001872675400700202
Fitzsimmons-Craft EE (2011) Social psychological theories of disordered eating in college women: review and integration. Clin Psychol Rev 31:1224–1237. https://doi.org/10.1016/j.cpr.2011.07.011
Fitzsimmons-Craft EE, Bardone-Cone AM (2014) One-year temporal stability and predictive and incremental validity of the body, eating, and exercise comparison orientation measure (BEECOM) among college women. Body Image 11:27–35. https://doi.org/10.1016/j.bodyim.2013.09.003
Fitzsimmons-Craft EE, Bardone-Cone AM, Harney MB (2012) Development and validation of the body, eating, and exercise comparison orientation measure (BEECOM) among college women. Body Image 9:476–487. https://doi.org/10.1016/j.bodyim.2012.07.007
Fredrickson BL, Roberts TA (1997) Objectification theory: toward understanding women’s lived experiences and mental health risks. Psychol Women Q 21:173–206
Fuller-Tyszkiewicz M, Skouteris H, Watson B, Hill B (2012) Body image during pregnancy: an evaluation of the suitability of the body attitudes questionnaire. BMC Pregnancy Childbirth 12:91. https://doi.org/10.1186/1471-2393-12-91
Goldschmidt AB, Wall MM, Loth KA, Neumark-Sztainer D (2015) Risk factors for disordered eating in overweight adolescents and young adults. J Pediatr Psychol 40:1048–1055
Gow RW (2012) Representations of celebrities’ weight and shape during pregnancy and postpartum: a content analysis of three entertainment magazine websites. Body Image 9:172–175
Green K, Broome H, Mirabella J (2006) Postnatal depression among mothers in the United Arab Emirates: socio-cultural and physical factors. Psychol Health Med 11:425–431. https://doi.org/10.1080/13548500600678164
Harper EA, Rail G (2011) Contesting “silhouettes of a pregnant belly”: young pregnant women’s discursive constructions of the body. Aporia 3:5–14
Hartley E, Hill B, Bailey C, Fuller-Tyszkiewicz M, Skouteris H (2018) The associations of weight status and body attitudes with depressive and anxiety symptoms across the first year postpartum. Womens Health Issues 28:530–538. https://doi.org/10.1016/j.whi.2018.07.002
Hawkins LK, Gottlieb BR (2013) Screening for eating disorders in pregnancy: how uniform screening during a high-risk period could minimize under-recognition. J Women's Health 22:390–392. https://doi.org/10.1089/jwh.2013.4313
Heinberg LJ, Guarda AS (2002) Body image in obstetrics and gynecology. In: Body image. The Guilford Press, New York, pp 351–360
Hodgkinson EL, Smith DM, Wittkowski A (2014) Women’s experiences of their pregnancy and postpartum body image: a systematic review and meta-synthesis. BMC Pregnancy Childbirth 14:1–11. https://doi.org/10.1186/1471-2393-14-330
Huxley CJ, Halliwell E, Clarke V (2015) An examination of the tripartite influence model of body image: does Women’s sexual identity make a difference? Psychol Women Q 39:337–348. https://doi.org/10.1177/0361684314554917
Institute of Medicine (2007) Influence of pregnancy weight on maternal and child health: workshop report. National Academies Press
Jenkin W, Tiggemann M (1997) Psychological effects of weight retained after pregnancy. Women Health 25:89–98. https://doi.org/10.1300/J013v25n01_06
Keery H, van den Berg P, Thompson K (2004) An evaluation of the tripartite influence model of body dissatisfaction and eating disturbance with adolescent girls. Body Image 1:237–251. https://doi.org/10.1016/j.bodyim.2004.03.001
Knoph C, Von Holle A, Zerwas S et al (2013) Course and predictors of maternal eating disorders in the postpartum period. Int J Eat Disord 46:355–368. https://doi.org/10.1002/eat.22088
Krones PG, Stice E, Batres C, Orjada K (2005) In vivo social comparison to a thin-ideal peer promotes body dissatisfaction: a randomized experiment. Int J Eat Disord 38:134–142. https://doi.org/10.1002/eat.20171
Lacey JH, Smith G (1987) Bulimia nervosa. The impact of pregnancy on mother and baby. Br J Psychiatry J Ment Sci 150:777–781
Larsson G, Andersson-Ellström A (2003) Experiences of pregnancy-related body shape changes and of breast-feeding in women with a history of eating disorders. Eur Eat Disord Rev 11:116–124. https://doi.org/10.1002/erv.497
Lemberg R, Phillips J (1989) The impact of pregnancy on anorexia nervosa and bulimia. Int J Eat Disord 8:285–295. https://doi.org/10.1002/1098-108X(198905)8:3<285::AID-EAT2260080304>3.0.CO;2-P
Lin LF, Kulik JA (2002) Social comparison and women’s body satisfaction. Basic Appl Soc Psychol 24:115–123. https://doi.org/10.1207/S15324834BASP2402_4
Lin L, Soby M (2016) Appearance comparisons styles and eating disordered symptoms in women. Eat Behav 23:7–12. https://doi.org/10.1016/j.eatbeh.2016.06.006
Luce KH, Crowther JH (1999) The reliability of the eating disorder examination—self-report questionnaire version (EDE-Q). Int J Eat Disord 25:349–351. https://doi.org/10.1002/(SICI)1098-108X(199904)25:3<349::AID-EAT15>3.0.CO;2-M
Mills A, Schmied V, Dahlen HG (2013) “Get alongside us”, women’s experiences of being overweight and pregnant in Sydney, Australia. Matern Child Nutr 9:309–321. https://doi.org/10.1111/j.1740-8709.2011.00386.x
Morgan JF, Lacey JH, Sedgwick PM (1999) Impact of pregnancy on bulimia nervosa. Br J Psychiatry 174:135–140. https://doi.org/10.1192/bjp.174.2.135
Nash M (2012) Weighty matters: negotiating ‘fatness’ and ‘in-betweenness’ in early pregnancy. Fem Psychol 22:307–323. https://doi.org/10.1177/0959353512445361
Neumark-Sztainer D, Falkner N, Story M et al (2002) Weight-teasing among adolescents: correlates with weight status and disordered eating behaviors. Int J Obes 26:123–131. https://doi.org/10.1038/sj.ijo.0801853
Nunes MA, Pinheiro AP, Hoffmann JF, Schmidt MI (2014) Eating disorders symptoms in pregnancy and postpartum: a prospective study in a disadvantaged population in Brazil. Int J Eat Disord 47:426–430. https://doi.org/10.1002/eat.22236
Papp I, Urban R, Czegledi E et al (2013) Testing the tripartite influence model of body image and eating disturbance among Hungarian adolescents. Body Image 10:232–242
Patel P, Lee J, Wheatcroft R, Barnes J, Stein A (2005) Concerns about body shape and weight in the postpartum period and their relation to women’s self-identification. J Reprod Infant Psychol 23:347–364. https://doi.org/10.1080/02646830500273657
Pettersson CB, Zandian M, Clinton D (2016) Eating disorder symptoms pre- and postpartum. Arch Womens Ment Health 19:675–680. https://doi.org/10.1007/s00737-016-0619-3
Rallis S, Skouteris H, Wertheim EH, Paxton SJ (2007) Predictors of body image during the first year postpartum: a prospective study. Women Health 45:87–104. https://doi.org/10.1300/J013v45n01_06
Rodgers R, Chabrol H, Paxton S (2011) An exploration of the tripartite influence model of body dissatisfaction and disordered eating among Australian and French college women. Body Image 8:208–215
Rodgers RF, Paxton SJ, McLean SA (2014) A biopsychosocial model of body image concerns and disordered eating in early adolescent girls. J Youth Adolesc 43:814–823. https://doi.org/10.1007/s10964-013-0013-7
Rodgers RF, Donovan E, Cousineau T, Yates K, McGowan K, Cook E, Lowy AS, Franko DL (2018a) BodiMojo: efficacy of a mobile-based intervention in improving body image and self-compassion among adolescents. J Youth Adolesc 47:1363–1372. https://doi.org/10.1007/s10964-017-0804-3
Rodgers RF, O’Flynn JL, Bourdeau A, Zimmerman E (2018b) A biopsychosocial model of body image, disordered eating, and breastfeeding among postpartum women. Appetite 126:163–168. https://doi.org/10.1016/j.appet.2018.04.007
Schaefer LM, Thompson JK (2014) The development and validation of the physical appearance comparison scale-revised (PACS-R). Eat Behav 15:209–217. https://doi.org/10.1016/j.eatbeh.2014.01.001
Schaefer LM, Burke NL, Thompson JK, Dedrick RF, Heinberg LJ, Calogero RM, Bardone-Cone AM, Higgins MK, Frederick DA, Kelly M, Anderson DA, Schaumberg K, Nerini A, Stefanile C, Dittmar H, Clark E, Adams Z, Macwana S, Klump KL, Vercellone AC, Paxton SJ, Swami V (2015) Development and validation of the sociocultural attitudes towards appearance Questionnaire-4 (SATAQ-4). Psychol Assess 27:54–67. https://doi.org/10.1037/a0037917
Shloim N, Hetherington MM, Rudolf M, Feltbower RG (2015) Relationship between body mass index and women’s body image, self-esteem and eating behaviours in pregnancy: a cross-cultural study. J Health Psychol 20:413–426. https://doi.org/10.1177/1359105313502568
Shrewsbury VA, Robb KA, Power C, Wardle J (2009) Socioeconomic differences in weight retention, weight-related attitudes and practices in postpartum women. Matern Child Health J 13:231–240. https://doi.org/10.1007/s10995-008-0342-4
Stice E (2002) Risk and maintenance factors for eating pathology: a meta-analytic review. Psychol Bull 28:825–848. https://doi.org/10.1037/0033-2909.128.5.825
Thompson JK, Heinberg LJ, Altabe M, Tantleff-Dunn D (1999) Exacting beauty: theory, assessment, and treatment of body image disturbance. American Psychological Association, Washington, DC
Thompson JK, van den Berg P, Roehrig M, Guarda AS, Heinberg LJ (2004) The sociocultural attitudes towards appearance scale (SATAQ-3): development and validation. Int J Eat Dis 35:293–304
Thompson KA, Kelly NR, Schvey NA, Brady SM, Courville AB, Tanofsky-Kraff M, Yanovski SZ, Yanovski JA, Shomaker LB (2017) Internalization of appearance ideals mediates the relationship between appearance-related pressures from peers and emotional eating among adolescent boys and girls. Eat Behav 24:66–73. https://doi.org/10.1016/j.eatbeh.2016.12.008
Tiller J, Treasure J (1998) Eating disorders precipitated by pregnancy. Eur Eat Disord Rev 6:178–187. https://doi.org/10.1002/(SICI)1099-0968(199809)6:3<178::AID-ERV231>3.0.CO;2-Y
Trottier K, Polivy J, Herman CP (2007) Effects of exposure to thin and overweight peers: evidence of social comparison in restrained and unrestrained eaters. J Soc Clin Psychol 26:155–172. https://doi.org/10.1521/jscp.2007.26.2.155
Upton RL, Han SS (2003) Maternity and its discontents: “getting the body Back” after pregnancy. J Contemp Ethnogr 32:670–692. https://doi.org/10.1177/0891241603257596
van den Berg P, Paxton SJ, Keery H, Wall M, Guo J, Neumark-Sztainer D (2007) Body dissatisfaction and body comparison with media images in males and females. Body Image 4:257–268. https://doi.org/10.1016/j.bodyim.2007.04.003
Walker L (1998) Weight-related distress in the early months after childbirth. West J Nurs Res 20:30–44. https://doi.org/10.1177/019394599802000103
Walker LO, Gao J, Xie B (2015) Postpartum psychosocial and behavioral health: a systematic review of self-administered scales validated for postpartum women in the United States. Womens Health Issues 25:586–600. https://doi.org/10.1016/j.whi.2015.05.006
Watson B, Fuller-Tyszkiewicz M, Broadbent J, Skouteris H (2015) The meaning of body image experiences during the perinatal period: a systematic review of the qualitative literature. Body Image 14:102–113. https://doi.org/10.1016/j.bodyim.2015.04.005
Watson B, Broadbent J, Skouteris H, Fuller-Tyszkiewicz M (2016) A qualitative exploration of body image experiences of women progressing through pregnancy. Women Birth J Aust Coll Midwives 29:72–79. https://doi.org/10.1016/j.wombi.2015.08.007
Wisner KL, Scholle SH, Stein B (2008) Perinatal disorders: advancing public health opportunities. J Clin Psychiatry 69:1602–1605. https://doi.org/10.4088/JCP.v69n1010
Yamamiya Y, Shroff H, Thompson JK (2008) The tripartite influence model of body image and eating disturbance: a replication with a Japanese sample. Int J Eat Disord 41:88–91
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Thompson, K. An application of psychosocial frameworks for eating disorder risk during the postpartum period: A review and future directions. Arch Womens Ment Health 23, 625–633 (2020). https://doi.org/10.1007/s00737-020-01049-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00737-020-01049-5