
Abstract
In contrast to closed Achilles tendon ruptures, open injuries are rarely reported in the literature. This paper provides information about open Achilles tendon wounds that are eventually seen in the Middle East. The reporting unit, Hamad Medical Corporation, is one of the biggest trauma centers in the Gulf area and the major health provider in Qatar. This is a retrospective study including patients admitted and operated for open Achilles tendon injuries between January 2011 and December 2013. Two hundred and five cases of open Achilles tendon lacerations were operated in Hamad General Hospital in this period. Forty-eight cases showed partial injuries, and the remaining are complete tendons cut. In the same period, fifty-one closed ruptured Achilles tendons were operated in the same trauma unit. In the majority of cases, the open injury resulted from a slip in the floor-leveled traditional toilette seats. Local damage to the toilette seats resulted in sharp edges causing the laceration of the heel if the patient was slipping over the wet floor. This occurrence is the cause in the vast majority of the cases. Wounds were located 1–5 cm proximal to tendon insertion. Standard treatment principles were applied. This included thorough irrigation in the emergency room, intravenous antibiotics, surgical debridement and primary repair within 24 h. Patients were kept in the hospital 1–7 days for intravenous antibiotics and possible dressing changes. Postoperatively below knee slabs were applied in the majority of patients and were kept for about 4 weeks followed by gradual weight bearing and range of motion exercises. Outpatients follow up in 1–2 weeks. Further follow-up visits at around 2-, 4-, 8- and 12-week intervals until complete wound healing and satisfactory rehabilitation outcome. Sixteen cases needed a second procedure. A high incidence of Achilles tendon open injuries is reported. This seems to be related to partially damaged floor-level toilettes in the typical Middle-East lavatory. The surgical treatment resulted in excellent outcome in the vast majority of the cases. Low incidence of complications resulted despite dramatic injury pattern.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Most literature about Achilles tendon injuries describe closed ruptures rather than open lacerations. This is probably because the vast majority of Achilles tendon injuries in the world are closed ruptures. Literature searches for open Achilles tendon laceration will result therefore in large amount of publications about closed ruptures and only few reports about open injuries [1–3]. In contrast to that a high incidence of the open Achilles tendon injury is observed in Qatar. Therefore, we wanted with this study to focus more on this clinical entity and to publish it.
In the majority of cases, the injury occurred due to a slippage in floor-leveled toilette. This is similar to the description reported by Chatterjee [1], Dar et al. [2]. However, their reported incidence is much lower, and their interpretation of the direct cause of laceration was unclear to us.
The primary aim of our study is to develop public awareness about this injury to hopefully contribute to reduce it. We hope also to provide medical literature with our unusual experience.
Methods
This is a retrospective study of patients admitted and operated for open Achilles tendon injuries in Hamad General Hospital (HGH) in the time from January 1, 2011 to December 31, 2013. Patient’s data with this diagnosis were retrieved and analyzed. Patient’s demographics, the management of these injuries and reported major complications will be presented. Human and patients rights and were observed in this study.
Results
Two hundred and five cases (198 males and 7 females) of open Achilles tendon lacerations were operated in HGH in the index period; forty-eight of them were partial injuries. Average age was 34 years (18–52). One hundred and seventy-seven were laborer living in camps. In the same period, only 51 patients with closed ruptured Achilles tendons were operated in the same hospital (Figs. 1, 2, 3).

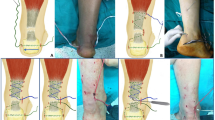
Open wound of an Achilles tendon laceration in a bathroom injury

Intraoperative suture repair of open cut Achilles tendon

Healed Achilles tendon laceration wound
In the majority of cases (n = 183), the open injury resulted from a slip in the floor-leveled traditional toilette. These are preferred because of lack of skin contact and ease of cleaning. The offended toilette seats, however, were found upon patients questioning to be partially broken with a sharp edge causing the laceration.
About 2–5 cm deep, transverse or mildly oblique laceration wounds were found. Wounds were located 1–5 cm proximal to tendon insertion.
The wounds were irrigated in the emergency room with several liters saline. Tetanus prophylaxis was given, and intravenous antibiotics were initiated. First-generation cephalosporin ± gentamycin ± metronidazole was selected. Repeat irrigation in the operating theatre, wound extension as needed, debridement and primary tendon and wound repair were done as early as possible within 24 h. Two hundred and two procedures were done prone, and three were done in lateral position. One hundred and thirty-six cases were done under spinal, 23 under regional and the remaining under general anesthesia. Absorbable and non-absorbable stitches were used for the tendon upon surgeon decision. Paratenon and subcutaneous tissues sutured with absorbable poly filaments. Patients were kept in the hospital 1–7 days for intravenous antibiotics and possible dressing changes. Postoperatively below knee slabs were applied in the majority of patients and were kept for about 4 weeks followed by gradual weight bearing and range of motion exercises. Outpatients follow up in 1–2 weeks. Further follow-up visits at around 4-, 4-, 8- and 12 week intervals until complete wound healing and satisfactory rehabilitation outcome.
Seven patients needed second surgery for wound infection, one for tendon rupture after primary repair and eight for stitch sinuses. One patient needed local skin release incision and one patient needed wound flab coverage. Hypertrophy of the involved tendon was reported in three cases. Mild reduction in ankle dorsal flexion was found in 13 patients and was improved on physiotherapy. Mild skin tethering was found in 18 cases.
Discussion
Only few reports about open injuries of the Achilles tendon could be found in the literature. It is in fact a large subcutaneous structure, which should make it exposed to injury. However, its posterior location makes it less exposed to fall from the hands of sharp objects. Its vertical orientation makes it also less likely to be affected by falling objects. However, there were scattered literatures about open Achilles tendon injuries. Zhu et al. [3] reported a large series of 289 children with bicycle or motorcycle spoke heel injuries. Many of them were not cutting the Achilles tendon. One hundred and seventy-nine were males and 110 females aged 2–12 years old (average 3.9 years old). There are millions of adults and children cyclists in the Western world; however, we did not come across a publication about Achilles tendon injuries in cyclists. This is may be underreported, or the incidence of spoke heel injuries in the Western world may be lower. Similarly, few reports were found about open Achilles tendon injuries as a result of slippage. Chatterjee et al. [1] reported eighteen patients presenting with acute open injuries of the Achilles tendon from July 1995 to October 2005. Of these, 15 were between March 2003 and October 2005. All the patients gave a history of slipping of the foot into the hole of a lavatory pan sustaining injury both during entry and extraction of the foot. Dar et al. [2] presented a case series of twelve patients with toilette seat injury to the Achilles tendon. These examples are only exceptions to the majority of world literature about Achilles tendon injuries, which describe closed ruptures rather than open lacerations. This is probably because the vast majority of Achilles tendon injuries in the world are closed ruptures. In contrast to that a high incidence of the open Achilles tendon injury is observed in Qatar. Therefore, we wanted with this study to focus more on this clinical entity and to present it. We hope with this to provide medical literature with our unusual experience.
The mechanism of injury itself is mysterious. In the majority of cases, the injury occurred due to a slippage in floor-leveled toilette. Floor-level toilette seats are popular in shared housings like labor camps because skin contact to the seat is avoided. In addition to that they are simpler to clean. The majority of the seats available in the common market is designed to be blunt with no sharp edges and would be unlikely to cause such a deep sharp laceration. This adds more to the mystery how does it come to the open laceration of the skin and the underlying strong Achilles tendon. It is probable that the jerky reflex withdrawal of the foot is a contributor to the injury, but it is unlikely to be the single factor. The mechanism of injury is similar to the description reported by Chatterjee [1], Dar et al. [2]; however, their interpretation of the direct cause of laceration was unclear to us. In our series upon patients questioning, many of them reported certain damage to exist in the offended seats. The incidence in Qatar is also much higher than reported before. This is probably for the huge and rapid labor influx in the country with large number of camps, which were built to be practical and to the need.
The primary aim of our study is to develop a public awareness about this injury to hopefully contribute to reduce it. This might be achievable with reducing slipperiness of the footsteps. Seats should be also rapidly replaced when local damage is discovered.
Conclusion
A high incidence of Achilles tendon open injuries is reported. It is related to partially damaged floor-level toilette. Relative low incidence of major complications resulted despite dramatic injury pattern.
References
Chatterjee SS, Sarkar A, Misra A (2006) Management of acute open tendo-achilles injuries in Indian lavatory pans. Indian J Plast Surg 39:29–30
Dar TA, Sultan A, Dhar SA, Ali MF, Wani MI, Wani SA (2011) Toilet seat injury of the Achilles tendon a series of twelve cases. Foot Ankle Surg 17(4):284–286
Zhu Y, Xu Y, Li J, Yag J, Ouyang Y, He X, Chen H, Fan X (2009) Treatment of spoke heel injuries in children. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 23(10):1180–1182
Conflict of interest
No conflict of interests related to this publication by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Said, M.N., Al Ateeq Al Dosari, M., Al Subaii, N. et al. Open Achilles tendon lacerations. Eur J Orthop Surg Traumatol 25, 591–593 (2015). https://doi.org/10.1007/s00590-014-1554-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-014-1554-5