
Abstract
Purpose
In adolescent idiopathic scoliosis (AIS), spinal deformity can be seen in the thoracic or in the lumbar area. Although differences according to curve location are well described on standard radiographs, dynamic consequences of such difference remain unclear. Our objective was to explore the differences in dynamic spinal balance according to curve location in AIS patients using gait analysis
Methods
We prospectively included 22 females with AIS planned for surgical correction (16.3 years old, 81% Risser ≥ 4). Patients were divided into two matched cohorts, according to major curve location [right thoracic (Lenke 1) or left lumbar (Lenke 5)]. Gait analysis was performed the day before surgery. Global balance was analyzed as the primary outcome. Local curves parameters (dynamic Cobb angles) were defined as the secondary outcome.
Results
In coronal plane, Lenke 5 patients had a left trunk shift, whereas trunk was shifted to the right in Lenke 1 patients (− 20.7 vs 6.3, p = 0.001). In the sagittal plane, the main difference between the two groups was T12 position that remained over the pelvis during gait in Lenke 5 patients, whereas it was anterior to the pelvis in Lenke 1 patients. In the transversal plane, Lenke 5 and Lenke 1 patients presented the same gait abnormalities, with a global trunk rotation to the left (− 4.8 vs − 7.6, p = 0,165).
Conclusion
This is the first study to provide the results of a direct comparison between Lenke 1 and Lenke 5 patients during gait. Curve location influenced coronal and sagittal balance, but abnormalities of transversal trunk motion were the same, wherever the curve was located.
Graphic abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescent idiopathic scoliosis is three-dimensional deformity of the spine. It is described as the result of vertebral rotation at the apex of the deformity, causing a coronal deviation of the spine and sometimes altering the sagittal profile. Coronal deviation direction is directly linked to vertebral rotation direction [1,2,3]. Thereby, right-side rotation will lead to a right-side coronal deviation, and vice versa [4, 5]. In 2005, Lenke et al. proposed a classification for these patients, according to the location of the main deformity [6]. Lenke type 1 defines scoliosis with a main thoracic curve, generally right-sided. Conversely, Lenke type 5 defines scoliosis with a main thoraco-lumbar or lumbar curve, toward the left side in most of the cases. So far, mechanisms leading to idiopathic scoliosis remain unknown. Especially, the reason why rotation direction according to curve location is stereotyped has not been elucidated.
Long-term studies have established that some curves keep worsening after skeletal maturity and therefore need surgical correction during adolescence or early adulthood, in order to prevent progression. Most of the authors agree that lumbar curves are generally more evolutive after skeletal maturity and will therefore need arthrodesis for lower magnitude than thoracic curves [7]. However, the impact of these curves on spine functioning during adolescence is not well documented. Furthermore, no data explain why lumbar curve is more at risk of worsening in adulthood than thoracic ones.
Modern tools such as gait analysis are now available for the assessment of spine functioning during daily life activities. Originally designed for neuro-orthopedics patients, this technique has gained in popularity and has enlarged its field of application, such as hip and knee reconstruction surgery [8, 9]. An increasing number of studies have shown that it was feasible to assess trunk and spine motion with this innovative technique [10,11,12]. Using gait analysis, several authors have reported that adolescents with idiopathic scoliosis suffered gait impairment, mostly in the transverse plane [11,12,13,14,15,16]. However, most of the results were reported in patients with right thoracic scoliosis. To the best of our knowledge, no study has attempted to compare gait impairment in adolescent idiopathic scoliosis patients according to curve location.
Our hypothesis was that curve location and rotation direction had an influence on gait abnormalities in adolescent idiopathic scoliosis patients. Our objective was to compare trunk kinematics between Lenke type 1 and Lenke type 5 adolescent idiopathic scoliosis patients using gait analysis.
Patients and methods
Ethics
The study was approved by our institutional review board. Prior to inclusion in the study, a written consent was obtained from each participant after clear information was given.
Study design and population
From January 2015 to August 2018, we conducted a single-center prospective observational study. We recruited adolescents consecutively planned for idiopathic scoliosis surgical correction. Inclusion criteria were as follows: (1) diagnosis of adolescent idiopathic scoliosis, (2) right thoracic curve (Lenke 1) or left lumbar curve (Lenke 5). In order to avoid being biased by any lumbar component, only Lenke 1 patients with a lumbar modifier type A according to Lenke classification were included. Patients with history of major orthopedic trauma, previous spine surgery or transitional vertebrae were excluded from the study.
Protocol
The day before surgery, antero-posterior and lateral full-spine standing radiographs were taken. Additionally, patients underwent gait analysis. Our laboratory is equipped with six high-resolution infrared cameras sampled at the frequency of 100 Hz. Following the plug-in-gait protocol modified by Blondel et al. [17,18,19,20], patients were equipped with a set of 36 reflective markers. Six markers were used for the description of the spine (C7, T6, T9, T12, L3, S1). Patients were asked to walk barefoot, on a 9-m walkway at a self-selected speed. Several trials were performed (mean number 4), and the best one (all markers visible, constant speed) was kept for analysis.
Evaluation parameters
Radiographic parameters were measured using a spine dedicated software with a semi-automated measurement method. On AP views, we evaluated the thoracic and lumbar Cobb angles and the coronal vertical axis (horizontal distance between the C7-plumbline and the center of S1, CVA). On lateral views, we measured C2-C7 cervical lordosis, T4-T12 thoracic kyphosis, L1-S1 lumbar lordosis, pelvic parameters (pelvic incidence (PI), pelvic tilt (PT) and sacral slope (SS)) and the sagittal vertical axis (horizontal distance between C7-plumbline and the posterior superior angle of S1, SVA). Curves’ flexibility was assessed using lateral bending films and by calculating the Cincinnati index [21].
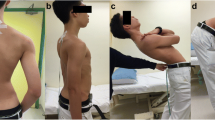
During gait analysis, different local curve parameters were measured (Fig. 1), including dynamic thoracic and lumbar Cobb angles, dynamic thoracic kyphosis (Dyn-TK), dynamic lumbar lordosis (Dyn-LL) and dynamic pelvic tilt (Dyn-PT). In the transverse plane, “orientation” referred to the angle between a line and a line perpendicular to the axis of gait: Shoulder-line orientation (Dyn-SL orientation) was defined as the angle between the bi-acromion line and a line perpendicular to the axis of gait; pelvic orientation (Dyn-P orientation) was defined as the angle between the bi-anterior superior iliac spines line and a line perpendicular to the axis of gait. Finally, the acromion-pelvis angle (APA) was defined as the angle between the bi-acromion line and the bi-ASIS line.

Method of measurement of the different gait parameters. ACR acromion, ASIS antero-superior iliac spine
Global spinal balance parameters were measured as well during gait analysis (Fig. 1), including dynamic CVA (Dyn-CVA), dynamic SVA (Dyn-SVA), C7-S1 coronal and sagittal angles and T12-S1 coronal and sagittal angles. Global spinal balance parameters were defined as the primary outcome of comparison between the two groups and local curves parameters as the secondary outcome.
Statistical analysis
Values are presented as means. In order to improve statistical power, patients were matched according to main Cobb angle magnitude (± 5° tolerance). Prior to analysis, paired T tests were performed and revealed no statistical difference between right and left gait cycles regarding the evaluated parameters (Table 1). Gait parameters were measured at every percentage of the right gait cycle and compared between groups using unpaired T tests when normally distributed. The mean values of every parameter were calculated and compared between groups using unpaired Student’s t tests. The threshold for statistical significance was set at 5% (i.e., p < 0.05).
Results
Study population
During the inclusion period, 321 adolescents underwent idiopathic scoliosis surgical correction in our department. Among them, 126 underwent a gait analysis. After application of our inclusion criteria and matching, 22 patients remained and were included for final analysis (11 in each group). Mean age was 16.3 years old (± 1.8). There were only females. Mean main Cobb angle was 44.1° (± 8.3). Cincinnati indices were not different between the two groups (34% vs 41%, p = 0.342). Demographic and radiographic parameters are reported in Table 2. By design, there was no difference in main Cobb angle between Lenke 1 and Lenke 5 patients (44.8° vs 43.4°, p = 0.321). CVA was different between the two groups, deviated toward the convex side (7.5 mm in right thoracic curves vs − 16.2 mm in left lumbar curves, p = 0.007).
Global spinal balance assessment (primary outcome)
In the coronal plane, there was a clear difference according to curve location (Table 3 and Fig. 2). In Lenke 1 patients, the mean Dyn-CVA during gait was deviated to the right, whereas it was deviated to the left in Lenke 5 patients (6.3 vs − 20.7 mm, p = 0.001). The mean deviation to the convexity was larger in Lenke 5 patients (20.7 vs 6.3 mm, p = 0.013). Therefore, C7-S1 and T12-S1 coronal angles were significantly different between Lenke 1 and Lenke 5 patients (3.2 vs − 5.2°, p < 0.001 and 0.9 vs − 2.7°, p = 0.006, respectively) (Fig. 3).

Comparison of local curves gait parameters between Lenke 1 and Lenke 5 patients. Bold points indicate statistical significance under 5% (p < 0.05)

Comparison of global balance gait parameters between Lenke 1 and Lenke 5 patients. Bold points indicate statistical significance under 5% (p < 0.05)
In the sagittal plane, there was no difference in overall balance, represented by Dyn-SVA and C7-S1 sagittal angle, between Lenke 1 and Lenke 5 patients (Fig. 3). On the other hand, the T12-S1 sagittal angle was significantly lower in Lenke 5 patients when compared to Lenke 1 patients (0.6 vs 8.6°, p = 0.009), meaning that T12 mean position during gait was straight above the pelvis in Lenke 5 patients, whereas the lumbar spine was more inclined forward in Lenke 1 patients.
Finally, in the transverse plane, Lenke 1 and 5 patients had the same gait pattern with the trunk being overall turned to the left side (− 7.6° vs − 4.8°, p = 0.165).
Local curves assessment (secondary outcome)
In the coronal plane, only dynamic thoracic Cobb angle was significantly different between the two groups (12.7° vs 5.8°, p = 0,027) (Table 4 and Fig. 4). Dynamic lumbar Cobb angle was not different in the two groups. None of the other parameters were different between the two groups. Of note, Dyn-SL orientation and Dyn-P orientation were not different (− 5.3° vs − 3.2°, p = 0.303 and 2.3° vs 1.7°, p = 0.656, respectively).

Schematic representation of the mean position during gait of C7 and T12 above the pelvis in the two groups of patients, in the coronal plane (a) and sagittal plane (b). Bold points indicate statistical significance under 5% (p < 0.05)
Discussion
This study is the first one to compare gait parameters in adolescent idiopathic scoliosis patients according to curve location. To the best of our knowledge, only Nishida et al. have reported results on Lenke 1 and Lenke 5 patients, but they compared convex to concave side within these two populations, without proposing a direct comparison [22].
In our study, the main differences between the two populations were found in coronal global balance. There was a lateral trunk shift in the two groups, toward the convexity of the main curve. Lateral shift was significantly larger in Lenke 5 patients (20.7 vs 6.3, p = 0.013), suggesting that lumbar curves lead to more coronal imbalance than thoracic curves during gait. The consequences of this result are uncertain, but this asymmetrical trunk motion during gait may explain why Lenke 5 curves are usually more at risk of worsening after skeletal maturity.
Sagittal balance varied as well. Although overall balance was the same wherever the curve was located (no difference in SVA and C7-S1 sagittal angle), our results suggest that the mechanisms within the spine may be different according to curve location. It has already been reported that in normal gait, a forward inclination of the trunk is needed [23, 24]. Therefore, T12 and C7 should be anterior to S1 when walking. In our study, the mean position of T12 was above the pelvis in Lenke 5 patients, whereas it was more anterior in Lenke 1 patients. Our first hypothesis is that Lenke 1 patients usually lack thoracic kyphosis. Considering that forward leaning of the trunk is mandatory during gait, flexion of the lumbar spine is necessary to provoke a forward trunk inclination, leading to a more anterior position of T12. The second hypothesis is that stiffness of lumbar curves may preclude the lumbar spine from flexion; therefore, T12 remains over S1 and global tilting of the trunk is provoked by flexion of the thoracic area. But this is only hypothetical; further studies including sagittal bending analysis could help elucidating this specific point. So far, very little is known about sagittal balance in AIS patients and future research should focus on clarifying sagittal posture adjustment mechanisms in these patients.
Surprisingly, we found that despite opposite vertebral rotation, Lenke 1 and Lenke 5 patients had the same gait abnormalities in the transversal plane. Indeed, gait abnormalities in the transversal plane have been previously reported by several authors [11,12,13, 16]: AIS patients have been described to walk with the left shoulder remaining backward throughout gait cycle, leading to an overall trunk rotation to the left. However, it only has been reported in Lenke 1 patients. The reason why trunk and vertebras were turned in opposite directions remains unclear. Our results clearly show that trunk rotation abnormalities during gait are not related to vertebral rotation direction or curve location. Indeed, patients in our two groups had opposite vertebral rotation but same transverse plane abnormalities. Nishida et al. have reported differences in transversal plane motion between Lenke 1 and Lenke 5 patients [22]. However, their study was limited to stance phase, which represents about 40–50% of the gait cycle. Our results are in line because we found significant differences in SL-orientation between Lenke 1 and 5 patients during stance phase. However, when considering the whole gait cycle, there was no difference anymore and the mean SL-orientation was to the left in the two groups, whatever the vertebral rotation direction was.
Our study has several limitations. We present our results on a limited sample of patients. However, our sample is homogeneous, with matched cohorts allowing for a reasonable comparison. This study attempts to help understanding idiopathic scoliosis mechanisms and its consequences on spine functioning. Otherwise, using APA as an indicator of spinal rotation is quite inaccurate. Indeed, this parameter only reflects the global behavior of the trunk in the horizontal plane. Due to the absence of consistent osseous landmarks on the anterior aspect of the trunk, it is difficult to catch the exact behavior of the spine itself in the transversal plane. However, APA has been used by many authors [11, 13] and we believe this is the best surrogate when analyzing dynamic aspect of the spinal deformity in this plane and it gives a lot of information about spinal motion. Lastly, we did not analyze kinetic data such as ground reaction forces and moments that were applied at different levels of the spine. This is of great importance, and future research should focus on investigating the role of forces that are applied to the spine in spinal deformity patients.
In conclusion, we found that curve location had an influence on coronal and sagittal balance, but the abnormalities of transversal trunk motion were the same, wherever the curve was located. Our results may suggest that vertebral rotation is not the cause of gait abnormalities. As suggested by some authors, spine deformity may be the consequence of postural control failure [12, 25, 26]. However, as the relationship between gait abnormality and spinal deformity remains unclear, further studies are needed to shed light on this particular point. Including larger samples or comparing patients with opposite rotation in the same spinal area could help understanding this relationship.
References
Perdriolle R, Vidal J (1985) Thoracic idiopathic scoliosis curve evolution and prognosis. Spine (Phila Pa 1976) 10:785–791. https://doi.org/10.1097/00007632-198511000-00001
Perdriolle R, Vidal J (1987) Morphology of scoliosis: three-dimensional evolution. Orthopedics 10:909–915
Stokes IA (1989) Axial rotation component of thoracic scoliosis. J Orthop Res 7:702–708. https://doi.org/10.1002/jor.1100070511
Cholewicki J, Crisco JJ, Oxland TR et al (1996) Effects of posture and structure on three-dimensional coupled rotations in the lumbar spine. A biomechanical analysis. Spine (Phila Pa 1976) 21:2421–2428. https://doi.org/10.1097/00007632-199611010-00003
Tredwell SJ, Sawatzky BJ, Hughes BL (1999) Rotations of a helix as a model for correction of the scoliotic spine. Spine (Phila Pa 1976) 24:1223–1227. https://doi.org/10.1097/00007632-199906150-00009
Lenke LG (2005) Lenke classification system of adolescent idiopathic scoliosis: treatment recommendations. Instr Course Lect 54:537–542
Pesenti S, Jouve JL, Morin C et al (2015) Evolution of adolescent idiopathic scoliosis: results of a multicenter study at 20 years’ follow-up. Rev Chir Orthop Traumatol. https://doi.org/10.1016/j.otsr.2015.05.004
Gage JR (1983) Gait analysis for decision-making in cerebral palsy. Bull Hosp Jt Dis Orthop Inst 43:147–163
Ollivier M, Parratte S, Lunebourg A et al (2016) The John Insall Award: no functional benefit after unicompartmental knee arthroplasty performed with patient-specific instrumentation: a randomized trial. Clin Orthop Relat Res 474:60–68. https://doi.org/10.1007/s11999-015-4259-0
Ranavolo A, Don R, Draicchio F et al (2013) Modelling the spine as a deformable body: feasibility of reconstruction using an optoelectronic system. Appl Ergon 44:192–199. https://doi.org/10.1016/j.apergo.2012.07.004
Lenke LG, Engsberg JR, Ross SA et al (2001) Prospective dynamic functional evaluation of gait and spinal balance following spinal fusion in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 26:E330–E337
Kramers-de Quervain IA, Müller R, Stacoff A et al (2004) Gait analysis in patients with idiopathic scoliosis. Eur Spine J 13:449–456. https://doi.org/10.1007/s00586-003-0588-x
Patel A, Pivec R, Shah NV et al (2018) Motion analysis in the axial plane after realignment surgery for adolescent idiopathic scoliosis. Gait Posture 66:181–188. https://doi.org/10.1016/j.gaitpost.2018.08.015
Yang JH, Suh SW, Sung PS, Park WH (2013) Asymmetrical gait in adolescents with idiopathic scoliosis. Eur Spine J 22:2407–2413. https://doi.org/10.1007/s00586-013-2845-y
Mahaudens P, Banse X, Mousny M, Detrembleur C (2009) Gait in adolescent idiopathic scoliosis: kinematics and electromyographic analysis. Eur Spine J 18:512–521. https://doi.org/10.1007/s00586-009-0899-7
Nishida M, Nagura T, Fujita N et al (2019) Spinal correction surgery improves asymmetrical trunk kinematics during gait in adolescent idiopathic scoliosis with thoracic major curve. Eur Spine J 28:619–626. https://doi.org/10.1007/s00586-018-5741-7
Blondel B, Pomero V, Moal B et al (2012) Sagittal spine posture assessment: feasibility of a protocol based on intersegmental moments. Orthop Traumatol Surg Res 98:109–113. https://doi.org/10.1016/j.otsr.2011.12.001
Blondel B, Viehweger E, Moal B et al (2015) Postural spinal balance defined by net intersegmental moments: results of a biomechanical approach and experimental errors measurement. World J Orthop 6:983–990. https://doi.org/10.5312/wjo.v6.i11.983
Pesenti S, Prost S, Blondel B et al (2019) Correlations linking static quantitative gait analysis parameters to radiographic parameters in adolescent idiopathic scoliosis. Orthop Traumatol Surg Res. https://doi.org/10.1016/j.otsr.2018.09.024
Pesenti S, Prost S, Pomero V et al (2019) Characterization of trunk motion in adolescents with right thoracic idiopathic scoliosis. Eur Spine J 28:2025–2033. https://doi.org/10.1007/s00586-019-06067-1
Vora V, Crawford A, Babekhir N et al (2007) A pedicle screw construct gives an enhanced posterior correction of adolescent idiopathic scoliosis when compared with other constructs: myth or reality. Spine (Phila Pa 1976) 32:1869–1874. https://doi.org/10.1097/BRS.0b013e318108b912
Nishida M, Nagura T, Fujita N et al (2017) Position of the major curve influences asymmetrical trunk kinematics during gait in adolescent idiopathic scoliosis. Gait Posture 51:142–148. https://doi.org/10.1016/j.gaitpost.2016.10.004
Thorstensson A, Nilsson J, Carlson H, Zomlefer MR (1984) Trunk movements in human locomotion. Acta Physiol Scand 121:9–22. https://doi.org/10.1111/j.1748-1716.1984.tb10452.x
Chung CY, Park MS, Lee SH et al (2010) Kinematic aspects of trunk motion and gender effect in normal adults. J Neuroeng Rehabil 7:9. https://doi.org/10.1186/1743-0003-7-9
Assaiante C, Mallau S, Jouve J-L et al (2012) Do adolescent idiopathic scoliosis (AIS) neglect proprioceptive information in sensory integration of postural control? PLoS ONE 7:e40646. https://doi.org/10.1371/journal.pone.0040646
Mallau S, Bollini G, Jouve J-L, Assaiante C (2007) Locomotor skills and balance strategies in adolescents idiopathic scoliosis. Spine (Phila Pa 1976) 32:E14–22. https://doi.org/10.1097/01.brs.0000251069.58498.eb
Funding
No funding was received by any of the author for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare no conflict of interest related to this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Pesenti, S., Pomero, V., Prost, S. et al. Curve location influences spinal balance in coronal and sagittal planes but not transversal trunk motion in adolescents with idiopathic scoliosis: a prospective observational study. Eur Spine J 29, 1972–1980 (2020). https://doi.org/10.1007/s00586-020-06361-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-020-06361-3