
Abstract
Background
Burr hole trepanation (BHT) is the most commonly used surgical method for the treatment of chronic subdural haematoma (cSDH).
Method
We give a brief overview on the indication for surgical treatment of cSDH, the surgical technique of BHT, and specific perioperative considerations. In particular, we emphasise on the technique of a subperiosteal drain placement.
Conclusion
BHT is a valid option to treat chronic subdural haematoma. Careful surgical technique and placement of a subperiosteal drain is required to minimise complications and improve outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Relevant surgical anatomy
The subdural space is a virtual space between the dura and the arachnoid, which is tethered together by a layer of dural border cells. Due to the absence of tight junctions, the subdural space predisposes to the formation of haematomas [5].
The most common cause for chronic subdural haematoma (cSDH) is a traumatic injury of bridging veins with consecutive venous bleeding. Current evidence suggests that cSDH is caused by neo-membranes formed around the subdural haematoma cavity leading to microbleeds from the fragile neo-capillaries within these membranes, reinforced by profibrinolytic and inflammatory factors within the subdural fluid, leading to the maintenance or enlargement of the haematoma [5].
Description of the technique
Under general anaesthesia, in a supine position, the head is placed in a horseshoe and rotated to the contralateral side so that the frontal burr hole can be placed at the highest point. This step is important to avoid postoperative pneumocephalus. Prophylactic anticonvulsant medication is not applied routinely, whilst all patients receive a single shot of antibiotics (cefuroxime) 30 min prior to skin incision. Typically, the frontal burr hole is placed over the intersection of the superior temporal line and the coronal suture, and the parietal burr hole is placed above the parietal tuber, approximately 7–8 cm behind the frontal one. Depending on the maximum width of the haematoma, the placement of the burr holes is adjusted if needed. After draping, two incisions are made 3 cm in length over the abovementioned points. Following the burr holes, haemostasis of the bone is achieved with bone wax and the dura mater is coagulated. A cruciate durotomy is performed, followed by coagulation of the dural leaflets against the skull. The haematoma is then evacuated with extensive irrigation using warm saline solution. The irrigation process is continued until the evacuated fluid from the subdural space becomes clear. During the process of irrigation, it is important to pay attention that a communication between the burr holes exists and that the cortex is visible in the depth. If the cortex is not visible or no good communication exists, visible membranes within the haematoma cavity should be addressed. In such cases, our routine is not to remove the membranes but solely to create a communication between the different compartments within the haematoma cavity created by the membranes. Membranes that are not visible and seem to block the communication between the burr holes can be perforated using a nelaton catheter connected to a syringe using continuous irrigation. Alternatively, for membranes lying on the surface of the brain, bipolar forceps or a pointed hook is carefully used to perforate the membranes and evacuate the trapped haematoma. We try to avoid these manoeuvres if possible and take great care during these potentially risky manoeuvres, which are only performed under good vision. After the whole haematoma is evacuated and the cortex is visible in the depth, a drain is placed in all patients. Drain placement is essential, since it is the only factor proven to reduce recurrence rates [4]. Our routine is to insert a subperiosteal drain (SPD) since it showed comparable recurrence rates to the insertion of a subdural drain (SDD), whilst infection and misplacement rates are significantly lower [6]. A clamp is inserted from the parietal burr hole, between the bone and the periosteum towards the frontal burr hole. The passive Jackson-Pratt (Cardinal Health, Dublin, OH, USA) drain is retrieved using the clamp and tunnelled back towards the parietal burr hole (Fig. 1). The drain is externalised approximately 3 cm behind the parietal burr hole and is sutured to the skin to avoid dislocation. Placement of any material covering the burr holes (e.g. bone dust or Spongostan) must be avoided, since a communication between the subdural space and the subperiosteal space is imperative for further drainage of the haematoma by the drain. Thereafter, closure of the subcutis and skin is completed, beginning with the parietal wound. Irrigating the subdural space through the frontal burr hole with warm saline solution and clamping the drain during frontal skin closure are essential in order to avoid pneumocephalus. Finally, the frontal wound is closed using subcutaneous sutures and staples for the skin.

Surgical steps of the subperiosteal drain placement. a Overview of the cranium after burr holes are performed and the chronic subdural haematoma is evacuated. b Insertion of a clamp subperiosteally and retrieving the end of the drain. c The drain is pulled through towards the parietal burr hole. d Using a scalpel, a stab incision is performed approximately 3 cm behind the parietal burr hole. Subperiosteal tunnelling towards the parietal burr hole and the drain is externalised. e The drain is pulled through until the perforated part lies over the two burr holes. f The frontal part of the drain is cut and adjusted to the right length, and the frontal tip is placed subperiosteally using a dissector. g It is crucial that the burr holes are left open to ensure communication between the subdural space and the subperiosteal space. h Wound closure in ordinary fashion and fixation of the drain to avoid drain dislocation
Indications
The main indication for burr hole trepanation (BHT) is chronic or subacute subdural haematoma with significant midline shift, haematoma thickness of > 10 mm, or if neurologic symptoms are apparent. Asymptomatic small haematomas without significant mass effect are often managed conservatively. This surgery can be done under general or local anaesthesia and does not have an age limit.
Limitations
Although BHT is considered the gold standard for the treatment of cSDH, some controversies concerning the operative method and techniques still exist. Twist drill craniostomy, craniotomy, and embolization of the middle meningeal artery are techniques discussed within the literature [9]. The amount of burr holes needed, intraoperative irrigation, opening of membranes, postoperative bed rest, and placement of an active or passive drain remain controversial issues [8, 9]. In addition, various pharmacological treatments of cSDH (e.g. corticosteroids, tranexamic acid, and statins) have been proposed, whilst results from ongoing randomised controlled trials (RCT) are awaited [7].
How to avoid complications
Beyond the abovementioned technical nuances, we stress one issue: the placement of a SPD. After Santarius et al. performed a RCT, showing significant reduction of recurrence rates of surgically drained cSDHs with SDD insertion compared with no drain, the current standard should be to insert a drain [4].
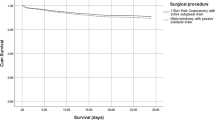
Our group showed in a further RCT that the insertion of a SDD was associated with significantly lower infection and drain misplacement rates compared with patients with SDD [6]. The rate of recurrence of cSDH was lower in the SPD group as well but without statistical significance.
Specific perioperative considerations
Patients who suffer from cSDH are often under anticoagulant (AC) or platelet inhibitor (PI) therapy, whilst guidelines for the management of these patients are still lacking [1,2,3, 7].
Our routine is to remove the drainage regardless of the amount of drained fluid 48 h postoperatively. During this time, patients are kept in a flat position whilst mobilisation is kept to a minimum and is only done with a clamped drain. Postoperative CT imaging is not conducted on a routine basis, and thrombosis prophylaxis is commenced on the first postoperative day [2].
Specific information to give to the patient about surgery and potential risks
It is possible that the burr holes have to be transformed into a small bone flap due to unsuccessful evacuation of haematoma. Further, the risk for recurrence in approximately 9% of the cases, in addition to the risk of infections, acute postoperative bleeding, and seizures, should be discussed with the patient [6].
References
Kamenova M, Lutz K, Schaedelin S, Fandino J, Mariani L, Soleman J (2016) Does early resumption of low-dose aspirin after evacuation of chronic subdural hematoma with burr-hole drainage Lead to higher recurrence rates? Neurosurgery 79(5):715–721
Licci M, Kamenova M, Guzman R, Mariani L, Soleman J (2018) Influence of postoperative thrombosis prophylaxis on the recurrence of chronic subdural hematoma after burr-hole drainage. Crit Care Med 46(1):e26–e32
Poon MTC, Al-Shahi Salman R (2018) Association between antithrombotic drug use before chronic subdural haematoma and outcome after drainage: a systematic review and meta-analysis. Neurosurg Rev 41(2):439–445
Santarius T, Kirkpatrick PJ, Ganesan D et al (2009) Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: a randomised controlled trial. Lancet 374(9695):1067–1073
Santarius T, Kirkpatrick PJ, Kolias AG, Hutchinson PJ (2010) Working toward rational and evidence-based treatment of chronic subdural hematoma. Clin Neurosurg 57:112–122
Soleman J, Lutz K, Schaedelin S, Kamenova M, Guzman R, Mariani L, Fandino J (2019) Subperiosteal vs subdural drain after burr-hole drainage of chronic subdural hematoma: a randomized clinical trial (cSDH-drain-trial). Neurosurgery 85(5):E825–E834
Soleman J, Nocera F, Mariani L (2017) The conservative and pharmacological management of chronic subdural haematoma. Swiss Med Wkly 147:w14398
Unterhofer C, Freyschlag CF, Thomé C, Ortler M (2016) Opening the internal hematoma membrane does not alter the recurrence rate of chronic subdural hematomas: a prospective randomized trial. World Neurosurg 92:31–36
Weigel R (2003) Outcome of contemporary surgery for chronic subdural haematoma: evidence based review. J Neurol Neurosurg Psychiatry 74(7):937–943
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Key points
- BHT is considered, to date, the gold standard surgical technique for drainage of cSDH.
- BHT of cSDH is indicated in symptomatic patients or haematomas leading to a significant space-occupying effect.
- The insertion of a drain after BHT of cSDH significantly reduces the recurrence rate.
- The insertion of a SPD should be encouraged.
- After haematoma irrigation, the cortex surface should be visible; otherwise, membranes need to be carefully perforated.
- Avoid wide opening or removal of membranes, due to the risk of seizures.
- The SPD is placed over both burr holes, without sealing them off, in order to allow communication between the subdural space and the SPD.
- The parietal wound should be closed first, to allow continuous irrigation frontally, preventing pneumocephalus.
- The passive SPD is left in situ for 48 h, and the patients should be kept in a flat position.
- Postoperative CT scans are not routinely performed, and thrombosis prophylaxis is administered on the first postoperative day.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Neurosurgery general
Electronic supplementary material
Video showing the drainage of a right-sided chronic subdural haematoma by double burr hole trepanation and the stepwise insertion of a subperiosteal drain (MP4 281,130 kb)
Rights and permissions
About this article

Cite this article
Ebel, F., Guzman, R. & Soleman, J. Burr hole trepanation and insertion of a subperiosteal drain for chronic subdural haematoma: how I do it. Acta Neurochir 162, 2707–2710 (2020). https://doi.org/10.1007/s00701-020-04442-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-020-04442-2