
Abstract
Background
Mechanical thrombectomies (MT) in stroke have changed the standard treatment regimen with a continuous increase of MTs during the last years. A subsequent reduction in the rates of decompressive craniectomies (DC) as well as a change in clinical characteristics of patients undergoing an additional DC after MT may be assumed. Therefore, objective of this study was to investigate the influence of nowadays regularly performed MT on patients undergoing DC.
Methods
Patients with DC due to cerebral infarctions between January 2009 and January 2018 were included. Patients’ clinical presentation and surgical parameters were collected retrospectively. Initial GCS and NIHSS, extent of the stroke, time interval from symptom onset to DC, and neurological outcome were compared between patients with and without thrombectomy.
Results
A total of 5469 ischemic strokes were treated in the investigated period, leading to DC in 119 cases (2.2%). A decrease in the rate of performed DCs was recorded: in 2009, 2.8% of ischemic stroke patients underwent surgery compared to 1.9% in 2017. In the meantime, the number of MTs in our center has increased from 84 in 2014 to 160 in 2017. MT was performed in 32 patients prior to DC. No significant differences could be seen between the groups regarding age, initial NIHSS (median 18 in both groups, p = 0.81), extent of the infarctions prior to DC (median ASPECTS 0 in both groups, p = 0.87), time interval from symptom onset to DC, and neurological outcome.
Conclusions
The introduction of routinely performed MT as part of the standard treatment regimen for ischemic stroke has led to a decrease in DCs. However, DC patients with and without MT showed no differences regarding their initial clinical criteria and outcome. These results suggest that earlier DC studies in patients with MCA infarction also apply for the collective of thrombectomized patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Decompressive craniectomy (DC) is a well-established neurosurgical intervention in patients suffering from malignant infarction of the middle cerebral artery (MCA). While prospective randomized trials showed a decrease in mortality and an improvement in functional recovery, mechanical thrombectomies (MT) were not part of the standard treatment regimen in stroke patients back then [12, 16, 17, 26, 27].
In recent years, multiple randomized controlled trials showed a benefit for endovascular treatment in terms of functional outcome at 90 days and underlined the importance of MT as a further effective tool in large vessel occlusions that limits the extent of ischemic brain damage [5, 6, 10, 15, 24]. A significant reduction in the number of malignant infarctions and mortality rates due to endovascular treatment was demonstrated by Fuhrer et al. [7].
It may be assumed that with the introduction of MT, the clinical characteristics of patients undergoing an additional DC have changed. Additionally, one may expect a reduction in the overall rate of decompressive craniectomies after implementation of MT as has been demonstrated recently [3, 4, 22, 25].
In this context, the aim of this study was to investigate the influence of nowadays regularly performed mechanical thrombectomies on patients undergoing DC.
With regard to their clinical course and outcome, we compared patients undergoing DC subsequently to mechanical thrombectomy to those patients in whom MT was not a component of the treatment.
Methods and materials
All patients undergoing DC due to malignant MCA infarction between January 2009 and January 2018 were included in this study. To investigate the influence of MT on the collective of patients with DC, only infarctions of thrombotic or embolic origin were analyzed. Patients who underwent MT prior to DC were compared to DC patients without endovascular treatment.
Clinical data
Patients’ demographics and clinical data, including sex, age, laboratory findings, side of DC, and the number of modifiable cardiovascular risk factors (CVRF) were collected retrospectively. CVRF included hypercholesterolemia, arterial hypertension, diabetes mellitus, obesity, nicotine and alcohol abuse, and chronic renal insufficiency. Additionally, initial National Institutes of Health Stroke Scale (NIHSS) and the time interval from symptom onset to DC were compared between patients with and without thrombectomy. Functional outcome was assessed via modified Rankin Scale (mRS) at the end of rehabilitation.
Imaging and treatment
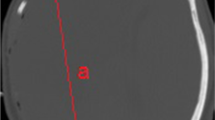
The extent of the stroke prior to surgery was determined using the Alberta Stroke Program Early CT score (ASPECTS) on CT imaging (Fig. 1).

Collecting the Alberta Stroke Program Early CT Score (ASPECTS). 1 point is deducted from the initial score of 10 for every MCA vascular territory involved. Case courtesy of Dr. Subash Thapa, Radiopaedia.org, rID: 40018
The indication for endovascular treatment was predominantly based on a multimodal CT examination: non-enhanced CT, CT angiography, and, in about half of the cases, an additional CT perfusion. In 11% of all patients, a magnetic resonance imaging was performed.
Endovascular treatment in our institution included access via an 8 F femoral sheath and an 8 F guiding catheter/balloon catheter for the carotid artery. An access via brachial, radial, or carotid puncture was not performed in this series. The degree of reperfusion achieved was quantified using the TICI-score which has been described by Higashida et al. [11].
Early decompressive craniectomy was performed in patients at risk of malignant cerebral swelling. Each indication was verified by an interdisciplinary team of the senior neurosurgeon and neurologist in charge, based on patient’s characteristics (age, medical history, laboratory findings), neurological condition, and neuroradiological imaging. This strategy corresponds with the current guideline of the German Society of Neurology, which recommends making the decision for or against DC on an individual basis [13].
A question mark–shaped skin incision was made fronto-parieto-temporal, ending approximately 10 mm anterior of the tragus, followed by retraction of the musculocutaneous flap, removal of the bone flap, and dural opening [14, 23].
Anticoagulants taken by patients before the event are discontinued perioperatively or, if possible, antagonized. A single thrombocyte aggregation inhibition might be maintained perioperatively, depending on the initial indication. In cases of dual antiplatelet therapy, the ADP receptor antagonist is paused.
Statistics
Statistical analyses were performed using IBM SPSS® v. 23 (IBM Corp., Armonk, NY, USA). Univariate analysis was performed using chi-squared tests or ANOVA tests, depending on the scale of the measurements, to examine correlations between the parameters. Probability values of p < 0.05 were considered statistically significant.
This study was conducted according to the Declaration of Helsinki, local and institutional laws, and was reported to the local ethical committee (No.: WF-09/19).
Results
The number of patients with ischemic strokes treated in our institution has increased annually in recent years. While 465 ischemic strokes were recorded in 2009, the admission rate increased to 731 in 2017 (Fig. 2). During this period, the absolute number of DCs remained constant at an average of 13 per year, while a relative decrease in the rate was recorded: in 2009, 2.8% of ischemic stroke patients underwent surgery, compared with 1.9% in 2017 (Fig. 2). During this period, mechanical thrombectomies were introduced and doubled in number within 3 years from n = 84 in 2014 to n = 160 in 2017 (see also Fig. 2).

Temporal development of ischemic infarction, thrombectomy, and DC
In total 119 DCs due to malignant MCA infarction were performed between January 2009 and January 2018. Ninety-six patients (59 males; 61.5%) were eligible for inclusion due to thrombotic or embolic origin of the infarction. One third (n = 32) of these patients had undergone MT prior to surgery. TICI-scores from 0 to 3 were reported in this group, while successful reperfusion (TICI-score 2b/3) was achieved in 13 patients (40.7%, Table 1).
In comparison, DC patients without thrombectomy had no statistically significant differences with respect to their clinical characteristics: both groups did not differ in age, sex, or neurological status at admission including the presence of anisocoria (Table 2).
Comparing thrombectomized and non-thrombectomized patients, the mean age was 54 vs. 54.7 years and the proportion of female patients was 37.5 and 39.1%, respectively. Median initial NIHSS was 18 in thrombectomized patients vs. 18 in non-thrombectomized patients. The mean number of modifiable cardiovascular risk factor was 1.5 vs. 1.7. No differences could be seen on laboratory findings at admission such as C-Reactive Protein (CRP) (16.2 and 28.4 mg/dl, respectively) or hemoglobin (8.6 vs. 8.4 mmol/l). Likewise, the groups did not differ regarding coagulation parameters such as international normalized ratio (INR) or partial thromboplastin time (PTT) (Table 2). The time between onset of symptoms and surgery did not differ significantly in the groups. In addition, there was no difference in the ASPECT score, describing the same extent of infarction on CT-imaging (median 0 in both groups).
No significant difference could be shown regarding the neurological outcome after completion of rehabilitation. The mRS was assessed 372 days after surgery (mean) and did not differ in the groups with median scores of 4 in both groups.
Discussion
The encouraging results of mechanical thrombectomies in stroke patients have changed the standard treatment regimen with a continuous increase of MTs during the last years. At our institution, we could record a parallel relative decline in the number of decompressive craniectomies. This decrease is most likely attributable to the increase in interventional treatments. This trend following the introduction of routine thrombectomies has also been described in other studies [3, 4, 22, 25].
In our cohort of MT patients that required DC, 40% of the patients had a successful MT with a TICI-score of 2b or more on final angiography (complete or nearly complete reperfusion). The fact that these patients required DC suggests that even successful MT does not exclude all patients from life-threatening clinical courses requiring decompressive surgery. The outcome of the MT depends on various factors: in addition to the timing and success of the revascularization, some patients also experience very early severe infarct edema, which is not reversible despite thrombectomy [20, 21]. Therefore, in some cases, an operation remains necessary even after a successful MT.
Patients who had undergone thrombectomy prior to surgery did not differ from those without MT regarding their clinical parameters. Elevated CRP and anemia at admission have been described as prognostic markers for worse outcome in infarct patients [9, 18]. Our patient groups did not differ in this respect. Likewise, no differences were found between the groups with respect to cardiovascular risk factors as indicators of the cardiovascular risk profile of patients [8, 19]. Radiologically, the ASPECT-score is reported to have a prognostic significance regarding the functional outcome [1, 2]. No differences between patient groups could be found regarding the extent of the infarct, quantified by ASPECT-score or the functional outcome. Furthermore, an endovascular treatment performed prior to craniectomy did not lead to a delay of the surgery as there were no differences between patient groups regarding the timing of the operation.
Although our study has some limitations in its retrospective and single-center character, the results support the thesis that present studies on decompressive craniectomy in malignant MCA infarction can be compared to previous data and that they are still valid in times of thrombectomy due to a comparable patient collective [12, 16, 17, 26, 27].
In conclusion, the introduction of routinely performed mechanical thrombectomy as part of the standard treatment regimen for ischemic stroke has led to a relative decrease in decompressive craniectomies over time. Nevertheless, a successful thrombectomy does not seem to be a guarantee that surgical decompressive craniectomy will not be required in some patients.
Since DC patients with and without MT showed no differences regarding their initial clinical criteria and outcome, the following conclusions can be drawn: on the one hand, it can be concluded that mechanical thrombectomy does not increase the risks of subsequently performed DC since the outcome in the groups did not differ. On the other hand, these results further suggest that earlier studies on DC in patients with malignant MCA infarction also apply today for the collective of mechanically thrombectomized patients as the collectives are comparable.
References
Aviv RI, Mandelcorn J, Chakraborty S, Gladstone D, Malham S, Tomlinson G, Fox AJ, Symons S (2007) Alberta Stroke Program Early CT Scoring of CT perfusion in early stroke visualization and assessment. AJNR Am J Neuroradiol 28:1975–1980. https://doi.org/10.3174/ajnr.A0689
Barber PA, Demchuk AM, Zhang J, Buchan AM (2000) Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group Alberta Stroke Programme Early CT Score. Lancet 355:1670–1674
Beez T, Steiger HJ (2019) Impact of randomized controlled trials on neurosurgical practice in decompressive craniectomy for ischemic stroke. Neurosurg Rev 42:133–137. https://doi.org/10.1007/s10143-018-0967-8
Beez T, Munoz-Bendix C, Steiger HJ, Beseoglu K (2019) Decompressive craniectomy for acute ischemic stroke. Crit Care 23:209. https://doi.org/10.1186/s13054-019-2490-x
Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, Schonewille WJ, Vos JA, Nederkoorn PJ, Wermer MJ, van Walderveen MA, Staals J, Hofmeijer J, van Oostayen JA, Lycklama A, Nijeholt GJ, Boiten J, Brouwer PA, Emmer BJ, de Bruijn SF, van Dijk LC, Kappelle LJ, Lo RH, van Dijk EJ, de Vries J, de Kort PL, van Rooij WJ, van den Berg JS, van Hasselt BA, Aerden LA, Dallinga RJ, Visser MC, Bot JC, Vroomen PC, Eshghi O, Schreuder TH, Heijboer RJ, Keizer K, Tielbeek AV, den Hertog HM, Gerrits DG, van den Berg-Vos RM, Karas GB, Steyerberg EW, Flach HZ, Marquering HA, Sprengers ME, Jenniskens SF, Beenen LF, van den Berg R, Koudstaal PJ, van Zwam WH, Roos YB, van der Lugt A, van Oostenbrugge RJ, Majoie CB, Dippel DW, Investigators MC (2015) A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 372:11–20. https://doi.org/10.1056/NEJMoa1411587
Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, Yan B, Dowling RJ, Parsons MW, Oxley TJ, Wu TY, Brooks M, Simpson MA, Miteff F, Levi CR, Krause M, Harrington TJ, Faulder KC, Steinfort BS, Priglinger M, Ang T, Scroop R, Barber PA, McGuinness B, Wijeratne T, Phan TG, Chong W, Chandra RV, Bladin CF, Badve M, Rice H, de Villiers L, Ma H, Desmond PM, Donnan GA, Davis SM, Investigators E-I (2015) Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 372:1009–1018. https://doi.org/10.1056/NEJMoa1414792
Fuhrer H, Schonenberger S, Niesen WD, Seide S, Meyne J, Gerner ST, Vollmuth C, Beck C, Meckel S, Schocke M, Wodarg F, Huttner HB, Mohlenbruch MA, Kieser M, Ringleb P, Neugebauer H, group IG-s (2019) Endovascular stroke treatment’s impact on malignant type of edema (ESTIMATE). J Neurol 266:223–231. https://doi.org/10.1007/s00415-018-9127-x
Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, Creager MA, Culebras A, Eckel RH, Hart RG, Hinchey JA, Howard VJ, Jauch EC, Levine SR, Meschia JF, Moore WS, Nixon JV, Pearson TA, American Heart Association Stroke C, Council on Cardiovascular N, Council on E, Prevention, Council for High Blood Pressure R, Council on Peripheral Vascular D, Interdisciplinary Council on Quality of C, Outcomes R (2011) Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 42:517–584. https://doi.org/10.1161/STR.0b013e3181fcb238
Gong X, Zou X, Liu L, Pu Y, Wang Y, Pan Y, Soo YO, Leung TW, Zhao X, Wang Y, Wong KS (2013) Prognostic value of inflammatory mediators in 1-year outcome of acute ischemic stroke with middle cerebral artery stenosis. Mediat Inflamm 2013:850714. https://doi.org/10.1155/2013/850714
Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, Roy D, Jovin TG, Willinsky RA, Sapkota BL, Dowlatshahi D, Frei DF, Kamal NR, Montanera WJ, Poppe AY, Ryckborst KJ, Silver FL, Shuaib A, Tampieri D, Williams D, Bang OY, Baxter BW, Burns PA, Choe H, Heo JH, Holmstedt CA, Jankowitz B, Kelly M, Linares G, Mandzia JL, Shankar J, Sohn SI, Swartz RH, Barber PA, Coutts SB, Smith EE, Morrish WF, Weill A, Subramaniam S, Mitha AP, Wong JH, Lowerison MW, Sajobi TT, Hill MD, Investigators ET (2015) Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 372:1019–1030. https://doi.org/10.1056/NEJMoa1414905
Higashida RT, Furlan AJ, Roberts H, Tomsick T, Connors B, Barr J, Dillon W, Warach S, Broderick J, Tilley B, Sacks D, Technology Assessment Committee of the American Society of I, Therapeutic N, Technology Assessment Committee of the Society of Interventional R (2003) Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke 34:e109–e137. https://doi.org/10.1161/01.STR.0000082721.62796.09
Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB, investigators H (2009) Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol 8:326–333. https://doi.org/10.1016/S1474-4422(09)70047-X
Huttner H (2018) Intrakranieller Druck (ICP), S1-Leitlinie, 2018 in: Deutsche Gesellschaft für Neurologie (Hrsg.), Leitlinien für Diagnostik und Therapie in der Neurologie. http://www.dgn.org/leitlinien Accessed 05.02. 2019
Johnson RD, Maartens NF, Teddy PJ (2011) Technical aspects of decompressive craniectomy for malignant middle cerebral artery infarction. J Clin Neurosci 18:1023–1027. https://doi.org/10.1016/j.jocn.2010.12.025
Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, San Roman L, Serena J, Abilleira S, Ribo M, Millan M, Urra X, Cardona P, Lopez-Cancio E, Tomasello A, Castano C, Blasco J, Aja L, Dorado L, Quesada H, Rubiera M, Hernandez-Perez M, Goyal M, Demchuk AM, von Kummer R, Gallofre M, Davalos A, Investigators RT (2015) Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med 372:2296–2306. https://doi.org/10.1056/NEJMoa1503780
Juttler E, Schwab S, Schmiedek P, Unterberg A, Hennerici M, Woitzik J, Witte S, Jenetzky E, Hacke W, Group DS (2007) Decompressive Surgery for the Treatment of Malignant Infarction of the Middle Cerebral Artery (DESTINY): a randomized, controlled trial. Stroke 38:2518–2525. https://doi.org/10.1161/STROKEAHA.107.485649
Juttler E, Unterberg A, Woitzik J, Bosel J, Amiri H, Sakowitz OW, Gondan M, Schiller P, Limprecht R, Luntz S, Schneider H, Pinzer T, Hobohm C, Meixensberger J, Hacke W, Investigators DI (2014) Hemicraniectomy in older patients with extensive middle-cerebral-artery stroke. N Engl J Med 370:1091–1100. https://doi.org/10.1056/NEJMoa1311367
Kellert L, Martin E, Sykora M, Bauer H, Gussmann P, Diedler J, Herweh C, Ringleb PA, Hacke W, Steiner T, Bosel J (2011) Cerebral oxygen transport failure?: decreasing hemoglobin and hematocrit levels after ischemic stroke predict poor outcome and mortality: STroke: RelevAnt Impact of hemoGlobin, Hematocrit and Transfusion (STRAIGHT)--an observational study. Stroke 42:2832–2837. https://doi.org/10.1161/STROKEAHA.110.606665
O'Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, Rangarajan S, Islam S, Pais P, McQueen MJ, Mondo C, Damasceno A, Lopez-Jaramillo P, Hankey GJ, Dans AL, Yusoff K, Truelsen T, Diener HC, Sacco RL, Ryglewicz D, Czlonkowska A, Weimar C, Wang X, Yusuf S, investigators I (2010) Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 376:112–123. https://doi.org/10.1016/S0140-6736(10)60834-3
Peng G, Huang C, Chen W, Xu C, Liu M, Xu H, Cai C (2019) Risk factors for decompressive craniectomy after endovascular treatment in acute ischemic stroke. Neurosurg Rev. https://doi.org/10.1007/s10143-019-01167-4
Rocha M, Jovin TG (2017) Fast versus slow Progressors of infarct growth in large vessel occlusion stroke: clinical and research implications. Stroke 48:2621–2627. https://doi.org/10.1161/STROKEAHA.117.017673
Rumalla K, Ottenhausen M, Kan P, Burkhardt JK (2019) Recent Nationwide impact of mechanical thrombectomy on decompressive hemicraniectomy for acute ischemic stroke. Stroke 50:2133–2139. https://doi.org/10.1161/STROKEAHA.119.025063
Sahuquillo J, Arikan F (2006) Decompressive craniectomy for the treatment of refractory high intracranial pressure in traumatic brain injury. Cochrane Database Syst Rev:CD003983. https://doi.org/10.1002/14651858.CD003983.pub2
Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, Albers GW, Cognard C, Cohen DJ, Hacke W, Jansen O, Jovin TG, Mattle HP, Nogueira RG, Siddiqui AH, Yavagal DR, Baxter BW, Devlin TG, Lopes DK, Reddy VK, du Mesnil de Rochemont R, Singer OC, Jahan R, Investigators SP (2015) Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 372:2285–2295. https://doi.org/10.1056/NEJMoa1415061
Sporns PB, Minnerup J, Warneke N, Dziewas R, Hanning U, Berkemeyer S, Zoubi T, Heindel W, Schwindt W, Niederstadt T (2017) Impact of the implementation of thrombectomy with stent retrievers on the frequency of hemicraniectomy in patients with acute ischemic stroke. Clin Neuroradiol 27:193–197. https://doi.org/10.1007/s00062-015-0478-8
Vahedi K, Hofmeijer J, Juettler E, Vicaut E, George B, Algra A, Amelink GJ, Schmiedeck P, Schwab S, Rothwell PM, Bousser MG, van der Worp HB, Hacke W, Decimal D, investigators H (2007) Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials. Lancet Neurol 6:215–222. https://doi.org/10.1016/S1474-4422(07)70036-4
Vahedi K, Vicaut E, Mateo J, Kurtz A, Orabi M, Guichard JP, Boutron C, Couvreur G, Rouanet F, Touze E, Guillon B, Carpentier A, Yelnik A, George B, Payen D, Bousser MG, Investigators D (2007) Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL trial). Stroke 38:2506–2517. https://doi.org/10.1161/STROKEAHA.107.485235
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Neurosurgical intensive care
Rights and permissions
About this article

Cite this article
Göttsche, J., Flottmann, F., Jank, L. et al. Decompressive craniectomy in malignant MCA infarction in times of mechanical thrombectomy. Acta Neurochir 162, 3147–3152 (2020). https://doi.org/10.1007/s00701-019-04180-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-019-04180-0