
Abstract
Preterm delivery can precipitate maternal psychological morbidities. Family Nurture Intervention (FNI) was designed to minimize these by facilitating the emotional connection between mother and infant, beginning early in the infant’s neonatal intensive care unit (NICU) stay. We examined depression and anxiety symptoms of mothers of preterm infants at 4 months infant corrected age (CA). One hundred fifteen mothers who delivered between 26 and 34 weeks gestational age were randomized to receive standard care (SC) or standard care plus FNI. Mothers’ self-reported depressive symptoms (Center for Epidemiologic Studies Depression Scale: CES-D) and state anxiety (Spielberger State-Trait Anxiety Inventory: STAI) symptoms were assessed at enrollment, near to term age, and 4 months (CA). At 4 months CA, mean CES-D and STAI scores were significantly lower in FNI mothers compared to SC mothers. Effectiveness of FNI can only be evaluated as an integrated intervention strategy as it was not possible to control all aspects of FNI activities. Although there was considerable loss to follow-up, analyses suggest that resulting biases could have masked rather than inflated the measured effect size for depressive symptoms. FNI may be a feasible and practicable way to diminish the impact of premature delivery on maternal depressive and anxiety symptoms.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prevalence of postpartum depression following a premature delivery has been estimated between 28 and 70 % (Davis et al. 2003; Miles et al. 2007; Younger et al. 1997). Anxiety symptoms are also elevated following premature delivery (Misund et al. 2013; Singer et al. 1999). Infants born prematurely can have prolonged hospitalization in the neonatal intensive care unit (NICU), and the resulting physical separation can adversely affect the emotional well-being of both mothers and infants (Aylward 2005; Moster et al. 2008). Symptoms of maternal depression and anxiety have been related to concerns about the infant’s appearance and condition (Singer et al. 1999), feelings of guilt about not carrying to term (Brett et al. 2011), and fears for the infant’s survival (Aagaard and Hall 2008; Cho et al. 2008; Johnson 2008). Additionally, women report decreased confidence in their role as mothers (Aagaard and Hall 2008; Woodward et al. 2014). These negative affective states can persist well beyond the time of the infant’s discharge home (Garel et al. 2007; Vigod et al. 2010) and have even been reported at 7 years following birth (Treyvaud et al. 2014).
In preterm infants, cognitive development and behavioral outcomes negatively correlate with maternal depression and anxiety (McManus and Poehlmann 2012; Zelkowitz et al. 2011). These conditions can be detrimental to the initiation of maternal behavior and the maintenance of dyadic relationships (Field 2010; Tietz et al. 2014). Depressed and anxious mothers have trouble interacting with and responding to cues from their preterm infants (Forcada-Guex et al. 2006). These mothers tend to be less sensitive and responsive, providing less language input and attention to their infants’ specific needs (Feeley et al. 2005; Korja et al. 2008; Zelkowitz et al. 2009). Early mother-infant interactions following term birth are critical factors in child development (Forcada-Guex et al. 2011; Hofer 1994; Meijssen et al. 2011) and are of great relevance for premature infants due to their increased vulnerability to cognitive, socio-emotional, and behavioral difficulties (Feeley et al. 2005; Landry et al. 2003). Enhanced sensitivity and responsiveness between mothers and preterm infants can lead to better long-term outcomes in cognitive and social development (Feeley et al. 2005; McManus and Poehlmann 2012; Poehlmann et al. 2012). Work by others suggests that promoting more optimal parent-infant interactions through an educational and behavioral intervention may lead to reductions in post-discharge maternal depression and anxiety (Melnyk et al. 2008). The current study tests another approach. Family Nurture Intervention (FNI), described previously (Welch et al. 2012), is based on animal and human research, which has identified key roles of olfactory, sensorimotor, and nurturing activities in the development of normal mother-infant relationships (Hofer 1975, 1994, 1996; Myers et al. 1989a, b). We have demonstrated that FNI is safe and feasible to implement in the NICU (Welch et al. 2013) and that electroencephalographic activity at term age is increased in infants who received FNI compared with those having standard NICU care (Welch et al. 2014). As compared with other interventions in this patient population, this is the first trial to assess the effects of facilitated affective communication between mother and infant using a randomized controlled trial design and which initiates mother-infant interactions early in the NICU stay while the infant is confined to the isolette and continues outside the isolette until discharge. The intervention was designed to support maternal and family emotional connections with their infant to promote physical, social, emotional, and cognitive development by nurture specialist-facilitated activities including odor cloth exchange, emotional speech and touch, and holding. Our hypothesis was that the intervention mothers would have lower levels of depressive and anxiety symptoms post-discharge than mothers in the standard care group.
Methods
Study design
A randomized controlled trial (RCT) was conducted with mothers of very preterm infants admitted to the level IV NICU at Morgan Stanley Children’s Hospital at Columbia University Medical Center. In an effort to minimize the effects of separation of mothers and their infants during this critical period, FNI was initiated as soon as clinically possible after birth (mean of 7 days) and continued for the duration of the infants’ hospitalization. Infants were enrolled from January 2009 through June 2012.
Mothers eligible for the RCT had recently delivered a singleton or a set of twins between 26 and 34 weeks gestational age (GA) who were free of congenital defects. Mothers were ≥18 years old; fluent in English; free of current or prior mental illness, addiction, or substance use; and had access to social support from at least one adult in the home. A total of N = 115 mothers of N = 150 infants were enrolled for prospective study and randomized to either FNI or standard care (SC). FNI nurture specialists worked with the (N = 59) FNI group mothers, their infants, and families to facilitate all aspects of the intervention, while the (N = 56) SC group mothers and infants received standard patient care during their NICU stay.
Written informed consent was obtained from mothers for their own and their infants’ participation. The study was approved by the Institutional Review Board of the Columbia University Medical Center, overseen by a Data Safety Monitoring Board and registered at ClinicalTrials.gov (#NCT01439269). FNI has been found to be safe and feasible (Welch et al. 2013) and to significantly increase frontal brain activity during sleep at term corrected age (CA) (Welch et al. 2014).
Intervention
FNI is based on the hypothesis that adverse consequences of prolonged separation of mother and infant following preterm birth can be ameliorated by a dyadic intervention comprising repeated experience with calming activities, as described previously (Welch et al. 2012). These activities occur during calming sessions that are facilitated by nurture specialists, former NICU nurses trained in implementing the FNI protocol. Calming session activities engage the mother and infant reciprocally in physical, sensory, and emotional experiences. Each session was comprised of as many of the calming procedures as possible. Prior to engaging in any of the FNI activities, mothers and family members were instructed in infection prevention procedures. Nurture specialists also involve and engage family members in reassuring and calming the mother and in providing continued support for her after discharge from the hospital. The FNI calming procedures were as follows.
Scent cloth exchange
Mothers were instructed to exchange special 12-by-16-in. cotton cloths with their infants on a daily basis. The mother’s scent cloth was worn close to her skin overnight and was placed with the infant each day; the infant’s scent cloth was placed in bed with the infant during the preceding 24 h and was taken home each day by the mother.
Calming touch
Mothers were shown how to calm their infants using firm sustained touch by placing both hands on the infant’s torso or by cupping one hand around the infants’ legs and feet and placing the other hand on the abdomen. While engaging in calming touch, the nurture specialist prompted the mother to communicate her thoughts and emotions to the infant in her native language. During all of these activities, the mother was encouraged to seek and maintain eye contact with her infant as much as possible.
Holding
When infants could be taken out of the incubator, the nurture specialists assisted the mother to engage in skin-to-skin or clothed calming sessions. Nurture specialists aimed to facilitate holding sessions at least four times per week; however, mothers were encouraged to engage in calming techniques at all of their visits.
Although feeding is a critical mother-infant interaction, feeding was not included as one of the facilitated mother-infant activities because the NICU employed a feeding specialist for all mothers. However, the nurture specialists encouraged mothers to feed, change, and bathe their infants. Fathers were also encouraged to engage in these activities.
Standard care
Mothers in the SC group followed hospital protocol. SC mothers were able to engage in nurturing activities of their choosing, which in this NICU included skin-to-skin or non-skin-to-skin holding. These activities of SC mothers were optional and not documented by the study staff; however, SC mothers recorded these activities on a self-report visit log.
Psychological evaluation
Maternal psychological variables were assessed via self-report. Standardized, validated instruments were completed by study participants at enrollment, near to term age, and at the infants’ 4-month CA follow-up visit.
The Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff 1977) was used to assess maternal depressive symptoms. Mothers selected responses from a Likert scale ranging from 0 (never) to 3 (almost always) for each of the 20 items representing various manifestations of depression, for a total scale score ranging from 0 to 60. A score equal to or greater than 16 is typically considered a criterion for referral (Radloff 1977). The CES-D has been widely used in epidemiological and social science research and demonstrates reliability and construct validity in evaluating depressive symptoms in adult populations, including among mothers during and after parturition (Ballantyne et al. 2013; Melchior et al. 2012; Miles et al. 2007; Phillips et al. 2010).
The Spielberger State-Trait Anxiety Inventory (STAI) (Spielberger et al. 1970) was used to assess maternal anxiety trait and state at enrollment and anxiety state at near to term age and 4 months CA. This instrument comprises two 20-item subscales, one for “State,” a transitory response to a temporary stressor, and one for “Trait,” a stable response style for approaching life stress. Item responses range from 1 to 4 representing low (1 = not at all) to high (4 = very much) state stress and rare (1 = almost never) to frequent (4 = almost always) trait stress, giving possible subscale scores between 20 and 80, following reverse coding. Construct validity has been demonstrated for the state anxiety subscale through concordance with the Anxiety Sensitivity Index (Peterson and Reiss 1987), while strong correlation with both the Anxiety Scale Questionnaire and Manifest Anxiety Scales (Tilton 2008) has provided evidence of concurrent validity for the trait anxiety subscale. This instrument has been successfully used among new mothers of both term and preterm infants (Brandon et al. 2011; Dayan et al. 2006; Kikkert et al. 2010; Neu et al. 2014). There is no standard cutoff for referral; however, we used a score of 30 as a threshold to signify elevated levels of anxiety.
Behavioral Inhibition System and Behavioral Activation System (BISBAS) (Carver 1994) scales were used to assess maternal motivation systems at enrollment. This 24-item Likert-style instrument assesses the activation systems of drive (4 items), fun seeking (4 items), and reward responsiveness (5 items) (BAS subscales), as well as the inhibitory system through a single 7-item BIS subscale (4 filler items are not used for scoring). The personality traits measured by this instrument are correlated with anxiety and hence possible predictors of maternal adaptation to and capacity to withstand the stresses associated with caring for a very preterm infant. These trait scores were also included as potential predictors of response to intervention. The BISBAS and trait STAI assessments were included to assess possible group differences in the mothers’ baseline psychological characteristics.
Data analyses
Using an intent-to-treat approach, comparisons were made between mothers assigned to the FNI group and those assigned to the SC group, irrespective of the frequency or duration of supported calming activity received. The FNI and SC groups were compared with respect to baseline demographic characteristics using Student’s t test for continuous measures and Pearson’s chi-squared or Fisher’s exact tests for discrete variables, as appropriate. Descriptive statistics were compiled for the dependent variables (CES-D; STAI), by study group and follow-up visit. Group mean depression and state anxiety scores were compared for all available respondents at enrollment, near to term age, and 4 months CA. Relationships between baseline and 4-month CES-D and STAI scores were assessed by Pearson correlations. Statistical analyses were conducted using SPSS Version 21.0 (IBM Corporation, Armonk, NY).
Results
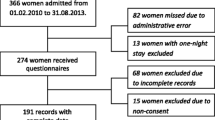
Randomization produced no significant differences between SC (N = 56) and FNI (N = 59) families with regard to mothers’ and fathers’ age, race/ethnicity, education, or household income at study entry (Table 1, Supplemental Table 1). Mean Spielberger trait anxiety and BISBAS scores at enrollment are presented by study group in Table 2. There were no significant differences in these psychological measures. By term age, N = 30 (26 %) families were no longer able to participate as a result of infants’ transfer to other facilities (SC: N = 4, 7 %; FNI: N = 4, 7 %), death (SC: N = 1, 1.8 %; FNI: N = 1, 1.7 %), withdrawal (SC: N = 0; FNI: N = 4, 7 %), or loss to follow-up (SC: N = 10, 18 %; FNI: N = 6, 11 %). By 4 months CA, an additional 2.6 % (SC: N = 1, 1.8 %; FNI: N = 2, 3.4 %) of recruits had been lost to follow-up (see Supplemental Figure 1). After these losses to follow-up, there were still no significant group differences in family demographics for mothers assessed when infants were near to term age (SC: N = 41; FNI: N = 44) or at 4 months CA (SC: N = 40; FNI: N = 42).
Similarly, infant clinical characteristics did not differ by group at enrollment (SC: N = 72; FNI: N = 78), near to term age (SC: N = 54; FNI: N = 57), or at 4 months CA (SC: N = 50; FNI: N = 52) (Table 1, Supplemental Tables 1 and 2). Across both study groups, families retained at 4 months were similar to the baseline cohort with respect to parental age, race/ethnicity, paternal education, and income, but mothers who presented with their infants for the 4-month assessment were significantly more likely to be married (χ 2 = 7.82; p = 0.005) and better educated (χ 2 = 8.28; p = 0.016) than mothers of infants who had transferred out, withdrawn, died, been lost to follow-up, or failed to attend the scheduled 4-month follow-up for reasons unknown to the investigators. Furthermore, infants whose mothers were not assessed at 4 months did not differ from those whose mothers were included in the present study with respect to assessed clinical characteristics (data not shown).
At enrollment, there were no significant differences in mean self-reported depressive symptoms between groups. However, at 4 months CA, average CES-D scores were significantly lower in FNI mothers (t = 2.12, p = 0.038) (Fig. 1a). Of the N = 108 mothers who completed the CES-D at baseline, 38.3 % (SC: N = 20, 36 %; FNI: N = 24, 45 %) rated themselves at or above a 16-point cutoff to indicate possible clinical depression (Radloff 1977). CES-D scores declined in both groups over time (see Fig. 1a), but group comparisons at each visit showed a progressive divergence in mean depression scores over the follow-up periods. By 4 months, eight mothers had scores that exceeded the 16-point depression cutoff; seven of these were in the SC group (17.5 %) whereas only one (2.5 %) was FNI (Fisher’s exact test p = 0.028).

a Mothers in the FNI group (shaded bars) had significantly reduced depressive symptoms compared with the SC group (open bars) at 4 months CA. b Mothers in the FNI group reported significantly fewer anxiety symptoms than those in the SC group at 4 months CA
As was the case for CES-D depressive symptom scores, mean state anxiety scores were significantly lower in FNI mothers at 4 months CA (t = 2.79, p = 0.004); whereas at baseline, neither the current state nor the more stable trait anxiety scores differed by group (see Fig. 1b). At baseline, 57 % of SC mothers and 53 % of FNI mothers reported trait anxiety scores greater than 30 (ns). Also at baseline, 70 % of SC mothers and 71 % of FNI mothers reported state anxiety scores greater than 30 (ns). At baseline, 36 % of SC mothers and 43 % of FNI mothers had CES-D scores greater than 15 (ns). At the near to term age evaluations, the percentage of women with state anxiety scores above 30 had declined from 70 to 59 % of SC and from 71 to 41 % of FNI mothers; this group difference approached significance (χ 2 = 2.64, p = 0.10). Similarly, the percentage of women with CES-D scores greater than 15 had declined from enrollment to term age from 36 to 17 % for SC and from 43 to 9 % for FNI; but the group difference at term age was not statistically significant. However, by the time of the 4-month CA follow-up visit, the percentage of SC mothers reporting state anxiety greater than 30 (53 %) was significantly higher than that for FNI mothers (26 %; χ 2 = 5.96; p = 0.015). At 4 months, 18 % of SC mothers reported CES-D depressive symptoms greater than 15 while only 3 % of FNI mothers exceeded this threshold (χ 2 = 5.00; p = 0.025).
In additional analyses, STAI state anxiety scores for both groups were found to be strongly correlated with CES-D scores at baseline (r (df = 106) = 0.74, p < 0.001) and at 4 months (r (df = 78) = 0.67, p < 0.001). As shown in Fig. 2, within-group correlations were highly significant for both SC and FNI (r (df = 38) = 0.65, p < 0.001 and r (df = 38) = 0.68, p < 0.001, respectively) at the 4-month visit. Inspection of this figure reveals that 7 of the mothers had CES-D scores at or above 16 and state anxiety levels at or above 30; 6 of these were in the SC group. Moreover, at 4 months, 72.5 % (N = 29) of FNI mothers reported both CES-D and STAI state anxiety levels below these cutoffs whereas only 42.5 % (N = 17) of SC mothers were within this lower depressive symptom and anxiety symptom range (χ 2 = 7.37, p = 0.007).

STAI state scores were strongly correlated with CES-D scores at 4 months CA in both SC (green circles) and FNI (purple squares) mothers. Group cutoff scores for depressive and anxiety symptoms are indicated by the solid red lines. Note that predominantly SC mothers are represented in the upper right quadrant of mothers having high levels of depression and anxiety symptoms (six of seven)
In the SC group, 28.6 % of the mothers were recorded as attempting to breastfeed at least one time as compared to 37.5 % of the FNI mothers (χ 2 = 1.02, p = 0.32). Moreover, there was no significant main effect of breastfeeding (Y/N) nor a significant interaction between breastfeeding and the intervention group with regard to 4-month CES-D (p = 0.13, p = 0.24) or STAI (p = 0.24, p = 0.94) levels. Similarly, CES-D and STAI scores were decreased by FNI at 4 months, controlling for twin status (p < 0.04 and p < 0.02, respectively).
Skin-to-skin holding was encouraged in the FNI group, and we reported previously (Welch et al. 2013) that FNI mothers had more skin-to-skin holding sessions each week (2.0 ± 0.17) than did SC mothers (0.8 ± 0.14 p < 0.001). These sessions were of longer duration (FNI 83 ± 5; SC 63 ± 4 min/session, p < 0.01). In the current study, those SC mothers who returned for the 4-month visit engaged in skin-to-skin holding during their NICU stay for an average of 331 ± 83 min compared to 786 ± 110 min for FNI mothers (p < 0.002). Across both groups, there was no significant correlation between the total number of skin-to-skin minutes and the CES-D or STAI scores at follow-up (p = 0.77, p = 0.58, respectively). Moreover, the effect of FNI on reducing depressive and anxiety symptoms at 4 months remained significant even when the number of skin-to-skin minutes was included as a covariate (p < 0.04 and p < 0.01, respectively).
To determine the potential impact of selective subject dropout on the depressive symptoms and anxiety results, we computed the baseline scores for mothers in each group who did and who did not return for the 4-month visit. There were 53 FNI mothers with baseline CES-D scores (14.2 ± 1.1) and 55 with baseline STAI scores (38.1 ± 1.7). In the SC group, there were 55 mothers with baseline CES-D (14.0 ± 1.3) and 56 with baseline STAI (38.8 ± 1.7) scores. Among mothers randomized to receive FNI, there was no significant difference in mean baseline CES-D scores between the 40 who did and the 13 who did not return for assessment at 4 months (14.3 ± 1.4 vs 13.9 ± 1.4, respectively), nor was there a significant difference in mean baseline STAI scores for the 42 FNI mothers who did and the 13 who did not complete the STAI (38.2 ± 2.0 vs 37.7 ± 3.0, respectively). However, in the SC group, the 15 mothers without a 4-month CES-D had higher baseline depressive symptoms than the 40 with a 4-month CES-D (18.5 ± 2.6 vs 12.3 ± 1.5, respectively, p = 0.04). There was no significant difference in baseline STAI scores between SC mothers who did not versus those who did return at 4 months (39.2 ± 3.1 vs 38.6 ± 2.1, respectively).
To determine whether the mean 4-month CES-D score for the SC group might have been higher had 15 mothers not been lost to follow-up, we conducted correlation analyses of baseline and 4-month depressive symptoms. For the entire cohort, baseline CES-D scores were correlated with those at 4 months (r = 0.34, p < 0.002, N = 80). However, within each group, these correlations were significant only in the SC group. In the SC group (N = 40), the correlation between baseline and 4-month CES-D was 0.47 (p = 0.002), but in FNI, this relationship was not significant (r = 0.26, p = 0.11, N = 40, Fig. 3a). Thus, it appears that the mean CES-D scores at 4 months were unlikely to have been affected by loss to follow-up in the FNI group but may have been biased downward in the SC group.

Maternal depression and anxiety symptoms are correlated with baseline scores for SC (green circles), but not FNI (purple squares) mothers. a Depressive symptoms (CES-D) at 4 months are significantly correlated with baseline CES-D in SC but not FNI mothers. b Anxiety symptoms (STAI) at 4 months are significantly correlated with baseline STAI in SC but not FNI mothers
We also conducted baseline to 4-month regression analyses for STAI scores. As was the case for CES-D, across both groups, we found that baseline STAI scores were correlated with those at 4 months (r = 0.45, p < 0.001, N = 82). Also, as was found for CES-D, in SC mothers, the correlation between baseline and 4-month STAI was r = 0.67 (p < 0.001, N = 40), but in FNI mothers, this correlation was not significant (r = 0.21, p = 0.19, N = 42, Fig. 3b).
Discussion
This study tested the hypothesis that FNI in the NICU would decrease maternal symptoms of depression and anxiety precipitated by preterm delivery. We found that when mothers and infants returned for follow-up at 4 months corrected age, FNI mothers reported significantly reduced depressive symptoms and anxiety symptoms when compared to SC mothers. Maternal depressive symptoms and anxiety scores in both groups had been equally elevated at the time of their admission to the NICU, which is consistent with other studies (Mew et al. 2003; Rogers et al. 2013; Vasa et al. 2014; Yurdakul et al. 2009). Early in the NICU stay, mothers are confronting the reality of their new baby’s fragile appearance and condition and are managing the ambiguity of their role in the NICU setting. In addition, they are often fearful for the survival of their babies.
Overall, when their infants were 4 months CA, both FNI and SC mothers reported some reduction in depressive and anxiety symptoms since their date of admission to the study, as has been found in other studies of mothers after NICU discharge (Brooten et al. 1988; Trause and Kramer 1983). This would be expected since mothers have left the stressful NICU environment and are able to care for their infant in the comfort of their home. In addition, by this time point, the infants are out of incubators and have gained weight, thus increasing mothers’ confidence in the prospects of their infants’ survival. However, at their infants’ 4-month CA visit, although there was an overall decline in affective symptoms, more SC than FNI mothers reported elevated levels of both depression and anxiety symptoms. This is important developmentally because young infants who have depressed mothers demonstrate decreased positive affect even when interacting with a non-depressed adult (Field et al. 1988). This impairment of social interactions may place their infants at risk for long-term deficits. Thus, reduction in depressive symptoms in the mother at 4 months could be of clinical significance.
Maternal depression at 4 months postpartum is of developmental importance in its own right and is predictive of depression throughout the first year (Pauli-Pott 2008). This is a period when social skills blossom but undeveloped gross and fine motor skills limit forms of exploration to those embedded in mother-infant interactions. Thus, 4 months is ideal for studying face-to-face interactions as well as a time when mother-infant interactions are compromised by concurrent maternal depression (Beebe et al. 2011; Moszkowski et al. 2009). Furthermore, maternal depression at 4 months predicts fearfulness and toddler anxiety (Gartstein et al. 2010) and negative parenting behavior at 18 months (Bridgett et al. 2013). Moreover, the most robust predictor of behavioral inhibition in infants at 14 months of age were depression and anxiety measured at 6 weeks and depression at 4 months (whereas depression and anxiety at 14 months were not associated with behavioral inhibition) (Mertesacker et al. 2004). Maternal depression at 4, but not 8 months, may impair sensitivity and reactivity to highly negative infants over time (Moehler et al. 2007).
Several factors may account for the reduced maternal anxiety and depression symptoms in FNI mothers at 4 months. Various activities of the intervention (scent exchange, vocal soothing, comforting touch, eye contact, and emotional communication) are specifically designed to enhance maternally mediated sensory experiences of preterm infants, as well as infant-mediated sensory experiences of the mother (Welch et al. 2012). Taken together, these factors increase the likelihood that the mother will emotionally connect with her infant, the basis of an optimally co-regulated dyad.
The follow-up retention rates in the study were not as high as we had hoped. Thus, there is a possible self-selection bias in the results. Such a bias might have gone in either direction. That is, one can think of reasons why mothers who took the time and effort to come back for the follow-up session might have been either more or less depressed than mothers who declined follow-up. Importantly, we found that mothers and infants who returned at 4 months had similar demographic characteristics, and their infants had similar clinical courses when compared to those who did not return at 4 months CA. In addition, analyses showed there was no difference in baseline CES-D or STAI scores between FNI mothers who did or did not return at 4 months. In contrast, SC mothers who did not return at 4 months had higher baseline anxiety and depressive symptom scores than SC mothers who did return. Moreover, baseline scores in SC mothers were highly correlated with scores at 4 months. Together, these results suggest that our findings would have been even stronger had all mothers come back and the findings would generalize to the RCT cohort as a whole.
Concurrent breastfeeding has been associated with decreases in maternal depression (Ip et al. 2009). However, it is not clear from the literature whether a prior history of breastfeeding of preterm infants during the NICU stay alone also has a protective effect. We found that FNI did not alter engagement in breastfeeding in the NICU and was not related to the effects of FNI on reducing depressive and anxiety symptoms at 4 months.
Feldman and colleagues reported that skin-to-skin holding of prematurely born infants is associated with decreased maternal depressive symptoms at term age, particularly in lower risk infants (Feldman et al. 2002). We did not find a significant correlation between the amount of skin-to-skin holding and maternal depressive or anxiety symptoms at 4 months or at term age, irrespective of infant body weight either less or greater than 1500 g (data not shown). However, it is important to recognize that mothers in our study engaged in much less skin-to-skin care than in the Feldman et al. study (26.6 vs 13.1 h in FNI and 5.5 h in SC). Regardless, in our study, results from covariate analyses showed that decreases in depressive and anxiety symptoms at 4 months were not related to the amount of skin-to-skin care.
A recent meta-analysis identified few effective interventions that reduce maternal depression and anxiety following preterm birth, and the results were generally of small magnitude (Kraljevic and Warnock 2013). However, a recent RCT of a trauma-focused psychotherapy intervention (six to nine sessions) in mothers of prematurely born infants found robust decreases in maternal depression and anxiety at 6 months (effect sizes = 0.64 and 0.63, respectively) (Shaw et al. 2014). Effect sizes of FNI were of similar magnitude: 0.46 and 0.63 for maternal depressive and anxiety symptoms at 4 months, respectively. It is remarkable that FNI, which is focused on encouraging mother and infant emotional connectivity, was as effective at reducing post-discharge maternal depressive and anxiety symptoms as the aforementioned intervention which was specifically designed to target these outcomes. This is encouraging because FNI can start soon after birth, even when the baby is confined to the incubator, and is designed to be integrated into standard care administered by NICU nurses and does not require added NICU staff trained in psychotherapy.
Our parallel group RCT used a standard care (i.e., usual care) group as control. While commonly used in RCTs, there are limitations with this approach. First, there were no control conditions employed for specific aspects of the intervention. For example, the SC mothers and infants did not exchange sham odor cloths, i.e., cloths not exposed to the infants and mothers. FNI was designed to improve emotional connectivity by normalizing, to the extent possible in the NICU, the mother/infant experiences of each other. Accordingly, there were multiple opportunities and modes of facilitated interactions: odor exchange, soothing touch, vocal and eye contact, as well as skin-to-skin holding. In this first trial of FNI, it was not possible to include control manipulations for all activities comprising the intervention. Thus, for the present, the effectiveness of FNI can only be evaluated as an integrated and comprehensive intervention strategy.
It is also possible that the effectiveness of the intervention, even on long-term outcomes, was not related to specific aspects of the intervention but rather a more general effect related to the special attention that the FNI mothers received. It is important to note that the SC control group, while receiving clinical care as usual, also received increased attention from the study staff throughout their infants’ NICU stay. SC control mothers were aware that they were in a study and, prior to their acceptance in study, agreed that they could be available to meet on a regular basis with study staff, regardless of which group they were assigned. Study research assistants met with the SC control mothers each week to administer and collect questionnaire information. These questions included tracking when and for how long they visited as well as questions about their activities during visits, for example, “How long did you hold your baby?” Thus, while increased attention from study staff could in part be responsible for effectiveness of the trial, increased attention given to the control group may have actually contributed to smaller differences between the groups. Even if the positive effects of FNI on reducing maternal depressive and anxiety symptoms at 4 months were merely due to participation in the protocol, this would indicate that relatively simple changes in non-clinical activities in the NICU can benefit these mothers and infants.
This study has several strengths. First, it is a randomized controlled trial. Second, we found no systematic differences in demographic characteristics of those who provided, versus those who did not provide reports, at any time points: either at the time of randomization, at the infants’ near to term age, or at 4-month corrected age. Finally, following subjects to 4 months proved to be critical because we found that significant effects of the intervention on maternal depressive and anxiety symptoms did not emerge until this time point. Interestingly, two other hospital-based interventions also demonstrated delayed emergence of effects well beyond the period of intervention (Melnyk et al. 2008; Shaw et al. 2014). It is possible that FNI mothers continue to engage in FNI nurture behaviors post-discharge and that beneficial effects increase with time. It is also possible that beneficial effects of the intervention on the mother can only be manifest after the mother and infant are safely united at home.
The FNI RCT was designed to test the effect of this NICU-based intervention on preterm infant neurodevelopment. Results from analyses of brain activity at term age give biological support to the effectiveness of this approach (Welch et al. 2014). The present study demonstrates that FNI is also effective in alleviating self-reported depressive symptoms and anxiety in mothers of preterm infants at 4 months CA, well beyond the time when FNI mothers were engaged in the facilitated intervention. These results indicate that this early hospital-based intervention, which is aimed at facilitating mother-infant emotional connection, may be an effective way to reduce maternal depressive and anxiety symptoms during a crucial period of development of mother/infant co-regulation. Reductions in maternal symptoms mediated by FNI are of potential clinical significance to infant development, as well as to maternal health.
References
Aagaard H, Hall EO (2008) Mothers’ experiences of having a preterm infant in the neonatal care unit: a meta-synthesis. J Pediatr Nurs 23:e26–e36
Aylward GP (2005) Neurodevelopmental outcomes of infants born prematurely. J Dev Behav Pediatr : JDBP 26:427–440
Ballantyne M, Benzies KM, Trute B (2013) Depressive symptoms among immigrant and Canadian born mothers of preterm infants at neonatal intensive care discharge: a cross sectional study. BMC Pregnancy Childbirth 13:S11
Beebe B, Steele M, Jaffe J, Buck KA, Chen H, Cohen P, Kaitz M, Markese S, Andrews HF, Margolis A, Feldstein S (2011) Maternal anxiety symptoms and mother-infant self- and interactive contingency. Infant Ment Health J 32:174–206
Brandon DH, Tully KP, Silva SG, Malcolm WF, Murtha AP, Turner BS, Holditch-Davis D (2011) Emotional responses of mothers of late-preterm and term infants. J Obstet Gynecol Neonatal Nurs : JOGNN / NAACOG 40:719–731
Brett J, Staniszewska S, Newburn M, Jones N, Taylor L (2011) A systematic mapping review of effective interventions for communicating with, supporting and providing information to parents of preterm infants. BMJ Open 1:e000023
Bridgett DJ, Laake LM, Gartstein MA, Dorn D (2013) Development of infant positive emotionality: the contribution of maternal characteristics and effects on subsequent parenting. Inf Child Dev 22:362–382
Brooten D, Gennaro S, Brown LP, Butts P, Gibbons AL, Bakewell-Sachs S, Kumar SP (1988) Anxiety, depression, and hostility in mothers of preterm infants. Nurs Res 37:213–216
Carver CSW (1994) Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: the BIS/BAS scales. J Pers Soc Psychol 67:319–333
Cho J, Holditch-Davis D, Miles MS (2008) Effects of maternal depressive symptoms and infant gender on the interactions between mothers and their medically at-risk infants. J Obstet Gynecol Neonatal Nurs : JOGNN / NAACOG 37:58–70
Davis L, Edwards H, Mohay H, Wollin J (2003) The impact of very premature birth on the psychological health of mothers. Early Hum Dev 73:61–70
Dayan J, Creveuil C, Marks MN, Conroy S, Herlicoviez M, Dreyfus M, Tordjman S (2006) Prenatal depression, prenatal anxiety, and spontaneous preterm birth: a prospective cohort study among women with early and regular care. Psychosom Med 68:938–946
Feeley N, Gottlieb L, Zelkowitz P (2005) Infant, mother, and contextual predictors of mother-very low birth weight infant interaction at 9 months of age. J Dev Behav Pediatr : JDBP 26:24–33
Feldman R, Eidelman AI, Sirota L, Weller A (2002) Comparison of skin-to-skin (kangaroo) and traditional care: parenting outcomes and preterm infant development. Pediatrics 110:16–26
Field T (2010) Postpartum depression effects on early interactions, parenting, and safety practices: a review. Infant Behav Dev 33:1–6
Field T, Healy B, Goldstein S, Perry S, Bendell D, Schanberg S, Zimmerman EA, Kuhn C (1988) Infants of depressed mothers show “depressed” behavior even with nondepressed adults. Child Dev 59:1569–1579
Forcada-Guex M, Pierrehumbert B, Borghini A, Moessinger A, Muller-Nix C (2006) Early dyadic patterns of mother-infant interactions and outcomes of prematurity at 18 months. Pediatrics 118:e107–e114
Forcada-Guex M, Borghini A, Pierrehumbert B, Ansermet F, Muller-Nix C (2011) Prematurity, maternal posttraumatic stress and consequences on the mother-infant relationship. Early Hum Dev 87:21–26
Garel M, Dardennes M, Blondel B (2007) Mothers’ psychological distress 1 year after very preterm childbirth. Results of the EPIPAGE qualitative study. Child Care Health Dev 33:137–143
Gartstein MA, Bridgett DJ, Rothbart MK, Robertson C, Iddins E, Ramsay K, Schlect S (2010) A latent growth examination of fear development in infancy: contributions of maternal depression and the risk for toddler anxiety. Dev Psychol 46:651–668
Hofer MA (1975) Studies on how early maternal separation produces behavioral change in young rats. Psychosom Med 37:245–264
Hofer MA (1994) Hidden regulators in attachment, separation, and loss. Monogr Soc Res Child Dev 59:192–207
Hofer MA (1996) On the nature and consequences of early loss. Psychosom Med 58:570–581
Ip S, Chung M, Raman G, Trikalinos TA, Lau J (2009) A summary of the Agency for Healthcare Research and Quality’s evidence report on breastfeeding in developed countries. Breastfeed Med : Off J Acad Breastfeed Med 4(Suppl 1):S17–S30
Johnson AN (2008) Promoting maternal confidence in the NICU. J Pediatr Health Care : Off Publ Natl Assoc Pediatr Nurse Assoc Pract 22:254–257
Kikkert HK, Middelburg KJ, Hadders-Algra M (2010) Maternal anxiety is related to infant neurological condition, paternal anxiety is not. Early Hum Dev 86:171–177
Korja R, Savonlahti E, Ahlqvist-Bjorkroth S, Stolt S, Haataja L, Lapinleimu H, Piha J, Lehtonen L, Group P.s. (2008) Maternal depression is associated with mother-infant interaction in preterm infants. Acta Paediatr 97:724–730
Kraljevic M, Warnock FF (2013) Early educational and behavioral RCT interventions to reduce maternal symptoms of psychological trauma following preterm birth: a systematic review. J Perinat Neonatal Nurs 27:311–327
Landry SH, Smith KE, Swank PR (2003) The importance of parenting during early childhood for school-age development. Dev Neuropsychol 24:559–591
McManus BM, Poehlmann J (2012) Parent-child interaction, maternal depressive symptoms and preterm infant cognitive function. Infant Behav Dev 35:489–498
Meijssen D, Wolf M-J, van Bakel H, Koldewijn K, Kok J, van Baar A (2011) Maternal attachment representations after very preterm birth and the effect of early intervention. Infant Behav Dev 34:72–80
Melchior M, Chastang JF, de Lauzon B, Galera C, Saurel-Cubizolles MJ, Larroque B, Group, E.M.-C.C.S. (2012) Maternal depression, socioeconomic position, and temperament in early childhood: the EDEN Mother-Child Cohort. J Affect Disord 137:165–169
Melnyk BM, Crean HF, Feinstein NF, Fairbanks E (2008) Maternal anxiety and depression after a premature infant’s discharge from the neonatal intensive care unit: explanatory effects of the creating opportunities for parent empowerment program. Nurs Res 57:383–394
Mertesacker B, Bade U, Haverkock A, Pauli-Pott U (2004) Predicting maternal reactivity/sensitivity: the role of infant emotionality, maternal depressiveness/anxiety, and social support. Infant Ment Health J 25:47–61
Mew AM, Holditch-Davis D, Belyea M, Miles MS, Fishel A (2003) Correlates of depressive symptoms in mothers of preterm infants. Neonatal Netw 22:51–60
Miles MS, Holditch-Davis D, Schwartz TA, Scher M (2007) Depressive symptoms in mothers of prematurely born infants. J Dev Behav Pediatr : JDBP 28:36–44
Misund AR, Nerdrum P, Braten S, Pripp AH, Diseth TH (2013) Long-term risk of mental health problems in women experiencing preterm birth: a longitudinal study of 29 mothers. Ann Gen Psychiatr 12:33
Moehler E, Kagan J, Parzer P, Brunner R, Reck C, Wiebel A, Poustka L, Resch F (2007) Childhood behavioral inhibition and maternal symptoms of depression. Psychopathology 40:446–452
Moster D, Lie RT, Markestad T (2008) Long-term medical and social consequences of preterm birth. N Engl J Med 359:262–273
Moszkowski RJ, Stack DM, Girouard N, Field TM, Hernandez-Reif M, Diego M (2009) Touching behaviors of infants of depressed mothers during normal and perturbed interactions. Infant Behav Dev 32:183–194
Myers MM, Brunelli SA, Shair HN, Squire JM, Hofer MA (1989a) Relationships between maternal behavior of SHR and WKY dams and adult blood pressures of cross‐fostered F1 pups. Dev Psychobiol 22:55–67
Myers MM, Brunelli SA, Squire JM, Shindeldecker RD, Hofer MA (1989b) Maternal behavior of SHR rats and its relationship to offspring blood pressures. Dev Psychobiol 22:29–53
Neu M, Hazel NA, Robinson J, Schmiege SJ, Laudenslager M (2014) Effect of holding on co-regulation in preterm infants: a randomized controlled trial. Early Hum Dev 90:141–147
Pauli-Pott U (2008) Mothers with depressive symptoms: cross-situational consistency and temporal stability of their parenting behavior. Infant Behav Dev 31:679–687
Peterson RA, Reiss S (1987) Anxiety Sensitivity Index manual. IDS Publishing Worthington, OH
Phillips GS, Wise LA, Rich-Edwards JW, Stampfer MJ, Rosenberg L (2010) Prepregnancy depressive symptoms and preterm birth in the Black Women’s Health Study. Ann Epidemiol 20:8–15
Poehlmann J, Hane A, Burnson C, Maleck S, Hamburger E, Shah PE (2012) Preterm infants who are prone to distress: differential effects of parenting on 36-month behavioral and cognitive outcomes. J Child Psychol Psychiatry 53:1018–1025
Radloff LS (1977) The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1:385–401
Rogers CE, Kidokoro H, Wallendorf M, Inder TE (2013) Identifying mothers of very preterm infants at-risk for postpartum depression and anxiety before discharge. J Perinatol 33:171–176
Shaw RJ, St John N, Lilo E, Jo B, Benitz W, Stevenson DK, Horwitz SM (2014) Prevention of traumatic stress in mothers of preterms: 6-month outcomes. Pediatrics
Singer LT, Salvator A, Guo S, Collin M, Lilien L, Baley J (1999) Maternal psychological distress and parenting stress after the birth of a very low-birth-weight infant. JAMA 281:799–805
Spielberger CD, Gorsuch RL, Lushene RE (1970) Manual for the State-Trait Anxiety Inventory. Consulting Psychologists Press, Palo Alto
Tietz A, Zietlow AL, Reck C (2014) Maternal bonding in mothers with postpartum anxiety disorder: the crucial role of subclinical depressive symptoms and maternal avoidance behaviour. Arch Womens Ment Health, 1-10
Tilton SR (2008) Review of the State-Trait Anxiety Inventory (STAI). NewsNotes 48
Trause MA, Kramer LI (1983) The effects of premature birth on parents and their relationship. Dev Med Child Neurol 25:459–465
Treyvaud K, Lee KJ, Doyle LW, Anderson PJ (2014) Very preterm birth influences parental mental health and family outcomes seven years after birth. J Pediatr 164:515–521
Vasa R, Eldeirawi K, Kuriakose VG, Nair GJ, Newsom C, Bates J (2014) Postpartum depression in mothers of infants in neonatal intensive care unit: risk factors and management strategies. Am J Perinatol 31:425–434
Vigod SN, Villegas L, Dennis CL, Ross LE (2010) Prevalence and risk factors for postpartum depression among women with preterm and low-birth-weight infants: a systematic review. BJOG 117:540–550
Welch MG, Hofer MA, Brunelli SA, Stark RI, Andrews HF, Austin J, Myers MM, Family Nurture Intervention Trial, G. (2012) Family nurture intervention (FNI): methods and treatment protocol of a randomized controlled trial in the NICU. BMC Pediatr 12:14
Welch MG, Hofer MA, Stark RI, Andrews HF, Austin J, Glickstein SB, Ludwig RJ, Myers MM, Group, F.N.I.T. (2013) Randomized controlled trial of family nurture intervention in the NICU: assessments of length of stay, feasibility and safety. BMC Pediatr 13:148
Welch MG, Myers MM, Grieve PG, Isler JR, Fifer WP, Sahni R, Hofer MA, Austin J, Ludwig RJ, Stark RI, Group, F.N.I.T. (2014) Electroencephalographic activity of preterm infants is increased by family nurture intervention: a randomized controlled trial in the NICU. Clin Neurophysiol : Off J Int Fed Clin Neurophysiol 125:675–684
Woodward LJ, Bora S, Clark CAC, Montgomery-Honger A, Pritchard VE, Spencer C, Austin NC (2014) Very preterm birth: maternal experiences of the neonatal intensive care environment. J Perinatol
Younger JB, Kendell MJ, Pickler RH (1997) Mastery of stress in mothers of preterm infants. J Soc Pediatr Nurses : JSPN 2:29–35
Yurdakul Z, Akman I, Kuscu MK, Karabekiroglu A, Yaylali G, Demir F, Ozek E (2009) Maternal psychological problems associated with neonatal intensive care admission. Int J Pediatr 2009:591359
Zelkowitz P, Papageorgiou A, Bardin C, Wang T (2009) Persistent maternal anxiety affects the interaction between mothers and their very low birthweight children at 24 months. Early Hum Dev 85:51–58
Zelkowitz P, Na S, Wang T, Bardin C, Papageorgiou A (2011) Early maternal anxiety predicts cognitive and behavioural outcomes of VLBW children at 24 months corrected age. Acta Paediatr 100:700–704
Acknowledgments
We would like to thank the NICU staff at the Morgan Stanley Children’s Hospital of New York as well as the participating families for their invaluable assistance to our program of research. We also want to acknowledge and thank our Data and Safety Monitoring Board for their thoughtful contributions to the conduct of this study (Bruce Levin, PhD; Michael Weitzman, MD; and Deborah E. Campbell, MD). This study was funded by the Einhorn Family Charitable Trust, the Fleur Fairman Family to the BrainGut Initiative at Columbia University Medical Center, and Columbia University’s CTSA from NCRR/NIH (UL1RR024156).
Conflict of interest
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. Author MMM received salary support from the New York State Office of Mental Health Research Scientist position. Donors and institutions funding this work had no direct role in study design, data interpretation, or preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Welch, M.G., Halperin, M.S., Austin, J. et al. Depression and anxiety symptoms of mothers of preterm infants are decreased at 4 months corrected age with Family Nurture Intervention in the NICU. Arch Womens Ment Health 19, 51–61 (2016). https://doi.org/10.1007/s00737-015-0502-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00737-015-0502-7