
Abstract
Background
Calcaneal fractures are often major injuries associated with considerable morbidity. The optimal surgical management of displaced calcaneal fractures remains contentious with open, percutaneous and arthroscopically assisted percutaneous approaches all offering potential benefits for patients. The aim of this study was to assess which of these three separate surgical approaches to the management of displaced calcaneal fractures provides the best radiographic deformity correction.
Methods
This is a retrospective observational study of all calcaneal fractures undergoing operative fixation at a single major trauma centre in the UK. The primary outcome was pre- and post-operative assessment of the deformity correction using radiographic parameters (angle of Gissane and Bohler’s angle). Secondary outcomes included fracture configuration, complications and re-operation rate.
Results
Between 01/01/2009 and 31/12/2019, 152 calcaneal fractures in 134 patients underwent operative management via either an open or percutaneous approach. One-way ANOVA testing of the pre- and post-operative radiographic parameters demonstrated that an open approach offered superior post-operative correction of Bohler’s angle when compared to percutaneous alone (p < 0.05); however, there was no difference in post-operative angle of Gissane (p > 0.05). The mean follow-up for complication and re-operation data was 3.5 years (range 0.1–12.4). Overall complication rate following all surgical fixation was 7.2% with a further 32.2% requiring further long-term surgical intervention for subtalar arthritis or removal of metalwork.
Conclusion
Arthroscopically assisted percutaneous fixation does not offer superior radiographic deformity correction compared to percutaneous technique alone. Open fixation yielded improved correction of Bohler’s angle when compared to percutaneous alone; however, there was no difference in post-operative angle of Gissane.
Level of evidence: III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fractures of the calcaneus constitute 2% of all fractures and are the most common fracture of the tarsal bones [1,2,3]. These high-energy injuries frequently occur in young males following a fall from height or road traffic collision [3, 4]. They are challenging to manage and subsequent osteoarthritis of the subtalar joint is associated with significant morbidity [5,6,7,8,9]. Anatomical restoration of the articular surface and calcaneal shape has been shown to predict greater functional outcome scores [4].
Controversy exists over the best management of displaced intra-articular calcaneal fractures [10, 11]. Surgical options include open reduction and internal fixation (ORIF) through an extended lateral approach or sinus tarsi incision, minimally invasive reduction with percutaneous fixation (MIRPF) or primary arthrodesis [12,13,14,15,16]. Prospective randomised controlled trials have failed to achieve a consensus on whether operative intervention provides any long-term functional benefit over conservative management [10, 17,18,19]. The UK Heel Fracture Trial [17] reported a significantly higher complication rate in operatively managed injuries though an extended lateral approach, performed within 3 weeks of injury. However, only 7.5% of all calcaneal fractures attending hospitals were enrolled in this trial during the study period. The generalisability of this trial remains contentious within the orthopaedic community.
Anatomical reduction of the articular surface may help reduce the risk of pain from subsequent subtalar arthritis in a generally active patient cohort, often requiring a good level of mobility to continue working. However, other important aims of surgery are to correct the overall calcaneal shape, restoring calcaneal height, width and correcting out of varus. This aims to prevent the additional secondary problems of calcaneofibular impingement from the lateral wall blowout, a locked midfoot from the hindfoot varus and anterior ankle impingement from loss of the usual talar calcaneal angle. There remains debate about the relative importance of calcaneal shape versus subtalar joint reduction in these fractures.
Percutaneous or minimally invasive approaches may reduce disruption to the soft tissue envelope and lower the risk of complications [20, 21]. A variety of such techniques have been described including K-wire fixation, cannulated screw fixation and calcaneal nail (C-nail) [22]. A percutaneous approach offers the potential to correct shape, avoiding the risks of larger incisions, relying on fluoroscopy to judge joint reduction. The use of arthroscopy to assist with joint reduction has also been described [23]. A recent systematic review of the literature found a total of 8 studies looking at outcomes from percutaneous arthroscopically assisted fixation, concluding the technique provides a good alternative with low complication rates [24]. The optimal surgical management of displaced calcaneal fractures remains contentious with open, percutaneous and AA-perc approaches all offering potential benefits for patients.
Aims and objectives
The aim of this study was to assess which surgical approach (open, percutaneous or AA-perc) for the management of displaced calcaneal fractures provided the best radiographic deformity correction.
Methods
Study design
This is a retrospective observational study of consecutive patients with a calcaneal fracture who underwent operative management with either an open, percutaneous or AA-perc surgical approach.
Study setting
This study took place at a single Major Trauma Centre in the UK. All operations were performed by one of six consultant foot and ankle or trauma surgeons.
Study outcomes
The primary outcome was pre- and post-operative assessment of the deformity correction using radiographic parameters. The specific parameters chosen were the angle of Gissane and Bohler’s angle which were assessed according to the original literature recommendations [25,26,27] (Fig. 1). Secondary outcomes included complications and re-operation rates.

Normal lateral weight-bearing radiograph of calcaneum demonstrating a angle of Gissane and b Bohler’s angle
Participants
The inclusion criteria for this study were patients aged 16 years and older who presented with an open or closed calcaneal fracture and underwent operative intervention using either an open, percutaneous or AA-perc surgical approach. The decision for operative fixation was made in a multidisciplinary trauma meeting with consultant consensus. The technique chosen represents an evolution in our departmental philosophy in the treatment of these fractures, which has predominantly moved to percutaneous fixation. The addition of arthroscopy is individual surgeon choice, with no clear departmental guidelines. Non-operative calcaneal fractures were excluded. Fractures are managed non-operatively if they are very minimally displaced or if patients were not fit for surgery. Rarely highly comminuted fractures are managed non-operatively if the consensus opinion is that the fracture is unreconstructable. A decision was made to compare these three groups in order to understand the difference between open and percutaneous approaches as well as the impact of arthroscopic assistance on radiographic outcomes.
Data collection
Data including patient demographics, radiographic parameters, operative fixation technique and complications were retrospectively collected in August 2021 from hospital records. Data collection was conducted using a standardised proforma. All assessment of radiographic parameters, fracture configuration and classification was conducted by a fellowship-qualified surgeon. Radiographic assessment of fracture configuration (assessed using the Essex-Lopresti and Sanders classifications) and deformity correction was based on non-weight-bearing lateral foot and axial calcaneal radiographs.
Operative technique
All patients were managed under general anaesthesia. Intravenous antibiotics were given on induction. Tourniquet use was at the discretion of the operating surgeon. A pre-operative CT scan was obtained in all patients to aid pre-operative planning.
Open technique
When the soft tissue swelling has improved the patient is typically positioned in the lateral position, operated side upwards. An extended lateral incision is used as described by Eastwood and Atkins [28]. A full thickness flap is elevated protecting the sural nerve and peroneal tendons. This allows direct access to that whole lateral calcaneum and visualisation into the posterior facet of the subtalar joint. Intra-articular joint depression-type fractures can be reduced by folding out the blown out lateral wall, elevating the depressed posterior facet fragments and correcting the calcaneal tuberosity out of varus. The fracture is then stabilised with a low-profile small fragment calcaneal plate. The wound is closed with deep interrupted absorbable sutures and interrupted nylon to skin, and care is taken to avoid tension on the skin edges. The patient is typically placed in a backslab for 2 weeks to protect the wound. Once healed, patients are transitioned into a walking boot and allowed non-weight-bearing foot and ankle range of motion. Weight bearing is usually started from 6 weeks.
Percutaneous technique
The patient is typically positioned in the lateral position operative side upwards. There is no need to wait for soft tissue swelling to settle. Depending on surgeon choice, the patient can be positioned with the lower limb prone (either patient entirely prone or in the floppy lateral position with the operative side down, which with hip external rotation allows the ankle to be positioned prone). A tourniquet is usually not required. The aim of this technique is similar to open surgery, to correct the tuberosity out of varus, correct height and length, reduce the lateral wall blow out and elevate the depressed posterior facet fragments. Surgery is performed under fluoroscopic guidance. The exact sequence of reduction manoeuvres depends on surgeon choice and fracture configuration. The tuberosity position is usually addressed first. Two large guidewires from the cannulated screw system are inserted parallel from a posterosuperior entry point in the tuberosity. They aim plantarward. They are advanced as far as the primary fracture line and then used to joystick the tuberosity restoring length, pulling it down to restore height and out of varus. This helps to disimpact the depressed posterior facet joint fragments. If there is poor hold in the fragment, a 5 mm Steinmann pin can be inserted to aid the manoeuvre.
A periosteal elevator or equivalent is inserted through a percutaneous lateral stab incision under the depressed posterior facet lateral fragment. These fragments can then be elevated under fluoroscopic guidance. When the joint reduction is achieved, the guidewire for a small cannulated screw is inserted through this fragment and into the sustentaculum tali, often through an additional incision. Typically a partially threaded headed screw is used to apply some compression. They final position of the tuberosity is then confirmed clinically and fluoroscopically before the large guidewires are advanced into the anterior process. Following this, if a good wire position is not achieved others can be inserted to replace them. Two large fully threaded headed cannulated screws are then inserted, acting as positional screws for the tuberosity and raft screws to support the posterior facet reduction (Fig. 2). A ‘kickstand’ screw can be inserted for further stability. This screw runs from the plantar posterior position of the tuberosity with the tip ending under the lateral posterior facet fragment.

Pre- and post-operative radiographs demonstrating percutaneous fracture reduction and fixation of a calcaneal fracture
Arthroscopically assisted percutaneous technique
This technique follows the same operative steps as the percutaneous technique. The major difference is the use of arthroscopy as an adjunct for visualisation of the reduction of the posterior facet. We typically use 2 sinus tarsi portals, but occasionally a posterior approach is used with standard posterolateral and posteromedial portals. A standard 30-degree, 4.0-mm knee arthroscope and an arthroscopic shaver are used to achieve adequate visualisation. The fracture haematoma is cleared allowing excellent visualisation of the posterior facet of the subtalar joint. Under arthroscopic visualisation, the posterior facet can be reduced percutaneously using a periosteal elevator or similar. Percutaneous screw placement and reduction of the tuberosity are performed as described for the percutaneous technique.
Statistical analysis (including power calculation)
A post hoc power calculation was performed, and sample size calculations were based on an independently established data of radiographic deformity correction following surgical fixation of calcaneal fractures. A sample of 31 feet in each group was estimated to give a power of 0.80 and an alpha risk of 5%. The paired t test was used to compare pre- and post-operative radiographic measurements. One-way ANOVA testing was used to determine whether there was any statistically significant difference between the means of the three groups. Categorical data were reported with descriptive statistics. Statistical significance was defined as a P value of less than 0.05.
Ethics and funding
This project was registered and approved by the trust Clinical Governance Department. This study was reported in line with STROBE [29] guidelines for reporting of observational studies. There was no funding to support this study. None of the authors have any financial conflicts of interest to declare.
Results
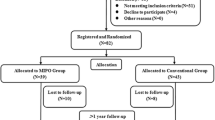
Between 01/01/2009 and 31/12/2019, 152 calcaneal fractures in 134 patients (91 males and 43 females). The mean age was 46.1 ± 13.9 (range 16.0–77.0) years. The median number of days from injury to operation was 4. Table 1 shows the patient demographics and classification of calcaneal fractures for patients included in the study. The mean follow-up for complication and re-operation data was 3.5 years (range 0.1–12.4). Complete pre- and post-operative imaging was available for 86.8% of cases (Table 2).
One-way ANOVA testing of the pre- and post-operative radiographic parameters was used to compare the deformity correction as shown in Table 3. All techniques showed a significant improvement in both angle of Gissane and Bohler’s angle. The open approach offered superior post-operative correction of Bohler’s angle when compared to percutaneous alone (p < 0.05); however, there was no difference in post-operative angle of Gissane. The addition of arthroscopy for percutaneous fixation did not significantly improve the deformity correction when compared to percutaneous fixation alone. Visualisation of the data is shown in Figs. 3 and 4.

Graph illustrating radiographic deformity correction of Bohler’s angle of calcaneal fracture stratified by operation type. Error bars demonstrate 95% confidence intervals

Graph illustrating radiographic deformity correction of angle of Gissane of calcaneal fracture stratified by operation type. Error bars demonstrate 95% confidence intervals
Five patients (n = 6 calcaneal fractures) died during the study period. The mean time from injury to death was 3.6 years (range 0.13–7.4). A thigh tourniquet was used in 48 cases (23 Percutaneous and 25 Open) with an average time of 87.9 min (range 26–137). Complication rates are high regardless of surgical technique. We observed 2 wound complications in the extended lateral group and 9 in those fixed percutaneously. One of the nine percutaneous complications required surgical debridement and metalwork removal. Both (2/2) of the wound complications seen in the extended lateral approach required debridement, metalwork removal and soft tissue coverage. There was a higher percentage of patients requiring subtalar fusion in the open group compared to either percutaneous or AA-perc. However, percutaneous surgery was associated with a higher re-operation rate for minor elective removal of metalwork (usually due to prominent screw heads causing secondary irritation once the fracture had united).
Discussion
This study has demonstrated that regardless of surgical technique, significant sagittal deformity correction can be achieved with either open or percutaneous surgery. The Open approach offered superior post-operative correction of Bohler’s angle when compared to percutaneous alone; however, there was no difference in post-operative angle of Gissane. Complication rates and re-operation rates are high for both open and percutaneous techniques. Although not statistically significant, wound complication in 2/2 patients who underwent open surgery required reconstructive surgery under the care of the plastic surgeons compared to none of the percutaneously fixed patients.
It remains unclear whether operatively treated calcaneal fractures have superior clinical outcomes than non-operatively treated [7, 10, 30], though a recent meta-analysis suggested that operative intervention does significantly reduce the rate of subtalar arthrodesis [3, 11]. Buckley et al. [10] demonstrated that a Bohler angle on presentation of < 0 degrees was 10 times more likely to require a secondary subtalar fusion than a Bohler angle on presentation of > 15 degrees and a Sanders type IV calcaneal fractures were 5.5 times more likely to be fused than a simple Sanders type II fracture. Non-operative care was six times more likely to lead to a late fusion as compared to open reduction and internal fixation treatment [31]. A greater proportion of calcaneal fractures treated with open reduction and internal fixation went on to undergo subtalar fusion whilst those treated with AA-perc fixation had the lowest proportion going on to subtalar fusion.
In this study, arthroscopic assistance to help in fracture reduction was not significantly improved over the standard percutaneous approach which is reflected by a recent systematic review which found that there is no evidence to support the routine use of arthroscopy in fracture reduction and fixation [23, 24, 32, 33]. There is a dearth of evidence looking specifically at calcaneal fractures, and this is certainly an avenue for future research [34,35,36].
In non-operatively treated intra-articular calcaneal fractures, Bohler's angle has been shown to decrease by 11 degrees in the subsequent year [37]. Numerous RCTs have shown that a severely depressed Bohler’s angle on presentation has a poor 2-year outcome regardless of treatment and worse functional outcomes [38], but correlation of improvement in/restoration of Bohler's angle after treatment with improved clinical outcomes has also been proved [39, 40] and disproved in multiple studies [19, 41]. Studies have suggested the Sanders and Essex-Lopresti classification of injury has greater prognostic value in functional outcomes [42], but not all studies are in agreement [10, 38, 41].
Bohler’s and Gissane’s angle restoration improves some but not all post-operative clinical outcome measures, where other radiological markers (calcaneal length, posterior facet height, length of posterior facet) had no correlation with the same outcomes [43]. Critically, the angle of Gissane is rarely utilised in the literature, but in some respects it performs better than Bohler's angle, particularly in relation to intra-observer error [44].
In this study, the groups were not completely heterogeneous, with more even distribution of Sanders type 2 and 3 fractures in the open fixation group, but more skewed towards type 3 fractures in the percutaneous and AA-perc group. This may represent a different mechanism of injury, with more high-energy injuries occurring in recent years (as open fixation was predominately performed in the early years of data set collection) or it may represent changes in surgical decision-making over the course of the study. Decision making may have changed relative to the intended aims of fixation (anatomical reduction, compared to restoration of calcaneal height, pitch and lateral wall congruity such that future subtalar arthrodesis yields an acceptable outcome). Open reduction may traditionally have been reserved for those cases where an anatomical reduction was deemed possible pre-operatively (as reflected in the tighter range of post-operative values from normal radiological values in the operative set of open procedures than in the percutaneous data set), and surgeons may have been more inclined to manage severe fracture patterns (Sanders 3 and 4) either non-operatively or with acute subtalar arthrodesis. The higher-energy cases may also have had significant soft tissue considerations that made open fixation a less viable option. Surgeons may be more inclined to undertake severe fracture patterns utilising a percutaneous approach due to less concerns over wound healing, a perceived ability to better restore bony architecture or due to changes in surgical aims from strict anatomical reduction. Restoration of calcaneal pitch, height and width is now regularly considered more important than anatomical restoration of the subtalar joint, particularly as many with severe fracture patterns will go on to subtalar arthrodesis in the future regardless of the surgical outcome. The rate of removal of metalwork in the percutaneous group can potentially be reduced in the future through advances in technology and design of screws, e.g. headless compression screws. This would give the percutaneous treatment option a more favourable re-operation profile.
Although open approach cases showed a more reliable restoration of near normal radiological values, the cases in the percutaneous and arthroscopically assisted data set were shown to have greater pre-operative articular deformity (50% Sanders II or IV) with worse mean Bohler's angles than the open approach data set.
Ultimately, surgical aims, including the implications for complications and future surgeries, will determine the most appropriate method of fixation. Other studies investigating the outcomes between percutaneous fixation with cannulated screws and open fixation show no difference in radiographic outcomes, complications and implant cost [45,46,47].
Limitations
This study was appropriately powered to investigate the radiological deformity correction following three different methods of surgical osteosynthesis following calcaneal fracture. This study, although retrospective in nature, had a large sample size with a mean 3-year follow-up for complications and re-operation.
Future directions
Importantly, this study lacks the use of validated foot-specific or health-related quality of life clinical patient-reported outcome measures. Further research would enable comparison between the different surgical techniques in terms of clinical as well as radiographic outcome.
Conclusion
The optimal surgical approach for the management of displaced calcaneal fractures remains contentious. The main finding from this study is that AA-perc fixation does not offer superior radiographic deformity correction compared to percutaneous technique alone. It also demonstrates a superior restoration of Bohler’s angle when using open compared to percutaneous methods. The clinical significance of this is unknown. Taking into account surgeon familiarity, we would propose percutaneous fixation ± arthroscopy for such injuries given reduced soft tissue insult and less severe complication profile. The role of arthroscopy to assist fracture reduction needs further research as in our series did not appear to improve anatomical restoration. Further work should also focus on the clinical patient-reported outcomes following the different surgical techniques used for operative management of calcaneal fractures.
Abbreviations
- AA-perc:
-
Arthroscopically assisted percutaneous fixation
- ORIF:
-
Open reduction internal fixation
- MIRPF:
-
Minimally invasive reduction with percutaneous fixation
- ANOVA:
-
Analysis of variance
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology
- RCT:
-
Randomised control trial
References
Humphrey JA, Woods A, Robinson AHN (2019) The epidemiology and trends in the surgical management of calcaneal fractures in England between 2000 and 2017. Bone Joint J 101-B:140–146
Mitchell MJ, McKinley JC, Robinson CM (2009) The epidemiology of calcaneal fractures. Foot 19:197–200
Majeed H, Barrie J, Munro W, McBride D (2018) Minimally invasive reduction and percutaneous fixation versus open reduction and internal fixation for displaced intra-articular calcaneal fractures: A systematic review of the literature. EFORT Open Rev 3:418–425
Sanders R (2000) Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 82:225–250
Law GW, Yeo NEM, Yeo W et al (2017) Subtalar arthroscopy and fluoroscopy in percutaneous fixation of intra-articular calcaneal fractures. J Orthop Surg 25:230949901668499
Alexandridis G, Gunning AC, Leenen LPH (2015) Patient-reported health-related quality of life after a displaced intra-articular calcaneal fracture: a systematic review. World J Emerg Surg 10:62
Bruce J, Sutherland A (2013) Surgical versus conservative interventions for displaced intra-articular calcaneal fractures. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD008628.pub2
Veltman ES, Doornberg JN, Stufkens SAS et al (2013) Long-term outcomes of 1,730 calcaneal fractures: systematic review of the literature. J Foot Ankle Surg 52:486–490
Lim EV, Leung JP (2001) Complications of intraarticular calcaneal fractures. Clin Orthop Relat Res 7–16
Buckley R, Tough S, McCormack R et al (2002) Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 84:1733–1744
Luo X, Li Q, He S, He S (2016) Operative versus nonoperative treatment for displaced intra-articular calcaneal fractures: a meta-analysis of randomized controlled trials. J Foot Ankle Surg 55:821–828
Bai L, Hou Y-L, Lin G-H et al (2018) Sinus tarsi approach (STA) versus extensile lateral approach (ELA) for treatment of closed displaced intra-articular calcaneal fractures (DIACF): a meta-analysis. Orthop Traumatol Surg Res 104:239–244
Nosewicz TL, Dingemans SA, Backes M et al (2019) A systematic review and meta-analysis of the sinus tarsi and extended lateral approach in the operative treatment of displaced intra-articular calcaneal fractures. Foot Ankle Surg 25:580–588
Yeap EJ, Rao J, Pan CH et al (2016) Is arthroscopic assisted percutaneous screw fixation as good as open reduction and internal fixation for the treatment of displaced intra-articular calcaneal fractures? Foot Ankle Surg 22:164–169
Tomesen T, Biert J, Frölke JPM (2011) Treatment of displaced intra-articular calcaneal fractures with closed reduction and percutaneous screw fixation. J Bone Joint Surg Am 93:920–928
Tantavisut S, Phisitkul P, Westerlind BO et al (2017) Percutaneous reduction and screw fixation of displaced intra-articular fractures of the calcaneus. Foot Ankle Int 38:367–374
Griffin D, Parsons N, Shaw E et al (2014) Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ 349:g4483
Meena S, Gangary SK, Sharma P (2016) Review Article: Operative versus nonoperative treatment for displaced intraarticular calcaneal fracture: a meta-analysis of randomised controlled trials. J Orthop Surg 24:411–416
Ibrahim T, Rowsell M, Rennie W et al (2007) Displaced intra-articular calcaneal fractures: 15-year follow-up of a randomised controlled trial of conservative versus operative treatment. Injury 38:848–855
Biz C, Barison E, Ruggieri P, Iacobellis C (2016) Radiographic and functional outcomes after displaced intra-articular calcaneal fractures: a comparative cohort study among the traditional open technique (ORIF) and percutaneous surgical procedures (PS). J Orthop Surg Res 11:92
Shams A, Gamal O, Mesregah MK (2021) Outcome of minimally invasive osteosynthesis for displaced intra-articular calcaneal fractures using cannulated screws: a prospective case series. J Foot Ankle Surg 60:55–60
Zwipp H, Paša L, Žilka L et al (2016) Introduction of a new locking nail for treatment of intraarticular calcaneal fractures. J Orthop Trauma 30:e88-92
Grün W, Molund M, Nilsen F, Stødle AH (2020) Results after percutaneous and arthroscopically assisted osteosynthesis of calcaneal fractures. Foot Ankle Int 41:689–697
Marouby S, Cellier N, Mares O et al (2020) Percutaneous arthroscopic calcaneal osteosynthesis for displaced intra-articular calcaneal fractures: Systematic review and surgical technique. Foot Ankle Surg 26:503–508
Böhler L (1931) Diagnosis, pathology, and treatment of fractures of the OS CALCIS. JBJS 13:75
Gissane W (1947) Discussion on “Fractures of the os calcis.” Proc Br Orthop Assoc J Bone Joint Surg Am 29:254–255
Essex-Lopresti P (1952) The mechanism, reduction technique, and results in fractures of the os calcis. Br J Surg 39:395–419
Eastwood DM, Atkins RM (1992) Lateral approaches to the heel A comparison of two incisions for the fixation of calcaneal fractures. Foot 2:143–147
von Elm E, Altman DG, Egger M et al (2007) Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335:806–808
Dhillon MS, Bali K, Prabhakar S (2011) Controversies in calcaneus fracture management: a systematic review of the literature. Musculoskelet Surg 95:171–181
Csizy M, Buckley R, Tough S et al (2003) Displaced intra-articular calcaneal fractures: variables predicting late subtalar fusion. J Orthop Trauma 17:106–112
Williams CE, Joo P, Oh I et al (2021) Arthroscopically assisted internal fixation of foot and ankle fractures: a systematic review. Foot Ankle Orthop 6:2473011420950214
Pastides PS, Milnes L, Rosenfeld PF (2015) Percutaneous arthroscopic calcaneal osteosynthesis: a minimally invasive technique for displaced intra-articular calcaneal fractures. J Foot Ankle Surg 54:798–804
Park CH (2019) Role of subtalar arthroscopy for displaced intra-articular calcaneal fractures. Clin Podiatr Med Surg 36:233–249
Sharr PJ, Mangupli MM, Winson IG, Buckley RE (2016) Current management options for displaced intra-articular calcaneal fractures: Non-operative, ORIF, minimally invasive reduction and fixation or primary ORIF and subtalar arthrodesis. A contemporary review. Foot Ankle Surg 22:1–8
Pujol O, Sallent A, Salom J et al (2023) ORIF assisted by open subtalar small joint arthroscopy for intra-articular displaced calcaneus fractures. Foot Ankle Orthop 8:24730114231163824
Bakker B, Halm JA, Van Lieshout EMM, Schepers T (2012) The fate of Böhler’s angle in conservatively-treated displaced intra-articular calcaneal fractures. Int Orthop 36:2495–2499
Loucks C, Buckley R (1999) Bohler’s angle: correlation with outcome in displaced intra-articular calcaneal fractures. J Orthop Trauma 13:554–558
Su Y, Chen W, Zhang T et al (2013) Bohler’s angle’s role in assessing the injury severity and functional outcome of internal fixation for displaced intra-articular calcaneal fractures: a retrospective study. BMC Surg 13:40
Kulkarni HG, Mane VS, Gaonkar KL et al (2015) Plating for intra-articular calcaneal fractures…. Is it an overkill? J Clin Orthop Trauma 6:153–159
Paul M, Peter R, Hoffmeyer P (2004) Fractures of the calcaneum. A review of 70 patients. J Bone Joint Surg Br 86:1142–1145
Gusic N, Fedel I, Darabos N et al (2015) Operative treatment of intraarticular calcaneal fractures: Anatomical and functional outcome of three different operative techniques. Injury 46(Suppl 6):S130–S133
Qiang M, Chen Y, Jia X et al (2017) Post-operative radiological predictors of satisfying outcomes occurring after intra-articular calcaneal fractures: a three dimensional CT quantitative evaluation. Int Orthop 41:1945–1951
Otero JE, Westerlind BO, Tantavisut S et al (2015) There is poor reliability of Böhler’s angle and the crucial angle of Gissane in assessing displaced intra-articular calcaneal fractures. Foot Ankle Surg 21:277–281
Pitts CC, Almaguer A, Wilson JT et al (2019) Radiographic and Postoperative Outcomes of Plate Versus Screw Constructs in Open Reduction and Internal Fixation of Calcaneus Fractures via the Sinus Tarsi. Foot Ankle Int 40:929–935
Wallin KJ, Cozzetto D, Russell L et al (2014) Evidence-based rationale for percutaneous fixation technique of displaced intra-articular calcaneal fractures: a systematic review of clinical outcomes. J Foot Ankle Surg 53:740–743
van Hoeve S, Poeze M (2016) Outcome of minimally invasive open and percutaneous techniques for repair of calcaneal fractures: a systematic review. J Foot Ankle Surg 55:1256–1263
Funding
The authors declare that no funds, grants or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Daniel Yeomans, Bradley Stone and Thomas Lewis. The first draft of the manuscript was written by Daniel Yeomans, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
This is an observational study. North Bristol NHS Trust has confirmed that no ethical approval is required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

{kind=link}
Cite this article
Yeomans, D., Lewis, T.L., Pearkes, T. et al. Radiological outcomes following open versus percutaneous fixation versus arthroscopically assisted percutaneous fixation of calcaneal fractures: a ten-year retrospective observational study. Eur J Orthop Surg Traumatol 34, 823–832 (2024). https://doi.org/10.1007/s00590-023-03716-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-023-03716-6