
Abstract
Multidirectional instability (MDI) of the shoulder is a condition where the dislocation occurs in more than one direction with minimal or no causative trauma. Its pathoanatomy is complex and characterized by a redundant capsule, resulting in increased glenohumeral joint volume. The fact that several further factors may contribute to symptom onset complicates the diagnosis and hampers the identification of a therapeutic approach suitable for all cases. There is general agreement that the initial treatment should be conservative and that surgery should be reserved for patients who have not responded to an ad hoc rehabilitation program. We review the biomechanics, clinical presentation, and treatment strategies of shoulder MDI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Multidirectional instability (MDI) of the shoulder was initially described by Neer and Foster as a condition where the dislocation occurs in more than one direction with minimal or no causative trauma [1]. Three patient groups have been identified based on the direction of dislocation: anterior-inferior with posterior subluxation, posterior-inferior with anterior subluxation, and global dislocation [1, 2]. Additional classifications including instability in two [3] or three directions [4, 5] have subsequently been introduced. TUBS (traumatic, unilateral, Bankart lesion, surgery) and AMBRI (atraumatic multidirectional, bilateral, rehabilitation, inferior capsular shift) were devised by Matsen et al. [6] to describe shoulder instability based on etiology, but this classification did not allow instability to be discriminated from hyperlaxity and microtrauma to be distinguished from macrotrauma. In 2002, Gerber and Nyffeler [7] introduced a novel classification of dynamic instability: unidirectional or multidirectional, with or without hyperlaxity. The latter system provides fresh insights, identifying different MDI populations that may respond differently to treatment. However, an exhaustive classification of shoulder instability is difficult to achieve, also due to the contribution of multiple factors [8]. The pathoanatomy of MDI due to ligamentous laxity is complex and is characterized by a redundant capsule, resulting in increased glenohumeral joint (GHJ) volume [9] caused by an excess of elastin in capsular tissue [10, 11].
Patients with MDI may be recurrent subluxators or dislocators [12]. However, since several factors can contribute to symptom onset, MDI diagnosis may be uncertain, hampering the identification of a treatment strategy suitable for all cases. There is general consensus that the initial approach should be conservative, whereas surgical treatment should be reserved for those cases that have not responded to an ad hoc rehabilitation program. However, the rate of patients eventually requiring surgery is unclear [13–16]. In this review, we describe the pathomechanics, clinical presentation, and treatment strategy of MDI.
Biomechanics of multidirectional instability
The hallmark of MDI is symptomatic inferior instability associated with anterior and/or posterior instability [1–5]. Capsule redundancy is a key predisposing factor. Dewing et al. [17] demonstrated elongation of capsular cross-sectional areas in MDI patients compared with healthy subjects and with patients with anterior or posterior instability, the elongation being more marked in the posterior-inferior capsular portion. Although some studies have highlighted a role for repetitive episodes of instability in the development of capsular laxity [18], Uhthoff and Piscopo [19] found a redundant capsule in 23 % of fetal and embryonic shoulders, concluding that a pouched and redundant anterior capsule may be a developmental variant rather the consequence of trauma; moreover, MDI is associated with generalized ligamentous laxity in a small number of cases [2]. Finally, the analysis of collagen and elastic fibers from the shoulder capsule of patients with unidirectional anterior instability, multidirectional instability undergoing primary surgery, multidirectional instability undergoing revision surgery, and subjects with no history of shoulder instability [10] showed similar capsule properties in patients with unidirectional and multidirectional instability; however, since the mean collagen fibril diameter was significantly smaller in skin from patients with primary multidirectional instability than in those with unidirectional anterior instability, the authors suggested the possibility of an underlying connective tissue abnormality [10].
Scapular position may be another factor contributing to MDI onset, since it influences the position of the glenoid both at rest and during arm movement. The resting scapular position has an internal rotation (IR) that is around 35° in most series [20–22] and a much more variable frontal inclination. Reduced scapular inclination worsens inferior shoulder instability; in contrast, increased inclination prevents inferior displacement of the humeral head (HH) by tightening the superior capsule, thus increasing the slope of the glenoid fossa, and also acts as a bony cam, tightening the overlying structures and stabilizing the HH in the glenoid fossa [23]. These findings have been confirmed by Warner et al. [24], who demonstrated that in patients with anterior shoulder instability, the scapula has a downward inclination compared with asymptomatic subjects. Although scapular static variations are important factors in MDI onset, the role of dynamic alterations is even more important. In normal arm elevation, the scapula rotates upward and externally and tilts posteriorly during shoulder elevation [21]. In MDI patients, scapulothoracic movements are increased from 90° to the end range of shoulder elevation [25]. In addition, during arm elevation, they show a pattern of upward rotation, anterior tilt, and excessive scapular IR [26]. This position eventually results in inhibition of subscapularis (SSC), lower trapezius, and serratus anterior muscle activation, and in increased activation of the pectoralis minor and latissimus dorsi muscles [27]. Furthermore, the contribution of the different rotator cuff (RC) components varies depending on position [28–32], and the “concavity-compression” mechanism is active throughout the range of motion (ROM) [30–33]. The result is a stabilizing mechanism sustained by low compression forces, such as those of resting muscle tone, which produces a strong resistance to translation [33, 34].
Since proprioception contributes to joint functional integrity and stability through a mechanism by which the neuromuscular control system works as a kind of “injury prophylactic” [35], impaired proprioception may also play a role in MDI [36, 37]. Recent findings from a 3D video motion analysis system that tracked limb position and determined spatial hand position error found a significantly greater error in subjects with MDI compared with control subjects [35].
Clinical evaluation and imaging
MDI symptom onset is often subtle in patients aged 20–30 years, who report non-specific activity-related pain [38] and frequently change lifestyle, either learning to avoid certain positions or developing compensatory routines to avoid inciting activities. The GHJ ROM may be normal or painful on the apprehension test [39]. Signs of generalized hyperlaxity may also be found, including elbow or metacarpophalangeal joint hyperextension, genu recurvatum, patellar instability, and the ability to rest the thumb on the ipsilateral forearm [38]. All Brighton’s criteria should be investigated to exclude benign joint hypermobility syndrome [40]. However, the term hyperlax is not precisely defined despite its frequent use; similarly, since joint laxity is variable among individuals [7], pathological laxity is also hard to define, which may explain the broad range of its reported prevalence [16, 41]. In clinical practice, hyperlaxity can be considered as a condition at risk of giving rise to a painful unstable shoulder. When a patient with a hyperlax shoulder sustains a macrotrauma, it may result in unidirectional instability; conversely, repetitive microtrauma may occur in a shoulder with prior anterior instability due to macrotrauma, resulting in symptomatic instability in more than one direction. MDI may also be found in patients with connective tissue disorders [42]. Impaired strength and athletic performance may be reported in association with pain and inciting activities, especially in subjects involved in overhead sports such as gymnastics, volleyball, and swimming. Among the clinical tests applied to assess shoulder instability [6, 39, 43–46], the sulcus sign [1] (Fig. 1), the load-and-shift test [44] (Fig. 2), and the hyperabduction test [47] (Fig. 3) are the most sensitive in diagnosing suspected MDI. Abnormal mobility in external rotation (ER) is another common finding in MDI patients (Fig. 4). Clinical examination is critical for voluntary instability, where the patient is able to cause a subluxation by voluntary muscle activation [11].These subjects tend to place the shoulder in IR, with a typical winging of the inferior medial tip of the scapula (type I dyskinesis) or of its entire border (type II dyskinesis) (Fig. 5a, b) [11]. The reasons for the abnormal scapular motion are hyperactivity of the internal rotators of the shoulder, anterior deltoid, pectoralis major, and latissimus dorsi, and a strongly reduced activity of the posterior deltoid and external rotators [11]. A positive sulcus sign and posterior shoulder subluxation when the arm is actively placed in IR is common in this condition, which is viewed as a form of MDI. Less frequently, patients can displace the HH anteriorly, or anteriorly and posteriorly. The drawer test [45] (Fig. 6a, b) and the load-and-shift test [44] are generally positive. Standard plain radiographs are usually taken to assess the relationship of the HH with the glenoid, which in static position is commonly preserved. Radiograms are also helpful in case of bone abnormalities, such as glenoid dysplasia/hypoplasia, glenoid bone loss, and HH defects. If bone deformity or abnormality is suspected, a multiplanar computed tomography scan in the axial and coronal planes can identify and quantify any bone defects and demonstrate GHJ stability. Nevertheless, bony abnormalities are not common in MDI patients due to their capsular laxity. Magnetic resonance imaging (MRI) is the gold standard to demonstrate MDI, because it provides excellent detail of soft tissues, especially of the capsule and ligaments. MR arthrography (MR-A) is more useful because capsule distension highlights the labrum, rotator interval (RI), and glenohumeral ligaments (GHL) [17] (Fig. 7).

Positive sulcus sign: When an inferior traction is applied to the arm, a dimple appears distal to the lateral aspect of the acromion

Load-and-shift test: Application of a small axial load results in anterior and posterior translation of the humeral head

Gagey hyperabduction test: The examiner pushes down the patient’s shoulder girdle while lifting the relaxed upper limb

Abnormal external rotation in a patient with generalized hyperlaxity

a–b Scapular dyskinesis. a Type I: winging of the inferior medial tip (left) and b type II: winging of the entire medial border (right)

a–b Drawer test: With the shoulder in 90° of abduction, the examiner draws the upper limb anteriorly (a) and posteriorly (b) (black arrows) to demonstrate the humeral head subluxation due to ligament laxity or insufficiency. The examiner can hold the scapula with the left hand to ensure that it does not move during the maneuver

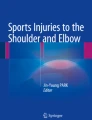
MR arthrogram. Abnormal glenohumeral joint volume in a patient with multidirectional instability. The arm is in abduction/external rotation (ABER image)
Although labral tears—due to microtrauma or less commonly to macrotrauma—may be present, the most common finding in MDI is a pathological capsule with an increased GHJ volume and RI dimension. Diagnostic signs and measures have recently been evaluated on MR arthrograms including standard and abduction/external rotation (ABER) images, to assess capsular redundancy in MDI [48]. On ABER images, the combination of an enhancing layer between HH and anterior-inferior GHL (AIGHL) (“crescent sign”) and a triangular space between HH, AIGHL, and the glenoid (“triangle sign”) was associated with good sensitivity (range 48–62 %) and excellent specificity (range 94–100 %) in diagnosing MDI, and the triangle sign was associated with HH decentering. RI herniation and width were not significantly different between MDI patients and subjects with stable shoulders [48]. Provencher et al. [49] also used MR-A to assess the relationship between increased RI and shoulder instability and found that the RI distance between the supraspinatus and SSC tendons was nearly identical in patients with unidirectional and multidirectional instability and did not differ from control groups. von Eisenhart-Rothe et al. [50] used open MRI for simultaneous 3D assessment of glenoid shape, HH centering, and scapular positioning in atraumatic shoulder instability. They calculated glenoid size based on an interpolated and 3D reconstructed dataset of the separated glenoid cavity; each contour point was connected to the closest point in the next slice to form a triangle, and glenoid size was then calculated by adding the size of all triangles. HH diameter was determined using a sphere that was fitted to the spherical load-bearing part of the HH using virtual reality software. Finally, a 3D GH index was calculated by dividing glenoid size by the radius of the HH. The authors reported that glenoid size, HH radius, and GH index tended to be smaller in both shoulders of subjects with instability compared with healthy shoulders. They also found that scapular IR was significantly increased in unstable compared with healthy shoulders, while assessment of HH centering demonstrated HH malcentering in the direction of instability in unstable shoulders in some arm positions.
Treatment strategy
Conservative treatment
Several studies have suggested that the initial therapeutic approach to MDI should be an ad hoc rehabilitation program [4, 13, 51], based on the rationale that strengthening of scapular and RC muscles would compensate for the lack of passive stability and assist in active control of the shoulder [52, 53]. Retraining of the concavity-compression mechanism combined with the activity of the scapular stabilizers also has the potential to improve shoulder stability [54]. In one of the earliest reports on the issue, published in 1956, Rowe [55] stated that most patients with atraumatic shoulder instability responded favorably to an exercise program during short-term follow-up. Burkhead and Rockwood reported good or excellent results in 80 % of 66 patients with MDI treated with a program of shoulder exercises [13]. Misamore et al. [56] reported the results of non-surgical treatment of 36 young, athletic subjects with MDI. At a mean follow-up of 8 years, pain outcomes were good or excellent in 23 patients and instability outcomes were good or excellent in 17; on the modified Rowe scale, results were excellent in five and good in 12 patients; the remaining 19 patients had a poor outcome; only eight subjects reported being free of all pain and instability. The authors concluded that MDI has a relatively poor response to non-surgical treatment in young athletic patients. Recently, Darlow et al. [57] described a three-step muscle retraining protocol derived from the concavity-compression program of Magarey et al. [54]. The first step consisted of isolated control of the local muscle system, then muscles were trained to control motion, and finally control was integrated into functional activities. In addition, taping and scapular muscle retraining were applied to improve GHJ stability through upward rotation and retraction of the scapula, to provide a stable base for RC cuff muscles. The use of external devices to influence muscle action is not new. Ide et al. [58] proposed a complex, 8-week, daily rehabilitation program associated with a novel shoulder orthosis that increases scapular inclination and scapular stability. It consists of RC and scapular stabilizer (serratus anterior and rhomboids) strengthening (Fig. 8), isometric exercises (resisted contraction for 8 s followed by 2 s rest) for IR and ER according to Burkhead and Rockwood’s program [13], and isotonic shoulder strengthening with a Thera-Band™. Scapular stabilizer strengthening and synchrony training of the scapulothoracic muscles were done with wall push-ups. These reports [13, 54, 58] highlight a scarcity of quality evidence in support of a specific exercise regimen in preference to another to guide clinicians in treating MDI with exercise in drill types or dosages [59]. In fact despite the publication of several rehabilitation protocols, there is little evidence of their relative value, and direct comparison of data from different papers is usually hampered by different patient selection and assessment methods.

Elastic resistance exercise for the rhomboid muscles: With the hips and knees flexed and the torso bent forward, the patient pulls the elastic band to the chest keeping the shoulder in 90° of abduction
The program usually starts with an exhaustive explanation of the problem and its etiology to the patient. Initially, the program should also include proprioceptive exercises, to improve joint position sense, and re-learning of correct movement patterns with the development of scapulothoracic and GH muscle strength and endurance. Mirrors, closed circuit TV, proprioceptive neuromuscular facilitation, and biofeedback may be used for correction and retraining of scapulothoracic and GHJ movement patterns. Stability can be enhanced by improving muscle balance and proprioception using strengthening and closed-chain exercises. An optimal rehabilitation protocol for subjects with voluntary shoulder instability is structured into (i) assessment and correction of abnormal muscle patterns and faulty posture, (ii) restoration of physiological active scapular motion, and (iii) muscle training and strengthening. The details of such a program are described in a recent paper [11].
Surgical procedures and results
When conservative treatment fails to restore shoulder stability, operative treatment is mandatory. A recent biomechanical study showed that MDI patients treated with capsular shift and physiotherapy exhibited better kinematic and muscle activity than subjects treated with physiotherapy alone [60]. Shoulder stabilization for symptomatic MDI can be performed with open or arthroscopic surgery, but arthroscopy has become the preferred method. Arthroscopic approaches to shoulder MDI include anterior, posterior, and pancapsular plication. Before beginning the surgical procedure, shoulder stability is examined under anesthesia (EUA) and compared with the contralateral shoulder; special attention is devoted to assessing anterior, posterior, and inferior shoulder laxity with the load-and-shift test and the sulcus sign as described above (clinical evaluation and imaging). Inferior laxity is diagnosed by a grade II sulcus sign (failure of capsular tightening with ER). Findings are correlated with preoperative MRI data and preoperative symptoms of instability. Open and arthroscopic techniques are described below.
Open capsular shift
The patient is placed in the beach chair position under general anesthesia combined with an interscalene block. A deltopectoral approach is used, with a 7- to 8-cm or shorter incision extending from the coracoid process to the axilla. The deltoid, the cephalic vein, and the pectoralis major are retracted, and the conjoint tendon is exposed and retracted medially. The SSC can be approached using a complete vertical tenotomy as described in the original standard procedure for open shoulder instability [61]; its musculo-tendinous insertion is detached 0.5–1 cm medial to the lesser tuberosity. Alternatively, it can be dissected using an inverted L-shaped tenotomy to preserve the anterior circumflex humeral vessels and the lower muscular attachment, thus reducing the risk of axillary nerve damage during the procedure [62]. A less invasive approach involves a muscle-sparing split along the direction of its fibers (SSC split) to prevent postoperative scarring and avoid any ER limitations or SSC insufficiency [63]. When using an SSC split, the muscle fibers are opened longitudinally at the junction of the middle and inferior thirds of the tendon, from the muscle tendon junction to the medial border of the long head of the biceps tendon. Then the capsule is exposed by blunt and sharp dissection—to free the inferior surface of the SSC tendon—and incised using a humeral-based T shape, with the short bar of the T being lateral and oriented longitudinally [1], or a glenoid-based T shape [2]. The dissection is continued inferiorly, and the inferior capsule is mobilized and rotated superiorly until the inferior recess is obliterated: This determines the amount of the shift superiorly; in some cases, complete obliteration of the recess cannot be obtained, because of a change in the position of the posterior band of the inferior GHL (IGHL); in such cases, a minor inferior recess can be accepted to avoid transecting the posterior IGHL band. The inferior flap of the ligament is then shifted superiorly deep into the superior limb and fixed with #2 non-absorbable suture. The inferior shift is closed by tightening the sutures with the arm in 45° of abduction and neutral rotation. The superior flap is then pulled down laterally and inferiorly and sutured to the mobilized inferior flap with the arm in adduction and neutral rotation. Associated SSC defects are treated as appropriate by direct repair of the tendon and/or closure and imbrication of the RI [64].
Arthroscopic capsular plication
This procedure is also performed under combined anesthesia. The patient is placed in lateral decubitus position with the shoulder in approximately 30° of abduction and 15° of forward flexion and a traction of 5 kg; the beach chair position can also be used. The arthroscopic procedure begins with the introduction of the optics into the GHJ through a posterior portal established about 2 cm inferior to the posterior acromial angle [65]. Next, the anterior-superior portal [66] is created by the inside-out technique using a Wissinger rod to identify the entry site and insert a 6-mm cannula behind the biceps tendon. An anterior portal to facilitate the procedure and afford direct visualization of the anterior capsule can be considered. The third, anterior-inferior portal [67] is established above the SSC tendon, just lateral and distal to the coracoid, by the outside-in technique using a spinal needle, to introduce an additional 8.5-mm threaded cannula.
Diagnostic arthroscopy, with systematic evaluation of the labrum, capsule, biceps tendon, SSC, rotator RI, RC, and articular surfaces, is conducted from the posterior portal. The decision to perform capsular plication-shift is based on a positive drive-through sign and a patulous axillary pouch. The posterior shoulder is evaluated through the anterior portal, looking specifically for a patulous posterior capsule, capsular tears, labral fraying, and posterior labral tears.
The anterior capsule and labrum are evaluated from the posterior portal, while the anterior portal is used for the instrumentation. The capsule is abraded with a rasp; in the absence of labral tears, a 45° suture passer is used to plicate the capsule 1 cm off the labrum at the 5:30-o’clock position on the glenoid and then advanced in a superomedial direction to the 4:30-o’clock position on the glenoid. This effectively advances the inferior capsule. Plication sutures (absorbable #0 PDS or polyglyconate) are placed up the face of the glenoid. The degree of tightening depends on the amount of capsular laxity encountered intraoperatively. At this point, the surgeon decides whether RI closure is also required. The issue is controversial, because there is no clear evidence for its actual value [65, 68]. Locking sliding knots are used to fold the capsule over itself. Then the arthroscope is passed through the anterior portal and the instrumentation through the posterior portal to assess and treat the posterior-inferior instability. Posterior-inferior capsular plication begins at the 6:30-o’clock position on the posterior-inferior labrum; 3–4 non-absorbable capsular plication sutures are placed by advancing up the glenoid similarly to the anterior-inferior procedure, their tightening depending on the amount of capsular laxity encountered. The sutures are tied with sliding locking knots backed up with three half stitches. At the end of the procedure, the shoulder is stabilized with the HH centered in the glenoid. Wiley et al. [69] described in detail a single-pleat technique that included capsular abrasion and then passing of a suture 1 cm lateral and inferior to the labrum, similar to the one just described. Although the capsular plication procedure described above is the one used most commonly, other arthroscopic techniques have also been suggested [68–72]. McIntyre et al. [70] first described a transglenoid technique for arthroscopic capsular shift. Through a capsular incision adjacent to the labrum, the IGHL is dissected so that it can be shifted superiorly; the anterior glenoid is freshened with a burr; multiple #0 or #2-0 PDS stitches are placed in the ligament and brought out posteriorly through a transglenoid hole; ligament release and placement of multiple stitches are also performed for the posterior labrum. Finally, the sutures are brought out and tied from a supraclavicular portal. Gartsman et al. [71] treated bidirectional instability arthroscopically using suture anchors to fix the labrum, capsular plication, thermal capsulorrhaphy, and RI closure. When the labrum was seen to be detached from the glenoid, the anchors were placed through the glenoid articular surface 1–2 mm from the lateral glenoid margin. The labrum was sutured so that it was in contact with the scapular neck and it extended onto the glenoid articular surface to obtain a “bumper” to recreate optimal conditions for concavity-compression mechanism [32]. Sekiya published a technical note describing multiple-pleat plication through a single working portal. He used three suture anchors to shift the middle GHL and the IGHL and repair the detached labrum. Braided sutures were tied with locking sliding knots backed with three half stitches [72]. Patients with MDI and anterior labrum detachment require a standard procedure of labrum fixation with suture anchors.
Cicak et al. [68] published a technical note describing an alternative arthroscopic extra-articular plication technique and emphasizing that it achieves greater capsular reduction than intra-articular plication.
Recent cadaver studies have shown that the percent GHJ volume reduction that can be achieved by capsular plication is 19 % using four 1-cm tucks, 22 % with three 10-mm tucks, and 33 % with four 10-mm pleats [73–75].
Rehabilitation
Similar postoperative rehabilitation programs are applied after open and arthroscopic procedures, but the time until complete recovery of IR may vary with the type of SSC approach used. Immobilization in a shoulder orthosis is required for 3–6 weeks depending on the procedure performed [76, 77]; patients with labral repair using suture anchors should avoid active ER for 4–6 weeks [76]. Recent findings show that placing the arm in 10°–20° of ER and approximately 30° of abduction is associated with a greater and prompter ROM recovery and functional score improvement [78]. The therapist may apply gentle passive and active ROM in 90°–100° of elevation for the first 4–6 weeks. Gentle isometric strengthening activities are initiated in the fourth week to prevent atrophy of the surrounding musculature. Six weeks after surgery, passive and active mobilizations are increased until full motion is achieved by approximately 10–12 weeks. Tissue stretching is not advised because it may result in excessive humeral translation [76]. Active mobilization after 4 weeks can be performed in a water pool. After 60 days, an isotonic RC and scapular stabilizer strengthening program may be initiated to improve dynamic stability and neuromuscular control. At 90 days, all patients return to work and/or to specific sport-related shoulder training, but competitive throwing, shoulder overloading, and overhead sports are not allowed before 6–9 months from surgery [76].
Results
Several surgical approaches have been developed to treat MDI and result in different outcomes. Whatever the treatment, results seem partially to deteriorate with time [2, 16, 53, 79]. Although a variety of open and arthroscopic techniques have been described, the rate of good to excellent early- and mid-term results ranges from 80 to 94 % [5, 16]; however, data stratification shows that the clinical outcomes of MDI patients are less favorable than those of patients with unidirectional shoulder instability. Addressing pathoanatomy is critical to obtaining satisfactory results. Neer first described the inferior capsular shift procedure to reduce capsular redundancy and laxity, reporting high patient satisfaction and shoulder stability on clinical examination, with only one shoulder that began subluxating again within 7 months [1]. Favorable mid-term results (2 years) using Neer’s technique have also been described by Cooper et al. [16], who reported a satisfactory postoperative ROM, 91 % of patients with no residual instability, four with symptomatic MDI, and nine with continuing episodes of apprehension; overall 34/38 patients were satisfied. van Tankeren et al. [80] reported similar satisfactory outcomes at a mean follow-up of 39 months using Rowe’s and Constant’s scores and Dawson’s 12-item questionnaire, with results that were excellent in 14 patients, fair in two, and poor in one.
Fleega and El Shewy [81] reported very good long-term results (7 years) of arthroscopic inferior capsular shift; they described a significant improvement in ASES, Constant-Murley and UCLA scores, complete recovery of shoulder motion, and a 4 % rate of redislocation. Voigt et al. [82] performed arthroscopic anterior-inferior and posterior-inferior capsular plication and RI closure in nine young overhead athletes with persistent, symptomatic MDI and reported excellent to good Rowe and Constant-Murley scores in nine patients (ten shoulders) at 39 months; however, three patients had to reduce their level of sport participation. Baker et al. [83] also described successful return to sports at 33.5-month follow-up in 40 MDI patients treated by arthroscopy, with a significant increase in postoperative ASES and WOSI scores. Other studies have also described arthroscopic capsular shift for GHJ volume reduction as a safe procedure to improve shoulder stability [84–86], but the low rate of return to high-level sport performance in some studies remains a challenge [85]. Some authors showed that RI closure has a prolonged effect on shoulder stability and function by improving not only static but also dynamic restraints [86]. Although the arthroscopic approach is widely recommended for its minimal invasiveness and patient preference, open procedures have been demonstrated to provide good outcomes with an acceptable failure rate [87–89]. Bak et al. [87] evaluated 25 athletes at 54 months and reported excellent to good Rowe and UCLA scores and a return to the previous sport in 16 (76 %); of these, 12 (57 %) patients actually returned to the same performance level. Choi et al. [88], applying ASES criteria, reported that successful treatment of instability in 91 % of anterior repairs and 81 % of posterior repairs with capsular shift in contact sports players, although the results of bilateral MDI were poor. Marquardt et al. [89] described satisfactory Rowe scores and postoperative ROM in 35/38 shoulders and a redislocation rate of 10.5 % at 7.4-year follow-up. Steinbeck and Jerosch [90] obtained a good average Rowe score improvement with a modified capsular shift at 3 years in 20 patients; of these, one suffered from recurrent subluxation and another had a redislocation. As regards the comparison of open vs arthroscopic procedures, a recent systematic review shows that arthroscopic capsular plication yields comparable results to open capsular shift in terms of instability recurrence, return to sports, loss of ER, and overall complications [91]. The results of thermal capsular shrinkage to treat capsular redundancy in MDI are more controversial [92–96]; in fact whereas the failure rate—as assessed by pain, recurrence of instability, return to work, and ASES score—described in non-randomized clinical studies ranges from 31 % at 2 years [96] to 37 % at 3 years [93], a recent multicenter randomized clinical trial [95] showed that there were no statistically or clinically significant differences at 2 years between MDI treated with arthroscopic electrothermal capsulorrhaphy and open inferior capsular shift based on ASES, WOSI, and Constant-Murley scores and active ROM. Although the results described Mohtadi et al. [95] document the value of thermal capsulorrhaphy in MDI, its usefulness in treating capsular redundancy in symptomatic shoulder instability is debated, also in terms of the potential negative effects that thermal energy may produce on capsular receptors and consequently proprioception.
Overview
MDI is a multifactorial condition whose major predisposing factor is capsular laxity, which is variably associated with bone and labral abnormalities and impaired muscular control. MDI patients have poor RC and scapulothoracic muscle coordination and strength; this is consistent with our clinical experience. Electromyography investigations have confirmed the hyperactivity of some muscles combined with a reduced activity of other muscles or muscle groups in many patients. Initial treatment should therefore be non-operative and aimed at restoring muscle balance and strength; surgery, whether arthroscopic or open, should be considered only in patients with poor outcomes. The results of operative treatment with the correct indications are overall good with high rates of patient satisfaction, even though return to sports may not be at pre-injury levels for all professional athletes, especially elite overhead sportsmen and women. Finally, patients with voluntary shoulder dislocation should not undergo surgery; in these subjects, a rehabilitation program correcting abnormal muscle patterns and restoring scapular motion has the potential to achieve a satisfactory quality of life including return to sports, performing arts, and the like.
References
Neer CS II, Foster CR (1980) Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder. A preliminary report. J Bone Joint Surg Am 62:897–908
Altchek DW, Warren RF, Skyhar MJ, Ortiz G (1991) T-plasty modification of the Bankart procedure for multidirectional instability of the anterior and inferior types. J Bone Joint Surg Am 73:105–112
Flatow EL, Miniaci A, Evans PJ, Simonian PT, Warren RF (1998) Instability of the shoulder: complex problems and failed repairs: part II. Failed repairs. Instr Course Lect 47:113–125
Neer CS II (1985) Involuntary inferior and multidirectional instability of the shoulder: etiology, recognition, and treatment. Instr Course Lect 34:232–238
Pollock RG, Owens JM, Flatow EL, Bigliani LU (2000) Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am 82:919–928
Matsen FA III, Thomas SC, Rockwood CA Jr, Wirth MA (2005) Glenohumeral instability. In: Rockwood CA Jr, Matsen FA III (eds) The shoulder, vol 1. Saunders, Philadelphia, pp 611–754
Gerber C, Nyffeler RW (2002) Classification of glenohumeral joint instability. Clin Orthop Relat Res 400:65–76
Cofield RH, Irving JF (1987) Evaluation and classification of shoulder instability. With special reference to examination under anesthesia. Clin Orthop Relat Res 223:32–43
Johnson SM, Robinson CM (2010) Shoulder instability in patients with joint hyperlaxity. J Bone Joint Surg Am 92:1545–1557
Rodeo SA, Suzuki K, Yamauchi M, Bhargava M, Warren RF (1998) Analysis of collagen and elastic fibers in shoulder capsule in patients with shoulder instability. Am J Sports Med 26:634–643
Merolla G, De Santis E, Cools AMJ, Porcellini G (2014) Functional outcomes and quality of life after rehabilitation for voluntary posterior shoulder instability: a prospective blinded cohort study. Eur J Orthop Surg Traumatol June 3 [Epub ahead of print]
Bankart A (1938) The pathology and treatment of recurrent dislocation of the shoulder joint. Br J Surg 26:23
Burkhead WZ, Rockwood CA Jr (1992) Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 74:890–896
Tibone JE, Bradley JP (1993) The treatment of posterior subluxation in athletes. Clin Orthop 291:124–137
Rowe CR, Pierce DS, Clark JG (1973) Voluntary dislocation of the shoulder. A preliminary report on a clinical, electromyographic, and psychiatric study of twenty-six patients. J Bone Joint Surg Am 55:445–460
Cooper RA, Brems JJ (1992) The inferior capsular-shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am 74:1516–1521
Dewing CB, McCormick F, Bell SJ, Solomon DJ, Stanley M, Rooney TB, Provencher MT (2008) An analysis of capsular area in patients with anterior, posterior, and multidirectional shoulder instability. Am J Sports Med 36:515–522
Ahmad CS, Freehill MQ, Blaine TA, Levine WN, Bigliani LU (2003) Anteromedial capsular redundancy and labral deficiency in shoulder instability. Am J Sports Med 31:247–252
Uhthoff HK, Piscopo M (1985) Anterior capsular redundancy of the shoulder: congenital or traumatic? An embryological study. J Bone Joint Surg Br 67:363–366
Oyama S, Myers JB, Wassinger CA, Ricci RD, Lephart SM (2008) Asymmetric resting scapular posture in healthy overhead athletes. J Athl Train 43:565–570
Ludewig PM, Phadke V, Braman JP, Hassett DR, Cieminski CJ, LaPrade RF (2009) Motion of the shoulder complex during multiplanar humeral elevation. J Bone Joint Surg 91:378–389
Freedman L, Munro RR (1966) Abduction of the arm in the scapular plane: scapular and glenohumeral movements: a roentgenographic study. J Bone Joint Surg 48:1503–1510
Itoi E, Motzkin NE, Morrey BF, An KN (1992) Scapular inclination and inferior stability of the shoulder. J Shoulder Elbow Surg 1:131–139
Warner JJ, Deng XH, Warren RF, Torzilli PA (1992) Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 20:675–685
Illyés A, Kiss RM (2006) Kinematic and muscle activity characteristics of multidirectional shoulder joint instability during elevation. Knee Surg Sports Traumatol Arthrosc 14:673–685
Struyf F, Nijs J, Baeyens JP, Mottram S, Meeusen R (2011) Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability. Scand J Med Sci Sports 21:352–358
Morris AD, Kemp GJ, Frostick SP (2004) Shoulder electromyography in multidirectional instability. J Shoulder Elbow Surg 13:24–29
Barden JM, Balyk R, Raso VJ, Moreau M, Bagnall K (2005) Atypical shoulder muscle activation in multidirectional instability. Clin Neurophysiol 116:1846–1857
Augé WK 2nd, Morrison DS (2000) Assessment of the infraspinatus spinal stretch reflex in the normal, athletic, and multidirectionally unstable shoulder. Am J Sports Med 28:206–213
Abboud JA, Soslowsky LJ (2002) Interplay of the static and dynamic restraints in glenohumeral instability. Clin Orthop Relat Res 400:48–57
Lee SB, Kim KJ, O’Driscoll SW, Morrey BF, An KN (2000) Dynamic glenohumeral stability provided by the rotator cuff muscles in the mid-range and end-range of motion. A study in cadavera. J Bone Joint Surg Am 82:849–857
Lippit SB, Vanderhooft JE, Harris SL, Sidles J, Harryman DT, Mattsen F (1993) Glenohumeral stability from concavity compression: a quantitative analysis. J Shoulder Elbow Surg 2:27–35
Halder AM, Kuhl SG, Zobitz ME, Larson D, An KN (2001) Effects of the glenoid labrum and glenohumeral abduction on stability of the shoulder joint through concavity-compression: an in vitro study. J Bone Joint Surg Am 83:1062–1069
Schiffern SC, Rozencwaig R, Antoniou J, Richardson ML, Matsen FA 3rd (2002) Anteroposterior centering of the humeral head on the glenoid in vivo. Am J Sports Med 30:382–387
Barden JM, Balyk R, Raso VJ, Moreau M, Bagnall K (2004) Dynamic upper limb proprioception in multidirectional shoulder instability. Clin Orthop Relat Res 420:181–189
Beard DJ, Dodd CAF, Simpson HARW (2000) Sensorimotor changes after anterior cruciate ligament reconstruction. Clin Orthop 372:205–216
Jerosch J, Prymka M (1996) Proprioception and joint stability. Knee Surg Sports Traumatol Arthrosc 4:171–179
Gaskill TR, Taylor DC, Millett PJ (2011) Management of multidirectional instability of the shoulder. J Am Acad Orthop Surg 19:758–767
Grahame R, Bird HA, Child A (2000) The revised (Brighton 1998) criteria for the diagnosis of benign joint hypermobility syndrome (BJHS). J Rheumatol 27:1777–1779
Rowe CR, Zarins B (1981) Recurrent transient subluxation of the shoulder. J Bone Joint Surg Am 63:863–872
Arendt EA (1988) Multidirectional shoulder instability. Orthopedics 11:113–120
Jerosch J, Castro WH (1990) Shoulder instability in Ehlers–Danlos syndrome: an indication for surgical treatment? Acta Orthop Belg 56:451–453
Jobe FW, Kvitne RS, Giangarra CE (1989) Shoulder pain in the overhand or throwing athlete: the relationship of anterior instability and rotator cuff impingement. Orthop Rev 18:963–975
Silliman JF, Hawkins RJ (1993) Classification and physical diagnosis of instability of the shoulder. Clin Orthop Relat Res 291:7–19
Gerber C, Ganz R (1984) Clinical assessment of instability of the shoulder: with special reference to anterior and posterior drawer tests. J Bone Joint Surg Br 66:551–556
Pollock RG, Bigliani LU (1993) Recurrent posterior shoulder instability: diagnosis and treatment. Clin Orthop Relat Res 291:85–96
Gagey OJ, Gagey N (2001) The hyperbaduction test. J Bone Joint Surg Br 83:69–74
Schaeffeler C, Waldt S, Bauer JS, Kirchhoff C, Haller B, Schröder M, Rummeny EJ, Imhoff AB, Woertler K (2014) MR arthrography including abduction and external rotation images in the assessment of atraumatic multidirectional instability of the shoulder. Eur Radiol 24:1376–1385
Provencher MT, Dewing CB, Bell SJ, McCormick F, Solomon DJ, Rooney TB (2008) Stanley M (2008) An analysis of the rotator interval in patients with anterior, posterior, and multidirectional shoulder instability. Arthroscopy 24:921–929
von Eisenhart-Rothe R, Mayr HO, Hinterwimmer S, Graichen H (2010) Simultaneous 3D assessment of glenohumeral shape, humeral head centering, and scapular positioning in atraumatic shoulder instability: a magnetic resonance-based in vivo analysis. Am J Sports Med 38:375–382
Matsen FA, Thomas SC, Rockwood CA (1990) Glenohumeral instability. In: Rockwood CA, Matsen FA (eds) The shoulder, vol 1. Saunders, Philadelphia, pp 526–569
Guerrero P, Busconi B, Deangelis N, Powers G (2009) Congenital instability of the shoulder joint: assessment and treatment options. J Orthop Sports Phys Ther 39:124–134
Mallon WJ, Speer KP (1995) Multidirectional instability: current concepts. J Shoulder Elbow Surg 4:54–64
Magarey ME, Jones MA (2003) Dynamic evaluation and early management of altered motor control around the shoulder complex. Man Ther 8:195–206
Rowe CR (1956) Prognosis in dislocations of the shoulder. J Bone Joint Surg Am 38:957–977
Misamore GW, Sallay PI, Didelot W (2005) A longitudinal study of patients with multidirectional instability of the shoulder with seven- to ten-year follow-up. J Shoulder Elbow Surg 14:466–470
Darlow B (2006) Neuromuscular retraining for multidirectional instability of the shoulder—a case study. NZ J Physioth 34:60–65
Ide J, Maeda S, Yamaga M, Morisawa K, Takagi K (2003) Shoulder-strengthening exercise with an orthosis for multidirectional shoulder instability: quantitative evaluation of rotational shoulder strength before and after the exercise program. J Shoulder Elbow Surg 12:342–345
Kiss J, Damrel D, Mackie A, Neumann L, Wallace WA (2001) Non-operative treatment of multidirectional shoulder instability. Int Orthop 24:354–357
Nyiri P, Illyés A, Kiss R, Kiss J (2010) Intermediate biomechanical analysis of the effect of physiotherapy only compared with capsular shift and physiotherapy in multidirectional shoulder instability. J Shoulder Elbow Surg 19:802–813
Rowe CR, Patel D, Slouthmayd WW (1978) The Bankart procedure: a long-term end-result study. J Bone Joint Surg Am 60A:1–16
Scheibel M, Habermeyer P (2008) Subscapularis dysfunction following anterior surgical approach to the shoulder. J Shoulder Elbow Surg 17:671–683
Jobe FW, Giangarra CE, Kvitne RS, Glousman RE (1991) Anterior capsulolabral reconstruction of the shoulder in overhead sports. Am J Sports Med 19:428–434
Field LD, Warren RF, O’Brien SJ, Altchek DW, Wickiewicz TL (1995) Isolated closure of rotator interval defects for shoulder instability. Am J Sports Med 23:557–563
Snyder SJ (2003) Shoulder arthroscopy. Lippincott Williams and Wilkins, New York, pp 22–28
Matthews LS, Zarins B, Michael RH, Helfet DL (1985) Anterior portal selection for shoulder arthroscopy. Arthroscopy 1:33–39
Wolf EM (1989) Anterior portals in shoulder arthroscopy. Arthroscopy 5:201–208
Cicak N, Klobucar H, Bicanic G, Trsek D (2005) Arthroscopic extracapsular plication to treat multidirectional instability of the shoulder. Arthroscopy 21:1278
Wiley WB, Goradia VK, Pearson SE (2005) Arthroscopic capsular plication-shift. Arthroscopy 21:119–121
McIntyre LF, Caspari RB, Savoie FH III (1997) The arthroscopic treatment of multidirectional shoulder instability: two-year results of a multiple suture technique. Arthroscopy 13:418–425
Gartsman GM, Roddey TS, Hammerman SM (2001) Arthroscopic treatment of bidirectional glenohumeral instability: two- to five-year follow-up. J Shoulder Elbow Surg 10:28–36
Sekiya JK (2005) Arthroscopic labral repair and capsular shift of the glenohumeral joint: technical pearls for a multiple pleated plication through a single working portal. Arthroscopy 21:766
Karas SG, Creighton RA, DeMorat GJ (2004) Glenohumeral volume reduction in arthroscopic shoulder reconstruction: a cadaveric analysis of suture plication and thermal capsulorrhaphy. Arthroscopy 20:179–184
Cohen SB, Wiley W, Goradia VK, Pearson S, Miller MD (2005) Anterior capsulorrhaphy: an in vitro comparison of volume reduction—arthroscopic plication versus open capsular shift. Arthroscopy 21:659–664
Flanigan DC, Forsythe T, Orwin J, Kaplan L (2006) Volume analysis of arthroscopic capsular shift. Arthroscopy 22:528–533
Wilk KE, Macrina LC (2013) Nonoperative and postoperative rehabilitation for glenohumeral instability. Clin Sports Med 32:865–914
Arciero RA, Wheeler JH, Ryan JB, McBride JT (1994) Arthroscopic Bankart repair versus nonoperative treatment for acute, initial anterior shoulder dislocations. Am J Sports Med 22:589–594
Yin B, Levy D, Meadows M, Moen T, Gorroochurn P, Cadet ER, Levine WN, Ahmad CS (2014) How does external rotation bracing influence motion and functional scores after arthroscopic shoulder stabilization? Clin Orthop Relat Res 472:2389–2396
Bigliani LU, Pollock RG, McIlveen SJ, Endrizzi DP, Flatow EL (1995) Shift of the posteroinferior aspect of the capsule for recurrent posterior glenohumeral instability. J Bone Joint Surg Am 77:1011–1020
van Tankeren E, de Waal Malefijt MC, van Loon CJ (2002) Open capsular shift for multi directional shoulder instability. Arch Orthop Trauma Surg 122:447–450
Fleega BA, El Shewy MT (2012) Arthroscopic inferior capsular shift: long-term follow-up. Am J Sports Med 40:1126–1132
Voigt C, Schulz AP, Lill H (2009) Arthroscopic treatment of multidirectional glenohumeral instability in young overhead athletes. Open Orthop J 24(3):107–114
Baker CL 3rd, Mascarenhas R, Kline AJ, Chhabra A, Pombo MW, Bradley JP (2009) Arthroscopic treatment of multidirectional shoulder instability in athletes: a retrospective analysis of 2- to 5-year clinical outcomes. Am J Sports Med 37:1712–1720
Lubiatowski P, Ogrodowicz P, Wojtaszek M, Breborowicz M, Długosz J, Romanowski L (2012) Arthroscopic capsular shift technique and volume reduction. Eur J Orthop Surg Traumatol 22:437–441
Ma HL, Huang HK, Chiang ER, Wang ST, Hung SC, Liu CL (2012) Arthroscopic pancapsular plication for multidirectional shoulder instability in overhead athletes. Orthopedics 35:e497–e502
Moon YL, Singh H, Yang H, Chul LK (2011) Arthroscopic rotator interval closure by purse string suture for symptomatic inferior shoulder instability. Orthopedics 34(4):11
Bak K, Spring BJ, Henderson JP (2000) Inferior capsular shift procedure in athletes with multidirectional instability based on isolated capsular and ligamentous redundancy. Am J Sports Med 28:466–471
Choi CH, Ogilvie-Harris DJ (2002) Inferior capsular shift operation for multidirectional instability of the shoulder in players of contact sports. Br J Sports Med 36:290–294
Marquardt B, Pötzl W, Witt KA, Steinbeck J (2005) A modified capsular shift for atraumatic anterior-inferior shoulder instability. Am J Sports Med 33:1011–1015
Steinbeck J, Jerosch J (1997) Surgery for atraumatic anterior-inferior shoulder instability. A modified capsular shift evaluated in 20 patients followed for 3 years. Acta Orthop Scand 68:447–450
Jacobson ME, Riggenbach M, Wooldridge AN, Bishop JY (2012) Open capsular shift and arthroscopic capsular plication for treatment of multidirectional instability. Arthroscopy 28:1010–1017
Oron A, Reshef N, Beer Y, Brosh T, Agar G (2012) The influence of radiofrequency ablation patterns on length, histological and mechanical properties of tendons. Muscles Ligaments Tendons J 10(2):85–90
D’Alessandro DF, Bradley JP, Fleischli JE, Connor PM (2004) Prospective evaluation of thermal capsulorrhaphy for shoulder instability: indications and results, two- to five-year follow-up. Am J Sports Med 32:21–33
Favorito PJ, Langenderfer MA, Colosimo AJ, Heidt RS Jr, Carlonas RL (2002) Arthroscopic laser-assisted capsular shift in the treatment of patients with multidirectional shoulder instability. Am J Sports Med 30:322–328
Mohtadi NG, Kirkley A, Hollinshead RM, McCormack R, MacDonald PB, Chan DS, Sasyniuk TM, Fick GH, Paolucci EO (2014) Electrothermal arthroscopic capsulorrhaphy: old technology, new evidence. A multicenter randomized clinical trial. J Shoulder Elbow Surg 23:1171–1180
Toth AP, Warren RF, Petrigliano FA, Doward DA, Cordasco FA, Altchek DW, O’Brien SJ (2011) Thermal shrinkage for shoulder instability. HSS J 7:108–114
Acknowledgments
The authors are grateful to Word Designs (www.silviamodena.com) for the language revision.
Conflict of interest
None of the authors have any conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Merolla, G., Cerciello, S., Chillemi, C. et al. Multidirectional instability of the shoulder: biomechanics, clinical presentation, and treatment strategies. Eur J Orthop Surg Traumatol 25, 975–985 (2015). https://doi.org/10.1007/s00590-015-1606-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-015-1606-5