
Abstract
Background
There is no universal management protocol concerning invasive malignant tumors of the scalp with bone and dura mater invasion. The aims of this study were to report and discuss our experience in the management of these forms of tumors.
Methods
We retrospectively reviewed all consecutive patients of microsurgical scalp reconstruction performed after resection of invasive cutaneous malignancies of the scalp, calvarium, and dura mater from 2017 to 2019, at Pitié-Salpêtrière University Hospital (Paris, France).
Results
Five patients met inclusion criteria. There were three squamous cell carcinomas and two sarcomas. Mean age at surgery was 63.6 years. The sex ratio male/female was 4. Two received radiation prior to resection and two patients had a history of prior scalp tumor surgery. All the patients underwent craniectomy and the mean cranial defect size was 41 cm2. Cranioplasty was performed in one patient. Soft tissue coverage was provided by free tissue transfer of latissimus dorsi muscle in all patients. In four patients, split thickness skin graft was performed in a second surgical stage few weeks later. There were no intraoperative complications and no complications into the donor site for the tissue transfer or the skin graft. Two patients had flap necrosis that healed after a new free flap of latissimus dorsi.
Conclusions
Wide resection with craniectomy and reconstruction with microvascular free tissue transfer provides safe and reliable treatment of recalcitrant invasive scalp skin cancers. The surgical management of these complex patients is a challenge that must be conducted by trained, experienced, and multidisciplinary teams.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Few data are available in the literature concerning scalp invasive malignancies and their surgical care (excision and reconstruction after large and complex resection of calvarium). Tumor excision with scalp and bone invasion can be a surgical challenge due to the size and the invasiveness of the tumor. Likewise, calvaria reconstruction after excision can be also challenging and is generally performed using skin grafts or large flap depending on the defect size. However, there is no universal management protocol for these forms of tumors. When they are invasive, craniectomy and dura mater excision may be required to obtain full tumor excision, which exposes the patient to a risk of cerebrospinal fluid leak and infection. After these procedures, there is no consensus on the need of cranioplasty after microsurgical reconstruction of the skin.
Reconstruction scalp and skull defect resulting from tumor excision present most difficulties for the surgeon. Wide excision may include skin, periosteum, skull, and dura mater, creating a complex wound. The use of radiation therapy and chemotherapy can compromise healing and scalp’s vascularization. Flaps used for reconstruction should be durable to support adjuvant treatment. In 1972, free tissue transfer for reconstruction of large scalp defect was used for the first time, with an omentum flap to cover the defect [15]. Since then, other series have demonstrated the efficacy of this approach [16, 23]. The aim of the present study was to report and discuss our experience in the management of invasive malignant tumors of the scalp with bone and dura mater invasion.
Patients and methods
Patient recruitment
We retrospectively reviewed all consecutive patients of microsurgical scalp reconstruction performed after resection of invasive cutaneous malignancies of the scalp, calvarium, and dura mater from February 2017 to July 2019, at Pitié-Salpêtrière University Hospital (Paris, France).
Presurgical evaluation included complete general and neurological examination, brain MRI and CT scan, body scanner, and in some cases body positron emission tomography (PET). These data were analyzed by a multidisciplinary team, including plastic surgeon, neurosurgeon, anesthetist, oncologist, radiotherapist, dermatologist, and radiologist, to determine whether surgical treatment was indicated and whether a postoperative treatment would be required.
Classification of comorbidities and outcomes
Patient’s data were collected through review of medical records. Current smoking was defined as smoking within 2 months of surgery. Hypertension and hyperlipidemia were defined by the use of antihypertensive and cholesterol-lowering drugs, respectively. Diabetes was defined by the use of oral hypoglycemic drugs or insulin. Immunosuppression was defined by use of immunosuppressive drugs or diagnosis known to cause an immunocompromised state. Patient’s preoperative physical status was classified using the American Society of Anesthesiologists (ASA) score. Patients with a mild systemic disease were classified as ASA II. Patients with a systemic disease which is not incapacitating were classified as ASA III, and patients with an incapacitating systemic disease which is life-threatening were classified as ASA IV.
Measurement of skull defects was performed on postoperative CT scans. Patients were carefully followed to ensure that no complications were missed. Cerebral spinal fluid (CSF) leak was defined by the presence of fluid collected from the operative site. Partial flap loss was defined as flap necrosis that resulted in subtotal loss of flap, while complete flap loss was defined as requiring total flap replacement.
Standard protocol approvals, registrations, and patient consents
The database is registered with the Commission Nationale de l’Informatique et des Libertés (no. 2214386). In accordance with the ethical standards of our hospital’s institutional review board, the Committee for the Protection of Human Subjects, and French law, written informed consent was not needed for demographic, physiological, and hospital-outcome data analyses because this observational study did not modify existing diagnostic or therapeutic strategies; however, patients were informed of their inclusion in the study. The manuscript was prepared in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement.
Results
Patient characteristics
We found five patients who underwent resection followed by reconstruction surgery for invasive malignant tumors of the scalp extending into the calvarium and the dura mater. Mean age at surgery was 63.6 ± 9.2 years (range 35–84). The sex ratio male/female was 4. Preoperative patient comorbidities are summarized in Table 1. The mean follow-up period was 19 (range 7–36) months.
Tumor characteristics and surgical management
Of the five patients included in the study, three had stage IVA squamous cell carcinomas and two had sarcomas (one grade III undifferentiated sarcoma and one low-grade myofibroblastic sarcoma). The three patients with squamous cell carcinomas presented both clinical and histological poor prognostic factors according to the National Comprehensive Cancer Network (NCCN, USA) classification [18]. Two patients were treated by radiation therapy prior to resection (#1 and #2) and two patients had a history of prior scalp tumor surgery (#1 and #5). None of the patients had adjuvant lymph node excision.
Two patients had active scalp infections at the time of presentation: one had methicillin-resistant Staphylococcus aureus (MRSA) plus Proteus mirabilis plus Enterococcus Faecalis extra- and subdural empyema with skull necrosis that required surgical evacuation and intravenous antibiotics prior to reconstruction surgery (#1, Fig. 1a, b), and the second one had methicillin-susceptible Staphylococcus aureus superficial infection treated with oral antibiotics (#4, Fig. 2a–c). Three patients had tumor-related cerebral venous thrombosis before surgery: two had partial superior sagittal sinus thrombosis (#2 and #4, Fig. 2a) and had one cortical vein thrombosis (#1, Fig. 1a) that needed postoperative anticoagulation therapy.

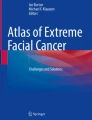
Patient #1: a 35-year-old man with a history of sarcoma (diagnosed in 2000 in Algeria with five resection surgeries between 2000 and 2017), arrived in France in July 2017. He presented a wide skin, bone, and dura mater damage (a, b) with a left extra and subdural empyema (a). A three-stage surgical management was performed. First, skin and pericranium resection with craniectomy and empyema evacuation have been performed. Postoperatively, intravenous antibiotics and anticoagulation therapy were started to threat both empyema and a cortical vein thrombosis. The second surgical stage was the reconstruction of cranial and skin defects, using a free flap of latissimus dorsi muscle (c), performed 1 month after the first surgical time. Finally, 2 weeks after the second surgical stage, a skin graft (donor site was anterior thigh face) allowed to cover the flap (d). Lateral view of follow-up at 6 weeks demonstrating stable soft tissue coverage (e)

Patient #4: a 70-year-old man who developed recurrent invasive squamous cell carcinoma after immunosuppression for living-related kidney transplant. Preoperative T1-weighted magnetic resonance imaging (a) and CT scan (b) show an ulcerated tumor with invasion through the scalp into the cranium with superior longitudinal sinus tumoral involvement (c). Scalp and calvarial defect after wide local excision (d). A large Surgicel sheet was used to repair the dural defect (d). The defect was then reconstructed by a latissimus dorsi muscle free flap
All patients underwent wide scalp resection, craniectomy, and dural electrocoagulation (Table 2). The mean cranial defect size was 41 cm2 (3.4–155). The three patients who had a dural resection required primary dural repair. Cranioplasty was performed on the same surgical stage in one patient (#2, Fig. 3c). Soft tissue coverage was provided by free tissue transfer of latissimus dorsi muscle in all patients (#1, Fig. 1c, e; #2, Fig. 3d; #3, Fig. 4e). The recipient vessels were the superficial temporal artery and vein in all patients. Mean surgical duration was 7.3 (range 5–10.5) hours. Mean intraoperative blood loss was 780 (range 400–1500) ml. In four patients (80%), split-thickness skin graft was performed in a second surgical stage few weeks later (Figs. 1d, e, 3d, and 4e).

Patient #2: a 61-year-old woman, with a long history of recurrent squamous cell carcinoma (diagnosed in 2012, treated by chemotherapy and radiotherapy between 2012 and 2015, with follow-up break between 2015 and 2017) arrived in September 2017. She presented a wide skin, bone, and dura mater damage with tumor invasion of the superior longitudinal sinus (a). We performed skin (b), bone (c), and dura mater excision. In the same time, the defect was reconstructed with tailored titanium cranioplasty (c) and free flap of latissimus dorsi muscle. The patient had a little CSF leak after surgery resolved with lumbar punctures. After 3 weeks, a skin graft (donor-site was antero-internal thigh face) allowed to cover the flap. View of follow-up after free latissimus dorsi muscle flap with split thickness skin graft and postoperative radiation (d)

Patient #3: a 68-year-old man presented in February 2018 with a giant retro-auricular left undifferentiated sarcoma (diameter was 29 cm) involving skin, bone, and dura mater (a, b). A preoperative embolization was performed to limit bleeding during the surgery. Two days after embolization, resection surgery was achieved (c, d). The defect was reconstructed in the same time with a free flap of latissimus dorsi muscle. Patient had a flap necrosis, 1 week after surgery, requiring a revision surgery with a new latissimus dorsi muscle free flap. This second surgery led to local healing (e)
Postoperative management
In the postoperative period, all patients underwent CT scan to detect potential early intracranial bleeding and then received subcutaneous heparin. Four patients had been staying for only 24 h in the intensive care unit, and one patient had been staying for 7 days (#1). The median total days of hospitalization were 9 (range 8–35) days. Four patients were discharged home and one was discharged to a rehabilitation center before returning home.
Patients operated on for squamous cell carcinomas did not receive any adjuvant treatment, while adjuvant radiotherapy has been performed in patients with sarcoma. A patient with systemic metastases of sarcoma (#3) received additional chemotherapy (adriamycin 60 mg/m2). Of the five patients, one patient who experienced an early local tumor recurrence died 7 months after surgery (#4), and one patient died within 10 months of surgery because of multiple systemic metastases (#3). The remaining three patients had no recurrence at 12, 34, and 36 months after the surgery, respectively.
Complications
There were no intraoperative complications and no complications into the donor site for the tissue transfer or the skin graft. All free tissue transfers achieved 100% soft tissue coverage. Postoperative complications included one CSF leak that required lumbar punctures (#2). Two patients had flap necrosis due to arterial thrombosis (#3 and #5) 7 and 3 days after surgery, respectively, that healed after a surgical management consisting of a new free flap of latissimus dorsi. One patient experienced flap dehiscence (#4) which was treated using topical skin care. There were no complications in the four patients who had skin grafts.
Discussion
The common cutaneous neoplasms of the scalp (squamous cell carcinoma, basal cell carcinoma, and malignant melanoma) are usually successfully treated with soft tissue excision and scalp reconstruction using primary repair, local flaps, or skin grafting [2, 17]. All of our patients showed invasion of their cutaneous malignancies into the cranium. This was evidenced preoperatively on imaging and confirmed intraoperatively. These patients were first rescued by other local or regional hospitals because of the risk of postoperative complications and then referred to our tertiary center. Reconstruction was considerably challenging in these patients given their tumor size and because the quality of the surrounding tissue was compromised by prior surgery, radiation, or infection. Our management of these cutaneous malignancies of the scalp with deep invasion was therefore guided by the balance between obtaining clear surgical margins while avoiding neurological complications. A multidisciplinary approach has been successful in achieving complete surgical excision and immediate single-stage soft tissue reconstruction.
Post-operative defect was covered by free tissue transfer of latissimus dorsi muscle with split-thickness skin graft. Other flap techniques such as rectus abdominis muscle or antero-lateral thigh were also eligible. However, free flaps are optimal for reconstruction of large skin defects [9]. In cases which require postoperative irradiation, free flap might be more reliable than local pedicle flaps. Furthermore, the skin graft at the donor site may not tolerate postoperative irradiation [6, 8, 16]. Latissimus dorsi muscle is a large, broad, and flat muscle providing stable soft tissue coverage, particularly if additional scalp needs to be resected in order to remove substrate for potential tumor recurrence [20]. The thoracodorsal artery and the thoracodorsal vein collected with this flap are of ideal caliber and length to perform the microsurgical vascular anastomosis [19]. The latissimus dorsi muscle flap also has the advantage of mimicking native scalp thickness and contour. Although secondary to the control of the malignancy, the aesthetic result of the reconstruction is an important consideration. Free flaps achieve good aesthetic results both in non-hearing and hearing areas [13].
Complications after surgery for reconstruction of scalp and calvaria in skin cancers are frequent [24]. They are more frequent when skin cancer involves bone and dura mater, and complications include CSF leak, sinus and cortical veins thrombosis, and neurological impairment. Our patients had voluminous and invasive tumors and had poor general health condition and serious comorbidities, which can explain the high rate of flap necrosis. The two cases of flap loss requiring revision surgery occurred in patients with poor general status and active smoking, the latter being a well-known risk factor for complication after free flap tissue transfer [3, 7, 22]. Special attention should therefore be paid to smoking patients in the postoperative period. We recommend a systematic intervention for smoking cessation before the surgery [4]. Moreover, chronic use of corticosteroids does not increase rates of wound complications, reoperation, or readmission. However, this population of patients may be at increased risk for major bleedings requiring blood transfusion following free flap reconstruction [25]. Superior longitudinal sinus thrombosis can occur especially in patients with tumoral involvement of the dura mater and requires pre- and/or postoperative anticoagulation therapy. Finally, patients whose surgery is delayed have a poor prognosis, suggesting that early detection and treatment are crucial [1].
Despite flap loss in two of our patients, we obtained local healing after surgical revision. The three other patients are currently in remission. Given the severity of the initial clinical presentation, these outcomes can be considered as good. Indeed, oncological and esthetical benefits were major in patients with no other therapeutic resources. Our experience, shared by other teams, with these advanced lesions is that even when resection is likely to be incomplete because of either sagittal sinus involvement or the magnitude of the lesion, palliative resection and reconstruction are worth considering [10, 14]. We therefore advocate for an aggressive and customized surgical management involving multidisciplinary collaboration and strategic thinking.
For patients with large skull defects, the indications for cranioplasty are both functional, in terms of cerebral protection, and aesthetic, to maintain the contour of the calvarium. Nevertheless, performing a cranioplasty during the immediate reconstruction remains controversial, because it increases the risk of postoperative infection while it does not require a second surgery. In our series, we performed immediate cranioplasty in only one patient who experienced no serious postoperative adverse events. The other patients presented exophytic ulcerated tumors with concomitant contamination or infection, which are contraindications for subsequent cranioplasty. In a study evaluating alloplastic cranioplasty, an infection rate of 40% was reported when calvarium was reconstructed with cranioplasty in the same surgical stage [5]. Several studies reported high complication rates (from 33 to 57%), when cranioplasty was performed during the immediate reconstruction, which required in most cases the removal of the prothesis [1, 3, 21]. However, these studies were not exclusively on patients with cranial defects due to resection of malignant tumors. Regardless of this, the higher complication rates reported in all studies about concomitant cranioplasty and scalp reconstruction have to be considered with caution. Several factors appeared to be important in these complications: the presence of residual devascularized or infected bone after excision, inadequate coverage of the cranioplasty with well-vascularized free tissue, and the nature of the material used for the cranioplasty [11, 14]. Preoperative and intraoperative recognition of the extent of the bony abnormality appears therefore fundamental to guide both tumor resection and cranioplasty. Cho et al. reported 11 cases of reconstruction without cranioplasty for recalcitrant invasive skin cancer of the scalp and proposed to avoid cranioplasty during the immediate reconstruction [5]. Moreover, in the Bethesda Cranial Facial Reconstruction Protocol, delayed skull reconstruction resulted in a lower complication rate than previously described [12]. This approach is based on the two major advantages theoretically provided if cranioplasty is avoided at first excision. First, as seen in patients without dural repair, having a vascularized graft immediately on the dura mater can limit the creation of epidural fluid collections [12]. The second advantage of delaying cranioplasty is evidenced in patients who underwent dural repair using xenograft material and in whom the contact with a well-vascularized flap seemed to aid in healing and decreased CSF leaks [5]. Finally, although experience with cranioplasty is limited, the use of titanium mesh satisfies our requirements of a malleable but sturdy implant, which can be fixed rigidly.
Conclusion
Wide resection with craniectomy and reconstruction with free tissue transfer with or without cranioplasty provide safe and reliable treatment for invasive malignant tumors of the scalp. The free tissue transfer of latissimus dorsi muscle is the mainstay to cover complex scalp defects and tolerate radiation. The place of cranioplasty during the immediate reconstruction remains controversial and is still debated. Anyhow, the surgical management of these complex patients is a challenge that must be conducted by trained, experienced, and multidisciplinary teams comprising neurosurgeons, plastic surgeons, and dedicated anesthetists.
References
Afifi A, Djohan RS, Hammert W, Papay FA, Barnett AE, Zins JE (2010) Lessons learned reconstructing complex scalp defects using free flaps and a cranioplasty in one stage. J Craniofac Surg 21(4):1205–1209
Brandt MG, Moore CC (2019) Nonmelanoma skin cancer. Facial Plast Surg Clin N Am 27(1):1–13
Chao AH, Yu P, Skoracki RJ, Demonte F, Hanasono MM (2012) Microsurgical reconstruction of composite scalp and calvarial defects in patients with cancer: a 10-year experience. Head Neck 34(12):1759–1764
Chen D, Wu L-T (2015) Smoking cessation interventions for adults aged 50 or older: a systematic review and meta-analysis. Drug Alcohol Depend 154:14–24
Cho GJ, Wang F, Garcia SM, Viner J, Hoffman WY, McDermott MW, Pomerantz JH (2017) Recalcitrant invasive skin cancer of the scalp: combined extirpation and microsurgical reconstruction without cranioplasty. J Craniofac Surg 28(2):325–330
Earley MJ, Green MF, Milling MA (1990) A critical appraisal of the use of free flaps in primary reconstruction of combined scalp and calvarial cancer defects. Br J Plast Surg 43(3):283–289
Ehrl D, Heidekrueger PI, Haas EM, Coenen M, Giunta R, Ninkovic M, Broer PN (2018) Does cigarette smoking harm microsurgical free flap reconstruction? J Reconstr Microsurg 34(7):492–498
Furnas H, Lineaweaver WC, Alpert BS, Buncke HJ (1990) Scalp reconstruction by microvascular free tissue transfer. Ann Plast Surg 24(5):431–444
Hussussian CJ, Reece GP (2002) Microsurgical scalp reconstruction in the patient with cancer. Plast Reconstr Surg 109(6):1828–1834
Ioannides C, Fossion E, McGrouther AD (1999) Reconstruction for large defects of the scalp and cranium. J Cranio-Maxillo-fac Surg Off Publ Eur Assoc Cranio-Maxillo-fac Surg 27(3):145–152
Kozák J, Voska P, Zvĕrina E (1995) The management of extensive tumours of the scalp. Acta Chir Plast 37(3):71–75
Kumar AR, Tantawi D, Armonda R, Valerio I (2012) Advanced cranial reconstruction using intracranial free flaps and cranial bone grafts: an algorithmic approach developed from the modern battlefield. Plast Reconstr Surg 130(5):1101–1109
Lutz BS, Wei FC, Chen HC, Lin CH, Wei CY (1998) Reconstruction of scalp defects with free flaps in 30 cases. Br J Plast Surg 51(3):186–190
McCombe D, Donato R, Hofer SOP, Morrison W, Hofer S (2002) Free flaps in the treatment of locally advanced malignancy of the scalp and forehead. Ann Plast Surg 48(6):600–606
McLean DH, Buncke HJ (1972) Autotransplant of omentum to a large scalp defect, with microsurgical revascularization. Plast Reconstr Surg 49(3):268–274
Pennington DG, Stern HS, Lee KK (1989) Free-flap reconstruction of large defects of the scalp and calvarium. Plast Reconstr Surg 83(4):655–661
Richmond HM, Duvic M, Macfarlane DF (2010) Primary and metastatic malignant tumors of the scalp: an update. Am J Clin Dermatol 11(4):233–246
Rowe DE, Carroll RJ, Day CL (1992) Prognostic factors for local recurrence, metastasis, and survival rates in squamous cell carcinoma of the skin, ear, and lip. Implications for treatment modality selection. J Am Acad Dermatol 26(6):976–990
Serletti JM, Moran SL, Orlando GS, Fox I (1999) Thoracodorsal vessels as recipient vessels for the free TRAM flap in delayed breast reconstruction. Plast Reconstr Surg 104(6):1649–1655
Sood R, Easow JM, Konopka G, Panthaki ZJ (2018) Latissimus dorsi flap in breast reconstruction: recent innovations in the workhorse flap. Cancer Control J Moffitt Cancer Cent 25(1):1073274817744638
Sosin M, De la Cruz C, Bojovic B, Christy MR, Rodriguez ED (2015) Microsurgical reconstruction of complex scalp defects: an appraisal of flap selection and the timing of complications. J Craniofac Surg 26(4):1186–1191
Thomas WW, Brant J, Chen J, Coblens O, Fischer JP, Newman JG, Chalian AA, Shanti RM, Cannady SB (2018) Clinical factors associated with reoperation and prolonged length of stay in free tissue transfer to oncologic head and neck defects. JAMA Facial Plast Surg 20(2):154–159
Wackym PA, Feuerman T, Strasnick B, Calcaterra TC (1990) Reconstruction of massive defects of the scalp, cranium, and dura after resection of scalp neoplasms. Head Neck 12(3):247–253
Wang HT, Erdmann D, Olbrich KC, Friedman AH, Levin LS, Zenn MR (2007) Free flap reconstruction of the scalp and calvaria of major neurosurgical resections in cancer patients: lessons learned closing large, difficult wounds of the dura and skull. Plast Reconstr Surg 119(3):865–872
Weisberger JS, Oleck NC, Ayyala HS, Malhotra R, Lee ES (2019) Analysis of the impact of chronic corticosteroid use on free flap reconstruction. Microsurgery. https://doi.org/10.1002/micr.30516
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (name of institute/committee) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study, formal consent is not required. Informed consent was obtained from all individual participants included in the study.
Patient photographic authorization
All patients included in this study had given photographic authorization.
Additional information
Comments
Marijon and colleagues present a description of five cases of invasive malignant tumors of the scalp with bone and dura mater invasion. The paper is concisely written and the figures are informative. Further, the existing literature about this topic is quite limited.
As the authors point out, this is a rare and challenging entity. In my opinion, in line with the authors, the key point in the therapy of these tumors is a meticulous and interdisciplinary planning of the regimen and in most cases also an interdisciplinary surgical approach.
Marcus Reinges
Bremen, Germany
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Tumor - Other
Rights and permissions
About this article

Cite this article
Marijon, P., Bertolus, C., Foy, JP. et al. Custom surgical management of invasive malignant tumors of the scalp. Acta Neurochir 162, 2991–2999 (2020). https://doi.org/10.1007/s00701-020-04525-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-020-04525-0