
Abstract
Purpose
The aim of this study; evaluate lumbar lordosis (LL) in symptomatic individuals with six different techniques and to examine the techniques comparatively. Thus, to provide an overview of lumbal lordosis and techniques.
Methods
Cobb L1-L5, Cobb L1-S1, Posterior Tangent, tangential radiologic assessment of lumbar lordosis (TRALL), vertebral centroid measurement of lumbar lordosis (CLL) and Risser Ferguson measurement techniques were used to assess LL from radiographs of 175 symptomatic adults. Correlations between techniques and relationship between the measurements obtained, gender and age were analyzed. Also ınterclass correlation (ICC) analyzed. Bland–Altman plots were performed to compare the techniques with Cobb.
Results
ICC for all methods were greater than 0.96. For each method, no difference in LL was observed with respect to gender or age (p > 0.05). High positive correlation was observed between the Risser Ferguson, Posterior Tangent, Cobb L1-L5, Cobb L1-S1 and CLL techniques (p < 0.001), and moderate positive correlation between TRALL and all other techniques (p < 0.001).
Conclusion
In this study, it was found that the mean lumbar lordosis values of symptomatic participants were lower than most of the other asymptomatic studies in the literature and there was no significant difference in lumbar lordosis values in terms of gender and age in symptomatic individuals. Based on statistical findings, Risser Ferguson can be used to assess LL. These results and the data obtained as a result of the comparative examination of techniques according to age groups and gender will benefit clinicians and those working in the field by providing a better understanding LL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The vertebral column has a number of important functions: It supports the trunk, permits movement to the body, carries and transfers load from one region to another, and helps protect internal organs and the spinal cord [1, 2]. It has a number of curvatures, one of which is associated with the lumbar region (lumbar lordosis) [3]. Lumbar lordosis was first described by Galen, with its original definition still being used today: It begins in the late fetal period, then rapidly develops, particularly as the adult pattern of walking is achieved [4]. An optimal lumbar lordosis is essential for the health of the vertebral column and individual, with studies showing a relationship between lumbar lordosis and functional disorders and other conditions associated with the vertebral column: [5,6,7] the extent of lumbar lordosis has been used in the diagnosis of some pathologies [8]. In abnormal lumbar lordosis, the risk of disc and vertebral degeneration, lumbar disc herniation and spondylosis increases [9]. Lumbar lordosis is also an important factor for gait kinematics, having been shown to develop more quickly in monkeys accustomed to walking than in those that did not walk [4, 10]. The lumbar region is the most susceptible part of the vertebral column to degeneration, as it is exposed to greater stresses than other regions, particularly the lumbosacral junction: This is why pathologies originating from the lumbar region are commonly observed [11].
Previous researches on the sagittal balance of the spine have shown both the functional and clinical significance of the degree of lumbar lordosis [12,13,14]. Lumbar lordosis should be taken into account in surgical approaches and therapeutic exercise applications involving the lumbar region, being used by clinicians as an important factor in the sagittal alignment of the vertebral column. Considering that pathologies caused by lumbar lordosis due to inactivity, obesity and occupational factors have increased in recent years, the anatomy of the lumbar region, especially lumbar lordosis, requires further investigation to improve the understanding of the region. In the current study, the five most common measurement techniques reported in the literature and the Risser Ferguson method, which evaluates coronal spinal curvatures, were used to determine and assess lumbar lordosis [15]. Due to its effect on spinal function and mechanics, correct evaluation of the degree of lumbar lordosis is very important for clinicians. Lumbar lordosis was analyzed in individuals with different professions, ages and spinal pathologies. [12, 16,17,18,19]. In this paper, symptomatic individuals with lower back complaints were assessed. The aim of this study; assess the lumbar lordosis values of 175 symptomatic individuals and to examine six techniques comparatively.
Material and methods
Permission to conduct the study was obtained from Çukurova University Non-Interventional Ethical Research Council and Niğde Ömer Halisdemir Training and Research Hospital. Lateral radiographs of 175 (100 female, 75 male) symptomatic individuals with pathology of the lumbar region were examined, from which measurements of lumbar lordosis using six different techniques were obtained: The radiographs were taken during 2020–2021.
Inclusion criteria for the study were:
-
(1)
Individuals had to be between the ages of 18 and 65
-
(2)
Radiographs had to have been taken with the individual standing
-
(3)
Radiographs had to show clearly the sacral and lumbar vertebrae
-
(4)
No surgical operation in the lumbar region
Cobb L1-S1, Cobb L1-L5, Vertebral Centroid Measurement of Lumbar Lordosis (CLL), Tangential Radiologic Assessment of Lumbar Lordosis (TRALL), Risser Ferguson and Posterior Tangent angles were determined from each radiograph.
The ages of the individuals included in the study were grouped as follows: young adults (18–30 years); middle aged adults (31–45 years); and older adults (46–65 years). Each radiograph was analyzed using the KarMED PACS VIEWER (Picture Archiving and Communications System/Turkey) program, which allowed reliable data to be obtained.
-
(1)
Cobb L1-S1 method
The angle between a line drawn parallel to the upper edge of L1 and a line drawn parallel to the upper edge of S1 was measured (angle ‘y’ in Fig. 1).
-
(2)
Risser Ferguson method

Determination of: Cobb L1-S1 angle (y). and the Risser Ferguson angle (x)
The angle between a line drawn from the center of L1 to the center of L3 and a line drawn from the center of L5 to the center of L3 was measured (angle ‘x’ in Fig. 1).
-
(3)
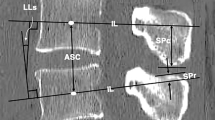
Vertebral centroid measurement of lumbar lordosis (CLL) method
The angle between the line drawn from the center of L1 to the center of L2 and the line drawn from the center of L5 to the center of L4 was measured (angle ‘z’ in Fig. 2).
-
(4)
Cobb L1-L5 method

Determination of: Cobb L1-L5 angle (t); Posterior Tangent angle (p); CLL angle (z)
The angle between a line drawn parallel to the upper edge of L1 and a line drawn parallel to the lower edge of L5 was measured (angle ‘t’ in Fig. 2).
-
(5)
Posterior tangent method
The angle between a line drawn parallel to the posterior edge of L1 and a line drawn parallel to the posterior edge of L5 was measured (angle ‘p’ in Fig. 2).
-
(6)
Tangential Radiologic Assessment of Lumbar Lordosis (TRALL) method
A line is drawn between the posterior superior corners of L1 and S2. The projection of the posterior longitudinal ligament (PLL) was determined, then a perpendicular line was drawn from the PLL to the furthest point on the straight line. Straight lines were then drawn to this intersection point from the superior corner of S2 and the superior corner of L1: The angle between the lines was measured (angle ‘r’ in Fig. 3).

Determination of TRALL angle (r)
Statistical analysis
The data obtained were analyzed using the Statistical Package for Social Sciences for Windows 21 (SPSS 21 inc) program. In the analysis, the mean, standard deviation (SD), minimum (min), and maximum (max) were obtained. Normality analysis was performed to check that the data were normally distributed. Data having a normal distribution were analyzed using parametric tests, while data not normally distributed were analyzed using nonparametric tests. The results were evaluated at the level of significance p < 0.05, with a confidence interval of 95%.
Frequency measurements were calculated for categorical variables. The minimum, maximum, mean and standard deviation were determined for each measurement. The relationship between measurements obtained with each of the six techniques was analyzed using the Pearson correlation test. The t test for the differences between measurements were used according to the 2-group variables: Differences between 3 or more groups were analyzed using ANOVA. If a difference was observed in the ANOVA test, the pairwise difference was analyzed with the Tukey test. The relationship between categorical variables was analyzed using the Chi-square test. Simple linear regression analyzes were conducted to determine relationships between measurement techniques. Interclass correlation (ICC) analyses was assessed using Cronbach’s Alpha. Bland–Altman plot was performed to assess the harmony of the techniques with the Cobb techniques (Figs. 4 and 5). For each analysis 20 images were randomly selected from the study dataset, with each of the different measurement methods undertaken independently by three examiners.

Bland–Altman plot of the Cobb L1-L5 with other techniques

Bland–Altman plot of the Cobb L1-S1 methods with other techniques
Results
The ICC showed acceptable reliability for each of the techniques used in the study. The mean measurements for each observer and the difference between the means were determined. The interclass correlation coefficient for each measurement method was greater than 0.96 (Table 1).
The mean, maximum and minimum values and standard deviation for each measurement method are shown in Table 2, together with the results of the normality tests conducted on each data set. It can be seen that there is a wide variation in the value of lumbar lordosis obtained for each technique: Not surprisingly Cobb L1-S1 has the greatest value (73.5°) due to the inclusion of S1 in the measurement, and Risser Ferguson has the smallest value (38.5°). The correlations between the various techniques are shown in Table 2: A significance level of p < 0.05 was set as being an acceptable correlation between techniques. As can be seen in Table 3, techniques other than TRALL have strong positive correlation with each other.
When the mean lumbar lordosis for each measurement method was analyzed with respect to age, no differences was observed between age groups for any of the methods (p > 0.05): The values obtained using different methods showed wide variation (Table 4).
When analyzed with respect to gender no difference (p < 0.05) was observed between males and females (Table 5): Again the values varied between techniques.
Discussion
The importance of lumbar lordosis in a clinical setting is becoming increasingly important, with the majority of individual’s concerns being related to a sagittal lumbar alignment disorder. It is clear that the importance of lumbar lordosis needs be better understood: to do this its assessment needs to be re-evaluated. To obtain better and more successful results in ergonomics and physical therapy, as well as in the outcome of surgical approaches, the extent and nature of lumbar lordosis must be taken into account [5, 16, 18,19,20]. Although many studies have been conducted concerning the sagittal alignment of the lumbar region, there appears to be little or no consensus on the optimal value of lumbar lordosis or the most appropriate technique to use in its evaluation. The Cobb methods are probably the most commonly used, due mainly to their ease of application and universal acceptance; However many different approaches have been developed and presented in the literature to overcome different limitations. Posterior Tangent, CLL, TRALL are the most well-known of these techniques [15, 21].
An accurate radiological evaluation is important to be able to detect primary and secondary pathologies originating from lumbar lordosis [22]. It is clear that the most advantageous technique, in terms of ease of use and accuracy, should be evaluated to enable an accurate radiological evaluation to be made. Furthermore, deficiencies in the literature need to be addressed to better understand lumbar lordosis and provide appropriate treatment. Lumbar lordosis can be influenced by many factors, including gender, age and profession [23]. It has been evaluated in different ages, professions, genders and pathologies [14, 16, 17, 24]. In the current study, lumbar lordosis in symptomatic individuals due to low back complaints was investigated using five recognized methods, as well as the Risser Ferguson method, for determining its value. Such a comprehensive data set from 175 individuals appears not to have been previously undertaken: It is a unique data set. Considering that 6 different techniques were evaluated on 175 individuals, it can be stated that this study made a rich and valuable contribution to the literature by providing an overview of the techniques used in the evaluation of lumbar lordosis.
Moring lang et al. stated that among the factors of age, weight and gender, gender was the factor that most affected lumbar lordosis in healthy people [24]. Gelb et al. reported a difference in the mean lumbar lordosis values of men and women [25]. Legaye et al. and Korovessis et al. reported findings that there were differences in the mean lumbar lordosis values of women and men [26,27,28]. In these researches, it was suggested that gender was a factor affecting lumbar lordosis. Esen et al. reported that lumbal lordosis values did not differ between age groups but were related with body mass index and gender [30]. Vialle et al. found a mean lumbar lordosis value of 46.2° in women and 41.4° in men [31]. In this study, no significant relationship between gender or age group and the measurement of lumbar lordosis was observed (p > 0.05) (Tables 4 and 5). Previous studies have shown that increasing age is one of the most common factors in the development of low back pain [32]; however, the number of individuals attending clinics for low back pain has increased. No difference in lumbar lordosis was observed in the current study, irrespective of the method of measurement. In the present study, the degree of lumbar lordosis was measured in symptomatic individuals. Based on our results, we can state that the measurement results in radiologic images of symptomatic individuals do not vary depending on gender and age (Tables 4 and 5).
The values of lumbar lordosis determined using different methods by various groups are given in Table 6: as can be seen the observations in the current study were similar to those previously reported symptomatic researches.
The most widely used method for measuring lumbar lordosis is the Cobb method and is accepted as the golden standard. Despite being an old approach, it is highly popular and still widely used. [40]. It is favored by practitioners due to its simple, straightforward and practical application. If a new technique is introduced, it is compared with the Cobb method. Some examples from other articles in the literature are presented in Table 6. In the present study, the mean Cobb L1-L5 angle was 38.1° and the mean Cobb L1-S1 angle was 51.1° in symptomatic adults. The angle measurements in our results are generally lower than those in other studies in the literature with healthy individuals and similar to those in studies with symptomatic individuals.
Posterior tangent and Cobb methods are most widely used by clinicians to measure lordosis [15]. Janik et al. compared the Posterior Tangent method and Cobb method to assess the degree of cervical lordosis. They reported that the Posterior Tangent method was more reliable in terms of low measurement error and high accuracy [41]. Since lumbar lordosis and cervical lordosis are similar curvatures, there is some commonality in their assessment. Russel et al. compared the Cobb L1-L5 method with the Posterior Tangent method in their study. In a study of 16 subjects, they found the mean Posterior Tangent angle 40.2° and the mean Cobb L1-L5 angle 49.6°. They reported that these two techniques showed a high degree of correlation. However, they noted that the measurement of the posterior tangent angle took more time [17]. Harrison et al., in a study conducted with 30 individuals, they determined the mean Cobb L1-L5 angle as 40.3° and the mean Posterior Tangent angle as 34.5° [27]. Hong et al. measured 90 individuals with scoliosis and found the mean Cobb L1-L5 angle 34.5° and the mean posterior tangent angle 36.5° [18]. They considered the Cobb L1-L5 and the Posterior Tangent as reliable methods [18]. In our study, the mean Cobb L1-L5 angle was found 38.09° and the mean Posterior Tangent L1-L5 angle was found 33.23°, as previously mentioned in text (Table 2). The results found by other researchers and the results found in our study are statistically close. At the same time, in the correlation analysis performed in our study, a very strong positive correlation was found between these two measurement techniques (r = 0.834) (Table 3). When Figs. 4 and 5 are analyzed, the compatibility of the posterior tangent method with Cobb techniques can be observed.
Chen et al. compared the Cobb L1-L5 and Cobb L1-S1 with the Central Measurement Method angle of Lumbar Lordosis (CLL). They reported that the mean Cobb L1-L5 angle was 35.8°, the mean Cobb L1-S1 angle was 50.4° and the mean CLL angle was 35.3°. They also reported that Cobb L1-L5 and Cobb L1-S1 methods showed statistical significance and a strong positive correlation with the CLL technique in the statistical analysis (p < 0.05). In addition to these findings, Chen et al. stated that changes in Cobb angles due to osteoporosis and vertebral degeneration would cause inter-observer differences and that the CLL angle referring to the center of the vertebra was more reliable in measuring lumbar lordosis [33]. In another study, Chen et al. used the CLL angle and Cobb angle in scoliosis measurements and reported that the CLL technique was more reliable because it was not affected by the vertebral end architecture [42]. In our study, the mean Cobb L1-L5 angle was 38.09°, the mean Cobb L1-S1 angle was 51.1° and the mean CLL angle was 24.99°. Our results are statistically similar to the study by Chen et al. The CLL method showed a high positive correlation with all techniques except the TRALL method (Table 3). In the CLL method, measurements are made from the center of the vertebra. Measurements are not affected by vertebral endplate architecture. The reference points are easy to determine. The harmony of the CLL method with Cobb techniques is shown in the Bland–Altman plots in Figs. 4 and 5.
TRALL technique developed by Chernutka as an alternative to Cobb [35]. In a study performed in 200 symptomatic individuals, Francis Osita Okpala found the mean Cobb L1-S1 angle 49.9° and the mean TRALL angle 47.3°. He detected a low correlation between the two techniques [34]. Chernutka et al. found the mean Cobb L1-S1 angle 51.9° and the mean TRALL angle 38.8°. Chernutka et al. also reported that measurements with Cobb techniques showed wide range of mean lumbar lordosis values with large standard deviations. They moreover stated that the TRALL technique is more advantageous in locating vertebral end plates. So that according to Chernutka the TRALL is more reliable and advantageous [35]. Harrison et al. did not recommend the TRALL angle because it did not have segmental analysis [27]. Hong et al. calculated the mean Cobb L1-S1 angle as 39.79° and the mean TRALL angle as 32.46° in 90 individuals and reported that the TRALL technique was more reliable than other methods involving the L5-S1 segment [18]. In our study, the mean TRALL angle was 37.24° and the mean Cobb L1-S1 angle was 51.01°. The Cobb L1-S1 angle values found in our study are very close to the values found by Chernutka et al. and Hong et al. The numbers we calculated for the TRALL angles are in agreement with the data of Chernutka, the creator of the technique. According to our findings, there is a strong positive correlation between TRALL angle and Cobb L1-S1, Cobb L1-L5 angle (r = 0.618, r = 0.612) and a moderate positive correlation between TRALL angle and CLL and Posterior Tangent angle (r = 0.501, r = 0.541). TRALL angle has shown high and moderate correlation with other methods commonly used in lordosis measurement, but the correlation values are low compared to the correlation values of other techniques with each other (Table 3). The agreement of the TRALL method with Cobb techniques is shown in the Bland–Altman plots in Figs. 4 and 5. This method uses more reference points and lines than other techniques. This increases the measurement time.
The Cobb technique is the golden standard, but the fact that many other techniques have been introduced to the literature to evaluate spinal curvatures is an evidence that the search for the perfect technique is still ongoing and alternatives to the Cobb method are being investigated. In this direction, many techniques have been developed and adapted. The Risser Ferguson method is essentially a technique used for the assessment of scoliosis in the coronal plane: [43] it has not been used in sagittal plane evaluation of the vertebral column. In the current study, the Risser Ferguson method was modified for the evaluation of lumbar lordosis: The current study appears to be the first to use it in the measurement of lumbar lordosis. The Risser Ferguson method is similar to the CLL method, differing in the vertebral centers used: It showed a very high ICC (0.98) (Table 1). Descriptive statistics were shown in Table 2 for Risser Ferguson angles. It showed very high positive correlations with the CLL and the Posterior Tangent methods, and a high positive correlations with the Cobb L1-L5 and Cobb L1-S1 methods (Table 3). According to Bland–Altman plots (Figs. 4 and 5) and correlation analysis, it is recommended Risser Ferguson technique can be used in the assessment and evaluation of lumbar lordosis. Further researches are definitely required to reveal the benefits and drawbacks of a new technique.
In conclusion, the current study is one of the most comprehensive in terms of the number of individuals examined and the number of techniques evaluated. From this point of view, it provides a wealth of data source in terms of correlation relationships between techniques and assessment of lumbar lordosis degrees according to gender and age. The adaption of the Risser Ferguson method, used for the evaluation of scoliosis, was used for the first time in this study for the evaluation of lumbar lordosis. Depending on the statistical findings, it can be used to evaluate but more research is necessary to reveal its advantages and limitations. On the other hand, when Cobb angles were analyzed, the symptomatic angle values found in our study were lower than many asymptomatic studies. In addition, there was no significant difference in the lumbar lordosis of individuals who presented to clinics symptomatically due to gender and age. The current study will aid clinicians and researchers in their understanding of lumbar lordosis.
Data Availability
The datasets generated during and/or analyzed during the current study are not publicly available due “Personal Data Protection Law” (No: 6698). But are available from the corresponding author on reasonable request.
References
Önen MR, Naderi S (2013) Spinal deformitelere genel Yaklaşım. Türk Nöroşirürji Dergisi 23(2):1–12
Üzümcügil O, Benli İT, Ofluoğlu E (eds) (2016) Omurganın sagital plan deformiteleri. Türk Omurga Derneği Yayınları, Fatih
Arıncı K, Anatomi EA, Kitapevi G (2006) 1. cilt. 4. baskı
Battié MC, Videman T, Kaprio J et al (2009) The Twin Spine Study: contributions to a changing view of disc degeneration. Spine J 9:47–59
Cote P, Cassidy JD, Yong-Hing K et al (1997) Apophysial joint degeneration, disc degeneration, and sagittal curve of the cervical spine. Can they be measured relaibly on radiographs? Spine 22:859–864
Adams MA, Hutton WC (1985) The effect of posture on the lumbar spine. J Bone Joint Surg [Br] 67:625–629
Bernhardt M, Bridwell KH (1989) Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine 14:717–721
Chokshi FH, Kadom N, Dwivedi N et al (2019) Radiographic Cobb angle: a feature of congenital lumbar spine stenosis. Curr Probl Diagn Radiol 48(1):45–49
Sunami T, Kotani T, Aoki Y et al (2022) Large lumbar lordosis is a risk factor for lumbar spondylolysis in patients with adolescent idiopathic scoliosis. Spine 47(1):76–81
Kawkabani G, Saliby RM, Mekhael M et al (2021) Gait kinematic alterations in subjects with adult spinal deformity and their radiological determinants. Gait Posture 88:203–209
Karademìr M, Karavelioğlu E, Boyaci MG et al (2014) Omurgada sagittal dengenin önemi ve spinopelvik parametreler. J Turkish Spinal Surg 25(2):139–148
Berlemann U et al (1999) The role of lumbar lordosis, vertebral end-plate inclination, disc height, and facet orientation in degenerative spondylolisthesis. Clin Spine Surg 12(1):68–73
Adams MA, Mannion AF, Dolan P (1999) Personal risk factors for first-time low back pain. Spine 24(23):2497
Booth KC et al (1999) Complications and predictive factors for the successful treatment of flatback deformity (fixed sagittal imbalance). Spine 24(16):1712
Been E, Kalichman L (2014) Lumbar lordosis. Spine J 14(1):87–97
Schwab F et al (2009) P26 Pre-operative pelvic parameters must be considered to achieve adequate sagittal balance after lumbar osteotomy. Spine J 9(10):129S
Russell BS, Muhlenkamp-Wermert KA, Hoiriis KT (2020) Measurement of lumbar Lordosis: a comparison of 2 alternatives to the cobb angle. J Manipulative Physiol Ther 43(8):760–767
Hong JY et al (2010) Reliability analysis for radiographic measures of lumbar lordosis in adult scoliosis: a case–control study comparing 6 methods. Eur Spine J 19:1551–1557
Lee JS et al (2013) Radiographic measurement reliability of lumbar lordosis in ankylosing spondylitis. Eur Spine J 22:813–818
Berlemann U et al (1998) Facet joint remodeling in degenerative spondylolisthesis: an investigation of joint orientation and tropism. Eur Spine J 7:376–380
Vrtovec T, Pernuš F, Likar B (2009) A review of methods for quantitative evaluation of spinal curvature. Eur Spine J 18:593–607
Celestre PC, Dimar JR, Glassman SD (2018) Spinopelvic parameters: lumbar lordosis, pelvic incidence, pelvic tilt, and sacral slope: what does a spine surgeon need to know to plan a lumbar deformity correction? Neurosurg Clin N Am 29(3):323–329
Anderson ROBERT (1999) Human evolution, low back pain. Evolut Med 17:333
Lang-Tapia M, España-Romero V, Anelo J et al (2011) Differences on spinal curvature in standing position by gender, age and weight status using a noninvasive method. J Appl Biomech 27:143–150
Gelb DE et al (1995) An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 20(12):1351–1358
Legaye J et al (1998) Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 7:99–103
Harrison DE, Harrison DD, Cailliet R et al (2001) Radiographic analysis of lumbar lordosis: centroid, Cobb, TRALL, and Harrison posterior tangent methods. Spine 26:E235-242
Korovessis P, Stamatakis M, Baikousis A (1999) Segmental roentgenographic analysis of vertebral inclination on sagittal plane in asymptomatic versus chronic low back pain patients. J Spinal Disord 12(2):131–137
Korovessis PG, Stamatakis MV, Baikousis AG (1998) Reciprocal angulation of vertebral bodies in the sagittal plane in an asymptomatic Greek population. Spine 23(6):700–704
Gülru ESEN et al (2020) Sağlıklı yetişkinlerde lumbal lordoz ve lumbosakral bölgenin fizyolojik sagital indeks değerleri. Adıyaman Üniversitesi Sağlık Bilimleri Dergisi 6(3):343–356
Vialle RAPHAËL et al (2005) Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. JBJS 87(2):260–267
Patrick N, Emanski E, Knaub MA (2014) Acute and chronic low back pain. Med Clin 98(4):777–789
Chen YL (1999) Centroid measurement of lumbar lordosis compared with the Cobb technique. Spine 24:1786–1790
Okpala FO (2018) Comparison of four radiographic angular measures of lumbar lordosis. J Neurosci Rural Pract 09(03):298–304
Chernukha KV, Daffner RH, Reigel DH (1998) Lumbar lordosis measurement A new method versus Cobb technique. Spine 23:74–79
OKCU G et al. (2000) Lomber Omurganın Sagittal planda radyolojik analizi
Demir M et al (2018) Radiographic analysis of the lumbar and sacral region angles in young Turkish adults. J Pak Med Assoc 68(8):1212–1216
Jackson RP, McManus AC (1994) Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine 19(14):1611–1618
Araújo F et al (2014) Individual and contextual characteristics as determinants of sagittal standing posture: a population-based study of adults. Spine J 14(10):2373–2383
Cobb JR (1948) Outline for the study of scoliosis. Instr Course Lect 5:261–275
Janik TJ et al (1998) Can the sagittal lumbar curvature be closely approximated by an ellipse? J Orthop Res 16(6):766–770
Chen Y, Chen W, Chiou W (2007) An alternative method for measuring scoliosis curvature. Orthopedics-New Jersey- 30(10):828
Ferguson AB (1930) Study and treatment of scoliosis. South M J 23:116
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of ınterest
There was no conflict of interest.
Ethical approval
Approval was obtained from the ethics committee of Çukurova University (Date: 04.02.2021, Decision no: 110/58).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article was produced from a master’s thesis.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Tekeli, M., Erdem, H., Kilic, N. et al. Evaluation of lumbar lordosis in symptomatic individuals and comparative analysis of six different techniques: a retrospective radiologic study. Eur Spine J 32, 4118–4127 (2023). https://doi.org/10.1007/s00586-023-07886-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07886-z