
Abstract
Purpose
Bioreactance is a non-invasive technology for measuring stroke volume (SV) in the operating room and critical care setting. We evaluated how the NICOM® bioreactance device performed against the CardioQ® esophageal Doppler monitor in patients undergoing major abdominal–pelvic surgery, focusing on the effect of different hemodynamic interventions.
Methods
SVNICOM and SVODM were simultaneously measured intraoperatively, including before and after interventions including fluid challenge, vasopressor boluses, peritoneal gas insufflation/removal, and Trendelenburg/reverse Trendelenburg patient positioning.
Results
A total of 768 values were collected from 21 patients. Pre- and post-intervention measures were recorded on 155 occasions. Bland–Altman analysis revealed a bias of 8.6 ml and poor precision with wide limits of agreement (54 and −37 ml) and a percentage error of 50.6%. No improvement in precision was detected after taking into account repeated measurements for each patient (bias: 8 ml; limits of agreement: 74 and −59 ml). Concordance between changes in SVNICOM and SVODM before and after interventions was also poor: 78.7% (all measures), 82.4% (after vasopressor administration), and 74.3% (after fluid challenge). Using Doppler SV as the reference technique, the area under the receiver operating characteristic curve assessing the ability of the NICOM device to predict fluid responsiveness was 0.81 (0.7–0.9).
Conclusions
In patients undergoing major abdomino-pelvic surgery, SV values obtained by NICOM showed neither clinically or statistically acceptable agreement with those obtained by esophageal Doppler. Although, in the setting of this study, bioreactance technology cannot reliably replace esophageal Doppler monitoring, its accuracy for predicting fluid responsiveness was higher, up to approximately 80%.
Trial registration
Observational study.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Perioperative hemodynamic optimization improves postoperative outcomes following major surgery [1, 2]. Various strategies have been adopted including stroke volume (SV) optimization by fluid challenges, or targeting a minimum tissue oxygen delivery value using fluid ± inotropic support. Pulmonary artery catheterization has now been largely supplanted by a variety of minimally or non-invasive hemodynamic monitoring techniques [3], albeit with varying strengths of validation.
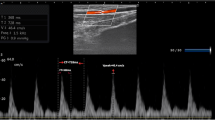
On the basis of its evidence base, esophageal Doppler flowmetry was the monitoring modality recommended for perioperative optimization by the National Institute for Health and Clinical Excellence (NICE) (https://www.nice.org.uk/guidance/mtg3). This technique measures the velocity of blood within the descending thoracic aorta using an esophageal probe sited at the level of the fifth to sixth thoracic vertebra emitting 4-MHz Doppler ultrasound. The area under the velocity–time waveform is the stroke distance, i.e., the distance a column of blood travels down the aorta with each left ventricular ejection. Using a formula incorporating the patient’s age, height, and weight, the descending aortic stroke distance can be translated into a reasonably accurate measure of left ventricular stroke volume [4, 5]. This technique has been validated in multiple studies [6]. Necessary assumptions are that fluctuations in blood pressure, body temperature, and cardiac output do not affect the ratio of upper-to-lower body blood flow [7].
The non-invasive cardiac output monitoring (NICOM) device utilizes bio-reactance. This technique is an evolution of bioimpedance and is based on the analysis of intra-beat variations in voltage phase shifts. It is totally non-invasive, requiring only the application of four electrodes onto the chest surface [8]. NICOM has been successfully used in adult and pediatric settings, especially as a tool for predicting fluid responsiveness [9, 10]. However, recent investigations in operating room or emergency settings comparing this device against different reference monitoring techniques, including esophageal Doppler, have produced conflicting results [11, 12]. The aim of this evaluation was to assess the validity and precision of stroke volume (SV) measurements using the bioreactance device (NICOM) compared against esophageal Doppler (ODM) during major elective abdomino-pelvic surgery. Particular emphasis was placed on the impact of specific interventions such as fluid challenge, vasopressor administration, peritoneal gas insufflation/removal, and Trendelenberg/reverse Trendelenberg positioning.
Methods
Patients and study design
The results presented in this paper were obtained as part of a service evaluation at University College London Hospitals, London, UK. The monitoring, interventions, and data collected were part of standard care. In addition, the analyzed data were fully anonymized and, as such, specific ethics committee permission was not required. Patients’ data were classified according to a sequential number without any medica reference code. During the study period (November 1, 2014 through January 31, 2015), all consecutive patients undergoing a major abdominal procedure (either laparoscopic or open) were considered eligible whenever intra-operative cardiac output (CO) and invasive arterial pressure monitoring were scheduled. Patients were enrolled if, in addition to standard cardiac output monitoring using esophageal Doppler (CardioQ, Deltex Medical, Chichester, UK), the attending consultant anesthetist decided to evaluate the NICOM (Cheetah Medical, Portland, Oregon, USA) as a completely non-invasive cardiac output monitoring tool. Subjects were excluded if they had any skin abnormalities or any relative contraindication to the use of esophageal Doppler monitoring (i.e., known or suspected esophageal ulcer, malformation, varicosities, or tumor). All patients underwent general anesthesia with propofol and fentanyl induction and desflurane in oxygen-enriched air for maintenance. The lungs were mechanically ventilated via an endotracheal tube at a tidal volume of 6–8 ml/kg ideal body weight. Normothermia was maintained using a whole-body convective warming blanket and a fluid warmer. Epidural analgesia and central venous pressure monitoring were performed where indicated. After surgery, patients were moved to either the recovery room or a high dependency area as clinically needed. The NICOM® system was calibrated before the induction of anesthesia. Four proprietary dual skin electrodes were placed over the left and right clavicles, and on the left and right lower thorax at the level of the diaphragm. Local body hair was shaved prior to placement, and the site cleaned with a 2% chlorhexidine sponge. A waterproof dressing was then applied over each dual electrode. One of the electrodes transmits a high frequency current across the body whereas the other connects to a voltage amplifier. Signals are applied to, and recorded from, both the left and right sides. The NICOM was calibrated to average stroke volume over 30 s. Electrodes were removed shortly after the end of surgery.
After the induction of anesthesia and tracheal intubation, the CardioQ esophageal Doppler device was set up. A probe was inserted into the esophagus to the mid-thoracic level, to a depth of approximately 35–40 cm from the teeth (or 5 cm further if inserted nasally). The probe position was then adjusted using visual and audible cues to obtain the highest Doppler frequency shift signal from blood flow in the thoracic descending aorta. The probe position was re-adjusted if signal quality deteriorated. Simultaneous snapshots of stroke volume were obtained from both devices every 5–15 min. Other collected data included cardiac output/index, mean arterial pressure, central venous pressure (when available), heart rate, and peak blood flow velocity and flow time corrected for heart rate (esophageal Doppler only). Two investigators (GDP, DB) evaluated the obtained waveforms and discarded any appearing as poor quality or artefactual. Patient hemodynamic status was recorded prior to and each minute after an intervention until the maximum effect was observed. Interventions included fluid challenges with either colloid or crystalloid (250–500 ml over 10 min), which were repeated if the patient was fluid responsive and still in need of further fluid, vasopressor administration for hypotension (metaraminol 0.5–1 mg bolus followed by norepinephrine infusion 0.5 mcg/kg/min or higher, if the patient was not responsive), peritoneal gas insufflation/removal (for laparoscopic procedures), and Trendelenburg/reverse Trendelenburg positions (robotic surgery and laparoscopic procedures).
Data analysis
The Kolmogorov–Smirnov test was used to evaluate variable distribution. Data with a non-normal distribution were assessed with the Mann–Whitney test with median and 25th to 75th centile values reported. Normally distributed data were assessed with Student’s t test. Categorical variables are presented as proportions. A p value below 0.05 was considered significant. Bland–Altman plots (mean stroke volume measurement from the two devices versus the difference in measurements between the devices) were used to calculate precision and bias. We determined a priori that a 30% error was acceptable, as recommended by Critchley and Critchley [13, 14]. The percentage error was calculated as 2SD divided by the mean of SVODM. Concordance was assessed by plotting the test ΔSVNICOM against the reference ΔSVODM on a four-quadrant scatter plot [15]. The concordance rate is the percentage of the number of data points lying in the upper right and the lower left quadrant of the scatter plot in relation to the total number of data points. Data at the center of the plot represent only small and random changes and hence were excluded from analysis (exclusion zone). Using recommendations recently proposed by Critchley et al., we applied an exclusion zone of 15%, with sufficient concordance to assume interchangeability >90% [15]. For testing the ability of the changes in SVNICOM induced by a fluid challenge to predict fluid responsiveness, we constructed receiver operating characteristics (ROC) curves. Sensitivity and specificity are expressed as median (95% confidence interval). Values considered inaccurate were discarded and not included in the analysis. MedCalc® Software (v. 12.2.1, MariaKerke, Belgium) was used for all statistical analyses. Graphing of data was undertaken using Prism version 6.0 for Windows (GraphPad Software, San Diego, CA, USA).
Results
Patients
The devices were evaluated in 21 patients whose characteristics are described in Table 1. The mean age of the cohort was 65 ± 12 years and were predominantly male (15/21, 71.4%). Main comorbidities were chronic cardiovascular disease, chronic respiratory disease, diabetes, and obesity: 81% of the patients were classified as ASA (American Society of Anaesthesiologists) 2 or 3. Six patients underwent laparoscopic robotic procedures (five prostatectomies, one cystectomy) and 15 open complex major abdominal procedures. Mean ± SD intraoperative fluid balance was +1564 ± 949 ml. Half of the patients were admitted to ICU for post-operative care.
A total of 471 paired measures were obtained from the 21 patients. Eighty-seven measures were discarded, as they were deemed inaccurate by the investigators: unreliable waveforms for esophageal Doppler (n = 36) and electrical cautery interference for NICOM (n = 51). These inaccurate measures mainly occurred during the initial and final surgical phase. Thus, 384 paired measurements [median (min–max) per patient: 16 (6–34)] have been included in the analysis.
One hundred and fifty-five paired SV values were collected before and after a standard intervention that would likely induce a hemodynamic change—66 fluid challenges, 68 boluses or infusions of vasopressor, 11 laparoscopic gas insufflations/removals, and ten postural changes.
Comparison of absolute values of SVODM and SVNICOM
Considering all 384 paired measures, the bias between SVODM and SVNICOM was 8.6 ml with precision (limits of agreement) of 54.3 and −37.1 ml and a percentage error of 50.6% (Fig. 1). When analyzed with a Bland–Altman plot, taking into account repeated measurements for each patient, the bias between SVODM and SVNICOM was 7.5 ml, with wider limits of agreement (74 and −59 ml).

Bland–Altman analysis for stroke volume (SV) measurements by esophageal Doppler (ODM) and bioreactance (NICOM) for all paired data values (n = 384). LOA limits of agreement, PE percentage error
The Bland–Altman analysis showed similar results: in those patients with an epidural, the bias between SVODM and SVNICOM was 9.7 ± 20.9 ml with precision (limits of agreement) of 50.6 and −31.3 ml and a percentage error of 44.2%. In patients without an epidural, the bias between SVODM and SVNICOM was 9.7 ± 26.4 ml with precision (limits of agreement) of 58.9 and −44.6 ml and a percentage error of 59.7%.
Comparison of changes in SVODM and SVNICOM
The concordance proportion between changes in SVODM and SVNICOM induced by any type of intervention (n = 155) was 78.7%. Excluding changes <15%, the concordance rate was 73% (Fig. 2a). The concordance proportion between changes in SVODM and SVNICOM induced by bolus vasopressor administrations/infusion (n = 68) was 82.4%; excluding changes <15% the concordance proportion was 82.1% (Fig. 2b).

Concordance proportions between NICOM and esophageal Doppler. a Concordance proportion with and without an exclusion zone of 15% (any intervention type, n = 155). b Concordance proportion with and without an exclusion zone of 15% (bolus vasopressors administrations, n = 68). c Concordance proportion with and without an exclusion zone of 15% (fluid challenges, n = 66). SV stroke volume, ODM esophageal Doppler
The concordance proportion between changes in SVODM and SVNICOM induced by fluid challenge administration (n = 66) was 74.3%; excluding changes <15%, the concordance proportion was 68.6% (Fig. 2c).
Ability of NICOM® device to assess fluid responsiveness
After fluid challenge, an increase in SVNICOM >10% predicted fluid responsiveness with a sensitivity of 80% (56.3–94.3) and specificity of 82.6% (68.6–92.2). The area under the ROC assessing the ability of the NICOM device to predict fluid responsiveness was 0.81 (0.7–0.9) (Fig. 3).

ROC curve testing the ability of the NICOM device, using ODM as the reference method, to predict fluid responsiveness using the percentage change in SV (SVNICOM) induced by fluid challenges. DSV NICOM delta-SVNICOM, ODM esophageal Doppler
Discussion
In this cohort of patients undergoing elective abdomino-pelvic operations, SV values obtained by NICOM did not show acceptable agreement, either clinically or statistically, against those obtained simultaneously with esophageal Doppler. The ability of NICOM to detect changes in SV after standard interventions capable of inducing hemodynamic changes was also suboptimal. Its accuracy in predicting fluid responsiveness was higher, with a sensitivity of 80% and a specificity of 82.6%.
The NICOM device utilizes bioreactance technology that is based on voltage shifts occurring when alternating electrical currents, passing through the thorax, are affected by pulsatile blood flow [8]. As it is completely non-invasive, safe, and very simple to use, this device does appear attractive, especially for specialties such as pediatrics [16]. Its application has recently extended to adult patients in the emergency department and operating theatres, where more invasive, well-validated monitoring systems are widely used [17]. We used an esophageal Doppler as our reference method for SV measurement, as this is the standard device used perioperatively within University College Hospital. Esophageal Doppler is widely accepted as a reliable method for cardiac output monitoring in clinical practice and has been validated against thermodilution and other techniques in multiple studies [6]. It is easy to use and allows continuous hemodynamic monitoring by online analysis of the features of the descending aortic blood flow velocity waveform.
In this study, considering all paired measures from the entire cohort, the agreement between the two monitoring systems was poor, with an error percentage much higher than the accepted 30% cut-off. We also evaluated concordance between the two methods by using repeated measures, performing Bland–Altman analysis accounting for different repeated measurements for each patient. However, taking into account the presence of a proportional error, the disagreement between the monitoring devices did not decrease. Most of the clinical data supporting the accuracy of bioreactance in adults derives from intra- and post-operative cardiac surgery [9, 10, 18]. Recent studies comparing NICOM against esophageal Doppler flowmetry have generated conflicting results. Waldron et al. compared NICOM and CardioQ devices for guiding goal-directed fluid therapy (GDFT) during colorectal surgery: although agreement in assessing response to a fluid challenge was poor (60-66%), they found no difference in clinical outcomes [19]. On the other hand, Conway et al. also studied patients undergoing major open-abdominal surgery and reported a bias of −6.9 ml, wide limits of agreement (−22.9 to 36.8 ml) and a percentage error of 57%. Both devices delivered unacceptable measures during electrical diathermy [11]. In another intraoperative study, Huang et al. compared NICOM simultaneously against both suprasternal and esophageal Doppler techniques. They observed that the trending ability of NICOM was less reliable, and was significantly influenced during upper abdominal interventions (e.g., open retractor placement, laparoscopic insufflation, and head-down tilt) with unpredictable shifts in cardiac output >1 l/min/m [2, 20]. The observations made by Huang et al. are in line with our data where cautery interference was significant for both monitors (18.5% of all collected readings). In such conditions, NICOM latency, based on the minimum sample interval value of at least 30 s, resulted in slower changes in SV than esophageal Doppler.
Overall, we found suboptimal agreement (78.7%) between the two devices in tracking change in stroke volume. Exclusion of changes <15% did not improve upon this level of agreement. Specific non-fluid interventions (e.g., vasopressors or postural change) were separately associated with suboptimal agreement. The overall accuracy of the NICOM device to predict fluid responsiveness was better, at approximately 81%, with comparable sensitivity and specificity.
Reasons for this disparity include a possible influence of current flux pathways related to the position of the lower chest NICOM electrodes as the dermatome level was not precisely identified. Changes in geometry of the upper abdomen related to the interventions may also affect the bioreactance readings. The esophageal Doppler technique assumes a fixed descending aortic diameter during systole and proportionality maintained between upper and lower body blood flow. These assumptions may not hold true with the varied interventions given, though Huang et al. did report good correlation between suprasternal and esophageal Doppler techniques [20].
This evaluation has limitations. First, no ‘gold standard’ technique was used as a comparator. Traditionally, thermodilution cardiac output measured by invasive pulmonary artery catheterization has been used for comparison studies. However, this technique is far from perfect [21, 22] and is now very rarely used at our center. Second, we only included patients undergoing elective abdominal–pelvic procedures and our findings should not be directly extrapolated to other settings or to patients in intensive care. Third, we did not address the role of NICOM calibration shifts during specific phases of the surgical intervention as a potential determinant of the suboptimal concordance with esophageal Doppler. Fourth, we were not blinded to the therapeutic interventions. Furthermore, due to the design of the study, we were not able to specifically analyze the time-course of the patients’ hemodynamic status and the clinical impact of the observed measures. Finally, this was not a clinical trial where interventions would have been standardized; due to the observational nature of the investigation, a selection bias cannot be excluded. However, these devices were being evaluated in a real-world clinical setting and how they would be used if adopted into practice at our institution. To date, our population is the largest in which interventions other than fluid have been specifically used to compare the CardioQ and NICOM devices.
Conclusions
In patients undergoing major surgery under general anaesthesia, stroke volume values obtained by NICOM showed an unacceptably high percentage error compared to those obtained with esophageal Doppler. Although trending ability following varied interventions was suboptimal, the observed accuracy for predicting fluid responsiveness was higher, up to approximately 80%.
References
Shoemaker WC, Appel PL, Kram HB, Waxman K, Lee TS. Prospective trial of supranormal values of survivors as therapeutic goals in high-risk surgical patients. Chest. 1988;94:1176–86.
Boyd O, Grounds RM, Bennett ED. A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk surgical patients. JAMA. 1993;270:2699–707.
Saugel B, Cecconi M, Wagner JY, Reuter DA. Non-invasive continuous cardiac output monitoring in perioperative and intensive care medicine. Br J Anaesth. 2015;114:562–75.
Singer M. Oesophageal Doppler monitoring: should it be routine for high-risk surgical patients? Curr Opin Anaesthesiol. 2011;24:171–6.
Singer M. Oesophageal Doppler. Curr Opin Crit Care. 2009;15:244–8.
Dark PM, Singer M. The validity of trans-oesophageal Doppler ultrasonography as a measure of cardiac output in critically ill adults. Intensive Care Med. 2004;30:2060–6.
Tomlin PJ, Duck FA. Transoesophageal aortic velography in man. Can Anaesth Soc J. 1975;22:561–71.
Raval NY, Squara P, Cleman M, Yalamanchili K, Winklmaier M, Burkhoff D. Multicenter evaluation of noninvasive cardiac output measurement by bioreactance technique. J Clin Monit Comput. 2008;22:113–9.
Marqué S, Cariou A, Chiche JD, Squara P. Comparison between Flotrac-Vigileo and Bioreactance, a totally noninvasive method for cardiac output monitoring. Crit Care. 2009;13:R73.
Squara P, Rotcajg D, Denjean D, Estagnasie P, Brusset A. Comparison of monitoring performance of Bioreactance vs. pulse contour during lung recruitment manoeuvres. Crit Care. 2009;13:R125.
Conway DH, Hussain OA, Gall I. A comparison of noninvasive bioreactance with oesophageal Doppler estimation of stroke volume during open abdominal surgery: an observational study. Eur J Anaesthesiol. 2013;30:501–8.
Kupersztych-Hagege E, Teboul JL, Artigas A, Talbot A, Sabatier C, Richard C, Monnet X. Bioreactance is not reliable for estimating cardiac output and the effects of passive leg raising in critically ill patients. Br J Anaesth. 2013;111:961–6.
Critchley LA, Critchley JA. A meta-analysis of studies using bias and precision statistics to compare cardiac output measurement techniques. J Clin Monit Comput. 1999;15:85–91.
Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8:135–60.
Critchley LA, Lee A, Ho AM. A critical review of the ability of continuous cardiac output monitors to measure trends in cardiac output. Anesth Analg. 2010;111:1180–92.
Weisz DE, Jain A, McNamara PJ. EL-Khuffash A. Non-invasive cardiac output monitoring in neonates using bioreactance: a comparison with echocardiography. Neonatology. 2012;102:61–7.
Dunham CM, Chirichella TJ, Gruber BS, Ferrari JP, Martin JA, Luchs BA, Hileman BM, Merrell R. Emergency department noninvasive (NICOM) cardiac outputs are associated with trauma activation, patient injury severity and host conditions and mortality. J Trauma Acute Care Surg. 2012;73:479–85.
Cheung H, Dong Q, Dong R, Yu B. Correlation of cardiac output measured by non-invasive continuous cardiac output monitoring (NICOM) and thermodilution in patients undergoing off-pump coronary artery bypass surgery. J Anesth. 2015;29:416–20.
Waldron NH, Miller TE, Thacker JK, Manchester AK, White WD, Nardiello J, Elgasim MA, Moon RE, Gan TJ. A prospective comparison of a noninvasive cardiac output monitor versus esophageal Doppler monitor for goal-directed fluid therapy in colorectal surgery patients. Anesth Analg. 2014;118:966–75.
Huang L, Critchley LA, Zhang J. Major upper abdominal surgery alters the calibration of bioreactance cardiac output readings, the NICOM, when comparisons are made against suprasternal and oesophageal Doppler intraoperatively. Anesth Analg. 2015;121:936–45.
Cecconi M, De Backer D, Antonelli M, Beale R, Bakker J, Hofer C, Jaeschke R, Mebazaa A, Pinsky MR, Teboul JL, Vincent JL, Rhodes A. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40(12):1795–1815.
Cecconi M, Arulkumaran N, Kilic J, Ebm C, Rhodes A. Update on hemodynamic monitoring and management in septic patients. Minerva Anestesiol. 2014;80:701–11.
Author information
Authors and Affiliations
Contributions
Dr. De Pascale takes responsibility for the content of the manuscript, including the data and analysis. Dr. De Pascale and Dr. Brealey contributed to conception and design, acquisition of data, or analysis and interpretation of data; drafted the submitted article, revised it critically for important intellectual content and provided final approval of the version to be published. Prof Singer contributed to the design of the study, critically revised the paper for important intellectual content and provided final approval of the version to be published.
Corresponding author
Ethics declarations
Funding
No funding was received from either Deltex (CardioQ manufacturer) or Cheetah (NICOM manufacturer) for this study. NICOM electrodes were provided free for this evaluation by Cheetah.
Conflict of interest
Mervyn Singer sits on an advisory board for Deltex; his academic fund at UCL receives an annual unrestricted donation from Deltex. UCL also hold shares in Deltex donated by the Pauline Thomas Charitable Trust. He was not involved in the collection of data for this study. The other authors declare no conflict of interests regarding this study.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors. The monitoring, interventions and data collected were part of standard care. In addition, the analyzed data were fully anonymized and, as such, specific ethics committee permission was not required.
Informed consent
For this type of study formal consent was not required.
About this article

Cite this article
De Pascale, G., Singer, M. & Brealey, D. Comparison of stroke volume measurement between non-invasive bioreactance and esophageal Doppler in patients undergoing major abdominal–pelvic surgery. J Anesth 31, 545–551 (2017). https://doi.org/10.1007/s00540-017-2351-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-017-2351-1