
Abstract
Purpose
Percutaneous thermal ablation is used for treating hepatic tumors. Recent advances in laparoscopy and imaging modalities have led to the development of a novel image-guided minimally invasive loco-regional treatment. The aim of this trial was to apply laparoscopic assistance to magnetic resonance (MR) image-guided thermoablation instead of ultrasonography, because of its various advantages.
Methods
Patients with hepatic tumors and liver cirrhosis underwent magnetic resonance (MR) image-guided laparoscopic microwave coagulation therapy using a borescope and endoscopic forceps. Six cases of laparoscopic microwave coagulation treatment using MR image guidance were successfully performed between January 2000 and December 2008. Tumors were detected, punctured, and ablated in an open-configured MR scanner. A total of nine hepatocellular carcinoma nodules were preoperatively identified in S3, S5 and S6 (mean diameter = 20.8 ± 5.4 mm).
Results
MR-guided microwave coagulation was laparoscopically achieved in all patients without any significant complications that required invasive treatment. The mean length of the operation was 275.3 ± 60.5 min, and the mean postsurgical hospital stay was 10.0 ± 2.3 days. Postoperative confirmation scanning was performed without moving the patients.
Conclusion
MR-guided laparoscopic microwave coagulation therapy is an effective treatment for hepatic tumors adjacent to other organs, as it allows for more accurate detection of lesions and for tumors to be treated safely while avoiding adjacent organs. It is less invasive than conventional procedures, because the MR real-time guidance enabled continuous monitoring throughout the procedure.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Surgical resection is the optimal curative treatment for primary liver malignancies, but it is sometimes not possible because of the poor physical condition or other medical problems of the patients. Such unresectable tumors have recently been treated using loco-regional therapies, such as cryotherapy [1, 2], lasers [3], radiofrequency ablation (RFA) [4] and microwave coagulation therapy (MCT) [5–7] as minimally invasive, safe and effective treatment modalities for achieving tumor destruction [8, 9]. Recently, laparoscopy-assisted loco-regional treatments were performed for tumors that were difficult to approach percutaneously because of their location and/or the presence of intra-abdominal adhesions [10–13].
Recent advances in imaging modalities have enabled not only ultrasonography (US), but also computed tomography (CT) and magnetic resonance (MR) imaging, to be used as guidance for loco-regional treatment [14, 15]. Among these, MR possesses many advantages for image guidance during surgical procedures because it is free from X-ray irradiation, has good soft tissue contrast, is suitable even for tissues with air and bone, and is flexible in terms of the image plane control. For these reasons, we developed a novel interventional MR-guided surgical system (IVMR) using a vertical type open-configured MR scanner for continuous real-time guidance during the surgical procedure. Over 200 cases of percutaneous MCT have been performed on the IVMR system [16–21]. In this study, we applied laparoscopic assistance to this system for patients with hepatic tumors who were not able to be treated via a percutaneous approach.
Materials and methods
Indications
The following criteria were the indications for patients with hepatocellular carcinoma (HCC) to undergo MR-guided MCT (IVMR-MCT): (1) tumor diameter up to 3 cm; (2) number of tumors confirmed, less than three and (3) tumor location, not attached to the major Glisson’s sheath [21]. A general assessment using the Child–Pugh classification was made at the time of the patient’s entry into the study. If preoperative assessment revealed severe impairment of the liver function (Child–Pugh C), patients were excluded from the procedure.
Patients
Laparoscopic-assisted IVMR-MCT was performed in six patients who fulfilled the inclusion criteria. The patient characteristics are listed in Table 1. The mean age of the patients was 65.3 years. All six patients had liver cirrhosis (hepatitis B:C = 3:3) as a background factor, which was diagnosed as grade A or B according to the Child–Pugh classification (A:B = 3:3). One patient had a surgical history of laparotomy, and another had undergone percutaneous MCT. Informed consent was obtained from all cases, and the procedure followed all of the guidelines for experimental investigation with human subjects required by the institution.
Surgical procedure
All procedures were performed using an open-configured MR scanner (Fig. 1; 0.5 T Signa SP/i; General Electric Healthcare, Milwaukee, WI, USA) and under general anesthesia. After a pneumoperitoneum of 11–14 mmHg was created using an open technique, a 10-mm trocar was inserted above the umbilicus. The 5-mm diameter borescope (Fig. 2; Karl Storz, Tuttlingen, Germany) and forceps for endoscopic surgery were made of weakly magnetic materials. After the first laparoscopic exploration of the abdominal cavity, the second and third 10-mm trocars were inserted at the epigastric fossa and right hypocondrium, respectively (Fig. 3). In ordinary cases, three trocars were used during the laparoscopic MCT procedure. These were used for the examination of the liver to confirm the preoperative volume data and navigate the puncture line (Fig. 4). Detected tumors were marked on pictures obtained using our original surgical navigating application [17].

The open-configured MR scanner (Signa SP/I 0.5T, General Electric Healthcare, Milwaukee, WI, USA). The scanner was used for intraoperative real-time navigation during microwave coagulation therapy. The surgery was performed under general anesthesia using the MR scanner. A liquid crystal monitor was placed in front of the surgeons to allow them to monitor the real-time MR images

The instruments we used a magnetic resonance (MR)-compatible borescope with a 5-mm diameter (Karl Storz, Tuttlingen, Germany). This did not affect the real-time MR images and induced only an eddy current

The procedure after a pneumoperitoneum of 11–14 mmHg was created using an open technique, two or three trocars were inserted above the umbilicus or at other points. An optical tracking device was used to detect the tumor location

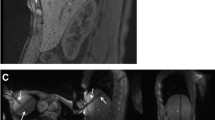
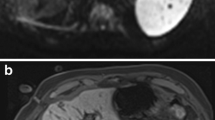
The intraoperative navigation monitoring for surgeons images similar to this figure were shown on the liquid crystal monitor placed in front of the surgeons. Upper images: a real-time image and laparoscopic view. Lower images: synchronized preoperative images acquired using the open-configured magnetic resonance scanner immediately before the operation
Hepatic tumors were coagulated with a microwave coagulation system (Microtaze, Model HSD20M; Alfresa Corporation, Tokyo, Japan). An MR-compatible needle (Daum Corp, Chicago, IL, USA) was introduced into the liver using a percutaneous approach. Using IVMR navigation, MCT at 60 W for 180 s was performed, and this was repeated until the treated area encompassed the entire tumor.
On postoperative day 7, the patients underwent enhanced CT scanning studies to confirm the ablated area, and were discharged if they had no postsurgical complications, such as hemorrhage, liver abscess or liver dysfunction.
Results
Between January 2000 and December 2008, 210 patients with hepatic tumors were treated with IVMR-MCT using an open MR scanner. In all MCT cases, laparoscopic-assisted punctuation was performed in six patients because their tumors were in contact with the visceral structures adjacent to the liver. The postoperative course of the cases is shown in Table 2. The mean total length of the operation was 275.3 ± 60.5 min. Nine HCC nodules were preoperatively identified, i.e., four patients had a solitary lesion and two patients had two or three lesions. The tumors were located in S3, S5 or S6. The mean diameter of the tumors was 20.8 ± 5.4 mm. IVMR-MCT was laparoscopically completed in all patients. No intraoperative or postoperative hemorrhage occurred, and no patient required a transfusion. The mean postoperative hospital stay was 10.0 ± 2.3 days. A cholecystectomy was performed in one case (Case 3). In this case, pleural effusion occurred, but resolved without drainage. Two patients (Cases 3 and 5) experienced HCC recurrence in another segment of liver within 1 year and died 502 and 652 days after the treatment, respectively. These two cases had been diagnosed with cirrhotic hepatitis C 11 and 5 years earlier, respectively. Case 6 died due to distant recurrence, and Case 4 died of lung cancer at another hospital (Table 2).
Discussion
Patients with untreatable hepatic tumors have a poor prognosis. Liver resection may not be indicated for such patients with advanced cancer or liver dysfunction. Thus, novel treatment modalities and approaches for patients with HCC should aim not only for a potential cure or control of hepatic disease, but should also be a minimally invasive treatment to allow for improved recovery and to allow more patients to undergo the procedure.
In the 1970s, Tabuse et al. [22] developed a microwave tissue coagulator that has been clinically applied for liver resection. Many patients and reports describing the outcomes of MCT for hepatic tumors have confirmed its efficacy and safety [5, 23]. Moreover, laparoscopic assistance is applied to thermal ablation for liver malignancies which exist in unapproachable locations [24]. CT and US have generally been used as the navigation tools for MCT [25]. However, these modalities have respective disadvantages. For example, one of the major issues associated with CT guidance is the radiation exposure, and the fact that the technique cannot be applied for real-time monitoring. US guidance is most widely used as a real-time image-guided modality. However, it sometimes has image disturbances owing to the generation of microbubbles. Therefore, there is a significant disadvantage regarding the use of US guidance. This disadvantage occasionally prevents repeated puncture, even if residual lesions are apparently observed after the initial ablation [16]. On the other hand, real-time MR image monitoring enables not only multiple punctures, but also confirmation scanning, without the need to move the patient from the operating room.
Using the MR-guided navigation system, we have successfully performed MCT at our institution since 2000 [16–21]. Seventy-three patients with liver malignancies adjacent to the diaphragm underwent a thoracoscopic procedure [26] and six patients with tumors adjacent to intra-abdominal organs were required to undergo a laparoscopic procedure.
Microwaves are expected to provide an equivalent or greater efficacy than RFA in the treatment of malignancy [24]. In addition, microwaves do not affect the MR images, and can be used in IVMR because they generally operate between 915 MHz and 2.45 GHz [27]. In contrast, RFA is operated at a frequency of approximately 500 kHz, which will affect MR images. The IVMR system enabled real-time navigation during the entire procedure while using microwaves as an energy source [16].
It is difficult for real-time MR imaging to detect the boundary between treated and untreated lesions after MCT. The safety margin is the most important factor for achieving the optimal treatment outcome [28–30]. To improve the accuracy of MCT, we developed a “Footprint” system [31]. A session of coagulation therapy produces an oval-shaped treated lesion. Based on this lesion, a football-shaped Footprint was placed at the heat center of the electrode on the navigation MR images [17].
MR navigation including the Footprint system should improve the prognosis in patients with liver malignancy adjacent to other organs and with severe liver dysfunction.
In comparison with the outcomes of previous studies of laparoscopy-assisted MCT (LMCT), IVMR-guided laparoscopic MCT (IVMR-LMCT) was not associated with as many complications as LMCT with US guidance [32]. Seki et al. [12] reported 68 cases treated with US-guided LMCT for HCC. In their report, the mean operation lasted 110 ± 29.4 min, and the five-year survival rate was 43 %. They experienced pleural effusions in some cases, which were treated conservatively. As there have been few randomized trials comparing the guidance modalities for LMCT, more studies of IVMR-LMCT in patients with the appropriate indications are necessary, and should be performed to evaluate the feasibility and accuracy of the treatment.
Recently, vertical type open-configured MR scanners have become outdated. Horizontal scanners are also not used widely, and have replaced by wide-bore scanners. Nevertheless, we still expect to make use of our experience by employing flexible endoscopes or surgical manipulators adjusted to the MR environment.
Conclusion
Laparoscopic MCT is an alternative and minimally invasive treatment for patients with unresectable hepatic tumors adjacent to other visceral organs. MR real-time guidance was introduced successfully instead of US guidance, and it improved the visibility and work-flow of laparoscopic MCT.
References
Seifert JK, Junginger T, Morris Dl. A collective review of the world literature on hepatic cryotherapy. J R Coll Surg Edinb. 1998;43:141–54.
Gilbert JC. Current advances in interventional MRI guided cryosurgery. Eur Radiol. 1997;7:1165.
Mack MG, Straub R, Eichler K, Engelmann K, Zangos S, Roggan A, et al. Percutaneous MR imaging-guided laser-induced thermotherapy of hepatic metastases. Abdom Imaging. 2001;26:369–74.
Rossi S, Di Stasi M, Buscarini E, Cavanna L, Quaretti P, Squassante E, et al. Percutaneous radiofrequency interstitial thermal ablation in the treatment of small hepatocellular carcinoma. Cancer J Sci Am. 1995;1(1):73–81.
Poon RT, Fan ST, Tsang FH, Wong J. Locoregional therapies for hepatocellular carcinoma: a critical review from the surgeon’s perspective. Ann Surg. 2002;235:466–86.
Ido K, Isoda N, Sugano K. Microwave coagulation therapy for liver cancer: laparoscopic microwave coagulation. J Gastroenterol. 2001;36:145–52.
Stattner S, Primavesi F, Yip VS, Jones RP, Ofner D, Malik HZ, et al. Evolution of surgical microwave ablation for the treatment of colorectal cancer liver metastasis: review of the literature and a single centre experience. Surg Today 2014 (Online First).
Head HW, Dodd GD III. Thermal ablation for hepatocellular carcinoma. Gastroenterology. 2004;127:167–78.
Ng KK, Poon RT. Radiofrequency ablation for malignant liver tumor. Surg Oncol. 2005;14:41–52.
Cillio U, Vitale A, Dupuis D, Corso S, Neri D, Damico, et al. Laparoscopic ablation of hepatocellular carcinoma in cirrhotic patients unsuitable for liver resection or percutaneous treatment: A cohort study. PLoS One 2013;8(2):1–8.
Santambrogio R, Opocher E, Montorsi M. Laparoscopic radiofrequency ablation of hepatocellular carcinoma: a critical review from the surgeon’s perspective. J Ultrasound. 2008;11:1–7.
Seki S, Sakaguchi H, Iwai S, Kadoya H, Kabayashi S, Kitada T, et al. Five-year survival of patients with hepatocellular carcinoma treated with laparoscopic microwave coagulation therapy. Endoscopy. 2005;37(12):1220–5.
Imura S, Shimada M, Utsunomiya T, Morine Y, Wakabayashi G, Kaneko H. Current status of laparoscopic liver surgery in Japan: results of a multicenter Japanese experience. Surg Today. 2014;44(7):1214–9.
Jolesz FA, Morrison PR, Koran SJ, Kelley RJ, Hushek SG, Newman RW, et al. Compatible instrumentation for intraoperative MRI: expanding resources. J Magn Reson Imaging. 1998;8(1):8–11.
Moscatel MA, Shellock FG, Morisoli SM. Biopsy needles and devices: assessment of ferromagnetism and artifacts during exposure to a 1.5-T MR system. J Magn Reson Imaging. 1995;5(3):369–72.
Morikawa S, Inubushi T, Kurumi Y, Naka S, Sato K, Tani T, et al. MR-guided microwave thermocoagulation therapy of liver tumors: initial clinical experiences using a.5 T open MR system. J Magn Reson Imaging. 2002;16:576–83.
Sato K, Morikawa S, Inubushi T, Kurumi Y, Naka S, Haque HA, et al. Alternate biplanar MR navi- gation for microwave ablation of liver tumors. Magn Reson Med Sci. 2005;4:89–94.
Morikawa S, Inubushi T, Kurumi Y, Naka S, Sato K, Demura K, et al. Feasibility of respiratory triggering for MR-guided microwave ablation of liver tumors under general anesthesia. Cardiovasc Intervent Radiol. 2004;27:370–3.
Morikawa S, Inubushi T, Kurumi Y, Naka S, Sato K, Tani T, et al. New assistive devices for MR-guided microwave thermocoagulation of liver tumors. Acad Radiol. 2003;10:180–8.
Morikawa S, Inubushi T, Kurumi Y, Naka S, Sato K, Demura K, et al. Advanced computer assistance for magnetic resonance-guided microwave thermocoagulation of liver tumors. Acad Radiol. 2003;10:1442–9.
Kurumi Y, Tani T, Naka S, Shiomi H, Shimizu T, Abe H, et al. MR-guided microwave ablation for malignancies. Int J Clin Oncol. 2007;12:85–93.
Tabuse K. A new operative procedure of hepatic surgery using a microwave tissue coagulator. Nippon Geka Hokan. 1979;48:160–72.
Murakami R, Yoshimatsu S, Yamashita Y, Matsukawa T, Takahashi M, Sagara K. Treatment of hepatocellular carcinoma: value of percutaneous microwave coagulation. AJR Am J Roentgenol. 1995;164(5):1159–64.
Laeseke PF, Lee FT, Sampson LA, van der Weide DW, Brace CL. Microwave ablation versus radiofrequency ablation in the kidney: high-power triaxial antennas create larger ablation zones than similarly sized internally cooled electrodes. J Vasc Interv Radiol. 2009;20(9):1224–9.
Okamoto T, Onda S, Yanaga K, Suzuki N, Hattori A. Clinical application of navigation surgery using augmented reality in the abdominal field. Surg Today 2014 (Online First).
Shiomi H, Naka S, Sato K, Demura K, Murakami K, Shimizu T, et al. Thoracoscopy-assisted magnetic resonance guided microwave coagulation therapy for hepatic tumors. Am J Surg. 2008;195(6):854–60.
Brace CL. Microwave tissue ablation: biophysics, technology and applications. Crit Rev Biomed Eng. 2010;38(1):65–78.
Mukaisho K, Kurumi Y, Sugihara H, Naka S, Kamitani S, Tsubosa Y, et al. Enzyme histochemistry is useful to assess viability of tumor tissue after microwave coagulation therapy (MCT): metastatic adenocarcinoma treated by lateral segmentectomy after MCT. Dig Dis Sci. 2002;47(11):2441–5.
Yamaguchi T, Mukaisho K, Yamamoto H, Shiomi H, Kurumi Y, Sugihara H, et al. Disruption of erythrocytes distinguishes fixed cells/tissues from viable cells/tissues following microwave coagulation therapy. Dig Dis Sci. 2005;50:1347–55.
Murakami K, Morikawa S, Naka S, Demura K, Sato K, Shiomi H, et al. Correlation between high field MR images and histopathological findings of rat transplanted cancer immediately after partial microwave coagulation. Magn Reson Med Sci. 2008;7(3):105–12.
Morikawa S, Inubushi T, Kurumi Y, Naka S, Sato K, Demura K, et al. Advanced computer assistance for magnetic resonance-guided microwave thermocoagulation of liver tumors. Acad Radiol. 2013;10(12):1442–9.
Simo KA, Sereika SE, Newton KN, Gerber DA. Laparoscopic-assisted microwave ablation for hepatocellular carcinoma: safety and efficacy in comparison with radiofrequency ablation. J Surg Oncl. 2011;104:822–9.
Acknowledgments
The authors would like to thank Enago (www.enago.jp) for the English language review.
Conflict of interest
Koichiro Murakami and co-authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Murakami, K., Naka, S., Shiomi, H. et al. Initial experiences with MR Image-guided laparoscopic microwave coagulation therapy for hepatic tumors. Surg Today 45, 1173–1178 (2015). https://doi.org/10.1007/s00595-014-1042-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-014-1042-x