
Abstract
Purpose
Exercise therapy such as motor control training (MCT) has been shown to reduce pain and disability in people with low back pain (LBP). It is unknown which patients are most likely to benefit. This longitudinal cohort study aimed to: (1) retrospectively examine records from a large cohort of patients who received MCT treatment, (2) identify potentially important predictors of response to MCT and (3) test the predictors on an independent (split) sample derived from the original cohort of patients, using one group to identify the predictors and the other to test them.
Methods
The response of 775 patients with LBP to MCT was classified as ‘improved’ or ‘not improved’ based on self-reported change in pain levels and symptoms. Measures were examined for associations with improvement and entered into a logistic regression model to classify patients as low, medium or high benefits of improvement with MCT. The model was tested on an independent sample.
Results
A positive response was seen in patients with: no evidence of scoliosis [OR = 4.0, 95% CI (1.7, 9.6)], LBP without associated groin pain [OR = 2.2, 95% CI (1.0, 5.0)], LBP which was chronic recurrent in nature [OR = 3.1, 95% CI (1.8, 5.3)] and poor results on muscle testing of the multifidus muscle [OR = 2.0, 95% CI (1.1, 3.7)]. Testing on an independent sample confirmed that patients could be classified into benefit groups.
Conclusions
This study provides a first step towards assisting clinicians to select patients most likely to respond to MCT.
Graphical abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over the last three decades, changes to key recommendations in clinical practice guidelines for management of low back pain (LBP) have placed greater emphasis on self-management and utilization of individually tailored exercise programmes targeting improvements in function [1]. One form of exercise therapy shown to decrease pain and disability associated with chronic LBP is motor control training (MCT) [2, 3]. MCT refers to the motor, sensory and central processes involved in control of posture and movement. The assumption underlying the MCT concept is that the manner in which the individual loads the spine by their postures, movements and muscle activation strategies contributes to symptom development and persistence. The MCT approach referred to in this paper initially involves retraining of control and endurance of key spinal muscles in static then progressively more functional positions [4, 5].
Due to its diversity in presentations, LBP has been identified as a condition which may be amenable to subgrouping, and the ability to classify or subgroup patients with heterogeneous disorders such as spinal pain has been highlighted previously as a research priority [6, 7]. Subgrouping aims to identify those who may be more or less responsive to treatment based on classifying certain presenting characteristics [8]. The aims of this study were to: (1) retrospectively examine records from a large cohort of patients who received MCT treatment, (2) identify potentially important predictors of response to MCT and (3) test the predictors on an independent (split) sample derived from the original cohort of patients, using one group to identify the predictors and the other to test them [9].
Methods
In this longitudinal cohort study, the medical records of patients who attended a hospital-based research clinic between 1998 and 2016 for assessment and management of LBP were audited. Charts were included if patients were aged 18 years and above at the time of assessment, reported a history of LBP and attended an initial assessment and at least two subsequent treatment sessions. LBP was defined as pain localized between the T12 vertebral level and the gluteal fold [10]. In addition, records were also audited for an independent sample of patients. The Mater Misericordiae Ltd Human Research Ethics Committee approved the study, and all patients provided informed consent.
Clinical assessment procedure
Experienced musculoskeletal physiotherapists performed the standardized assessments and treatments. Patients completed questionnaires to provide demographic information, their medical history and the location of their symptoms on a body chart. Pain intensity was assessed using a visual analogue scale (VAS) [11]. Patient-reported functional measures were assessed using the Roland Morris Disability Questionnaire (RMDQ) [12], which has been used extensively in LBP research and has excellent reliability and good construct validity [13]. Activity levels were ascertained using the Habitual Activity Questionnaire (HAQ) [14], a validated tool which addresses domains of occupational physical activity, sport during leisure time and physical activity during leisure time excluding sport [15]. Acute LBP was categorized as LBP lasting less than 4–6 weeks of duration [16]. Chronic LBP was categorized as ‘chronic continuous’ (ongoing pain with minimal variation in pain intensity), ‘chronic fluctuating’ (ongoing pain with variation in pain intensity and without periods of ‘no pain’) or ‘chronic recurrent’ LBP (or episodic, with more than one period of pain over one year separated by periods of ‘no pain’) [17].
The physical examination included a clinical assessment of posture, active range of spinal motion, neurological conduction tests of the lower extremity (if pain was referred beneath the gluteal fold, to determine whether radiculopathy was present), manual examination, clinical muscle testing of trunk muscles [10] and measurement of cross-sectional area (CSA) of the lumbar multifidus muscle using ultrasound imaging [18] (Diasonics Synergy, Japan, or LOGIQ e, GE Healthcare, Wuxi, China). Previous research has established the validity of this measurement method [19].
Treatment—motor control training approach
All participants received MCT, which included patient education/advice and provision of a self-managed exercise programme. The underlying premise of MCT is that input from the spine and/or related tissues secondary to suboptimal loading can contribute to ongoing symptoms. The MCT programme aimed to identify and modify the suboptimal features, with a focus on integration of these modifications into function. Details of the MCT programme have been previously described [5]. In brief, MCT consists of a staged programme including: testing and training control of key trunk muscles; training postures, movement patterns and body awareness; and functional integration and conditioning.
Chart review process
An independent researcher evaluated all medical records. Information obtained from the initial assessment included results of the formal questionnaires (RMDQ, HAQ, VAS) as well as information derived from the patient interview and physical examination. For the subsequent treatment sessions, self-reported level of pain and symptoms were extracted from the records. To determine outcome, patients were classified as ‘improved’ or ‘not improved’ based on their self-reported improvement (or lack of improvement) in their level of pain or nominated presenting symptoms at the last treatment session. Patients were asked to report whether they were ‘better’, ‘same’ or ‘worse’. Responses recorded as ‘better’ were categorized as the ‘improved’ group, and responses recorded as ‘same’ or ‘worse’ were categorized as the ‘not improved’ group.
Statistical analysis
Data were analysed using SPSS version 22.0 [IBM, USA]. Descriptive statistics for patient demographics and initial assessment outcome measures are presented for the ‘improved’ and ‘not improved’ groups as numbers and percentages (%) for categorical variables and means and standard deviations (SD) for continuous variables. Receiver operating characteristic (ROC) curves were used to calculate the optimal cut point in the continuous variables that predicted improvement. Optimal cut points were then used to convert significant continuous variables (p < 0.10) to a binary form. Cross-tabulations and Chi-squared tests were used to assess the relationship between the significant binary explanatory variables (p < 0.10) and improvement (yes or no). Variables were then ranked in order of their clinical significance and then their univariate association and were entered into a logistic regression using a forward sequential method to obtain their independent multivariate effects. To create a final parsimonious model, variables were retained in the model if p < 0.10 and the significance level was set at p < 0.05. To predict treatment success, beta coefficients from the final model were rounded and used to classify patients as being of high, medium or low levels of benefit of treatment. Sensitivity and specificity for each level of benefit were estimated from a 2 × 2 cross-tabulation using the low-benefit group as the reference category. Positive predictive value (PPV) was estimated for each level of benefit category using the row percentages from the cross-tabulation.
Testing the predictors
The predictors were tested on an independent (split) sample of patients who had completed a VAS rating at their initial and their last appointment at the clinic and who had received two or more treatment sessions. The subset sample was randomly selected by the statistician, who was independent of the research clinic, and the population was split into two groups. T tests and Chi-squared analysis were used to assess whether there were significant differences between the independent sample and the cohort used to develop the rule. Participants were classified into high, medium or low levels of benefit for improvement from MCT based on the clinical predictors identified in the logistic regression model. Using repeated measures ANOVA, the initial VAS and post-treatment VAS scores were compared across the different levels of benefit as a measure of the change in pain from the beginning to end of treatment. ‘Pain level’ (baseline versus end of treatment) was included as a within-subject factor, and ‘level of benefit’ (high, medium and low) was included as a between subjects factor. Homogeneity of variances assumption was satisfied (p > 0.05). Significance level was set at p < 0.05.
Results
Patient demographics and initial assessment findings
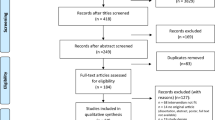
Of the 1861 patients who attended the clinic from 26 February 1998 to 15 January 2016, a total of 775 had complete data for their initial assessment and attended two or more treatment sessions. A large number of patients were not included in the study as they attended the clinic for consultation purposes only. Descriptive statistics for patient demographics and initial assessment outcome measures are presented for the ‘improved’ and ‘not improved’ groups in Table 1. Of the initial assessment findings, characteristics of LBP (chronic continuous and chronic recurrent), location of pain in other parts of the body (groin region), prior treatment (surgery), evidence of scoliosis (including mild) and the ability to contract the multifidus muscle at L5 were significantly different between the groups who did and did not improve with MCT (p < 0.10) (Table 1). Disability (RMDQ score), duration of current pain (months) and level of pain (VAS) were significantly different between groups (all p < 0.10) (Table 2). All other initial assessment findings were found to be not significantly different between groups (all p > 0.10) (see Online Resource 1).
Variables predictive of response to MCT treatment
To identify variables which were predictive of response to treatment, all continuous variables were dichotomized using the value that optimized the sensitivity and specificity in predicting level of improvement with MCT. ROC analyses identified that factors such as less disability (as indicated by the RMDQ), lower levels of pain and shorter duration of LBP predicted improvement in response to MCT (all p < 0.05) (see Online Resource 2).
Initial assessment variables that were predictive of a beneficial response to MCT treatment are shown in Table 3. Results of the logistic regression model indicated that the benefit variables for improvement with MCT were: ‘negative for evidence of scoliosis’ (including mild scoliosis), ‘positive for type of pain’ (chronic recurrent) and ‘positive for poor activation of the multifidus muscle at the L5 vertebral level’ (left and right sides) (all p < 0.05). Although ‘negative for groin pain’ was not statistically significant at the critical value, the point estimate and confidence intervals for its odds ratio provide evidence that it should be included as a benefit variable.
To predict treatment success, patients were then classified into ‘level of benefit’ groups based on the benefit variables: high level of benefit comprised the presence of four of the benefit variables, medium level of benefit comprised the presence of three variables and low level of benefit comprised the presence of two or less variables (Table 4).
Testing the predictors
To test the predictors, an independent sample of 47 patients who had received 2 or more treatment sessions and completed a VAS at their initial assessment and final treatment session was included. The sample was shown to be comparable with the larger cohort based on the assessment of demographic and initial assessment variables (all p > 0.05) (see Online Resource 3). Participants were classified into groups of high, medium or low levels of benefit for improvement with MCT based on the clinical predictors identified in the logistic regression model. There were 19 (40.4%) participants classified as high level of benefit, 18 (38.3%) classified as medium level of benefit and 10 (21.3%) classified as low level of benefit. Results of the repeated measures ANOVA found that there was a significant interaction between time and benefit group (F (2.0, 44.0) = 16.91, p = 0.009), indicating that there was a significant difference in pain intensity from the beginning to the end of treatment between the benefit groups (Table 5). The mean (SD) VAS for the sample of 47 patients at initial assessment was 5.5 (1.8) cm and 3.3 (2.2) cm at the conclusion of treatment, which exceeds the minimal clinically important effect (1.5 out of 10 points) for the VAS [20]. Results for each of the three benefit groups showed that the mean difference in the VAS exceeded the minimally clinically important effect (MCID) for the high- and medium-benefit groups, but did not exceed the MCID for the low-benefit group.
Discussion
Results of the current retrospective investigation showed that variables which were predictive of a positive response to MCT could be identified at the first treatment session. One variable predictive of a positive response to MCT was poor performance on testing of the multifidus muscle. Poor ability to contract the multifidus muscle has been previously demonstrated in people with acute [21] and chronic LBP [22]. The mechanisms underpinning changes in the multifidus muscle associated with LBP which might affect the ability to contract the muscle are complex and time dependent and are only beginning to be understood. In the acute phase, animal studies have demonstrated reduced neural drive to the multifidus muscle (consistent with muscle inhibition) immediately after injury [23]. However, the changes in the muscle appear to shift to fibrotic, adipose and muscle fibre-type changes in the subacute period [24]. In the chronic phase of LBP, more generalized changes appear which are more consistent with disuse [25]. A possible explanation for the finding in the current investigation is that those with poorer control of the muscle on initial assessment may have more potential to improve in response to intervention. Previous studies have shown that improvements in multifidus muscle size and function associated with MCT are commensurate with a reduction in LBP [21, 26]. The multifidus muscle plays a key role in proprioception [27] and control of the lumbar lordosis [28]. The ability to better control and be aware of the position of the lumbar lordosis may allow patients to optimize loading on the lumbar spine and thereby minimize the persistence of symptoms [29].
Results from the current investigation also showed that the type of pain presentation was important. A previous study which classified LBP patients reported that the ‘chronic recurrent’ (episodic) subgroup represented the most common presentation of LBP [17]. In the current investigation, MCT was found to be more effective for these patients. A possible explanation for this finding may be that patients with episodic LBP have opportunities to exercise in the pain-free periods between episodes. This is important, as the presence of LBP has been shown to be associated with inhibition of trunk muscles such as the multifidus muscle [23]. Being able to exercise effectively and possibly more often in pain-free periods may also potentially mitigate the changes seen in trunk muscles such as the multifidus muscle thought to be associated with disuse [30, 25]. Exercising in pain-free periods may therefore have the potential to assist recovery, and the adoption of self-management strategies may possibly help to prevent recurrences [31].
Our findings suggested that patients with LBP and groin pain were less likely to respond to MCT than those without groin pain. It is possible that these patients may have had associated hip joint pathology [32], as the groin region is the most common site of symptoms for hip joint pathologies such as hip osteoarthritis, femoroacetabular impingement and labral pathology [33].
Finally, patients with LBP who reported that they had a scoliosis were four times less likely to respond to MCT. However, these results should be interpreted with caution, as the presence of scoliosis was self-reported and only assessed clinically, not radiographically, so any relationship between the amount of structural deformity and the response to treatment is unknown.
In summary, results of the current investigation could represent a first step towards assisting clinicians to select patients who are the most likely to respond to MCT. Eighty-two per cent of patients with the four indicators identified were likely to respond to MCT treatment (high benefit), compared with only 54% of patients in the low-benefit category. When tested on an independent sample of patients, patients were successfully classified into high-, medium- and low-benefit categories regarding improvement associated with MCT.
The main limitations of this study were the use of retrospective clinical data, variation in the total number of treatments per patient and the lack of a control group. In addition, different physiotherapists administered the intervention, and it is possible that this may have had an impact on the outcome which was not adjusted for in the model. Another limitation is that the variables derived from the retrospective review of medical charts had low sensitivity and specificity. Future studies could include more detailed assessments of hip joint pathology and scoliosis to accurately estimate sensitivity and specificity.
References
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, Ferreira PH, Fritz JM, Koes BW, Peul W, Turner JA, Maher CG (2018) Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet (London, England) 391(10137):2368–2383. https://doi.org/10.1016/s0140-6736(18)30489-6
Searle A, Spink M, Ho A, Chuter V (2015) Exercise interventions for the treatment of chronic low back pain: a systematic review and meta-analysis of randomised controlled trials. Clin Rehabil 29(12):1155–1167. https://doi.org/10.1177/0269215515570379
Saragiotto BT, Maher CG, Yamato TP, Costa LO, Costa LC, Ostelo RW, Macedo LG (2016) Motor control exercise for nonspecific low back pain: a cochrane review. Spine (Phila Pa 1976) 41(16):1284–1295. https://doi.org/10.1097/brs.0000000000001645
Hides JA, Donelson R, Lee D, Prather H, Sahrmann SA, Hodges PW (2019) Convergence and divergence of exercise-based approaches that incorporate motor control for the management of low back pain. J Orthop Sports Phys Ther 49(6):437–452. https://doi.org/10.2519/jospt.2019.8451
Hides JA, Stanton WR, Mendis MD, Gildea J, Sexton MJ (2012) Effect of motor control training on muscle size and football games missed from injury. Med Sci Sports Exerc 44(6):1141–1149. https://doi.org/10.1249/MSS.0b013e318244a321
Borkan JM, Koes B, Reis S, Cherkin DC (1998) A report from the second international forum for primary care research on low back pain. Reexamining priorities. Spine 23(18):1992–1996
Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J, York J, Das A, McAuley JH (2009) Characteristics of patients with acute low back pain presenting to primary care in Australia. Clin J Pain 25(1):5–11. https://doi.org/10.1097/AJP.0b013e3181817a8d
Delitto A, Erhard RE, Bowling RW (1995) A treatment-based classification approach to low back syndrome: identifying and staging patients for conservative treatment. Phys Ther 75 (6):470-485. (discussion 485–479)
McGinn TG, Guyatt GH, Wyer PC, Naylor CD, Stiell IG, Richardson WS (2000) Users' guides to the medical literature: XXII: how to use articles about clinical decision rules. Evidence-Based Medicine Working Group. Jama 284(1):79–84
Hides J, Stanton W, Dilani Mendis M, Sexton M (2011) The relationship of transversus abdominis and lumbar multifidus clinical muscle tests in patients with chronic low back pain. Man Ther 16(6):573–577. https://doi.org/10.1016/j.math.2011.05.007
Scott J, Huskisson EC (1976) Graphic representation of pain. Pain 2(2):175–184. https://doi.org/10.1016/0304-3959(76)90113-5
Roland M, Morris R (1983) A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine (Phila Pa 1976) 8(2):141–144
Stevens ML, Lin CCW, Maher CG (2016) The Roland Morris disability questionnaire. J Physiother 62(2):116. https://doi.org/10.1016/j.jphys.2015.10.003
Baecke JA, Burema J, Frijters JE (1982) A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36(5):936–942
Florindo AA, Latorre Mdo R, Santos EC, Negrao CE, Azevedo LF, Segurado AA (2006) Validity and reliability of the Baecke questionnaire for the evaluation of habitual physical activity among people living with HIV/AIDS. Cad Saude Publica 22(3):535–541.https://doi.org/10.1590/S0102-311x2006000300008
Menezes Costa LDC, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LOP (2012) The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ 184(11):E613–E624. https://doi.org/10.1503/cmaj.111271
Kongsted A, Hestbaek L, Kent P (2017) How can latent trajectories of back pain be translated into defined subgroups? BMC Musculoskelet Disord. https://doi.org/10.1186/s12891-017-1644-8
Hides J, Gilmore C, Stanton W, Bohlscheid E (2008) Multifidus size and symmetry among chronic LBP and healthy asymptomatic subjects. Man Ther 13(1):43–49. https://doi.org/10.1016/j.math.2006.07.017
Hides JA, Richardson CA, Jull GA (1995) Magnetic resonance imaging and ultrasonography of the lumbar multifidus muscle. Comparison of two different modalities. Spine 20(1):54–58
Ostelo RWJG, Deyo RA, Stratford P, Waddell G, Croft P, Von Korff M, Bouter LM, De Vet HC (2008) Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine 33(1):90–94. https://doi.org/10.1097/BRS.0b013e31815e3a10
Hides JA, Richardson CA, Jull GA (1996) Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain. Spine 21(23):2763–2769. https://doi.org/10.1097/00007632-199612010-00011
Wallwork TL, Stanton WR, Freke M, Hides JA (2008) The effect of chronic low back pain on size and contraction of the lumbar multifidus muscle. Man Ther 14(5):496–500. https://doi.org/10.1016/j.math.2008.09.006
Hodges PW, Galea MP, Holm S, Holm AK (2009) Corticomotor excitability of back muscles is affected by intervertebral disc lesion in pigs. Eur J Neurosci 29(7):1490–1500. https://doi.org/10.1111/j.1460-9568.2009.06670.x
Hodges PW, James G, Blomster L, Hall L, Schmid A, Shu C, Little C, Melrose J (2015) Multifidus muscle changes after back injury are characterized by structural remodeling of muscle, adipose and connective tissue, but not muscle atrophy: molecular and morphological evidence. Spine 40(14):1057–1071. https://doi.org/10.1097/brs.0000000000000972
Zhao W-P, Kawaguchi Y, Matsui H, Kanamori M, Kimura T (2000) Histochemistry and morphology of the multifidus muscle in lumbar disc herniation: comparative study between diseased and normal sides. Spine 25(17):2191–2199. https://doi.org/10.1097/00007632-200009010-00009
Hides JA, Stanton WR, McMahon S, Sims K, Richardson CA (2008) Effect of stabilization training on multifidus muscle cross-sectional area among young elite cricketers with low back pain. J Orthop Sports Phys Ther 38(3):101–108. https://doi.org/10.2519/jospt.2008.2658
Nitz AJ, Peck D (1986) Comparison of muscle spindle concentrations in large and small human epaxial muscles acting in parallel combinations. The American surgeon 52(5):273–277
Kiefer A, Shirazi-Adl A, Parnianpour M (1997) Stability of the human spine in neutral postures. Eur Spine J: Off Publ Eur Spine Soc, Eur Spinal Deform Soc, Eur Sect Cerv Spine Res Soc 6(1):45–53
Welch N, Moran K, Antony J, Richter C, Marshall B, Coyle J, Falvey E, Franklyn-Miller A (2015) The effects of a free-weight-based resistance training intervention on pain, squat biomechanics and MRI-defined lumbar fat infiltration and functional cross-sectional area in those with chronic low back. BMJ Open Sport Exer Med 1(1):e000050–e000050. https://doi.org/10.1136/bmjsem-2015-000050
Hides JA, Belavý DL, Stanton W, Wilson SJ, Rittweger J, Felsenberg D, Richardson CA (2007) Magnetic resonance imaging assessment of trunk muscles during prolonged bed rest. Spine 32(15):1687–1692. https://doi.org/10.1097/BRS.0b013e318074c386
Hides JA, Jull GA, Richardson CA (2001) Long-term effects of specific stabilizing exercises for first-episode low back pain. Spine (Phila Pa 1976) 26(11):E243–E248
DeFroda SFMD, Daniels AHMD, Deren MEMD (2016) Differentiating radiculopathy from lower extremity arthropathy. Am J Med 129(10):1124.e1121–1124.e1127. https://doi.org/10.1016/j.amjmed.2016.06.019
Holmich P (2007) Long-standing groin pain in sportspeople falls into three primary patterns, a "clinical entity" approach: a prospective study of 207 patients. Br J Sports Med 41(4):247–252. (discussion 252). https://doi.org/10.1136/bjsm.2006.033373
Acknowledgements
This research was funded by the Queensland Health Physiotherapy Research Fellowship and Mater Research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The Mater Misericordiae Ltd Human Research Ethics Committee approved the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hides, J.A., Murphy, M., Jang, E. et al. Predicting a beneficial response to motor control training in patients with low back pain: a longitudinal cohort study. Eur Spine J 28, 2462–2469 (2019). https://doi.org/10.1007/s00586-019-06045-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-019-06045-7