
Abstract
Background
Aneurysmal subarachnoid haemorrhage is associated with significant morbidity and mortality due to the myriad of complications contributing to early brain injury and delayed cerebral ischaemia. There is increasing interest in the exploration of the association between blood-brain barrier integrity and risks of delayed cerebral ischaemia and poor outcomes. Despite recent advances in cerebral imaging, radiographic imaging of blood-brain barrier disruption, as a biomarker for outcome prediction, has not been adopted in clinical practice.
Methods
We performed a narrative review by searching for articles describing molecular changes or radiological identification of changes in BBB permeability following subarachnoid haemorrhage (SAH) on MEDLINE. Preclinical studies were analysed if reported structural changes and clinical studies were included if they investigated for radiological markers of BBB disruption and its correlation with delayed cerebral ischaemia.
Results
There is ample preclinical evidence to suggest that there are structural changes in BBB permeability following SAH. The available clinical literature has demonstrated correlations between permeability imaging and outcomes following aneurysmal subarachnoid haemorrhage (aSAH).
Conclusion
Radiological biomarkers offer a potential non-invasive prognostication tool and may also allow early identifications of patients who may be at risk of DCI.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Aneurysmal subarachnoid haemorrhage (aSAH) accounts for approximately 80% of spontaneous non-traumatic SAH presentations. It accounts for up to 5% of all new stroke presentations and 5% of deaths from stroke, with a mean age at presentation of 55 years and an increase in incidence with age [50, 74]. The common complications associated with aSAH include re-bleeding in the acute period before definitive aneurysm treatment, hydrocephalus, cerebral vasospasm, delayed cerebral ischaemia, seizures, hyponatraemia, myocardial injuries and pulmonary oedema. Several factors are also associated with poor outcomes following aSAH including age, poor WFNS grade, delayed cerebral ischaemia and radiological haemorrhage burden.
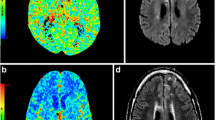
Delayed cerebral ischaemia, defined as the development of new focal neurological deficit(s) or radiological evidence of new infarction(s), occurs in up to a third of patients following the onset of aSAH and can result in significant morbidity and mortality [75]. The presence of thick cisternal blood and intraventricular haemorrhage (modified Fisher grade IV) increases the risk of a poor outcome for patients, with up to 40% risk of delayed cerebral ischaemia compared to computed tomography (CT)-negative aSAH (Fig. 1) [15]. Mean cerebral blood flow (CBF) has been shown to be significantly lower in patients with Fisher III–IV and poor-grade aSAH patients in comparison to patients with better clinical grades [86]. Historically, the terms “delayed cerebral ischaemia” (DCI) and “cerebral vasospasm” had been used interchangeably. This was because the mechanical relationship between narrowed blood vessels, reduced blood flow and cerebral ischaemia was thought to be intuitive. DCI, however, has now been shown to occur independent of cerebral vasospasm. In a study by Dankbaar et al., vasospasm, evident on CT angiography, was reported to correspond with the least perfused regions of the brain in only two-thirds of patients on CT perfusion. DCI was also evident in some patients who had no radiological evidence of vasospasm [18]. Furthermore, oral administration of nimodipine, an L-type calcium channel antagonist, has been shown to reduce the risk of DCI and poor outcome following aSAH [57]. However, this effect has not been shown to correlate with significant reduction in angiographic vasospasm in the patients administered nimodipine [3, 22]. There is also experimental evidence that the presence of oxyhaemoglobin in the perivascular and subarachnoid spaces results in the release of endothelin from the arterial walls. This response has been implicated in the pathogenesis of vasospasm, due to the effects of endothelin on vasoconstriction. These findings prompted the CONSCIOUS trials (clazosentan to overcome neurological ischaemia and infarct occurring after subarachnoid haemorrhage) which assessed the effect of clazosentan on mortality and DCI. Clazosentan is an endothelin receptor antagonist with a molecular weight of 577.6 Da. In the CONSCIOUS trials, its efficacy and safety at three doses (1, 5 and 15 mg/h) on the prevention of vasospasm and DCI was assessed. There was a dose-dependent reduction in moderate and severe angiographic cerebral vasospasm with a 65% relative risk reduction at 15 mg/h. However, there was no significant effect on mortality, vasospasm-related neurological complications and functional outcomes [45,46,47], further supporting that the pathogenesis of DCI is not fully a result of vasoconstriction. Other factors, such as microcirculatory constriction, micro-thrombosis, platelet aggregation, cortical spreading ischaemia, delayed cellular apoptosis, neuroinflammation and increased blood-brain barrier (BBB) permeability, have been hypothesised as potential contributors to the pathophysiology of DCI [23, 26, 58, 66]. As a result, various multimodal monitoring systems such as continuous EEG, brain tissue oxygen, intracranial pressure (ICP) and imaging modalities such as transcranial Doppler ultrasound, CT perfusion (CTP) and digital subtraction angiography (DSA) have been used in early identification and response to treatment of vasospasm and cerebral ischaemia. Several preclinical studies have demonstrated increased permeability of the BBB, at various time courses after subarachnoid haemorrhage, and its implications on early brain injury and DCI [40, 66]. However, there has been limited use of BBB imaging in clinical practice for the prediction and prognostication of DCI following aSAH. In this review, we discuss some of the mechanisms involved in BBB disruption following aSAH and the potential role of BBB integrity imaging in prediction of DCI and outcome prognostication following aSAH.

a, b Axial CT brain obtained at presentation, showing Fisher IV aSAH (diffuse SAH (asterisk) with IVH (white arrow); c, d Axial DWI MRI sequences obtained day 7 post-ictus showing areas of bi-hemispheric and pontine diffusion restriction representing infarction (white arrows); e, f Digital subtraction angiography (DSA) of cerebral vessels (e antero-posterior view, f lateral view) obtained on the day of presentation showing anterior communicating artery aneurysm (black arrow on image e) with no significant large vessel vasospasm; g, h DSA of cerebral vessels (g antero-posterior view, h lateral view) obtained on day 7 prior to balloon angioplasty, showing severe right middle cerebral artery (black arrow) and anterior cerebral artery (white arrow) vasospasm
Methods
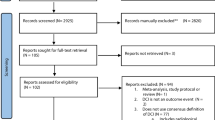
A systematic review of the literature was performed to identify peer-reviewed literature reporting association of radiological evidence of blood-brain barrier integrity with clinical or radiological outcomes following aSAH in humans. The approach for reporting was modelled on the PRISMA guidelines (Fig. 2). We conducted a literature search using the PubMed/MEDLINE database using the search terms “(subarachnoid haemorrhage OR SAH) AND (blood-brain barrier OR BBB) AND (magnetic resonance imaging OR MRI OR computed tomography OR CT OR imaging)”. Abstracts were screened for investigations of association of radiological evidence of BBB permeability and clinical or radiological outcomes pertaining to DCI. Eight studies were included in the qualitative synthesis of the literature, presented as a narrative review describing the utility of permeability imaging in predicting DCI or poor outcomes in humans with aSAH [20, 34,35,36, 38, 43, 48, 62].

PRISMA flow diagram
Disruptions to the blood-brain barrier in SAH
The basic anatomical structure of the BBB is a single layer of microvascular endothelial cells (ECs), lining the lumen of cerebral capillaries, supported by ensheathing pericytes and the foot processes of astrocytes (Fig. 3) [1, 14]. This complex network of cells restricts movement into the brain to lipophilic molecules with a molecular weight less than approximately 400 Da. The EC layer consists of luminal (blood-side) and abluminal (brain-side) membranes separated by ≈ 500 nm of cytoplasm. Cerebral ECs differ, morphologically, from peripheral ECs in 2 respects: (1) the presence of fluid-filled pinocytes and higher concentration of mitochondria in their cytoplasm, highlighting the important transport requirements and function of the BBB. (2) The high electrical resistance across the ECs is established in part by complex tight junctions (TJs) connecting neighbouring ECs [53]. Tight junctions play an important role in maintaining the integrity of the BBB through very intimate, but gated, membrane apposition of neighbouring ECs. Proteins, such as claudins, occludins and zonula occludens (ZO), are expressed in rodent embryos shortly after cerebral angiogenesis, as early as day 12 of embryogenesis [17]. These proteins, with their connections, form a junctional complex with structural integrity to regulate transport of solutes through the paracellular pathway in and out of the brain. Increased BBB permeability has been demonstrated in rodent models with decreased expression of claudin-5. Likewise, upregulating the expression of claudin-5 at the BBB has been associated with reduced cerebral oedema and haemorrhagic transformation of the focal area of cerebral ischaemia in mice [33, 51].

Brief overview of cellular and molecular structure of the blood-brain barrier
Occludin is another integral membrane and TJ-associated component of the BBB, with expression reported in various mammals. Although its function in the BBB is still not fully understood, the expression of occludin has been shown to be modified when exposed to conditions such as hypoxia/reoxygenation, matrix metalloproteinase 9 (MMP-9) activation and interleukins (IL), amongst others [9, 37, 78, 79]. Initially, a fence-barrier function was suggested; however, occludin-deficient stem cells had the potential to differentiate into epithelial cells with functioning tight junctions [64].
Changes in the integrity of the BBB have been implicated in a number of neurological conditions, e.g. Alzheimer-associated dementias, TBI and stroke. BBB disruption, in the acute setting after subarachnoid haemorrhage, was reported by Doczi in 1985, showing some correlations between abnormal post-contrast enhancement on CT, vasospasm and poor clinical outcomes [19]. There have been a number of preclinical studies confirming the impairment of BBB integrity since this study. Changes in the BBB have been observed as early as 10 minutes after SAH, evident by partial degradation of the basal lamina and platelet migration across abluminal membranes of ECs in experimental rat models of SAH [26]. The exact mechanism of BBB disruption following SAH remains poorly understood; however, a number of microvascular alterations have been reported in the literature.
One of the reported microvascular changes in the structure of the BBB in SAH is the focal destruction of collagen. Immunohistochemical studies of cerebral arteries in animal models of SAH have shown degradation of type IV collagen in the basal lamina [55, 67, 68]. This effect was not limited to the outer cortex exposed to subarachnoid blood. There was also a correlation between the observed collagen degradation and BBB dysfunction, as demonstrated by increased serum albumin content in the cortex of the animals in this cohort [67]. In normal physiological state, extravasation of albumin is limited by the BBB. The matrix metalloproteinase (MMP) system has been thought to contribute to the disruption of type IV collagen in a number of cerebral pathologies. Correlations have been established between a reduction in type IV collagen immune staining with increased matrix metalloproteinase 9 staining, as early as 3 hours after SAH [5, 54, 68]. A decrease in other basal lamina proteins, such as laminin, has also been reported in the context of SAH [77]. A correlation in the timing of basal lamina degradation and the increase in brain water further supports its role in early global vasogenic cerebral oedema following SAH [67, 76].
There has been a growing understanding of changes in the expression of BBB tight junction proteins in response to SAH. Experiments in rat models have reported alterations in expressions of claudin-5 [4, 8, 10, 11, 13, 24, 25, 32, 40, 44, 54, 60], occludin [4, 11, 13, 24, 27, 29, 30, 32, 40, 42, 44, 54, 60, 77, 80, 81, 84, 85] and ZO-1 [4, 11, 13, 24, 27, 29, 30, 32, 40, 42, 44, 54, 59, 60, 73, 77, 80, 81, 83,84,85] within 24–48 hours of exposure to SAH. While most studies have generally found a concurrent decrease in the expression of these proteins, Li et al. reported no decrease in claudin-5 expression. The temporal change in the expression of these proteins has also been explored in a few studies. While most studies have reported a monophasic decrease in TJ protein expression, Li et al. reported a biphasic response with decreased levels of ZO-1 and occludin [40]. Blecharz-Lang et al. showed a decrease in mRNA transcripts and protein expression for claudin-5 and vascular endothelial cadherin (VE-cadherin) at 8 hours and 24 hours following induction of SAH. However, although transcript levels of occludin remain unchanged at 8 hours, there was an increase in the protein expression. At 24 and 48 hours, there was a concurring decrease in both transcript and protein expressions of occludin [4]. The expression of other less-studied tight junction proteins, such as VE-cadherin, has also been shown to decrease following SAH [4, 29]. Interestingly, similar effects on basement membranes in extracranial organs have been described following experimental SAH in animals. These effects also seem to occur as a result of the same pathways reported in the BBB [12, 28].
BBB permeability imaging as a predictor of DCI
Global cerebral oedema (GCE), thought to be partially a result of increased BBB permeability, has been shown to be an independent predictor of morbidity and mortality in subarachnoid haemorrhage [16, 39]. A non-contrast computed tomography (CT) imaging of the brain can provide an easily accessible evaluation of cerebral oedema following aSAH. Although GCE may result from secondary pathological pathways leading to either increased brain water content or hyperaemia, the former has been demonstrated to correlate with regions of CT hypodensity more than the latter [49, 61]. This coupled with the concurrent increase of brain water content and structural changes in the BBB in preclinical studies supports the potential role of NCCT brain in the gross analysis of BBB integrity following aSAH in clinical practice [67, 76]. CT perfusion has been utilised in the assessment of alterations in cerebral perfusion in the context of delayed cerebral ischaemia, with prolonged mean transit time (MTT) and reduced cerebral blood flow (CBF) being prognostic indicators for DCI [65]. Following on from this, a number of recent studies have analysed the correlations between DCI and global cerebral ischaemia with the severity of BBB permeability, using CT perfusion (CTP). The main measurable radiological parameter in permeability imaging is Ktrans (Fig. 4). Ktrans represents a measurement of capillary associated signal change after injection of a contrast agent and reflects the kinetic diffusion of this tracer across the BBB-associated endothelium. It represents the sum of all the processes contributing to the net rate of the influx of contrast agent from the intravascular space into the extravascular extracellular space EES. Ve denotes the volume of EES per unit volume of tissue, representing the potential volume of interstitium that can be occupied by the contrast agent. Similarly, Vp represents the fractional volume of plasma (intravascular space). Kep is the time constant for contrast agent reflux from EES back into intravascular space, which is dependent on the former parameters, and permeability surface (PS) area product, representing flow from plasma to EES. Due to the selectivity of passage across an intact BBB, any observed change in BBB integrity is also significantly dependent on the molecular weight of the tracer (contrast agent) used. Ivanidze et al. analysed these parameters retrospectively from CTP in matched SAH patients who had radiological evidence of global cerebral oedema (GCE) and those who did not, within 72 hours of onset of SAH symptoms. They observed statistically significant decreased Ktrans, kep, and vp and increased Ve in the GCE group in comparison to non-GCE group [35]. The paradoxical decrease in Ktrans observed was attributed to the dependence of the derivation of Ktrans on cerebral blood flow rate, which can be reduced in the context of global cerebral oedema, likely as a result of elevated intracranial pressure. Subsequent studies have found correlations between increased PS and Ve and decreased kep and functional outcomes after SAH [34, 36].

Simple illustrations of compartments and radiological parameters commonly utilised in blood-brain barrier permeability imaging
One of the earliest reports of abnormal contrast enhancements, following aSAH, was by Doczi et al. [20]. The author described the utility of the quantitative measurement and comparison of Hounsfield units (HU) in regions of interest between NCCT brain and contrast-enhanced CT studies. The confinement of contrast agent by an intact BBB results in a slight increase in density of the cerebral parenchyma, since the cerebral blood volume represents 4–5% of the total brain volume. Therefore, normal white and grey matter exhibit a very slight hyper-attenuation in contrast-enhanced CT, on average, 1.9 HU for grey matter and 1.4 H for white matter. Hence, a significant increase in enhancement, to the effect of 4.5 HU, is considered evidence for abnormal permeability [63, 70, 71]. With analysis based on this threshold, Doczi et al. observed that 40% patients who had a post-contrast CT brain within 5 days of aSAH demonstrated abnormal enhancements, while 31% of patients scanned later than 5 days showed abnormal contrast enhancement. The enhancing regions were noted to be parenchymal suggesting disruption in BBB as an underlying factor. Interestingly, the authors reported a relationship between abnormal enhancements and outcome, such as infarction (DCI) and re-bleed, although the statistical significance of this finding is uncertain, given the small sample size [20].
Magnetic resonance imaging (MRI) is superior to CT for assessing tissue properties and subtle changes in regions of interest, although limited by longer time of image acquisition in comparison to CT. MRI has been used for the investigation of BBB permeability in a range of neurological conditions, i.e. neoplasm, TBI, neurodegenerative disorders, stroke and intra-cerebral haemorrhage [2, 31]. The basic principle of investigating BBB permeability using contrast-enhanced MRI is based on the potential of transmembrane efflux of paramagnetic contrast agents, typically gadolinium, from intravascular space, depending on degree of BBB disruption. Statistical differences in images before and after administration of contrast agents can be calculated in a static or dynamic fashion. One approach for evaluation of BBB integrity in preclinical and clinical studies using static contrast-enhanced MRI is the “post-pre” comparison method. This method uses enhancement differences between certain tissues with varying membrane permeability (muscle (permeable, no BBB), blood vessel and eyeball (intact blood-retina barrier)), as references for statistical calculations. For example, if the pre-contrast intensity of a region of interest (ROI) was in the range between the eyeball and blood vessel and there is a significant change in its intensity after contrast administration, this ROI is considered as a permeable brain region. A slice-wise paired t-test is performed to identify any statistically significant differences in the pre- and post-contrast images for specific pixels in the ROI [6, 7]. Dynamic contrast-enhanced MRI (DCE-MRI) on the other hand is used to quantify BBB permeability by monitoring changes in tracer/contrast agent concentration, over a longer period of time, on repeated scans after administration of the contrast agent. There are a number of tracer-kinetic models described in the literature (Patlak, one compartment, Tofts, steady state, etc.), with Tofts model most commonly used. A “linear dynamic method” was proposed by Chassidim et al., whereby linear slopes of scans taken at multiple time points after contrast agent administration are analysed [7]. Detailed descriptions of commonly used preclinical and clinical models have been described by Sourbron et al. [72]. A number of studies predominantly preclinical have utilised non-contrast-enhanced MRI, i.e. T2 hyperintensity analysis, in the investigation of BBB permeability [11, 56, 82]. Lin et al. proposed a non-contrast water-extraction-with-phase-contrast-arterial-spin-tagging (WEPCAST) sequence as an alternative to contrast-enhanced studies. This was achieved by manipulation and modelling water signals using selective detection of arterial spin labelling signals [41].
A prospective cohort study by Serlin et al. reported an association of BBB disruption with development of recurrent cerebral infarction. They presented a case whereby a patient presenting with transient ischaemic attack (TIA) was re-admitted after a few days with a diffusion weighted imaging (DWI) positive ischaemic stroke in areas that had previously been DWI negative at initial presentation, however demonstrated radiological (DCE-MRI) evidence of BBB disruption [69]. This highlights the potential for use of BBB disruption as a radiological biomarker, in conjunction with clinical history and signs, for prediction and prognostication in various neurological pathologies. BBB disruption has also been implicated in the sequelae of mild repetitive traumatic brain injury [21]. DCE-MRI has been used to demonstrate dynamic alterations in BBB integrity following exposure to varying levels of repetitive head trauma in mixed martial arts (MMA) fighters and rugby players [52]. There are, however, currently limited clinical studies exploring MRI changes in BBB following SAH [43, 62].
BBB disruption, measured radiologically with DCE-MRI, has been associated with poor outcomes following subarachnoid haemorrhage in a clinical study. Using the Patlak linear regression analysis, Russin et al. observed significantly higher Ktrans values (2.28 ± 0.09 × 10−3 min−1) in patients who subsequently developed DCI when compared to patients with radiographic only vasospasm (1.85 ± 0.12 × 10−3 min−1; p < 0.05) or no vasospasm/ischaemia (1.74 ± 0.07 × 10−3 min−1; p < 0.01), with ROC curve analysis showing Ktrans from DCE-MRI as an accurate radiological predictor of DCI [62]. A larger series by Lublinsky et al. also reported significant correlation between radiological quantification of BBB permeability and outcomes following aSAH. The post-imaging acquisition analysis used was the “post-pre” method described by Chassidim et al. The authors described abnormal brain tissue (ABT) as regions of apparently abnormal MRI signal (i.e. cytotoxic/vasogenic oedema, gliosis or haemorrhage). Interestingly, most voxels with BBBD were found in apparently normal brain tissue (NBT) and these were located within 1 cm from the core of a voxel of ABT. The extent of BBBD in ABT was associated with poor WFNS grades. There were no significant temporal changes in degree of BBBD in NBT between images acquired within 48 hours (t1) up to 19 days (t2 and t3) (Table 1), although some improvement was observed after 19 days (t4). On the other hand, worsening BBBD was observed in ABT at t2 and t3 with subsequent improvement at t4. As well as describing a temporal pattern of BBB changes, the serial DCE-MRI method used in this study demonstrated a significantly higher probability of transformation of NBT with BBBD to ABT, on follow-up imaging, when compared to initially intact voxels at t1. The degree of BBBD in both NBT and ABT was significantly larger in patients with poorer extended Glasgow outcome scores and the inclusion of BBBD in predictive algorithms improved predictive accuracy for outcomes than when only traditional factors such as age and WFNS grades were used [43].
Conclusion
There is sufficient evidence from preclinical studies to suggest that alterations to the permeability of the BBB play a crucial role in the complex pathophysiology of DCI following SAH. Radiological biomarkers offer a potential non-invasive prognostication tool and may also allow early identifications of patients who may be at risk of DCI. Radiological evidence of BBB breakdown has been demonstrated in humans in a wide variety of neurological disorders, particularly, neurodegenerative conditions and TBI. However, there is currently a paucity of human studies investigating the association between BBB dysfunction and its severity, with the severity of delayed cerebral ischaemia and overall patient outcomes. With the recent advances in permeability imaging, it is imperative that potential associations between BBB disruption and early and delayed brain injuries are investigated in patients with aSAH.
References
Alluri H, Wiggins-Dohlvik K, Davis ML, Huang JH, Tharakan B (2015) Blood-brain barrier dysfunction following traumatic brain injury. Metab Brain Dis 30:1093–1104. https://doi.org/10.1007/s11011-015-9651-7
Barzo P, Marmarou A, Fatouros P, Corwin F, Dunbar J (1996) Magnetic resonance imaging-monitored acute blood-brain barrier changes in experimental traumatic brain injury. J Neurosurg 85:1113–1121. https://doi.org/10.3171/jns.1996.85.6.1113
Bederson JB, Connolly ES Jr, Batjer HH, Dacey RG, Dion JE, Diringer MN, Duldner JE Jr, Harbaugh RE, Patel AB, Rosenwasser RH (2009) Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 40:994–1025. https://doi.org/10.1161/strokeaha.108.191395
Blecharz-Lang KG, Wagner J, Fries A, Nieminen-Kelha M, Rosner J, Schneider UC, Vajkoczy P (2018) Interleukin 6-mediated endothelial barrier disturbances can be attenuated by blockade of the IL6 receptor expressed in brain microvascular endothelial cells. Transl Stroke Res 9:631–642. https://doi.org/10.1007/s12975-018-0614-2
Cao S, Zhu P, Yu X, Chen J, Li J, Yan F, Wang L, Yu J, Chen G (2016) Hydrogen sulfide attenuates brain edema in early brain injury after subarachnoid hemorrhage in rats: Possible involvement of MMP-9 induced blood-brain barrier disruption and AQP4 expression. Neurosci Lett 621:88–97. https://doi.org/10.1016/j.neulet.2016.04.018
Chassidim Y, Vazana U, Prager O, Veksler R, Bar-Klein G, Schoknecht K, Fassler M, Lublinsky S, Shelef I (2015) Analyzing the blood-brain barrier: the benefits of medical imaging in research and clinical practice. Semin Cell Dev Biol 38:43–52. https://doi.org/10.1016/j.semcdb.2014.11.007
Chassidim Y, Veksler R, Lublinsky S, Pell GS, Friedman A, Shelef I (2013) Quantitative imaging assessment of blood-brain barrier permeability in humans. Fluids Barriers CNS 10:9. https://doi.org/10.1186/2045-8118-10-9
Chen D, Wei XT, Guan JH, Yuan JW, Peng YT, Song L, Liu YH (2012) Inhibition of c-Jun N-terminal kinase prevents blood-brain barrier disruption and normalizes the expression of tight junction proteins clautin-5 and ZO-1 in a rat model of subarachnoid hemorrhage. Acta Neurochir (Wien) 154:1469–1476; discussion 1476. https://doi.org/10.1007/s00701-012-1328-y
Chen F, Hori T, Ohashi N, Baine AM, Eckman CB, Nguyen JH (2011) Occludin is regulated by epidermal growth factor receptor activation in brain endothelial cells and brains of mice with acute liver failure. Hepatology 53:1294–1305. https://doi.org/10.1002/hep.24161
Chen J, Chen G, Li J, Qian C, Mo H, Gu C, Yan F, Yan W, Wang L (2014) Melatonin attenuates inflammatory response-induced brain edema in early brain injury following a subarachnoid hemorrhage: a possible role for the regulation of pro-inflammatory cytokines. J Pineal Res 57:340–347. https://doi.org/10.1111/jpi.12173
Chen J, Jin H, Xu H, Peng Y, Jie L, Xu D, Chen L, Li T, Fan L, He P, Ying G, Gu C, Wang C, Wang L, Chen G (2019) The Neuroprotective effects of necrostatin-1 on subarachnoid hemorrhage in rats are possibly mediated by preventing blood-brain barrier disruption and RIP3-mediated necroptosis. Cell Transplant 28:1358–1372. https://doi.org/10.1177/0963689719867285
Chen J, Qian C, Duan H, Cao S, Yu X, Li J, Gu C, Yan F, Wang L, Chen G (2015) Melatonin attenuates neurogenic pulmonary edema via the regulation of inflammation and apoptosis after subarachnoid hemorrhage in rats. J Pineal Res 59:469–477. https://doi.org/10.1111/jpi.12278
Chen T, Wang W, Li JR, Xu HZ, Peng YC, Fan LF, Yan F, Gu C, Wang L, Chen G (2016) PARP inhibition attenuates early brain injury through NF-kappaB/MMP-9 pathway in a rat model of subarachnoid hemorrhage. Brain Res 1644:32–38. https://doi.org/10.1016/j.brainres.2016.05.005
Chiba H, Osanai M, Murata M, Kojima T, Sawada N (2008) Transmembrane proteins of tight junctions. Biochim Biophys Acta 1778:588–600. https://doi.org/10.1016/j.bbamem.2007.08.017
Claassen J, Bernardini GL, Kreiter K, Bates J, Du YE, Copeland D, Connolly ES, Mayer SA (2001) Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after subarachnoid hemorrhage: the Fisher scale revisited. Stroke 32:2012–2020. https://doi.org/10.1161/hs0901.095677
Claassen J, Carhuapoma JR, Kreiter KT, Du EY, Connolly ES, Mayer SA (2002) Global cerebral edema after subarachnoid hemorrhage: frequency, predictors, and impact on outcome. Stroke 33:1225–1232. https://doi.org/10.1161/01.str.0000015624.29071.1f
Daneman R, Zhou L, Kebede AA, Barres BA (2010) Pericytes are required for blood-brain barrier integrity during embryogenesis. Nature 468:562–566. https://doi.org/10.1038/nature09513
Dankbaar JW, Rijsdijk M, van der Schaaf IC, Velthuis BK, Wermer MJ, Rinkel GJ (2009) Relationship between vasospasm, cerebral perfusion, and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Neuroradiology 51:813–819. https://doi.org/10.1007/s00234-009-0575-y
Doczi T (1985) The pathogenetic and prognostic significance of blood-brain barrier damage at the acute stage of aneurysmal subarachnoid haemorrhage. Clinical and experimental studies. Acta Neurochir (Wien) 77:110–132. https://doi.org/10.1007/bf01476215
Doczi T, Ambrose J, O'Laoire S (1984) Significance of contrast enhancement in cranial computerized tomography after subarachnoid hemorrhage. J Neurosurg 60:335–342. https://doi.org/10.3171/jns.1984.60.2.0335
Doherty CP, O'Keefe E, Wallace E, Loftus T, Keaney J, Kealy J, Humphries MM, Molloy MG, Meaney JF, Farrell M, Campbell M (2016) Blood-brain barrier dysfunction as a hallmark pathology in chronic traumatic encephalopathy. J Neuropathol Exp Neurol 75:656–662. https://doi.org/10.1093/jnen/nlw036
Dorhout Mees SM, Rinkel GJ, Feigin VL, Algra A, van den Bergh WM, Vermeulen M, van Gijn J (2007) Calcium antagonists for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev:Cd000277. https://doi.org/10.1002/14651858.CD000277.pub3
Dreier JP (2011) The role of spreading depression, spreading depolarization and spreading ischemia in neurological disease. Nat Med 17:439–447. https://doi.org/10.1038/nm.2333
Fan LF, He PY, Peng YC, Du QH, Ma YJ, Jin JX, Xu HZ, Li JR, Wang ZJ, Cao SL, Li T, Yan F, Gu C, Wang L, Chen G (2017) Mdivi-1 ameliorates early brain injury after subarachnoid hemorrhage via the suppression of inflammation-related blood-brain barrier disruption and endoplasmic reticulum stress-based apoptosis. Free Radic Biol Med 112:336–349. https://doi.org/10.1016/j.freeradbiomed.2017.08.003
Fang R, Zheng X, Zhang M (2016) Ethyl pyruvate alleviates early brain injury following subarachnoid hemorrhage in rats. Acta Neurochir (Wien) 158:1069–1076. https://doi.org/10.1007/s00701-016-2795-3
Friedrich V, Flores R, Muller A, Sehba FA (2010) Escape of intraluminal platelets into brain parenchyma after subarachnoid hemorrhage. Neuroscience 165:968–975. https://doi.org/10.1016/j.neuroscience.2009.10.038
Fujii M, Duris K, Altay O, Soejima Y, Sherchan P, Zhang JH (2012) Inhibition of Rho kinase by hydroxyfasudil attenuates brain edema after subarachnoid hemorrhage in rats. Neurochem Int 60:327–333. https://doi.org/10.1016/j.neuint.2011.12.014
Fujii M, Sherchan P, Soejima Y, Doycheva D, Zhao D, Zhang JH (2016) Cannabinoid receptor type 2 agonist attenuates acute neurogenic pulmonary edema by preventing neutrophil migration after subarachnoid hemorrhage in rats. Acta Neurochir (Wien) Suppl 121:135–139. https://doi.org/10.1007/978-3-319-18497-5_24
Han YW, Liu XJ, Zhao Y, Li XM (2018) Role of Oleanolic acid in maintaining BBB integrity by targeting p38MAPK/VEGF/Src signaling pathway in rat model of subarachnoid hemorrhage. Eur J Pharmacol 839:12–20. https://doi.org/10.1016/j.ejphar.2018.09.018
Hasegawa Y, Suzuki H, Altay O, Chen H, Zhang JH (2012) Treatment with sodium orthovanadate reduces blood-brain barrier disruption via phosphatase and tensin homolog deleted on chromosome 10 (PTEN) phosphorylation in experimental subarachnoid hemorrhage. J Neurosci Res 90:691–697. https://doi.org/10.1002/jnr.22801
Heye AK, Culling RD, Valdes Hernandez Mdel C, Thrippleton MJ, Wardlaw JM (2014) Assessment of blood-brain barrier disruption using dynamic contrast-enhanced MRI. A systematic review. Neuroimage Clin 6:262–274. https://doi.org/10.1016/j.nicl.2014.09.002
Hu HM, Li B, Wang XD, Guo YS, Hui H, Zhang HP, Wang B, Huang DG, Hao DJ (2018) Fluoxetine is neuroprotective in early brain injury via its anti-inflammatory and anti-apoptotic effects in a rat experimental subarachnoid hemorrhage model. Neurosci Bull 34:951–962. https://doi.org/10.1007/s12264-018-0232-8
Ishiguro M, Mishiro K, Fujiwara Y, Chen H, Izuta H, Tsuruma K, Shimazawa M, Yoshimura S, Satoh M, Iwama T, Hara H (2010) Phosphodiesterase-III inhibitor prevents hemorrhagic transformation induced by focal cerebral ischemia in mice treated with tPA. PLoS One 5:e15178. https://doi.org/10.1371/journal.pone.0015178
Ivanidze J, Ferraro RA, Giambrone AE, Segal AZ, Gupta A, Sanelli PC (2018) Blood-brain barrier permeability in aneurysmal subarachnoid hemorrhage: correlation with clinical outcomes. AJR Am J Roentgenol 211:891–895. https://doi.org/10.2214/ajr.17.18237
Ivanidze J, Kallas ON, Gupta A, Weidman E, Baradaran H, Mir D, Giambrone A, Segal AZ, Claassen J, Sanelli PC (2016) Application of Blood-brain barrier permeability imaging in global cerebral edema. AJNR Am J Neuroradiol 37:1599–1603. https://doi.org/10.3174/ajnr.A4784
Ivanidze J, Kesavabhotla K, Kallas ON, Mir D, Baradaran H, Gupta A, Segal AZ, Claassen J, Sanelli PC (2015) Evaluating blood-brain barrier permeability in delayed cerebral infarction after aneurysmal subarachnoid hemorrhage. AJNR Am J Neuroradiol 36:850–854. https://doi.org/10.3174/ajnr.A4207
Kebir H, Kreymborg K, Ifergan I, Dodelet-Devillers A, Cayrol R, Bernard M, Giuliani F, Arbour N, Becher B, Prat A (2007) Human TH17 lymphocytes promote blood-brain barrier disruption and central nervous system inflammation. Nat Med 13:1173–1175. https://doi.org/10.1038/nm1651
Kishore S, Ko N, Soares BP, Higashida RT, Tong E, Bhogal S, Bredno J, Cheng SC, Wintermark M (2012) Perfusion-CT assessment of blood-brain barrier permeability in patients with aneurysmal subarachnoid hemorrhage. J Neuroradiol 39:317–325. https://doi.org/10.1016/j.neurad.2011.11.004
Kreiter KT, Copeland D, Bernardini GL, Bates JE, Peery S, Claassen J, Du YE, Stern Y, Connolly ES, Mayer SA (2002) Predictors of cognitive dysfunction after subarachnoid hemorrhage. Stroke 33:200–208. https://doi.org/10.1161/hs0102.101080
Li Z, Liang G, Ma T, Li J, Wang P, Liu L, Yu B, Liu Y, Xue Y (2015) Blood-brain barrier permeability change and regulation mechanism after subarachnoid hemorrhage. Metab Brain Dis 30:597–603. https://doi.org/10.1007/s11011-014-9609-1
Lin Z, Li Y, Su P, Mao D, Wei Z, Pillai JJ, Moghekar A, van Osch M, Ge Y, Lu H (2018) Non-contrast MR imaging of blood-brain barrier permeability to water. Magn Reson Med 80:1507–1520. https://doi.org/10.1002/mrm.27141
Liu X, Zhang X, Ma K, Zhang R, Hou P, Sun B, Yuan S, Wang Z, Liu Z (2016) Matrine alleviates early brain injury after experimental subarachnoid hemorrhage in rats: possible involvement of PI3K/Akt-mediated NF-kappaB inhibition and Keap1/Nrf2-dependent HO-1 inductionn. Cell Mol Biol (Noisy-le-grand) 62:38–44
Lublinsky S, Major S, Kola V, Horst V, Santos E, Platz J, Sakowitz O, Scheel M, Dohmen C, Graf R, Vatter H, Wolf S, Vajkoczy P, Shelef I, Woitzik J, Martus P, Dreier JP, Friedman A (2019) Early blood-brain barrier dysfunction predicts neurological outcome following aneurysmal subarachnoid hemorrhage. EBioMedicine 43:460–472. https://doi.org/10.1016/j.ebiom.2019.04.054
Luh C, Feiler S, Frauenknecht K, Meyer S, Lubomirov LT, Neulen A, Thal SC (2019) The contractile apparatus is essential for the integrity of the blood-brain barrier after experimental subarachnoid hemorrhage. Transl Stroke Res 10:534–545. https://doi.org/10.1007/s12975-018-0677-0
Macdonald RL, Higashida RT, Keller E, Mayer SA, Molyneux A, Raabe A, Vajkoczy P, Wanke I, Bach D, Frey A, Marr A, Roux S, Kassell N (2011) Clazosentan, an endothelin receptor antagonist, in patients with aneurysmal subarachnoid haemorrhage undergoing surgical clipping: a randomised, double-blind, placebo-controlled phase 3 trial (CONSCIOUS-2). Lancet Neurol 10:618–625. https://doi.org/10.1016/s1474-4422(11)70108-9
Macdonald RL, Higashida RT, Keller E, Mayer SA, Molyneux A, Raabe A, Vajkoczy P, Wanke I, Bach D, Frey A, Nowbakht P, Roux S, Kassell N (2012) Randomized trial of clazosentan in patients with aneurysmal subarachnoid hemorrhage undergoing endovascular coiling. Stroke 43:1463–1469. https://doi.org/10.1161/strokeaha.111.648980
Macdonald RL, Kassell NF, Mayer S, Ruefenacht D, Schmiedek P, Weidauer S, Frey A, Roux S, Pasqualin A (2008) Clazosentan to overcome neurological ischemia and infarction occurring after subarachnoid hemorrhage (CONSCIOUS-1): randomized, double-blind, placebo-controlled phase 2 dose-finding trial. Stroke 39:3015–3021. https://doi.org/10.1161/strokeaha.108.519942
Murphy A, Manoel AL, Burgers K, Kouzmina E, Lee T, Macdonald RL, Bharatha A (2015) Early CT perfusion changes and blood-brain barrier permeability after aneurysmal subarachnoid hemorrhage. Neuroradiology 57:767–773. https://doi.org/10.1007/s00234-015-1529-1
Na DG, Kim EY, Ryoo JW, Lee KH, Roh HG, Kim SS, Song IC, Chang KH (2005) CT sign of brain swelling without concomitant parenchymal hypoattenuation: comparison with diffusion- and perfusion-weighted MR imaging. Radiology 235:992–948. https://doi.org/10.1148/radiol.2353040571
Nicholson P, O'Hare A, Power S, Looby S, Javadpour M, Thornton J, Brennan P (2019) Decreasing incidence of subarachnoid hemorrhage. J Neurointerv Surg 11:320–322. https://doi.org/10.1136/neurintsurg-2018-014038
Nitta T, Hata M, Gotoh S, Seo Y, Sasaki H, Hashimoto N, Furuse M, Tsukita S (2003) Size-selective loosening of the blood-brain barrier in claudin-5-deficient mice. J Cell Biol 161:653–660. https://doi.org/10.1083/jcb.200302070
O'Keeffe E, Kelly E, Liu Y, Giordano C, Wallace E, Hynes M, Tiernan S, Meagher A, Greene C, Hughes S, Burke T, Kealy J, Doyle N, Hay A, Farrell M, Grant GA, Friedman A, Veksler R, Molloy MG, Meaney JF, Pender N, Camarillo D, Doherty CP, Campbell M (2020) Dynamic blood-brain barrier regulation in mild traumatic brain injury. J Neurotrauma 37:347–356. https://doi.org/10.1089/neu.2019.6483
Oldendorf WH, Cornford ME, Brown WJ (1977) The large apparent work capability of the blood-brain barrier: a study of the mitochondrial content of capillary endothelial cells in brain and other tissues of the rat. Ann Neurol 1:409–417. https://doi.org/10.1002/ana.410010502
Pan P, Zhang X, Li Q, Zhao H, Qu J, Zhang JH, Liu X, Feng H, Chen Y (2017) Cyclosporine A alleviated matrix metalloproteinase 9 associated blood-brain barrier disruption after subarachnoid hemorrhage in mice. Neurosci Lett 649:7–13. https://doi.org/10.1016/j.neulet.2017.03.050
Pan P, Zhao H, Zhang X, Li Q, Qu J, Zuo S, Yang F, Liang G, Zhang JH, Liu X, He H, Feng H, Chen Y (2020) Cyclophilin a signaling induces pericyte-associated blood-brain barrier disruption after subarachnoid hemorrhage. J Neuroinflammation 17:16. https://doi.org/10.1186/s12974-020-1699-6
Pang J, Chen Y, Kuai L, Yang P, Peng J, Wu Y, Chen Y, Vitek MP, Chen L, Sun X, Jiang Y (2017) Inhibition of Blood-brain barrier disruption by an apolipoprotein E-mimetic peptide ameliorates early brain injury in experimental subarachnoid hemorrhage. Transl Stroke Res 8:257–272. https://doi.org/10.1007/s12975-016-0507-1
Pickard JD, Murray GD, Illingworth R, Shaw MD, Teasdale GM, Foy PM, Humphrey PR, Lang DA, Nelson R, Richards P et al (1989) Effect of oral nimodipine on cerebral infarction and outcome after subarachnoid haemorrhage: British aneurysm nimodipine trial. Bmj 298:636–642. https://doi.org/10.1136/bmj.298.6674.636
Pradilla G, Chaichana KL, Hoang S, Huang J, Tamargo RJ (2010) Inflammation and cerebral vasospasm after subarachnoid hemorrhage. Neurosurg Clin N Am 21:365–379. https://doi.org/10.1016/j.nec.2009.10.008
Qian C, Jin J, Chen J, Li J, Yu X, Mo H, Chen G (2017) SIRT1 activation by resveratrol reduces brain edema and neuronal apoptosis in an experimental rat subarachnoid hemorrhage model. Mol Med Rep 16:9627–9635. https://doi.org/10.3892/mmr.2017.7773
Qian H, Dou Z, Ruan W, He P, Zhang JH, Yan F (2018) ErbB4 preserves blood-brain barrier integrity via the YAP/PIK3CB pathway after subarachnoid hemorrhage in rats. Front Neurosci 12:492. https://doi.org/10.3389/fnins.2018.00492
Rieth KG, Fujiwara K, Di Chiro G, Klatzo I, Brooks RA, Johnston GS, O'Connor CM, Mitchell LG (1980) Serial measurements of CT attenuation and specific gravity in experimental cerebral edema. Radiology 135:343–348. https://doi.org/10.1148/radiology.135.2.6768102
Russin JJ, Montagne A, D'Amore F, He S, Shiroishi MS, Rennert RC, Depetris J, Zlokovic BV, Mack WJ (2018) Permeability imaging as a predictor of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. J Cereb Blood Flow Metab 38:973–979. https://doi.org/10.1177/0271678x18768670
Sage MR (1982) Blood-brain barrier: phenomenon of increasing importance to the imaging clinician. AJR Am J Roentgenol 138:887–898. https://doi.org/10.2214/ajr.138.5.887
Saitou M, Fujimoto K, Doi Y, Itoh M, Fujimoto T, Furuse M, Takano H, Noda T, Tsukita S (1998) Occludin-deficient embryonic stem cells can differentiate into polarized epithelial cells bearing tight junctions. J Cell Biol 141:397–408. https://doi.org/10.1083/jcb.141.2.397
Sanelli PC, Ugorec I, Johnson CE, Tan J, Segal AZ, Fink M, Heier LA, Tsiouris AJ, Comunale JP, John M, Stieg PE, Zimmerman RD, Mushlin AI (2011) Using quantitative CT perfusion for evaluation of delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. AJNR Am J Neuroradiol 32:2047–2053. https://doi.org/10.3174/ajnr.A2693
Sasaki T, Kassell NF, Yamashita M, Fujiwara S, Zuccarello M (1985) Barrier disruption in the major cerebral arteries following experimental subarachnoid hemorrhage. J Neurosurg 63:433–440. https://doi.org/10.3171/jns.1985.63.3.0433
Scholler K, Trinkl A, Klopotowski M, Thal SC, Plesnila N, Trabold R, Hamann GF, Schmid-Elsaesser R, Zausinger S (2007) Characterization of microvascular basal lamina damage and blood-brain barrier dysfunction following subarachnoid hemorrhage in rats. Brain Res 1142:237–246. https://doi.org/10.1016/j.brainres.2007.01.034
Sehba FA, Mostafa G, Knopman J, Friedrich V Jr, Bederson JB (2004) Acute alterations in microvascular basal lamina after subarachnoid hemorrhage. J Neurosurg 101:633–640. https://doi.org/10.3171/jns.2004.101.4.0633
Serlin Y, Ofer J, Ben-Arie G, Veksler R, Ifergane G, Shelef I, Minuk J, Horev A, Friedman A (2019) Blood-Brain Barrier Leakage: A New Biomarker in Transient Ischemic Attacks. Stroke 50:1266–1269. https://doi.org/10.1161/strokeaha.119.025247
Skriver EB, Olsen TS (1981) Transient disappearance of cerebral infarcts on CT scan, the so-called fogging effect. Neuroradiology 22:61–65. https://doi.org/10.1007/bf00344775
Skriver EB, Olsen TS (1982) Contrast enhancement of cerebral infarcts. Incidence and clinical value in different states of cerebral infarction. Neuroradiology 23:259–265. https://doi.org/10.1007/bf00339392
Sourbron SP, Buckley DL (2013) Classic models for dynamic contrast-enhanced MRI. NMR Biomed 26:1004–1027. https://doi.org/10.1002/nbm.2940
Suzuki H, Ayer R, Sugawara T, Chen W, Sozen T, Hasegawa Y, Kanamaru K, Zhang JH (2010) Protective effects of recombinant osteopontin on early brain injury after subarachnoid hemorrhage in rats. Crit Care Med 38:612–618. https://doi.org/10.1097/CCM.0b013e3181c027ae
Sweeney K, Silver N, Javadpour M (2016) Subarachnoid haemorrhage (spontaneous aneurysmal). BMJ Clin Evid 2016:1213
Teo M, Guilfoyle MR, Turner C, Kirkpatrick PJ (2017) What factors determine treatment outcome in aneurysmal subarachnoid hemorrhage in the modern era? A Post Hoc STASH Analysis. World Neurosurg 105:270–281. https://doi.org/10.1016/j.wneu.2017.05.005
Thal SC, Sporer S, Plesnila N, Schoeller K, Schmid-Elsaesser R, Zausinger S (2005) Evolution of brain edema after subarachnoid hemorrhage (SAH) in rats. J Cereb Blood Flow Metab 25:S271–S271
Wang Z, Meng CJ, Shen XM, Shu Z, Ma C, Zhu GQ, Liu HX, He WC, Sun XB, Huo L, Zhang J, Chen G (2012) Potential contribution of hypoxia-inducible factor-1alpha, aquaporin-4, and matrix metalloproteinase-9 to blood-brain barrier disruption and brain edema after experimental subarachnoid hemorrhage. J Mol Neurosci 48:273–280. https://doi.org/10.1007/s12031-012-9769-6
Winkler L, Blasig R, Breitkreuz-Korff O, Berndt P, Dithmer S, Helms HC, Puchkov D, Devraj K, Kaya M, Qin Z, Liebner S, Wolburg H, Andjelkovic AV, Rex A, Blasig IE, Haseloff RF (2020) Tight junctions in the blood-brain barrier promote edema formation and infarct size in stroke - Ambivalent effects of sealing proteins. J Cereb Blood Flow Metab:271678x20904687. https://doi.org/10.1177/0271678x20904687
Won S, Lee JH, Wali B, Stein DG, Sayeed I (2014) Progesterone attenuates hemorrhagic transformation after delayed tPA treatment in an experimental model of stroke in rats: involvement of the VEGF-MMP pathway. J Cereb Blood Flow Metab 34:72–80. https://doi.org/10.1038/jcbfm.2013.163
Xie Z, Enkhjargal B, Reis C, Huang L, Wan W, Tang J, Cheng Y, Zhang JH (2017) Netrin-1 preserves blood-brain barrier integrity through deleted in colorectal cancer/focal adhesion kinase/RhoA signaling pathway following subarachnoid hemorrhage in rats. J Am Heart Assoc 6. https://doi.org/10.1161/jaha.116.005198
Yan J, Chen C, Hu Q, Yang X, Lei J, Yang L, Wang K, Qin L, Huang H, Zhou C (2008) The role of p53 in brain edema after 24 h of experimental subarachnoid hemorrhage in a rat model. Exp Neurol 214:37–46. https://doi.org/10.1016/j.expneurol.2008.07.006
Yan J, Li L, Khatibi NH, Yang L, Wang K, Zhang W, Martin RD, Han J, Zhang J, Zhou C (2011) Blood-brain barrier disruption following subarchnoid hemorrhage may be faciliated through PUMA induction of endothelial cell apoptosis from the endoplasmic reticulum. Exp Neurol 230:240–247. https://doi.org/10.1016/j.expneurol.2011.04.022
Yi R, Xiao-Ping G, Hui L (2015) Atorvastatin prevents angiotensin II-induced high permeability of human arterial endothelial cell monolayers via ROCK signaling pathway. Biochem Biophys Res Commun 459:94–99. https://doi.org/10.1016/j.bbrc.2015.02.076
Yin D, Zhou S, Xu X, Gao W, Li F, Ma Y, Sun D, Wu Y, Guo Q, Liu H, Han L, Wang Z, Wang Y, Zhang J (2018) Dexmedetomidine attenuated early brain injury in rats with subarachnoid haemorrhage by suppressing the inflammatory response: The TLR4/NF-kappaB pathway and the NLRP3 inflammasome may be involved in the mechanism. Brain Res 1698:1–10. https://doi.org/10.1016/j.brainres.2018.05.040
Yuan J, Liu W, Zhu H, Zhang X, Feng Y, Chen Y, Feng H, Lin J (2017) Curcumin attenuates blood-brain barrier disruption after subarachnoid hemorrhage in mice. J Surg Res 207:85–91. https://doi.org/10.1016/j.jss.2016.08.090
Zhang H, Zhang B, Li S, Liang C, Xu K, Li S (2013) Whole brain CT perfusion combined with CT angiography in patients with subarachnoid hemorrhage and cerebral vasospasm. Clin Neurol Neurosurg 115:2496–2501. https://doi.org/10.1016/j.clineuro.2013.10.004
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organisation or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
For this type of study, formal consent is not required.
Informed consent
This article does not contain any studies with human participants performed by any of the authors.
Additional information
Comments
The authors claim that the manuscript is a narrative review on the hypothesis that clinical imaging of the blood-brain barrier permeability may serve as a predictor for delayed cerebral ischaemia following subarachnoid haemorrhage.
They state that there has been limited use of BBB imaging in clinical practice for the prediction and prognostication of DCI following aSAH. Accordingly, they discuss some of the mechanisms involved in BBB disruption following aSAH and the potential role of BBB integrity imaging in prediction of DCI and outcome prognostication following aSAH.
The concept that detection of focal BBB damage following aneurysmal subarachnoid haemorrhage in the acute phase of the disease as shown by abnormal contrast enhancement may be an early indicator/biomarker of development of delayed vasospasm/focal DCI is rather old. The authors rightly point out that DCI, however, has now been shown to occur independent of cerebral vasospasm, i.e. the pathogenesis of DCI may not be fully a result of pathological vasoconstriction.
The authors performed an anecdotical search in the English literature looking for papers dealing with disruptions to the blood-brain barrier in SAH; BBB permeability imaging as a predictor of DCI. Based on their critical reading experiences, they conclude that there is sufficient evidence from preclinical and clinical studies to suggest that alterations to the permeability of the BBB play a crucial role in the complex pathophysiology of DCI following SAH.
Radiological biomarkers offer a potential non-invasive prognostication tool and may also allow early identifications of patients who may be at risk of DCI.
With the recent advances in permeability imaging, it is imperative that potential associations between BBB disruption and early and delayed brain injuries are investigated in patients with aSAH.
Tamas Peter Doczi
Pecs, Hungary
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Vascular Neurosurgery – Aneurysm
Rights and permissions
About this article

Cite this article
Amoo, M., Henry, J., Pender, N. et al. Blood-brain barrier permeability imaging as a predictor for delayed cerebral ischaemia following subarachnoid haemorrhage. A narrative review. Acta Neurochir 163, 1457–1467 (2021). https://doi.org/10.1007/s00701-020-04670-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-020-04670-6