
Abstract
Purpose
Application of AOSpine subaxial cervical spine injury classification system to explore the optimal surgical decompression timing for different types of traumatic cervical spinal cord injury (CSCI).
Methods
A single-center prospective cohort study was conducted that included patients with traumatic CSCIs (C3–C7) between February 2015 and October 2016. After enrollment, patients underwent either early (< 72 h after injury) or late (≥ 72 h after injury) decompressive surgery of the cervical spinal cord. Each group was divided into A0, A1-4, B, C/F4 and F1-3 subgroups. The primary outcomes were ordinal changes in the ASIA Impairment Scale (AIS) and the Spinal Cord Independence Measure III (SCIM version 3) at a 12-month follow-up. The secondary outcomes included length of hospital stay, postoperative neurological deterioration, other complications and mortality.
Results
A total of 402 patients were included. Of these, 187 patients underwent early decompression surgery, and 215 patients underwent delayed decompression surgery. Statistical results included the following comparisons of the early vs late groups: AIS improvement ≥ 1 grade (combined groups: P < 0.0001; A0: P = 0.554; A1-4: P = 0.084; B: P = 0.013; C/F4: P = 0.040; F1-3: P = 0.742); AIS improvement ≥ 2 grades, P = 0.003 for all groups; SCIM version 3 (combined groups: P < 0.0001; A0: P = 0.126; A1-4: P = 0.912; B: P = 0.006; C/F4: P = 0.111; F1-3: P = 0.875).
Conclusion
Type A and F1-3 fractures are not required to undergo aggressive early decompression. Type B and type C/F4 fractures should receive early surgical treatment for better clinical outcomes.
Graphical abstract
These slides can be retrieved under Electronic Supplementary Material.

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of acute traumatic cervical spinal cord injury (CSCI) has been increasing worldwide, and surgical decompression is considered to be the most effective means of treatment; whether it is anterior decompression, posterior decompression or anterior–posterior combined decompression, there is still some controversy about surgical timing. At present, most scholars support the idea that early decompression can lead to better neurological recovery outcomes [1,2,3,4], so most spine surgeons are interested in early surgery when managing patients with a CSCI. However, whether all patients with different levels of trauma severity require early decompression surgery has not been studied. In addition, other factors such as length of hospital stay, neurological deterioration, other complications and mortality should also be taken into account.
In recent years, with the introduction of the AOSpine subaxial cervical spinal cord injury classification system (SCSICS), various types of cervical trauma have been summarized in detail. This classification system can comprehensively reflect the situation of patients at the time of injury and allows for the effective combination of imaging and clinical manifestations to facilitate doctor–patient communication and academic exchanges. Testing has shown that the system has a high reliability, validity and repeatability and is simple and clear [5,6,7]. However, the current classification cannot objectively and systematically guide clinical diagnosis and treatment, nor can it provide a good judgment on the prognosis of an injury [8]. Therefore, we used this classification system to explore the surgical decompression timing of each type of AOSpine SCSICS.
Materials and methods
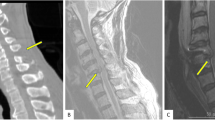
A prospective cohort study was designed in the Western Orthopedic Trauma Center in China, and patients who suffered a traumatic CSCI were enrolled between February 2015 and October 2016 after the approval of the Xi’an Jiaotong University-affiliated Honghui Hospital Ethics Committee. Inclusion criteria included the following: 1. age 16–80; 2. initial ASIA Impairment Scale (AIS) grade A-D; 3. spinal cord compression or injury confirmed by MRI or CT myelography; 4. patients and their families willing to incorporate this study after reading informed consent forms; 5. cervical spinal injury level C3–C7; 6. Subaxial Injury Classification (SLIC) score ≥ 4; and 7. treatment with decompression, fusion and fixation surgery. Exclusion criteria included the following: 1. penetrating injuries to the neck; 2. major neurological deficits or illness before the injury; 3. serious, life-threatening injury that prohibited early surgical decompression; 4. arrival at the orthopedic trauma center > 72 h after the CSCI; 5. surgery > 7 days after the CSCI; 6. lower cervical vertebral infection, tumors or ankylosing spondylitis with cervical spinal stenosis; and 7. CSCI combined with thoracolumbar fractures or multiple system injuries. After enrollment, patients underwent either early (< 72 h after injury) or late (≥ 72 h after injury) decompressive surgery of the cervical spinal cord. Surgical indications are based on the SLIC system, where a total score ≥ 5 recommends surgical treatment and a total score = 4 indicates that the decision for surgery should be based on the specific circumstances of patients, such as vital signs, patient’s intention for surgery and life quality requirements. The timing of the operation intervention was based on the time required for prehospitalization transportation, preoperative examination and medical preparation. Surgical planning for the patient, such as the surgical approach and number of decompression levels, was determined by the lead doctor. All patients underwent internal fixation and fusion at the same time as decompression. In addition to the surgical plan, all patients received appropriate medical support according to the 2002 American Association of Neurological Surgeons cervical SCI guidelines [9, 10]. Other appropriate medical treatments of assistive drugs such as methylprednisolone were used in strict accordance with the recommendations of the NASCIS-2 [11], with routine fluid and diet intake limitations after surgery. Patients underwent a postoperative review of cervical CT images to identify whether the internal fixation, spinal canal decompression and fracture reduction were satisfactory. If neurological function was found to deteriorate after surgery, MRI examinations were used to assess the state of the spinal cord to remove potential or continued pressure.
The patients were assessed by the AIS and Injury Severity Score within 12 h after admission, which recorded the patient’s gender, age, cause of injury, level of lesion and Charlson Comorbidity Index. The patient’s type of injury determined by the AOSpine SCSCICS was independently judged by two senior doctors who were familiar with the classification system, and consensus was achieved after discrepancies were resolved through discussions between the doctors. After surgery, patients were analyzed in groups according to the timing of their operative intervention. Each group was divided into an A0, A1-4, B, C/F4 or F1-3 subgroup according to the AOSpine SCSCICS. In the literature, a type A0 injury means no bony injury or a minor injury such as an isolated lamina or spinous process fracture associated with CSCI [6], so we divided type A fractures into two independent subgroups: type A0 and types A1-4. Type F4 was introduced with a low reliability (K = 0.06) [6], and we found that it was difficult to distinguish between type F4 and type C due to similarities between clinical and radiographic findings as well as the severity of injury and causes of injury. Therefore, two cases with F4 fractures were combined with the C subgroup, with types F1-3 as a separate subgroup. The primary outcomes were ordinal changes in the AIS and the Spinal Cord Independence Measure III (SCIM version 3) at a 12-month follow-up [12]. The secondary outcomes included length of hospital stay, postoperative neurological deterioration, other complications and mortality. AIS and SCIM version 3 scores were evaluated and recorded at a 12-month follow-up by an independent research assistant, blinded to the timing of patients’ surgical treatment. The data from patients who did not complete the follow-up due to attrition and death were not included in the analysis.
Student’s t tests were used for statistical analysis of continuous variables. Mean values are presented as the mean ± SD. For quantitative data, the Chi-square test was used. A significance level was set a = 0.05. All statistical analyses were performed using Statistical Product and Service Solutions Version 18.0 (SPSS, Inc., Chicago, IL, USA).
Results
Study population
From February 2015 to October 2016, the study center received a total of 473 patients with traumatic CSCIs, and ultimately only 402 were included in the study after the screening, with an average age of 46.8 ± 15.3 years and 281 males (69.9%). Of these patients, 187 underwent surgical decompression treatment within 72 h after their injury and were included in the early group; this group had a mean age of 45.4 ± 14.9 years and included 135 males (72.2%). Two hundred and fifteen patients underwent the delayed decompression surgery and were included in the late group, which had a mean age of 47.7 ± 15.6 years and included 146 males (67.9%). There were no significant differences in sex, age, causes of injury, level of lesion, surgical approach, Charlson Comorbidity Index, severity of injury, incidence of complete SCI, ratio of methylprednisolone received or AIS grade at admission between the early and late groups. Details are shown in Table 1. All patients were followed up with 12 months after discharge; five patients died, and nine patients were lost in the early group, leaving 173 patients with complete data. There were two cases of death and two cases lost to follow-up in the late group, leaving 211 patients who completed the study. Patient flow is shown in Fig. 1. A total of 140 (34.8%) of the patients enrolled in the study were treated with methylprednisolone before admission or upon admission. There was no significant difference in the rate of hormone therapy between two groups (P = 0.546).

Patient flow
The corresponding AOSpine type of injury was judged based on CT and MRI, and then, patients were divided into A0, A1-4, B, C/F4 or F1-3 groups, for a total of five subgroups. As shown in Table 2, the early group was divided as follows: A0 subgroup, 25 (14.5%); A1-4 subgroup, 37 (21.4%); B subgroup, 41 (23.7%); C/F4 subgroup, 60 (34.7%); and F1-3 subgroup, 16 (9.2%). The late group was divided as follows: A0 subgroup, 32 (15.2%); A1-4 subgroup, 45 (21.3%); B subgroup, 60 (28.4%); C/F4 subgroup, 53 (25.1%); and F1-3 subgroup, 21 (10.0%). There was no significant difference between the early and late groups, but some differences occurred between the C/F4 subgroups.
Neurological and functional recovery at 12 months
The neurological and functional recovery of patients was evaluated 12 months after surgery, and details of the AIS grade at admission and at follow-up in the early and late group are shown in Table 3; details of AIS grade improvements and functional recovery in each subgroup are shown in Table 4 and summarized in Fig. 2. One hundred patients in the early group and 76 patients in the late group showed an AIS improvement ≥ 1 grade (P < 0.0001 for the combined groups; A0: P = 0.554; A1-4: P = 0.084; B: P = 0.013; C/F4: P = 0.040; and F1-3: P = 0.742); the early group showed obvious AIS improvements, and the B and C/F4 subgroup results support this finding, while there were no significant differences in the A0, A1-4 or F1-3 subgroups. Thirty-one patients in the early group and 17 patients in the late group showed an AIS improvement ≥ 2 grades, (P = 0.003 for the combined groups). The results of SCIM version 3 also showed that the early group had better functional recovery, and the B subgroup results support this finding, while there were no statistically significant differences in the A0, A1-4, C/F4 or F1-3 subgroups (early vs. late: P < 0.0001, for the combined groups; A0: P = 0.126; A1-4: P = 0.912; B: P = 0.006; C/F4: P = 0.111; F1-3: P = 0.875).

AIS grade improvements at 12 months by subgroup: early versus late surgery
Length of stay and postoperative neurological deterioration
As shown in Table 5, it was clear that the length of stay in the late group was longer than that of the early group (P < 0.0001), and the results from each subgroup were consistent with that of the previous comparison. Neurological function deteriorated after the operation in eight patients (4.6%) in the early group and three (1.4%) in the late group. There was no significant difference between the two groups. No significant differences were found in subgroups.
Postoperative complications and mortality
The detailed complications in the early and late groups are shown in Tables 5 and 6; 56 (32.4%) patients in the early group and 97 (43.6%) patients in the late group showed one or more severe or minor complication. The late group showed more complications than the early group (P = 0.007). However, it is surprising that we did not find any differences in the incidence of complications between the early and late surgery in the five subgroups. In the early group, five patients (2.8%) died, three of whom died in the ICU due to adverse events such as respiratory failure and multiple organ failure and two of whom died from bed-related complications after discharge. In the late group, one (0.4%) patient died in the ICU due to respiratory failure and one patient died due to thrombosis, pneumonia and other related complications after discharge. Although the mortality in the early group was higher than that of the late group, there was no significant difference between groups (P = 0.157), and there were no significant differences among the subgroups (P > 0.05). The results from the B and C/F4 subgroups were consistent with the former finding, but in the A0, A1-4 and F1-3 subgroups, the mortality of the early group was not different from that of the late group.
Multivariate analysis
Considering age, AIS grade at admission, injury severity score, complete cervical spinal cord injury and received methylprednisolone therapy were the five major confounding factors in this study. Finally, multivariate analysis was used to determine the degree of influence of confounding factors on the results and to determine the credibility of the study results. Multivariate analysis showed that ISS (Injury severity score) was identified as a definite confounding factor can affect neurological recovery outcome of AIS improvement =2 grade (Online Resource 1) (P = 0.027), it means the ISS in late group, relative to that of in early group, every increased by one point, the probability of AIS improvement =2 grade will decrease by 9.7%, but it does not show a significant effect on AIS improvement =1 grade (P = 0.083).
Discussion
Traumatic CSCI can cause serious consequences or even be life-threatening. It is estimated that approximately 2.5 people per million suffer from a traumatic CSCI every year worldwide [13], while the surgical treatment can relieve spinal cord compression and restore cervical stability to avoid the long-term compression caused by a direct injury and the resulting secondary injury; however, the optimal timing of surgery is still controversial. Furlan et al. [14] study the timing of the surgical treatment of acute SCIs through an evidence-based medicine method, and animal experiments results showed that a timely decompression surgery after a SCI can effectively promote postoperative neurological function recovery. Fehlings et al. [2] conducted a multicenter, prospective cohort study and showed that for patients with an acute CSCI, surgery within 24 h was proven to be safe and effective and led to better neurological function recovery. A multicenter retrospective study by Liu et al. [15] divided patients with an acute CSCI into two groups based on a dividing line of 72 h after injury: an early surgery group and delayed operation group. Follow-up assessments showed that the patients in the early group had shorter hospital stays. However, there were no significant differences in ICU hospital stay, auxiliary ventilation time or complication rate (pneumonia, pulmonary embolism, wound infection, sepsis and urinary tract infection) between the early group and the delayed group, and the early group had a higher incidence of neurological deterioration and mortality, which demonstrated that surgery within 72 h after injury is safer and more effective. In 2004, a meta-analysis of results showed that operations < 24 h after SCI can lead to better clinical results than surgery ≥ 24 h after injury or conservative treatment [16]. In 2010, Fehlings et al. [17] conducted a systematic analysis of the literature and performed a prospective investigation that found that most spine surgeons tend to perform surgery within 24 h after an injury in patients with a complete or incomplete CSCI. Recent studies tend to define the early surgery as operations within 24 h after injury and suggest performing surgical treatment as early as possible [18]. The reason this study adopted a 72-h cutoff is because the research center is the largest in Western China and has the highest level of emergency traumas, and the tertiary nature of referral patterns require that patients must first receive treatment in a primary medical institution before being transferred to the larger center if the primary medical institution does not have the ability or conditions to treat the patient; thus, the majority of patient arrivals at this health center are more than 24 h after a CSCI.
A recent systematic review showed that most studies currently support the idea that the early surgical decompression leads to better neurological recovery results [18]. However, whether all types of lower CSCIs should be prioritized for the early decompression surgery has not been studied. Hence, we used the AOSpine SCSCICS to focus on this problem. This system can allow for the comprehensive evaluation of all cases with a high degree of credibility and repeatability and is easy to use clinically. However, the interobserver reliability of the F4-type fractures described in a previous paper was poor (k < 0.2), which is possibly explained by the fact that we found type F4 was easy mistaken as type C due to similarities in clinical and radiographic findings as well as the severity of injury and causes of injury. Therefore, we integrated type F4 and type C into one subgroup.
Our research showed that the early surgery led to better neurological and functional recovery, which is in accordance with the conclusions of most of the literature about the optimal timing for CSCI surgeries [1,2,3,4]. However, there were no differences in neurological and functional recovery from type A or F1-3 fractures between the early and late groups. Based on our experience, the reason for this finding may be that a component of the A0 and F1-3 fractures’ mechanism of injury is mainly a transient cervical dislocation caused by a whiplash injury in a sagittal plane or a transient, excessive lateral flexion in the coronal plane that thereby results in a slight contusion of the cervical spinal cord, unlike type B, C or F4 fractures, where there is sustained mechanical bone compression due to severe traumatic violence. A1-4 fractures except for A4 are all caused by a mild form of violence without severe mechanical compression of the spinal canal. Therefore, the spinal cord will not show further degeneration, necrosis or secondary injury. Type A4 injuries are burst fractures caused by relatively severe violence that sends fractured pieces into the vertebral canal and causes space-occupying compression, but the limited number of patients with type A4 fractures was not large enough to divide this type into an independent subgroup; this is also a limitation of this study. In addition, there was no significant difference between the early and late groups in terms of the functional recovery of patients with C/F4 fractures at a 12-month follow-up, but there is currently no definite explanation for this finding.
Our study also emphasized non-neurological outcomes relative to the timing of the surgical intervention. We reported that the length of hospital stay in the early group was significantly shorter than that of the late group, which may be due to earlier surgery and earlier activity in the early group. Moreover, all patients with a traumatic CSCI at the center are transferred to a professional rehabilitation institution for long-term recovery after completing the surgery. Therefore, the length of hospital stay in this study is generally short.
Liu et al. [15] retrospectively analyzed the clinical outcomes of 212 patients who underwent decompression within 72 h and 383 patients who underwent surgery after 72 h. The study found that the rate of neurological function deterioration in the early decompression group (6.6%) was significantly higher (0.7%) than that of the late decompression group. However, our research showed that the rate of postoperative neurological deterioration for the early surgery group was higher than that of the late surgical decompression group, but this difference was not statistically significant, which is contrary to the findings of Liu et al. Concerning complications, Liu et al. indicated that complications in the early group were significantly lower than those in the late group, and in this, Liu’s findings are consistent with our results. Samule et al. [19] identified that the timing of surgery was a risk factor for minor complications, and the later the surgery, the higher the risk of the occurrence of minor complications; as shown in Table 6, most of the complications in this study were minor complications, so the results of our study were supported by the research conclusions of Samule et al. However, this difference did not occur in each subgroup, which may be because the subgroups were divided too much and the significant difference was diluted.
Mortality is another risk factor that must be taken into account in the selection of surgery options for traumatic CSCIs. Croce et al. [20] found that patients with an injury severity score greater than 25 points had higher mortality following an early surgery than a late surgery. Samule et al. [19] identified the timing of the intervention and the Charlson Comorbidity Index as two risk factors for mortality. With a delay in surgery, the risk of death was significantly reduced, demonstrating that the late surgery was safer than the early surgery. However, our research showed no significant difference despite the mortality of early surgery being higher than that of the late surgery.
After a multivariate analysis, only ISS was identified as a confounding factor in our study. The higher the patient’s ISS, the less possibility of neurological recovery. The ISS of subgroups B and C/F4 was generally higher; due to this confounding factor, the number of patients in the late group that obtained a neurological recovery = 2 grade may be lesser compared with patients in the early decompression group, resulting in false-positive results. However, it failed to show a significant influence on number of patients in the late group that obtained a neurological recovery = 1 grade. Overall, the confounding factor did not significantly affect the credibility of the results of this study.
There are some limitations in this study. Subgroup analyses may dilute the significant differences between the early and late cohorts, which may add some bias to the findings. Confounding factor ISS has a potential that results in false-positive results. Additionally, surgeries were performed by different surgeons. Variations in patient management and evaluation may have led to the observed differences in results. Despite these limitations, this large sample research provides clear guidance on the timing of surgery for different types of AOSpine subaxial cervical fractures.
Conclusion
The early surgery for type A and type F1-3 fractures defined by the AOSpine system failed to show the significant clinical advantages and is not required to undergo aggressive early decompression surgery. Type B and type C/F4 fractures should be surgically treated early for better clinical outcomes.
References
Newton D, England M, Doll H, Gardner BP (2011) The case for early treatment of dislocations of the cervical spine with cord involvement sustained playing rugby. J Bone Joint Surg Br 93:1646–1652. https://doi.org/10.1302/0301-620x.93b12.27048
Fehlings MG, Vaccaro A, Wilson JR, Singh A, Cadotte DW, Harrop JS, Aarabi B, Shaffrey C, Dvorak M, Fisher C, Arnold P, Massicotte EM, Lewis S, Rampersaud R (2012) Early versus delayed decompression for traumatic cervical spinal cord injury: results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PLoS ONE 7:e32037. https://doi.org/10.1371/journal.pone.0032037
Wilson JR, Singh A, Craven C, Verrier MC, Drew B, Ahn H, Ford M, Fehlings MG (2012) Early versus late surgery for traumatic spinal cord injury: the results of a prospective Canadian cohort study. Spinal Cord 50:840–843. https://doi.org/10.1038/sc.2012.59
Stevens EA, Marsh R, Wilson JA, Sweasey TA, Branch CL Jr, Powers AK (2010) A review of surgical intervention in the setting of traumatic central cord syndrome. Spine J 10:874–880. https://doi.org/10.1016/j.spinee.2010.07.388
Urrutia J, Zamora T, Campos M, Yurac R, Palma J, Mobarec S, Prada C (2016) A comparative agreement evaluation of two subaxial cervical spine injury classification systems: the AOSpine and the Allen and Ferguson schemes. Eur Spine J 25:2185–2192. https://doi.org/10.1007/s00586-016-4498-0
Vaccaro AR, Koerner JD, Radcliff KE, Oner FC, Reinhold M, Schnake KJ, Kandziora F, Fehlings MG, Dvorak MF, Aarabi B, Rajasekaran S, Schroeder GD, Kepler CK, Vialle LR (2016) AOSpine subaxial cervical spine injury classification system. Eur Spine J 25:2173–2184. https://doi.org/10.1007/s00586-015-3831-3
Silva OT, Sabba MF, Lira HI, Ghizoni E, Tedeschi H, Patel AA, Joaquim AF (2016) Evaluation of the reliability and validity of the newer AOSpine subaxial cervical injury classification (C-3 to C-7). J Neurosurg Spine 25:303–308. https://doi.org/10.3171/2016.2.spine151039
Urrutia J, Zamora T, Yurac R, Campos M, Palma J, Mobarec S, Prada C (2017) An independent inter- and intraobserver agreement evaluation of the AOSpine subaxial cervical spine injury classification system. Spine 42:298–303. https://doi.org/10.1097/brs.0000000000001302
Hadley MN, Walters BC, Grabb PA, Oyesiku NM, Przybylski GJ, Resnick DK, Ryken TC (2002) Management of combination fractures of the atlas and axis in adults. Neurosurgery 50:S140–S147. https://doi.org/10.1097/00006123-200203001-00022
Chappell ET (2002) Pharmacological therapy after acute cervical spinal cord injury. Neurosurgery 51:855
Bracken MB, Shepard MJ, Collins WF, Holford TR, Young W, Baskin DS, Eisenberg HM, Flamm E, Leo-Summers L, Maroon J et al (1990) A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury: results of the second national acute spinal cord injury study. N Engl J Med 322:1405–1411. https://doi.org/10.1056/nejm199005173222001
Ackerman P, Morrison SA, McDowell S, Vazquez L (2010) Using the spinal cord independence measure III to measure functional recovery in a post-acute spinal cord injury program. Spinal Cord 48:380–387. https://doi.org/10.1038/sc.2009.140
Wyndaele M, Wyndaele JJ (2006) Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 44:523–529. https://doi.org/10.1038/sj.sc.3101893
Furlan JC, Noonan V, Cadotte DW, Fehlings MG (2011) Timing of decompressive surgery of spinal cord after traumatic spinal cord injury: an evidence-based examination of pre-clinical and clinical studies. J Neurotrauma 28:1371–1399. https://doi.org/10.1089/neu.2009.1147
Liu Y, Shi CG, Wang XW, Chen HJ, Wang C, Cao P, Gao R, Ren XJ, Luo ZJ, Wang B, Xu JG, Tian JW, Yuan W (2015) Timing of surgical decompression for traumatic cervical spinal cord injury. Int Orthop 39:2457–2463. https://doi.org/10.1007/s00264-014-2652-z
La Rosa G, Conti A, Cardali S, Cacciola F, Tomasello F (2004) Does early decompression improve neurological outcome of spinal cord injured patients? Appraisal of the literature using a meta-analytical approach. Spinal Cord 42:503–512. https://doi.org/10.1038/sj.sc.3101627
Fehlings MG, Rabin D, Sears W, Cadotte DW, Aarabi B (2010) Current practice in the timing of surgical intervention in spinal cord injury. Spine 35:S166–S173. https://doi.org/10.1097/BRS.0b013e3181f386f6
Nakashima H, Nagoshi N, Fehlings MG (2015) Timing of surgery in the setting of acute spinal cord injury. Curr Surg Rep 3:1–9
Samuel AM, Grant RA, Bohl DD, Basques BA, Webb ML, Lukasiewicz AM, Diaz-Collado PJ, Grauer JN (2015) Delayed surgery after acute traumatic central cord syndrome is associated with reduced mortality. Spine 40:349–356. https://doi.org/10.1097/brs.0000000000000756
Croce MA, Bee TK, Pritchard E, Miller PR, Fabian TC (2001) Does optimal timing for spine fracture fixation exist? Ann Surg 233:851–858
Funding
No funds were received in support of this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Yong Fan and Jin‑Peng Du are both considered to be the first authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Du, JP., Fan, Y., Zhang, JN. et al. Early versus delayed decompression for traumatic cervical spinal cord injury: application of the AOSpine subaxial cervical spinal injury classification system to guide surgical timing. Eur Spine J 28, 1855–1863 (2019). https://doi.org/10.1007/s00586-019-05959-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-019-05959-6