
Abstract
Creatine kinetics were measured in young healthy subjects, eight males and seven females, age 20-30 years, after an overnight fast on creatine-free diet. Whole body turnover of glycine and its appearance in creatine was quantified using [1-13C] glycine and the rate of protein turnover was quantified using L-ring [2H5] phenylalanine. The creatine pool size was estimated by the dilution of a bolus [C2H3] creatine. Studies were repeated following a five days supplement creatine 21 g.day−1 and following supplement amino acids 14.3 g day−1. Creatine caused a ten-fold increase in the plasma concentration of creatine and a 50 % decrease in the concentration of guanidinoacetic acid. Plasma amino acids profile showed a significant decrease in glycine, glutamine, and taurine and a significant increase in citrulline, valine, lysine, and cysteine. There was a significant decrease in the rate of appearance of glycine, suggesting a decrease in de-novo synthesis (p = 0.006). The fractional and absolute rate of synthesis of creatine was significantly decreased by supplemental creatine. Amino acid supplement had no impact on any of the parameters. This is the first detailed analysis of creatine kinetics and the effects of creatine supplement in healthy young men and women. These methods can be applied for the analysis of creatine kinetics in different physiological states.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Creatine, an ergogenic compound, is an important intermediate in the metabolism of the muscle, brain, and other tissues with high energy demand and fluxes (Wyss and Kaddurah-Daouk 2000; Brosnan and Brosnan 2007). It plays a critical role in buffering and translocation of energy via the creatine kinase phosphocreatine system. Functional impairment of this system leads to deterioration of energy metabolism, which is the phenotype for many neurodegenerative- and age-related disorders. It has been shown to affect satellite cell proliferation and differentiation in cell culture systems (Vierck et al. 2003), and increase satellite cell mitotic activity during compensatory hypertrophy in the rat skeletal muscle (Dangott et al.2000). In humans, creatine supplementation, in combination with strength training, amplified the training induced increase in satellite cell number and myonuclei concentration in skeletal muscle fibers (Olsen et al. 2006). A beneficial effect of creatine supplementation on muscle performance during resistance training has been suggested in some studies. Quantification of protein turnover following creatine supplementation has shown either no effect or a decrease in protein breakdown (Louis et al. 2003). However, supplement did not appear to impact the fractional rate of protein synthesis in the skeletal muscle.
Creatine is synthesized by a two-step process from glycine, arginine, and methionine. The first step involves the synthesis of guanidinoacetic acid (GAA) from glycine and arginine catalyzed by the reversible arginine glycine amidinotransferase (AGAT, EC2.1.4.1). Irreversible methylation of GAA by guanidine N-methyltransferase (GNMT, EC 3.5.3.2) utilizes s-adenosylmethionine (SAM) as the methyl donor and results in the formation of creatine and s-adenosylhomocysteine (SAH). In rats, AGAT is mainly expressed in the kidney and the GAMT is mainly localized in the liver resulting in an inter-organ synthesis of creatine (da Silva et al. 2009; Wyss and Kaddurah-Daouk 2000; Edison et al. 2007). The data in human are unclear, and a complete pathway for creatine synthesis may be present in the liver, pancreas, and possibly brain. The kidney is estimated to contribute 20–25 % of the GAA to total creatine synthesis in humans (Edison et al. 2007). Creatine is eliminated from the body following its spontaneous breakdown to creatinine.
Because of its multi-compartmental and large volume of distribution and a relatively slow rate of turnover, the rate of creatine synthesis has not been quantified systematically in healthy humans. Previous data have relied upon the rate of creatine/creatinine excretion in the urine, organ balance, or by using 14C or 15N tracers in a few subjects (Hoberman et al. 1948a, b; Sandberg et al. 1953; Crim et al. 1976). The long duration (days) of the tracer elimination and the errors associated with the measurements of urinary losses has made the study of creatine kinetics in vivo difficult. We have developed a GC-mass spectrometric method for the simultaneous measurement of tracer enrichment and concentration of GAA and creatine in biological fluids (Kasumov et al. 2009). In the present study, we have applied this technique in order to quantify the rate of creatine synthesis and its pool size in healthy subjects. In addition, we have quantified the response to the administration of supplemental creatine and of supplemental amino acids on creatine, glycine, and protein kinetics in the same subjects.
Materials and methods
Young, healthy subjects (8 males and 7 females) were recruited for the kinetic studies by advertisement. At recruitment, a detailed clinical history was obtained and a physical examination was done. Subjects with a family history of chronic illness were excluded from the study. Other exclusion criteria included intake of nutritional supplements, medication, prior history of creatine supplementation, and any known medical condition that may impact skeletal muscle, liver, or renal function. All eligible subjects had routine blood chemistries (liver function test, metabolic panel), complete blood count, and urinalysis performed prior to the study. The study protocol was reviewed and approved by the institutional review board of the Cleveland Clinic Foundation. Written informed consent was obtained from all participants after fully explaining the procedure. The study was registered with Clinical Trials.Gov (NCT01725503).
Anthropometric details of the study subjects are displayed in Table 1. Their blood counts, liver function test, and other metabolic parameters were within the normal range (supplement Table 1). Body composition analysis was done by dual-energy-X-ray absorptiometry (DEXA, Lunar iDXA, GE Healthcare). None of the subjects were overweight or obese (mean fat mass ~30 % of body weight, Table 1).
Creatine kinetics were measured (i) following 5 days of creatine-free diet (study 1), (ii) following 5 days of supplemental creatine 21 g d−1 (study 2) and (iii) following 5 days of an amino acid supplement (study 3). Seven subjects (5 males, 2 females) participated in the amino acid supplement study.
Study 1
The study design is displayed in Fig. 1. All subjects were advised a creatine-free (meat-free) 75 grams protein daily diet for 5 days prior to the tracer study. Dietary compliance was monitored by the clinical nutritionist. They were instructed not to engage in any exercise for 3 days prior to the tracer infusion study. A 24 h urine specimen was obtained to measure total creatinine excretion. Subjects reported to the Clinical Research Unit at the Cleveland Clinic at 7 AM, following a 10 h overnight fast. Their weight, height, and vital signs were measured. Two indwelling cannulae were placed in a superficial dorsal vein of each hand, one for tracer infusion and the other to obtain blood samples. The sampling site was kept warm by placing the hand in a thermostat-controlled warm blanket, and kept patent by a constant flow infusion of isotonic saline solution. Accurately weighed amounts of sterile, pyrogen free, [1-13C]glycine and L-ring[2H5]phenylalanine (from Cambridge Isotope Laboratories, Inc., Andover, MA, USA) were dissolved in a sterile 0.45 % saline solution in a laminar flow hood. Tracer solutions were further sterilized by filtering through a 0.22 micron filter (Millex; Millipore, Bedford, MA). The tracers were administered as prime-constant rate infusion for 8 h. Their respective doses were as follows: [1-13C]glycine, prime: 10 micromoles kg−1, constant infusion: 10 micromoles kg−1 h−1; L-ring[2H5]phenylalanine, prime: 2 micromoles kg −1, constant infusion: 2 micromoles.kg−1 h−1. The actual rate of infusion was confirmed by gravimetrically measuring the rate of flow using the same tubing and equipment at the end of the study. The concentration of glycine and phenylalanine in the infusate were measured as described in analytical methods. All tracer solutions were tested in the hospital clinical laboratory and were found to be sterile.

The plan for the tracer studies is displayed. All subjects were placed on a creatine (meat) free diet for 5 days prior to the tracer study. Following an overnight fast tracer [1-13C]glycine and [2H5]phenylalanine were infused intravenously as prime-constant rate infusion. A bolus infusion of [C2H3]creatine was administered to quantify the creatine pools. Blood samples were drawn at times shown. The rates of CO2 production were measured using a calorimetry system at time shown
A bolus dose (150 mg) of [C2H3]creatine monohydrate was administered over 3-5 min at the start of the study in order to measure the pool size of creatine. Three subjects, studied initially, received 250 mg bolus creatine. Blood samples in EDTA were obtained at 3 min intervals for the first 30 min, and at 30 min interval for the duration of the study. Samples of expired air were collected using a Rudolph one-way valve system as described (Kalhan et al. 1998). An aliquot of expired air was transferred into a sampling tube for the measurement of 13C enrichment of the expired CO2. The rate of production CO2 and the rate of consumption of O2 were measured using an open hood respiratory calorimetry system (Viasys Encore, Cardinal Health, Dublin, OH).
Study 2
All subjects were studied again 2–16 weeks later. They were placed on a regular diet containing a minimum 75 gm protein for 5 days prior to tracer study. In addition, they were given supplemental creatine, 21 gm/day, 7 gm 3 times a day, for 5 days. Creatine monohydrate for oral supplementation was purchased from General Nutrition Corporation, Pittsburgh, PA. It was dispensed as 7 gram aliquots. Each aliquot was dissolved in orange juice and taken orally. The subjects ingested the creatine without any problem. At the end of 5 days, the tracer isotope study was performed during fasting as described for study 1.
Study 3
Seven subjects (5 males, 2 females) were studied again while receiving an amino acid supplement. The supplement was given as amino acid capsules, 3 times a day (14.3 grams per day) with meals. Those who could not ingest the capsule were asked to open them and dissolve in juice. Each dose (4.766 gms) of the amino acid mixture contained l-leucine 1268.7 mg, l-isoleucine 339.6 mg, l-valine 348.7 mg, l-threonine 295.7 mg, l-lysine 528.4 mg, l-methionine 105.2 mg, l-histidine 52.9 mg, l-phenylalanine 211.4 mg, and l-tryptophan 21.2 mg. The amino acid mixture was prepared by Ajinomoto U.S.A., Inc. (Fort Lee, NJ) and packaged into capsule form by Atlantic Essential Products, Inc. (Hauppauge, NY). The tracer study was performed as described in Study 1.
Analytical methods
Enrichments of glycine, serine, and phenylalanine were measured using gas chromatography-mass spectrometry (GC–MS). Amino acids in the plasma were separated using mixed-bed ion exchange chromatography as described previously (Kalhan et al. 1998). An N-propyl-n-acetyl ester derivative of glycine, serine, and phenylalanine was prepared according to the method of Adams (Adams 1974), as described before (Kalhan et al. 1998). The glycine and serine derivatives were separated on a GC-mass spectrometry system (6890 N GC System coupled with 5973 mass selective detector; Agilent Technologies, Santa Clara, CA) using HP-INNOWAX capillary column (30 m × 0.25 mm × 0.25 µm) as described previously (Dasarathy et al. 2009; Kalhan et al. 2011). Positive chemical ionization and selected ion monitoring (SIM) were used to monitor mass-to-charge ratio (m/z) for ions 160 and 161 representing unlabeled (m0) and 13C-labeled (m1) glycine and m/z 232 and 233 corresponding to unlabeled serine and [1-13C]serine. For phenylalanine, the ions monitored were m/z 250 and 255 corresponding to unlabeled and 2H5-labeled (m5) phenylalanine. Standard solutions of known enrichments were run simultaneously to correct for variations in instrumentations. The concentrations of cysteine, homocysteine, and glutathione in the plasma were measured as described previously (Dasarathy et al. 2009). This method measures the total cysteine (cysteine and cysteine) and total homocysteine (free and protein bound) in the plasma.
Calculations
Fat mass and Lean mass were calculated from the body composition study by DEXA, using proprietary software (GE Healthcare). The muscle mass was estimated from the lean mass assuming that muscle mass represents 54 and 48 % of total fat free body weight, respectively, in males and females (Clarys et al. 1984). The rate of appearance of glycine and phenyalanine was calculated using tracer dilution equations during steady state as described previously (Kalhan et al. 1998). The rate of oxidation of glycine was calculated from the rate of CO2 production and the appearance of 13C in the expired CO2 using precursor product relationship (Dasarathy et al. 2009).
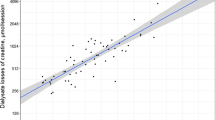
The pool size of creatine was estimated from the dilution of a given dose of [C2H3]creatine (m3) in the plasma. As shown in the Fig. 3, the dilution (enrichment of creatine in the plasma) of the bolus dose creatine tracer revealed a bi-exponential curve suggesting two distinct pools of creatine: a smaller rapidly mixing pool and a second large pool in which a slow distribution of the injected bolus tracer occurred. Using the “curve stripping” process and log transformation of the tracer enrichment time data, the tracer enrichment at time zero, where the best-fit lines cross the y axis, for the two exponents was calculated (Teuscher 2011). The estimated dilution of the tracer (m3/m0) at time zero relative to the administered dose was used to estimate the pool size (Q1 and Q2) of creatine in the two compartments.
The fractional rate of synthesis of creatine (FSR) was calculated from the [13C] enrichment of the immediate precursor, guadinoacetic acid, (EGAA) and that of the product, creatine, (EC) following [1-13C]glycine infusion, as follows: FSR creatine (%/day) = (slope of EC/EGAA)*1440*100. The absolute rate of creatine synthesis (ASR) equals FSR*creatine pool (Q2).
Statistical Analysis
All data are reported as mean ± std. dev. Paired t test were used to compare the response to supplemental creatine or with amino acids in the same subject. Correlations and curve fitting for each subject were done using Origin 9 data analysis and graphing software (OriginLab Corporation, Northampton, MA, USA).
Results
The anthropometric characteristics of the study subjects are displayed in Table 1. As shown, the study subjects were between 20 and 30 years of age, were in good health and their metabolic laboratory data (supplemental Table 1) were within the normal range. The concentrations of creatinine and urea nitrogen in the plasma also were within the normal range. Their fat mass and lean body mass estimated using DEXA and calculated muscle mass are displayed. The muscle mass was calculated from the lean body mass using the equations of Clarys et al. (1984). The responses to the administration of creatine are described below. Amino acid administration did not have any significant effect on any of the parameters studied (supplemental tables).
Body weight, plasma Creatine, Creatinine, Guanidinoacetic acid, and urinary Creatinine (Table 2)
Creatine supplement did not cause any significant change in the average body weight of the entire group. However when examined separately, in female subjects the increase in body weight (mean ~1.4 kg) was statistically significant (p = 0.002). Plasma creatine concentration was similar in males and females while on creatine-free diet. Five days of creatine supplement caused a marked increase in plasma concentration of creatine (measured ~12 h after the last creatine dose) in both males and females. The only exception was one male subject who did not show any change in plasma creatine and did not show significant change in other parameters. None the less he is included in all analysis. As reported by others in humans and animals (Derave et al. 2004; Edison et al. 2007), there was a significant decrease (50 %) in the concentration of guanidinoacetic acid in the plasma in all subjects following creatine supplementation. The plasma concentration of GAA was lower in the female subjects compared with the males on creatine-free diet and when receiving creatine supplement (Table 2). While on creatine-free diet, the plasma concentration of GAA was significantly correlated with estimated muscle mass in all subjects, Pearson r = 0.657, P = 0.008.
There was no effect of supplement creatine on plasma creatinine concentration or on the 24 h urinary creatinine excretion neither in male nor in female subjects (Table 2). The plasma concentrations of creatinine and the 24 h urinary creatinine excretion were significantly less in the female subjects while on creatine-free diet, reflecting their lower muscle mass (Table 2). The plasma concentration of creatinine in the females remained lower than that in the males while on creatine supplement.
Plasma cysteine, homocysteine, and glutathione
Creatine supplement caused a significant increase in the plasma concentration of total cysteine in the entire group. Individually, the increase was statistically significant only in the females and not in the males. There was no change in the total homocysteine concentration in the plasma following creatine supplement. Total glutathione concentration in the plasma was lower following creatine supplement in the female subjects but not in the males (Table 3). The plasma levels of cysteine, homocysteine, and glutathione were not correlated with plasma levels of creatine.
Plasma amino acid concentration
Five days of creatine supplement resulted in a significant decrease in plasma levels of glycine in all subjects (p = 0.004). There was a significant increase in plasma levels of citrulline, valine, and lysine and a significant decrease in the levels of glutamine and taurine (Table 4). There was no change in the levels of other amino acids in the plasma.
Glycine and phenylalanine kinetics
The rates of appearance (Ra) of phenylalanine and glycine were calculated, using tracer dilution equations, at isotopic steady state, achieved in all subjects between 1.5 and 2 h of tracer infusion. Creatine supplement had no effect on the whole body rate of protein turnover as measured by the rate of appearance of phenylalanine in the plasma neither in male nor in female subjects (Table 5). In contrast, there was a significant decrease in the rate of appearance of glycine in the entire group (130.3 ± 26.9 vs 117.3 ± 20.9 micromoles/kg/h, p = 0.006). Glycine Ra decreased in all subjects except two male subjects who showed an increase in Ra following creatine supplement. Although there was a decrease in mean Ra of glycine in both male and female subjects, the decrease was significant only in the female subjects (p = 0.04). The decrease in glycine Ra in the presence of unchanged Ra phenylalanine suggests a decrease in de-novo synthesis of glycine. Approximately 24 % of glycine Ra or ~30 micromoles kg−1 h−1 was oxidized (glycine cleavage system) and ~22 % of serine was derived from glycine. The rate of oxidation of glycine decreased significantly in the entire group (p = 0.02) and in the male subjects (p = 0.02) following creatine supplement. The fraction of serine derived from glycine was not affected by creatine supplement.
Guanidino acetic acid
Five days of creatine supplement resulted in ~50 % reduction in plasma GAA concentration in all subjects (Table 2). As shown in Fig. 2, there was a rapid appearance of tracer in the plasma GAA following the prime injection of tracer glycine, suggesting a rapid enrichment of glycine pool at the site/s of synthesis of GAA. This was followed by a slow linear increase in [13C] enrichment (m1) of GAA in the plasma (average slope of m1 mol % excess in GAA = 0.002/min). Creatine supplement did not impact the slope of enrichment in GAA in either male or female subjects, The average enrichment of GAA between 2nd and the 5th hr was used to calculate the fractional rate of synthesis of creatine. The average enrichment in GAA was 44 and 36 % of plasma glycine enrichment, respectively, on creatine-free diet and on creatine supplement (Table 6). The lower GAA/glycine enrichment ratio on creatine supplement diet was due to higher m1 enrichment of the plasma glycine pool.

The time course of appearance of [1-13C]glycine (m1) in the plasma guanidinoacetic acid following prime-constant rate infusion of tracer glycine in one subject (details in the text)
Creatine kinetics
As shown above, creatine supplement caused an almost tenfold increase in plasma concentration of creatine in all subjects (Table 2). The kinetics of synthesis of creatine are shown in Table 6. Creatine administration significantly decreased the mean rate of appearance of tracer glycine in the creatine pool (slope) in the entire group (p = 0.005). However when examined separately by gender, the decrease was statistically significant only in the female subjects. The mean fractional rate of creatine synthesis, calculated based upon the enrichment of the GAA pool, was 27 % day−1 while on creatine-free diet and decreased to 18.6 % day−1 following creatine supplement (p = 0.007). The decrease was statistically significant only in the male subjects.
We estimated the size of the rapidly mixing pools of creatine by examining the kinetics of a bolus dose of [C2H3]creatine. As shown in Fig. 3 the dilution of the bolus dose of the tracer revealed bi-exponential kinetics suggesting two different pools or compartments of creatine, a small rapidly mixing pool and a large slowly mixing pool. The estimated sizes of the two pools (Q1 and Q2) are displayed in Table 6. As shown, while on creatine-free diet, Q1 was not significantly different in males and females and was approximately 1 mmole. In contrast, the second larger pool (Q2) was significantly smaller in the female subjects when compared with the males (mean 19.3 mmoles vs. 36.2 mmoles, respectively, p = 0.01). Creatine supplement caused a fivefold increase in the rapidly mixing pool (Q1) in both males and females and in the entire group while it did not cause a significant change in the larger creatine pool (Q2). Q2 remained significantly smaller in females when compared with the males, as was the case when on creatine-free diet. We calculated the rate of synthesis of creatine from the appearance of [13C]creatine (m1) in the larger creatine pool (Q2).

Time course of dilution of the bolus [C2H3]ctreatine in plasma of one subject is shown. Curve stripping was employed to calculate the size of the creatine pools
The absolute synthesis rate of creatine was significantly less in the female as compared with the male subjects (p = 0.01) while on creatine-free diet. Creatine supplement caused a significant decrease in the rate of creatine synthesis in the entire group (from 7.41 ± 4.22 mmoles d−1 to 5.16 ± 2.29 mmoles d−1, p = 0.02). The decrease in creatine synthesis was statistically significant only in the males.
Amino acid supplement did not have any effect on glycine, phenylalanine, or creatine kinetics (Data in supplemental tables).
Discussion
The data from the present study show that creatine supplement for 5 days, (1) caused a marked increase in plasma concentration of creatine and a decrease in plasma concentration of GAA in all subjects, (2) did not impact plasma creatinine levels or daily urinary excretion of creatinine, (3) caused a fivefold increase in the rapidly mixing creatine pool but had no impact on the larger slowly mixing pool, (4) caused a significant decrease in the rate of de-novo synthesis of glycine while it had no effect on whole body rate of appearance of phenylalanine, (5) caused a significant decrease in the rate of synthesis of creatine. Oral supplementation with amino acids for five days had no measurable effect on any of these parameters. It should be underscored that we examined the response to 5 days of creatine supplement in the fasting state and that these data cannot be extrapolated to prolonged continuous administration.
Homocysteine, cysteine and glutathione
Creatine supplement did not affect the concentration of total homocysteine in the plasma in our study (Table 3). This is in contrast to the previous data in humans where a small but significant decrease was observed in one study (Korzun 2004) and a non-significant decrease in another (Steenge et al. 2001). In contrast, Stead et al. observed a 25 % decrease in plasma levels of homocysteine in rats maintained on a creatine supplemented diet for two weeks (Stead et al. 2001). The decrease in plasma homocysteine concentration has been attributed to a decrease in the methylation demands and therefore decreases in transmethylation of methionine, as a result of creatine supplement (Stead et al. 2001). The lack of effect on plasma homocysteine in our study may be related to the short duration of creatine supplement, to a difference in the dose of creatine given; although the use of creatine-free diet in our study 1 by increasing the methylation demand should have made the effect of creatine supplement more evident. In the study by Korzun (2004) and by Steenge et al. (2001), creatine supplement was given, respectively, for 4 and 8 weeks. Additionally, since the decrease in plasma homocysteine has been attributed to decrease in methylation demand the decrease in creatine synthesis (20–40 %), in our study, may not have been enough to show any significant differences in plasma homocysteine. The physiological reason for the increase in plasma cysteine and glutathione following creatine supplement cannot be discerned from these data and may be related to changes in glutathione metabolism.
Amino acids
There was a significant decrease in plasma concentration of glycine in all subjects following creatine supplement, likely related to decreased demands for glycine for creatine synthesis (discussed below). The changes in plasma taurine, glutamine, and other amino acids may be the consequence of subtle and not measurable changes in the metabolism of the skeletal muscle or the result of changes in tissue osmolarity as a result of retention of water (Powers et al. 2003).
Creatine supplement had no effect on the whole body rate of protein turnover as measured by the rate of appearance of phenylalanine. These data are consistent with the previous studies in literature which did not show any significant effect of creatine supplement on protein metabolism in the skeletal muscle in vivo (Louis et al. 2003; Parise et al. 1985; Ingwall et al. 1974); although there was significant increase in the skeletal muscle creatine levels. Parise et al. (1985) did observe a decrease in whole body rate of appearance of leucine and its rate of oxidation, in response to creatine in men only and not in women. They attributed it to possible change in hepatic metabolism of leucine.
In contrast to no change in phenylalanine Ra, there was a significant decrease in the rate of appearance of glycine in the plasma (Table 5). The rate of decarboxylation of glycine (glycine cleavage system) also decreased following supplemental creatine although the fraction of serine derived from glycine was not changed. The lower Ra of glycine in the presence of unchanged whole body rate of proteolysis suggests a lower rate of de-novo synthesis of glycine. Although the exact mechanism of the decrease in the rate of synthesis of glycine cannot be discerned, it is likely to be related to the decrease in the requirement of glycine for creatine synthesis and to a decrease in methylation demand i.e., decrease in the need for the methyl group as a result of lower rate of creatine synthesis (Stead et al. 2001). As discussed by Melendez-Hevia and Paz-Lugo (2008) and by Hofmeyr and Cornish-Bowden (2000), the stoichiometry of glycine biosynthesis from serine via glycine hydroxyl methyl transferase and its disposal via consumption of C1 units transferred via THF, results in unique metabolic constraints so that the rate glycine biosynthesis cannot exceed the flux of consumption of the methyl groups via THF or that they are closely linked. Based upon this analysis, we attribute the lower rate of glycine synthesis following creatine supplement to the decrease in the demand for glycine and for methyl groups for creatine synthesis.
Guanidinoacetic acid
As reported by Derave et al. (2004) in healthy humans and by Edison et al. (2007) in rat and humans, oral creatine supplement, in the present study, caused a marked (50 %) decrease in the plasma concentration of GAA (Table 2). The decrease in plasma GAA has been attributed to decreased synthesis of GAA. We did not see a change in tracer enrichment of GAA following creatine supplement (Table 6) possibly because of a small size of the GAA pool and its rapid equilibrium and enrichment following tracer priming of the glycine pool. Since the glycine pool in the tissues is the only source of GAA and because of rapid equilibrium between glycine and GAA, a change in rate of synthesis of GAA will not be reflected in the tracer enrichment of plasma GAA. This was the case in our study (Fig. 2 and Table 6). The decrease in the synthesis of GAA has been attributed to pre-translation inhibition and to lower activity of AGAT in the kidney caused by supplemental creatine (McGuire et al. 1984). In the rat, most of the GAA is produced in the kidney (Edison et al. 2007). Creatine supplement in the rat suppressed the synthesis of GAA in the kidney by decreasing both the amount of protein and the activity of AGAT (Edison et al. 2007). There was a close correlation between the rate of production of GAA by the kidney and urinary rate of excretion of creatinine further providing evidence for the kidney to be the major site of GAA synthesis in the rat (Edison et al. 2007). These data have been interpreted to suggest that at least in the rat there is an inter-organ synthesis of creatine, whereby GAA is synthesized in the kidney, released into circulation and converted to creatine in the liver. In contrast in humans, the renal production of GAA amounted to only 11–12 % of creatinine excretion by the kidney. The authors interpreted these data to suggest that in humans, GAA is possibly produced at sites other than the kidney (Edison et al. 2007). Such an inference is also suggested by the presence of AGAT in organs other than the kidney (Wyss and Kaddurah-Daouk 2000).
The slow linear increase in 13C enrichment (m1) of the GAA in the plasma (average slope moles % excess = 0.002/min) suggests multiple heterogeneous pools of GAA in different organs and tissues of varying size and kinetics as well as the differences in intracellular glycine flux and pools in different organs (Arends et al. 1995; Garfinkel and Lajtha 1963). These data are consistent with the study of Edison et al. (2007) who showed that unlike in rats, in humans only a small proportion of whole body GAA is synthesized in the kidney and released into the circulation.
Creatine
Plasma creatine concentration increased almost ten-fold following supplemental creatine. The creatine levels in the plasma were measured in the fasting state, ten to twelve hours after the last creatine dose. These data are similar to those reported by Brault et al. (2007). Corresponding to increase in plasma creatine, there was a fivefold increase in the rapidly mixing creatine pool (Q1) in all subjects (Table 6). The estimated volume of distribution of Q1 was approx. 35 % of the body weight suggesting distribution in little more than extracellular compartment. Interestingly, the larger slow mixing pool (Q2) did not change following creatine supplement. This may be related to mixing with the intracellular pools of creatine. The calculated size of the creatine pools is likely an under-estimation because of loss/excretion of some of the bolus tracer creatine in the urine prior to mixing in the entire pool. This is particularly true following creatine supplementation (Harris et al. 1992; Burke et al. 2001; Rawson et al. 2004) when the concentration of creatine in the plasma was high. Previous data in the literature show that as much as 30–40 % of the creatine supplement is excreted in the urine (Harris et al. 1992; Burke et al. 2001). We could not correct for this loss because we had not obtained timed urine collections. In addition, the multi-compartmental distribution of creatine and the regulation of its uptake by its transporter create some inherent problems for the estimation of pool size of creatine (Eloot et al. 2005; Snow and Murphy 2001). Although the plasma concentration of creatine increased markedly in all subjects, the larger creatine pool (Q2) increased, not significant, only in the females, a group with the smaller initial creatine pool compared with the males. Interestingly, the female subjects also showed a significant increase in body weight following creatine supplement, likely related to the retention of water in the body (Powers et al. 2003). The absolute rate of synthesis of creatine in female subjects, while on creatine-free diet, was ~50 % of that of male subjects (Table 6). The estimated muscle mass of the female subjects was also ~50 % of that of males (Table 1). Even though the fractional rate of synthesis of creatine decreased in all subjects, the absolute rate of synthesis decreased in males only. This was related to unchanged creatine pool in males and an increase in the creatine pool in females.
Our estimates of the rate of synthesis of creatine are the first detailed analysis in young healthy men and women. The measured rates of creatine synthesis for men (1.3 gms d−1), while on creatine-free diet although comparable with those in literature, are less than those reported (1.6 gms day−1). We could not find similar measurements for women. Previous data on a small group of subjects, mostly men, have used the rate of excretion of creatinine and creatine in the urine, organ balance data, or 15N, 13C, or 14C labeled tracers of creatine to estimate the rate of creatine synthesis (Cockcroft and Gault, 1976; Sandberg et al. 1953; Hoberman et al. 1948a, b; Crim et al. 1976; Kreisberg et al. 1970). Cockcroft and Gault (1976) measured the rate of creatinine excretion in 22 male subjects age 18–29 years to be ~24 mg kg−1 24 h−1 corresponding to ~1.6 gms d−1 for a 70 kg person. These measurements could be overestimates since urinary creatine excretion has been reported to be directly related to dietary creatine intake and these subjects were not on creatine-free diet. The studies using organ balance data and those using tracer labeled creatine were done on a small group of men, one to four subjects, and gave variable results (Hoberman et al. 1948a, 1948b; Crim et al. 1976). In contrast to the studies in literature, we studied both men and women over a short duration and observed less variability than that seen in previous tracer studies. The short duration of the study and ease of analysis allows for examination of effects of other nutritional and metabolic interventions. In addition, we studied subjects only in the fasting state, while the reported data in literature includes both fasting and fed state. The effect of feeding and dietary nutrient intake on creatine synthesis has not been explored in detail.
Our data confirm the estimates by Brosnan and colleagues, regarding metabolic burden of creatine synthesis on labile methyl groups provided by S-adenosylmethionine (Brosnan et al. 2011). Based upon measured transmethylation flux of 16.3mmoles per day for a 70 kg person (MacCoss et al. 2001), our data suggest that creatine synthesis consumes approximately 45 % of the S-adenosylmethionine generated in the transmethylation flux of methionine. This estimate is similar to the 40 % calculated by Brosnan et al. (2011).
Potential weaknesses
Since we did not supply the food when the subjects were on creatine-free diet, it is possible that they may not have adhered to the diet rigorously. This would result in an underestimation of rate of creatine synthesis. Even though we did monitor for dietary compliance by frequent contacts, one male subject appeared to have not taken creatine since his plasma creatine concentration remained unchanged following supplement creatine. We did include his data in the reported analysis.
References
Adams RF (1974) Determination of amino acid profiles in biological samples by gas chromatography. J Chromatogr 95:189–212
Arends J, Schafer G, Schauder P, Bircher J, Bier DM (1995) Comparison of serine and hippurate as precursor equivalents during infusion of [15 N]glycine for measurement of fractional synthetic rates of apolipoprotein B of very-low-density lipoprotein. Metabolism 44:1253–1258
Brault JJ, Towse TF, Slade JM, Meyer RA (2007) Parallel increases in phosphocreatine and total creatine in human vastus lateralis muscle during creatine supplementation. Int J Sport Nutr Exerc Metab 17:624–634
Brosnan JT, Brosnan ME (2007) Creatine: endogenous metabolite, dietary, and therapeutic supplement. Annu Rev Nutr 27:241–261
Brosnan JT, da Silva RP, Brosnan ME (2011) The metabolic burden of creatine synthesis. Amino Acids 40:1325–1331
Burke DG, Smith-Palmer T, Holt LE, Head B, Chilibeck PD (2001) The effect of 7 days of creatine supplementation on 24-hour urinary creatine excretion. J Strength Cond Res 15:59–62
Clarys JP, Martin AD, Drinkwater DT (1984) Gross tissue weights in the human body by cadaver dissection. Hum Biol 56:459–473
Cockcroft DW, Gault MH (1976) Prediction of Creatine clearance from serum creatinine. Nephron 16:31–41
Crim MC, Calloway DH, Margen S (1976) Creatine metabolism in men: creatine pool size and turnover in relation to creatine intake. J Nutr 106:371–381
da Silva RP, Nissim I, Brosnan ME, Brosnan JT (2009) Creatine synthesis: hepatic metabolism of guanidinoacetate and creatine in the rat in vitro and in vivo. Am J Physiol Endocrinol Metab 296:E256–E261
Dangott B, Schultz E, Mozdziak PE (2000) Dietary creatine monohydrate supplementation increases satellite cell mitotic activity during compensatory hypertrophy. Int J Sports Med 21:13–16
Dasarathy S, Kasumov T, Edmison JM, Gruca LL, Bennett C, Duenas C, Marczewski S, McCullough AJ, Hanson RW, Kalhan SC (2009) Glycine and urea kinetics in nonalcoholic steatohepatitis in human: effect of intralipid infusion. Am J Physiol Gastrointest Liver Physiol 297:G567–G575
Derave W, Marescau B, Vanden Eede E, Eijnde BO, De Deyn PP, Hespel P (2004) Plasma guanidino compounds are altered by oral creatine supplementation in healthy humans. J Appl Physiol 97:852–857
Edison EE, Brosnan ME, Meyer C, Brosnan JT (2007) Creatine synthesis: production of guanidinoacetate by the rat and human kidney in vivo. Am J Physiol Renal Physiol 293:F1799–F1804
Eloot S, Torremans A, De SR, Marescau B, De WD, De Deyn PP, Lameire N, Verdonck P, Vanholder R (2005) Kinetic behavior of urea is different from that of other water-soluble compounds: the case of the guanidino compounds. Kidney Int 67:1566–1575
Garfinkel D, Lajtha A (1963) A metabolic inhomogeneity of glycine in vivo. I. Experimental determination. J Biol Chem 238:2429–2434
Harris RC, Soderlund K, Hultman E (1992) Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci (Lond) 83:367–374
Hoberman HD, Sims EA, Peters JH (1948a) Creatine and creatinine metabolism in the normal male adult studied with the aid of isotopic nitrogen. J Biol Chem 172:45–58
Hoberman HD, Sims EA, Engstrom WW (1948b) The effect of methyltestosterone on the rate of synthesis of creatine. J Biol Chem 173:111–116
Hofmeyr JS, Cornish-Bowden A (2000) Regulating the cellular economy of supply and demand. FEBS Lett 476:47–51
Ingwall JS, Weiner CD, Morales MF, Davis E, Stockdale FE (1974) Specificity of creatine in the control of muscle protein synthesis. J Cell Biol 62:145–151
Kalhan SC, Rossi KQ, Gruca LL, Super DM, Savin SM (1998) Relation between transamination of branched-chain amino acids and urea synthesis: evidence from human pregnancy. Am J Physiol 275:E423–E431
Kalhan SC, Edmison J, Marczewski S, Dasarathy S, Gruca LL, Bennett C, Duenas C, Lopez R (2011) Methionine and protein metabolism in non-alcoholic steatohepatitis: evidence for lower rate of transmethylation of methionine. Clin Sci (Lond) 121:179–189
Kasumov T, Gruca LL, Dasarathy S, Kalhan SC (2009) Simultaneous assay of isotopic enrichment and concentration of guanidinoacetate and creatine by gas chromatography-mass spectrometry. Anal Biochem 395:91–99
Korzun WJ (2004) Oral creatine supplements lower plasma homocysteine concentrations in humans. Clin Lab Sci 17:102–106
Kreisberg RA, Bowdoin B, Meador CK (1970) Measurement of muscle mass in humans by isotopic dilution of creatine-14C. J Appl Physiol 28:264–267
Louis M, Poortmans JR, Francaux M, Hultman E, Berre J, Boisseau N, Young VR, Smith K, Meier-Augenstein W, Babraj JA, Waddell T, Rennie MJ (2003) Creatine supplementation has no effect on human muscle protein turnover at rest in the postabsorptive or fed states. Am J Physiol Endocrinol Metab 284:E764–E770
MacCoss MJ, Fukagawa NK, Matthews DE (2001) Measurement of intracellular sulfur amino acid metabolism in humans. Am J Physiol Endocrinol Metab 280:E947–E955
McGuire DM, Gross MD, Van Pilsum JF, Towle HC (1984) Repression of rat kidney l-arginine:glycine amidinotransferase synthesis by creatine at a pretranslational level. J Biol Chem 259:12034–12038
Melendez-Hevia E, Paz-Lugo PD (2008) Branch-point stoichiometry can generate weak links in metabolism: the case of glycine biosynthesis. J Biosci 33:771–780
Olsen S, Aagaard P, Kadi F, Tufekovic G, Verney J, Olesen JL, Suetta C, Kjaer M (2006) Creatine supplementation augments the increase in satellite cell and myonuclei number in human skeletal muscle induced by strength training. J Physiol 573:525–534
Parise G, Mihic S, MacLennan D, Yarasheski KE, Tarnopolsky MA (1985) Effects of acute creatine monohydrate supplementation on leucine kinetics and mixed-muscle protein synthesis. J Appl Physiol 91(1041–1047):2001
Powers ME, Arnold BL, Weltman AL, Perrin DH, Mistry D, Kahler DM, Kraemer W, Volek J (2003) Creatine supplementation increases total body water without altering fluid distribution. J Athl Train 38:44–50
Rawson ES, Persky AM, Price TB, Clarkson PM (2004) Effects of repeated creatine supplementation on muscle, plasma, and urine creatine levels. J Strength Cond Res 18:162–167
Sandberg AA, Hecht HH, Tyler FH (1953) Studies in disorders of muscle. X. The site of creatine synthesis in the human. Metabolism 2:22–29
Snow RJ, Murphy RM (2001) Creatine and the creatine transporter: a review. Mol Cell Biochem 224:169–181
Stead LM, Au KP, Jacobs RL, Brosnan ME, Brosnan JT (2001) Methylation demand and homocysteine metabolism: effects of dietary provision of creatine and guanidinoacetate. Am J Physiol Endocrinol Metab 281:E1095–E1100
Steenge GR, Verhoef P, Greenhaff PL (2001) The effect of creatine and resistance training on plasma homocysteine concentration in healthy volunteers. Arch Intern Med 161:1455–1456
Teuscher N (2011) What is curve stripping? http://learnpkpd.com/2011/07/06/what-is-curve-stripping/. Accessed 15 Aug 2014
Vierck JL, Icenoggle DL, Bucci L, Dodson MV (2003) The effects of ergogenic compounds on myogenic satellite cells. Med Sci Sports Exerc 35:769–776
Wyss M, Kaddurah-Daouk R (2000) Creatine and creatinine metabolism. Physiol Rev 80:1107–1213
Acknowledgments
The authors greatly appreciate the support provided by the nursing staff, the core lab staff, and by the research dietitian of the Cleveland Clinic Clinical Research Unit. This work was supported by the 3ARP grant from Ajinomoto Inc and by the Clinical & Translational Science Award, RR024989 to Case Western Reserve University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest in relation to the work presented in this manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Kalhan, S.C., Gruca, L., Marczewski, S. et al. Whole body creatine and protein kinetics in healthy men and women: effects of creatine and amino acid supplementation. Amino Acids 48, 677–687 (2016). https://doi.org/10.1007/s00726-015-2111-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00726-015-2111-1