
Abstract
Objective
Non-steroidal anti-inflammatory drugs have been shown to effectively decrease postoperative pain and reduce opioid requirements. Flurbiprofen axetil is an injectable non-selective cyclooxygenase inhibitor that has a high affinity for inflammatory tissues to achieve targeted drug therapy and prolonged duration of action. This meta-analysis examined the use of preoperative flurbiprofen axetil and its impact on postoperative analgesia.
Methods
An electronic literature search of the Library of PubMed, Cochrane CENTRAL, and EMBASE databases was conducted in Feb 2016. Searches were limited to randomized controlled trials. The primary outcome was pain scores. The secondary outcomes included cumulative postoperative opioid consumption and opioid-related adverse effects.
Results
A total of nine RCT studies involving 457 patients were included in this study. Compared to patients without perioperative flurbiprofen axetil, patients treated with preoperative flurbiprofen axetil had lower pain scores at 2 h (SMD −1.00; 95% CI −1.57 to −0.43, P = 0.0006), 6 h (SMD −1.22; 95% CI −2.01 to −0.43; P = 0.002), 12 h (SMD −1.19; 95% CI −2.10 to −0.28; P = 0.01), and 24 h (SMD −0.79; 95% CI −1.31 to −0.27; P = 0.003) following surgery. Preoperative flurbiprofen axetil had no significant effect on postoperative opioid consumption (SMD −13.11; 95% CI −34.56 to 8.33; P = 0.23). There was no significant difference between the groups with regard to adverse effects. Compared to patients with postoperative flurbiprofen axetil, however, preoperative flurbiprofen axetil resulted in decreased pain score only at 2 h after operation.
Conclusions
Preoperative use of flurbiprofen axetil will result in significantly lower postoperative pain scores, but no difference in nausea, vomiting, and opioid consumption compared to those who did not receive flurbiprofen axetil. However, more homogeneous and well-designed clinical studies are necessary to determine whether preoperative flurbiprofen axetil administration has more efficacy than that given at the end of surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Preemptive analgesia is an analgesic intervention initiated before a surgical procedure in order to prevent sensitization of the nervous system to subsequent stimuli that could amplify pain. A large number of experimental studies have suggested that pre-administration of local anesthetic and/or analgesic drugs prevents hyperplasticity of the central nervous system and thereby reduces postoperative pain [1, 2]. Based on the concept of preemptive analgesia, several clinical investigations were conducted to observe the analgesic effect of analgesics applied preoperatively, including non-steroidal anti-inflammatory drugs, opioid analgesics, clonidine, and neuromodulatory agents [3,4,5,6]. Despite the convincing evidence from experimental studies, however, results of clinical investigations regarding the value of preemptive analgesia are controversial.
Flurbiprofen axetil is an injectable non-selective cyclooxygenase inhibitor that formulated in emulsified lipid microspheres [7]. It has a high affinity for inflammatory tissues to achieve targeted drug therapy and prolonged duration of action [8]. It causes analgesia effect through decreasing the biological production of prostaglandins, reducing the reactivity of peripheral nerves to endogenous inflammatory factors, and inhibiting the sensitization of central as well as peripheral nervous systems [9, 10]. Flurbiprofen axetil has been used perioperatively, in conjunction with opioid analgesics, as part of a multimodal pain treatment.
There have been a number of randomized controlled trials (RCTs) evaluating the efficacy of flurbiprofen axetil on postoperative pain relief, but the results of preemptive analgesia effect of flurbiprofen axetil remain inconclusive [11]. We thus undertook this meta-analysis to investigate the use of preoperative flurbiprofen axetil and its impact on postoperative pain relief among all relevant randomized controlled studies to date.
Methods
Evidence acquisition
A prospective protocol of objective, literature-search strategies, inclusion and exclusion criteria, outcome measurements, and methods of statistical analysis was conducted according to the Cochrane Handbook.
Literature search strategy
All available randomized controlled trials (RCTs) about preemptive analgesia for postoperative pain relief were searched in PubMed, EMBASE, and CENTRAL. A broad search with restriction to publications in English was undertaken with all variants of terms. “Preemptive analgesia”, “postoperative pain”, “preventive analgesia”, “preoperative analgesia”, “analgesia”, “flurbiprofen axetil”, and “flurbiprofen” were entered as major subject headings. The Related Articles function was also used. Reference lists of retrieved reports and reviews were searched for additional trials. Unpublished reports and abstracts were not considered. When multiple studies that described the same population were published, the most recent or complete study was used. The date of the last search was February 29, 2016. Two authors independently conducted a comprehensive literature search to identify relevant studies. All authors examined each title and abstract to exclude clearly irrelevant articles. At least two authors extracted data independently. Any disagreements were resolved by discussion between two reviewers, with a third reviewer available for arbitration if necessary. Articles meeting the inclusion criteria were scored independently by two authors for methodological validity using the four-item, seven-point modified Jadad scale [12]. Any discrepancies were resolved by discussion with a third author. The minimum score of an included trial was 3 and the maximum was 7.
Criteria for inclusion and exclusion
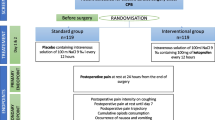
Articles that met the following criteria were included in this meta-analysis: (1) studies had been published; (2) they should be RCTs; (3) the intervention was preoperative flurbiprofen axetil in preemptive group; (4) the control groups were preoperative administration of normal saline/intralipid, or flurbiprofen axetil given at the end of surgery, respectively; (5) the manner and dosage of anesthesia were the same in the treatment and control groups; (6) at least one of the following outcomes were contained: pain scores, analgesic consumption, administration of rescue analgesics, time to first dose of analgesic, or the incidence of postoperative nausea and vomiting. Trials were included if they measured pain as either a primary or secondary outcome. We excluded trials when there was a lack of available data or experimental results. In addition, animal studies or reviews were not considered. Data from abstracts, letters to the editor, retrospective trials, and case reports were not included. Besides, studies scored less than 3 of the Jadad scale were not included in this meta-analysis [9, 13, 14].
Data extraction and analysis
Original data including general information (first author name, year of publication, country, and documents source), trial characteristics (surgery type, sample size, pain evaluation criteria, and the dosage of flurbiprofen axetil), participant-related data (participant age and weight) and all the experimental results were extracted, respectively. In trials which reported outcome as graphs, the means and standard deviations were estimated from these graphs. If data were not displayed numerically and could not be extracted from figures, then the study was not included. In papers using the median, range, or both as a measure of central tendency, the median, range, or both were converted to the mean, standard deviation, or both [15, 16]. Postoperative consumptions of tramadol, diclofenac, and buprenorphine were converted to morphine equivalents, respectively [17]. Pain intensity scores were assumed to be at rest unless otherwise noted. As to the incidence of adverse effect, we considered only the presence of the adverse effect, regardless of its severity.
Quality assessment and statistical analysis
Articles meeting the inclusion criteria were scored independently by two authors for methodological validity using the four-item, seven-point modified Jadad scale. The minimum score of an included trial was 3 and the maximum was 7. Research with the score more than 5 was regarded as a high-quality study.
All the meta-analyses were performed by Review Manager 5.3 (Cochrane collaboration, Oxford, UK). In this study, the odds ratio (OR), standardized mean difference (SMD) and the confounding 95% confidence interval (CIs) were calculated to assess the dichotomous variables and continuous variables, respectively. Heterogeneity was explored using I 2 statistic and statistic heterogeneity between studies was assessed using Chi-square test with significance set at P < 0.10. The random effects model was used if heterogeneity was existed. Otherwise, fixed effects model was used. Study results and estimates for analgesic effects were visualized by forest plot. P values less than 0.05 were considered to be statistically significant. When the data of the included studies could not be analyzed using software, the descriptively qualitative analysis was performed.
Statistical methods are available to assess the effects of unpublished studies on the results of meta-analysis (publication bias). This type of bias is assessed by studying the distribution of results on a funnel plot. The funnel plot is a scatterplot of the intervention effect of individual studies plotted against a measure of its precision or size. A funnel plot would normally be expected to symmetrical; however the absence of symmetry can suggest that some studies might not have been published because of their negative results. This asymmetry can also indicate the heterogeneity of results or the poor methodology in included studies [18, 19].
Results
Literature search
The systematic literature search identified 747 relevant publications. After reading the records, 687 non-relevant studies were excluded. After reading the full contexts, 60 studies were selected as potentially eligible for inclusion in this meta-analysis. Among the 60 studies, 46 were excluded for the following reasons: administration after surgery (n = 15); no outcomes suitable for analysis (n = 10); not RCTs (n = 7); administration orally (n = 9); unable to extract data (n = 5). Finally, we identified nine studies that met the including criteria after reading the full-text articles (Fig. 1). The publication year of studies ranged from 2000 to 2015. Five of the studies came from China, and the remaining four studies came from Japan. In total, 457 patients (229 patients in the flurbiprofen axetil group and 228 patients in the control group) were included. Among the nine included studies, seven evaluated the preemptive analgesia effect by comparing preemptive group (flurbiprofen axetil was given preoperatively) and control group (placebo or no treatment). The other two studies evaluated the preemptive analgesia effect by comparing preemptive group and conventional analgesia group (flurbiprofen axetil was given at some time point after initiation of the surgical procedure). VAS and postoperative analgesics consumption were used to evaluate postoperative pain. The administration dosage of flurbiprofen axetil was 50 mg per person or 1 mg/kg 15 or 30 min before surgery or at the end of the surgery (Table 1).

Flow diagram of literature search
Postoperative pain intensity
In this meta-analysis, pain scores were used as primary outcome to assess the postoperative pain. The following four figures showed the comparison between preemptive analgesia group and control group. Five studies [18,19,20,21,22] including 205 patients reported pain scores at 2 h after surgery. The random effects model was used because of significant heterogeneity (P = 0.007, I 2 = 71%) among the studies. The results indicated that there was a significant difference (P = 0.0006) between the preemptive analgesia group and the control group (Fig. 2). Four studies [17, 19,20,21] including 173 patients reported pain scores at 6 h after surgery. The random effects model was used because of significant heterogeneity (P = 0.001, I 2 = 82%) among the studies. The results indicated that there was significant difference (P = 0.002) between the preemptive analgesia group and the control group (Fig. 3). Five studies [18,19,20,21,22] reported pain scores at 12 h after surgery. The random effects model was used because of significant heterogeneity (P < 0.0001, I 2 = 88%) among the studies. The results indicated that there was significant difference (P = 0.01) between the preemptive analgesia group and the control group (Fig. 4). Seven studies [18,19,20,21,22,23,24] including 304 patients reported pain scores at 24 h after surgery. The random effects model was used because of significant heterogeneity (P = 0.0001, I 2 = 78%) among the studies. The results indicated that there was significant difference (P = 0.003) between preemptive analgesia group and control group (Fig. 5).

Forest plot showing the pain scores of 2-h postoperative between preemptive group and control group. Test for overall effect favors preemptive group (P = 0.0006). SMD standardized mean difference, 95% CI 95% confidence interval

Forest plot showing the pain scores of 6-h postoperative between preemptive group and control group. Test for overall effect favors preemptive group (P = 0.002). SMD standardized mean difference, 95% CI 95% confidence interval

Forest plot showing the pain scores of 12-h postoperative between preemptive group and control group. Test for overall effect favors preemptive group (P = 0.01). SMD standardized mean difference, 95% CI 95% confidence interval

Forest plot showing the pain scores of 24-h postoperative between preemptive group and control group. Test for overall effect favors preemptive group (P = 0.003). SMD standardized mean difference, 95% CI 95% confidence interval
Two studies [18, 25] reported the pain score comparisons between the preemptive analgesia group (flurbiprofen axetil was given preoperatively) and the conventional analgesia group (flurbiprofen axetil was given at the end of surgery). The fixed effects model was used because of no significant heterogeneity (P = 0.56, I 2 = 0%) between the studies. The pooled results indicated that there was significant difference (P = 0.02) between preemptive and conventional analgesia group at 2 h (P = 0.02, I 2 = 5%) after surgery while no reduction in pain scores was found at 6 h (P = 0.52), 12 h (P = 0.54) and 24 h (P = 0.92) after surgery (Fig. 6).

Forest plot showing the pain scores of 2, 6, 12, 24 h postoperative between preemptive group and routine group. Test for overall effect favors preemptive group at 2 h postoperative (P = 0.02). SMD standardized mean difference, 95% CI 95% confidence interval
Postoperative morphine consumption
Two studies [20, 21] reported morphine consumption. The random effects model was used because of significant heterogeneity (P < 0.00001, I 2 = 98%) among the studies. The results indicated that there was no significant difference (P = 0.23) between preemptive analgesia and the control group (Fig. 7).

Forest plot showing postoperative morphine consumption. Test for overall effect favors control group (P = 0.23). SMD standardized mean difference, 95% CI 95% confidence interval
Adverse incidence
Four studies [22,23,24, 26] reported adverse incidence. The fixed effects model was used because of no significant heterogeneity (P = 0.93, I 2 = 0%) among the studies. The results indicated that there was no significant difference (P = 0.83) between preemptive analgesia and control group (Fig. 8).

Forest plot showing postoperative adverse incidence. Test for overall effect favors control group (P = 0.83). SMD standardized mean difference, 95% CI 95% confidence interval
Publication bias
Figure 9 shows the funnel plot of the studies included. The bias funnel plot is not completely symmetrical, indicating that there may be some publication bias in this study.

Funnel plots illustrating the publication bias
Discussion
Preemptive analgesia has been investigated in two approaches [27, 28, 29]. One of them is to compare preoperative administration of analgesics with placebo or no treatment. Some of these studies have shown a reduction in pain intensity and/or analgesic use beyond the drug presence in the biophase. The other approach is to compare analgesic intervention made before surgery versus the same intervention made at some time point after initiation of the surgical procedure. In contrast to the first approach, however, many studies based on this approach state that the concept of preemptive analgesia is not clinically relevant.
This meta-analysis based on RCT studies including 457 patients showed the effectiveness of flurbiprofen axetil preoperative administration for postoperative pain relief. A total of seven studies analyzed the analgesic effect of preemptive flurbiprofen axetil group versus control group. The results showed a decrease of pain intensity within 24 h after surgery, and no significant differences were found in nausea and vomiting incidence. Only two studies that analyzed the preemptive effects of flurbiprofen axetil and conventional analgesia were included in this meta-analysis. Patients with preemptive flurbiprofen axetil administration showed lower pain scores only at 2 h after operation when compared to the patients with flurbiprofen axetil given at the end of surgery. In view of the short 2-h time and the lack of relevant research, we could not determine whether the 2-h validity is still within the range of analgesic pharmacokinetics of flurbiprofen axetil. Thus, the overall difference was small and may not be clinical relevant.
In a recent meta-analysis performed by Nir et al. [30], only two literatures were included to analyze the preemptive analgesia effect of flurbiprofen axetil. The authors did not analyze the pain scores changes during 24 h postoperatively. Our study included more investigations of flurbiprofen axetil on preemptive analgesia. In addition, we evaluated postoperative pain scores at 2, 6, 12, and 24 h after surgery. Furthermore, our meta-analysis conducted the comparison for the first time between preemptive analgesia in which flurbiprofen axetil given preoperatively and conventional analgesia in which flurbiprofen axetil was given at the end of the surgery. Similar to some studies [31], which proposed that the analgesic effect disappeared in a few hours and was insufficient for overnight pain relief, our meta-analysis showed that preoperative administration of flurbiprofen axetil provided about 2 h of analgesic effect compared with flurbiprofen axetil given after surgery.
Although the methodology was implemented strictly throughout the meta-analysis, it was hard to prevent the inherent limitations of the included studies. Thus, the results of our meta-analysis should be interpreted with much caution. First, the variability in the flurbiprofen axetil dose and timing, type of postoperative rescue analgesic, postoperative analgesia method, the type of surgery, and reported outcomes may have resulted in the high heterogeneity of continuous variables (pain scores, postoperative analgesic consumption). Although the random effects model was used to reduce the heterogeneity, it was still difficult to avoid the heterogeneity thoroughly. Besides, only nine studies were included in this meta-analysis, which makes it hard to conduct a subgroup analysis or sensitivity analysis. Second, data from some studies of high quality were reported as median or figures, which made the data extraction insufficient. We transformed median into mean and standard deviation according to the calculation method reported in the statistical literature, but the data obtained in this way can only approximately express the original data. Third, the volume and quality of the studies that were included in our meta-analysis are insufficient, and more well-designed studies will be needed for a comprehensive conclusion.
All studies included in this meta-analysis were double-blinded RCT designed to ensure the objectiveness and representativeness of the final results. Multiple strategies were applied strictly to minimize the heterogeneity. Using funnel plots, however, we demonstrated suspected publication bias for postoperative pain intensity, indicating that some studies of these outcomes with negative results were not published. Alternatively, this funnel plot asymmetry might also result from the great heterogeneity between studies.
Conclusions
This is the first meta-analysis with the focus on assessing the effectiveness and safety of flurbiprofen axetil for postoperative analgesia. The results suggest that flurbiprofen axetil administrated preoperatively was more efficacy for pain relief than placebo within 24 h after surgery, without increase the incidence of postoperative nausea and vomiting. However, flurbiprofen axetil administrated preoperatively only showed 2 h of superiority of analgesia than that given at the end of surgery. More homogeneous and well-designed clinical studies are necessary to determine the role of flurbiprofen axetil in perioperative pain management.
References
Woolf CJ, Chong MS. Preemptive analgesia-treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg. 1993;77:362–79.
Wall PD. The prevention of postoperative pain. Pain. 1988;33:289–90.
Penprase B, Brunetto E, Dahmani E, Forthoffer JJ, Kapoor S. The efficacy of preemptive analgesia for postoperative pain control: a systematic review of the literature. AORN J. 2015;101:94–105.
Yang L, Zhang J, Zhang Z, Zhang C, Zhao D, Li J. Preemptive analgesia effects of ketamine in patients undergoing surgery. A meta-analysis. Acta Cir Bras. 2014;29:819–25.
Kong Y, Yang X, Li X. The effect of parecoxib sodium for preemptive analgesia on nasal endoscopic surgery (in Chinese with English abstract). Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2015;29:1474–6.
Kilic E, Mizrak A, Goksu S, Cesur M. Preemptive analgesic efficacy of gabapentin and nimesulide in the functional endoscopic sinus surgery (in Turkish with English abstract). Agri. 2014;26:73–81.
Yamazaki Y, Sonoda H, Seki S. Effects of preoperatively administered flurbiprofen axetil on the action of inhaled anesthesia and postoperative pain (in Japanese with English abstract). Masui Jpn J Anesthesiol. 1995;44:1238–41.
Ohmukai O. Lipo-NSAID preparation. Adv Drug Deliv Dev. 1996;20:203–7.
Wang Y, Zhang HB, Xia B, Wang GM, Zhang MY. Preemptive analgesic effects of flurbiprofen axetil in patients undergoing radical resection of esophageal carcinoma via the left thoracic approach. Chin Med J (Engl). 2012;125:579–82.
Lin X, Zhang R, Xing J, Gao X, Chang P, Li W. Flurbiprofen axetil reduces postoperative sufentanil consumption and enhances postoperative analgesic effects in patients with colorectal cancer surgery. Int J Clin Exp Med. 2014;7:4887–96.
Nishiike S, Kato T, Nagai M, Nakagawa A, Konishi M, Sakata Y, Shimada F, Kida H, Ota M, Harada T. Preoperative flurbiprofen for pain prevention after tonsillectomy in adults. J Clin Anesth. 2007;19:596–600.
Zhang L, Zhu J, Xu L, Zhang X, Wang H, Luo Z, Zhao Y, Yu Y, Zhang Y, Shi H, Bao H. Efficacy and safety of flurbiprofen axetil in the prevention of pain on propofol injection: a systematic review and meta-analysis. Med Sci Monit. 2014;20:995–1002.
Liu ZF, Chai XQ, Chen KZ. Flurbiprofen axetil enhances analgesic effect of fentanyl associated with increase in beta-endorphin levels. J Anesth. 2011;25:679–84.
Zhou M, Li B, Kong M. Effects of flurbiprofen axetil on postoperative analgesia and cytokines in peripheral blood of thoracotomy patients. Cell Biochem Biophys. 2015;72:429–32.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135–8.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13.
Bradley JP. A comparison of morphine and buprenorphine for analgesia after abdominal surgery. Anaesth Intensive Care. 1984;12:303–10.
Sterne JA, Egger M, Smith GD. Systematic reviews in health care. Investigating and dealing with publication and other biases in meta-analysis. BMJ. 2001;323:101–5.
Sutton AJ, Higgins JP. Recent developments in meta-analysis. Stat Med. 2008;27:625–50.
Yamashita K, Fukusaki M, Ando Y, Fujinaga A, Tanabe T, Terao Y, Sumikawa K. Preoperative administration of intravenous flurbiprofen axetil reduces postoperative pain for spinal fusion surgery. J Anesth. 2006;20:92–5.
Takada M, Fukusaki M, Terao Y, Yamashita K, Inadomi C, Takada M, Sumikawa K. Preadministration of flurbiprofen suppresses prostaglandin production and postoperative pain in orthopedic patients undergoing tourniquet inflation. J Clin Anesth. 2007;19:97–100.
Takada M, Fukusaki M, Terao Y, Yamashita K, Takada M, Ando Y, Sumikawa K. Postoperative analgesic effect of preoperative intravenous flurbiprofen in arthroscopic rotator cuff repair. J Anesth. 2009;23:500–3.
Geng W, Hong W, Wang J, Dai Q, Mo Y, Shi K, Sun J, Qin J, Li M, Tang H. Flurbiprofen axetil enhances analgesic effects of sufentanil and attenuates postoperative emergence agitation and systemic proinflammation in patients undergoing tangential excision surgery. Mediat Inflamm. 2015;2015:601083.
Chen JQ, Wu Z, Wen LY, Miao JZ, Hu YM, Xue R. Preoperative and postoperative analgesic techniques in the treatment of patients undergoing transabdominal hysterectomy: a preliminary randomized trial. BMC Anesthesiol. 2015;15:70.
Shen JC, Sun HL, Zhang MQ, Liu XY, Wang Z, Yang JJ. Flurbiprofen improves dysfunction of T-lymphocyte subsets and natural killer cells in cancer patients receiving post-operative morphine analgesia. Int J Clin Pharmacol Ther. 2014;52:669–75.
Xu Y, Tan Z, Chen J, Lou F, Chen W. Intravenous flurbiprofen axetil accelerates restoration of bowel function after colorectal surgery. Can J Anaesth. 2008;55:414–22.
Zhang Z, Zhao H, Wang C, Han F, Wang G. Lack of preemptive analgesia by intravenous flurbiprofen in thyroid gland surgery: a randomized, double-blind and placebo-controlled clinical trial. Int J Med Sci. 2011;8:433–8.
Nakayama M, Ichinose H, Yamamoto S, Nakabayashi K, Satoh O, Namiki A. Perioperative intravenous flurbiprofen reduces postoperative pain after abdominal hysterectomy. Can J Anaesth. 2001;48:234–7.
Kissin I. Preemptive analgesia at the crossroad. Anesth Analg. 2005;100:754–6.
Nir RR, Nahman-Averbuch H, Moont R, Sprecher E, Yarnitsky D. Preoperative preemptive drug administration for acute postoperative pain: a systematic review and meta-analysis. Eur J Pain. 2016;20:1025–43.
Moiniche S. Pre-emptive analgesia. Br Med Bull. 2004;71:13–27.
Acknowledgements
This study was supported by Nature Science Foundation of Guangdong Province, China, Grant number 2015A030313781.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors have no conflicts of interests that are relevant to the content of this manuscript.
About this article

Cite this article
Wang, K., Luo, J., Zheng, L. et al. Preoperative flurbiprofen axetil administration for acute postoperative pain: a meta-analysis of randomized controlled trials. J Anesth 31, 852–860 (2017). https://doi.org/10.1007/s00540-017-2409-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-017-2409-0