
Abstract
Purpose
The purpose of this study was to determine the effects of an 8-week HIIT intervention on patient-reported outcomes and physical function in breast cancer patients undergoing anthracycline-based chemotherapy.
Methods
Thirty breast cancer patients were recruited prior to initiating treatment and randomized into the HIIT group (n = 15) or control (CON) group (n = 15). The HIIT group attended HIIT sessions three days per week for eight weeks. The CON group was asked to maintain their current level of physical activity. Patient-reported outcomes were assessed by the Functional Assessment of Cancer Therapy-Breast Cancer (FACT-B), Multidimensional Fatigue Inventory with 20 questions (MFI-20), and the 15-item Five-Facet Mindfulness Questionnaire (FFMQ-15). Physical function was assessed using the timed up and go (TUG), 30-s sit-to-stand (30STS), Margaria-Kalamen stair climb test, and 6-min walk test (6MWT). Repeated measures ANCOVA and paired t-tests were performed to assess group differences.
Results
All patients completed the 8-week study with 82.3% adherence to the intervention among the HIIT group. Post-intervention, significant improvements were found for the Margaria-Kalamen stair climb test (− 3.39%; P = 0.013) and 6MWT (+ 11.6%; P = 0.008) in the HIIT group compared to baseline and CON group. No changes in patient-reported outcomes, TUG, and 30STS were observed following the 8-week study period in both groups (P > 0.05).
Conclusions
HIIT may be an effective strategy to improve physical function and possibly maintain QOL in breast cancer patients undergoing the anthracycline-based chemotherapy.
Clinical trial registration
ClinicalTrials.gov: NCT02454777
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Approximately 32% of breast cancer patients are treated with anthracycline-based chemotherapy [1]. However, anthracycline-based chemotherapy induces multiple dose-dependent toxicities, which result in skeletal muscle weakness [2], cancer-related fatigue [3], and declines in physical function [4]. Up to 80% of cancer patients experience cancer-related fatigue [5], and this number is even higher (91%) among those treated with anthracycline-based chemotherapy [6]. Decreased physical function is of particular concern because patients who experience persistent declines in physical function in the first two years of diagnosis have a shorter 10-year survival rate compared to the patients who do not experience reductions in physical function [7]. As declines in physical function contribute to a reduced QOL, it is important to explore an effective strategy that can improve physical function during treatment.
Current guidelines of the American College of Sports Medicine recommend cancer survivors to perform moderate-intensity aerobic exercise for a total of 150 min per week or vigorous intensity aerobic exercise for a total of 75 min per week [8, 9]. However, the American Cancer Society’s National Cancer Survivor Transition Study reported that 66.5% of cancer survivors do not achieve the recommended amount of physical activity [10]. High-intensity interval training (HIIT) is a recent, novel exercise strategy referred to as using bursts of concentrated effort alternated with recovery periods and has been utilized in a clinical setting. HIIT has been proven to be a safe and feasible method of exercise with evidence of improvements seen in physical fitness, health-related outcomes, and patient-reported outcomes (PROs), including QOL, in a wide range of chronic diseases [11]. HIIT induces greater benefits on QOL and physical function compared to moderate-intensity exercise in patients with myocardial infarction [12]. HIIT has also shown to be superior to resistance exercise and moderate-intensity, continuous aerobic exercise in improving physical function in healthy older adults [13]. Further, greater enjoyment following a HIIT intervention compared to a moderate-intensity intervention has been observed, which may improve QOL in breast cancer patients [14]. While HIIT has been proven to be beneficial in other clinical populations, research regarding HIIT training in cancer patients remains limited [11], with a lack of data investigating the effects of HIIT on QOL and physical function in breast cancer patients undergoing anthracycline-based chemotherapy.
The purpose of this study was to determine the effects of an 8-week HIIT intervention on PROs and physical function in breast cancer patients undergoing anthracycline-based chemotherapy. We hypothesized that an 8-week HIIT intervention improves PROs and physical function in breast cancer patients undergoing anthracycline-based chemotherapy compared to the control (CON) group who maintained their level of physical activity.
Methods
Experimental design
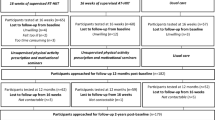
Details of the experimental design have been published previously [15]. Briefly, this study was a single-center, pilot randomized controlled trial with no formal sample size calculation. Ethical approval was obtained from the University of Southern California (USC) Institutional Review Board (HS-1500227), registered (ClinicalTrials.gov: NCT02454777; date of registration: May 27th, 2015), and written informed consent was obtained from participants. Participants were recruited from breast cancer clinics at the USC Norris Comprehensive Cancer Center (NCCC) and the Los Angeles County Medical Center via onsite recruitment by the principal investigator and medical oncologists. Screening for enrollment and the flow of participants both eligible and non-eligible have been published previously [16]. Participants were randomized in a 1:1 ratio of allocation (computer-generated, investigator-blinded randomization assignments) to the HIIT intervention group or the CON group by the Clinical Investigation Support Office at the NCCC and study investigators were blinded during randomization. Randomization was stratified by neoadjuvant versus adjuvant anthracyclines treatment.
Participants randomized to the HIIT group completed three supervised HIIT exercise sessions per week for the 8-week intervention period. The 8-week study duration was selected to mirror USC’s treatment duration of anthracyclines at the time of the study. Participants randomized to the CON group were asked to maintain their current level of physical activity, not exceeding 30 min of total structured exercise per week. Those within the CON group used self-reported logs, as a cost effective and reliable method. All participants returned within one week after the 8-week study period for post-testing. Outcome measures were obtained within 1–2 weeks before the first cycle of anthracyclines (week 0), and within seven days from their last exercise session in week eight. The CON group was then offered the exercise intervention after the 8-week control period. The trial reached completion after the last participant was recruited and completed testing.
Eligibility criteria
Participants were eligible if (1) women ≥ 18 years old diagnosed with a primary invasive (stage I–III) breast cancer; (2) planning to receive neoadjuvant or adjuvant anthracycline; (3) able to start an exercise program within 1–2 weeks of starting chemotherapy; (4) currently sedentary (< 30 min of physical activity per week); (5) refrained from smoking within the last 12 months; (6) willing to travel to exercise facility at USC, and (7) able to provide physician clearance for participation in the exercise program. The exclusion criteria included: (1) history of chronic disease including uncontrolled diabetes, uncontrolled hypertension, or uncontrolled thyroid disease; (2) weight reduction ≥ 10% within the past six months that may be indicative of an uncontrolled pre-existing condition; (3) metastatic disease; (4) any noticeable cardiovascular disease such as myocardial infarction, stroke, or angina; (5) contraindications to exercise, and (6) participation in regular exercise, over 30 min of exercise a week as screened by medical oncologist and principal investigator. These exclusion criteria were set forth to exclude patients who had uncontrolled pre-existing conditions and as a result may need further medical interventions. Patients with controlled comorbidities were eligible for the study.
Intervention
Participants assigned to the HIIT group received supervised exercise sessions performed on a stationary bike (Life Fitness 95 Elevation Series, Rosemont, IL, USA). Exercise intensity was individually prescribed for the HIIT group based on peak power output (PPO), which was measured by a VO2 max fitness testing performed on a stationary bike. Each exercise session consisted of a 5-min warm-up (10% PPO), followed by a 20-min HIIT protocol. The 20-min HIIT protocol consisted of seven bouts of 1-min high-intensity exercise (90% PPO) followed by two min of active recovery (10% PPO). Participants were encouraged to complete each exercise session with at least 24 h of rest between each session and to complete sessions on days when participants did not receive anthracycline infusions. Power output, heart rate, rating of perceived exertion (RPE; rated on the Borg scale of 6–20), and total minutes of exercise were documented for each session and for each interval. Participants were encouraged to make up any missed sessions in the same week or during the 8-week intervention period. Participants in the CON group were asked to maintain less than 30 min of total structured exercise per week during the 8-week study period. The CON group was asked to document their weekly physical activity in exercise logs.
Outcome measures
Outcome measures were assessed within one week of baseline testing and within one week of their last anthracycline infusion.
Quality of life
The Functional Assessment of Cancer Therapy-Breast Cancer (FACT-B) questionnaire was used to assess for multidimensional QOL [17]. The FACT-B includes 27 questions from the FACT-General (FACT-G), which measures physical well-being, social well-being, emotional well-being, and functional well-being, with an additional nine breast cancer specific questions [17]. Responses to questions from each subscale were scaled ranging from 0 (not at all) to 4 (very much), and the total FACT-B score was obtained from summing up the subscale scores [18]. The FACT-B total score ranged from 0 (low QOL) to 144 (high QOL), with higher scores representing better QOL.
Cancer-related fatigue
Cancer-related fatigue was assessed using the Multidimensional Fatigue Inventory (MFI-20). This is a self-reported 20-item tool to measure general, physical, and mental fatigue, as well as reduced motivation and reduced activity [19]. Participants were asked to rate statements on the MFI-20 range from a scale of 1 (yes, that is true) to 5 (no, that is not true). Intensity of fatigue was obtained by frequency distribution of responses to items with higher scores reflecting higher levels of fatigue.
Mindfulness
The 15-item Five-Facet Mindfulness Questionnaire (FFMQ-15) has been validated to measure mindfulness in clinical populations [20]. The five facets include observing, describing, acting with awareness, non-judging of inner experience, and non-reactivity to inner experience. Each question has a range from a scale of 1 (never or very rarely true) to 5 (very often or always true). Higher total scores represent higher levels of mindfulness and/or self-compassion.
Physical function
Physical function was assessed using the timed up and go (TUG), the 30-s sit-to-stand (30STS) test, the Margaria-Kalamen stair climb test, and the 6-min walk test (6MWT). All participants were asked to wear comfortable clothing and appropriate shoes for testing.
TUG was performed by having the participants start in a sitting position in a standard arm chair. Participants were instructed to stand up from the chair and walk to a line on the floor 3 m away [21]. Participants were asked to stand behind the start line, walk the designated 3-m distance when instructed, turn, and walk back to their chair, timing stopped as soon as they were seated. Participants were timed when told “ready, go,” until they returned to the seated position in the chair; a faster time indicates a better functional performance. Three trials were performed, and an average was calculated and recorded.
The 30STS was performed with a stable chair that was prevented from sliding backwards. Participants were instructed to sit in the middle of the chair, with their hands on the opposite shoulders, crossed at the wrists [22]. Participants were instructed to keep their feet flat on the floor and to keep their back straight, with arms against their chest. On “ready, go,” the participants were asked to rise to a full standing position and then sit back down, repeating this standing-sitting action as many times as possible in 30 s. The number of repetitions of full sit-to-stand motions completed in 30 s was recorded.
The 6MWT was performed to measure functional capacity associated with endurance levels [23]. The walking course was 30 m in length and the turnaround points were marked with orange-color cones to create a walking course. Participants were asked to walk as briskly as possible for 6 min on the course. Participants were allowed to slow down, to stop, and to rest as necessary. After six min, participants were asked to stop, and the distance each participant walked was measured in meters.
The Margaria-Kalamen stair climb test is a valid and reliable clinical test used to assess physical power and is associated with greater independence and lowered fall risk [24]. Participants were asked to ascend a flight of stairs as quickly as possible while timing how quickly each participant went from the third step to the ninth step. Each participant performed three trials and the fastest time was recorded to assess power. Power was calculated using a validated equation [25].
Statistical analyses
Baseline participant characteristics were summarized by descriptive statistics. Distribution of outcomes were evaluated and presented as mean (SD) for continuous outcomes and frequency (%) for categorical outcomes. Group comparisons of baseline participant characteristics were made using independent sample t-test or non-parametric corollary for continuous outcomes and χ2 test for categorical outcomes. Participant baseline characteristics that were different across groups were included as covariates in the statistical analyses. Given the small sample size (N = 30), baseline variables with a difference of P < 0.10 were considered as additional covariates after testing for collinearity. A repeated measures ANCOVA model was performed with treatment group and time (baseline/post-intervention) as factors. For within-group difference, the changes in the outcome measures from baseline to week nine were examined by a paired t-test, with a level of significance set at P < 0.05. Repeated measures ANCOVA on the trial outcomes was a two (group: HIIT, CON) × two (time: baseline, post-intervention) analysis. All analyses were performed with SPSS (v.22).
Results
We assessed 58 women for eligibility of which 30 were enrolled, consented, and randomized to the HIIT or CON groups. A complete CONSORT diagram of study flow has been published previously [16]. Participants were 46.9 ± 9.8 years old, Hispanic white (73%), and with a BMI 31.0 ± 7.5 kg/m2. Of note, while 73% of the patient population were Hispanic white, there were no differences seen among outcomes between Hispanic and non-Hispanic patients. Participants were diagnosed primarily with stage II (30%) or III (63%) breast cancer and largely treated with neoadjuvant chemotherapy (77%). Baseline characteristics have been published previously [15] and there were no significant differences between the two groups for any baseline characteristic (P > 0.05). There were no significant changes in BMI or weight. High attendance of 82.3% (overall average 19.2 of 24 sessions) was attained by the HIIT group without use of incentives for enrollment or attendance. Reports of attendance and completed session has been published previously [16]. No adverse events were reported over the duration of the intervention. Adverse events were identified at every exercise session and testing time point. Serious adverse events (events resulting in hospitalization) would have been reported within 24 h to research governance committees (Institutional Review Boards and Data and Safety Monitoring Committee).
Patient-reported outcomes (Table 1)
Post-intervention, there were no significant changes in PROs (P > 0.05) in the HIIT group; a statistical trend (P = 0.10) was observed for the physical well-being scale of the FACT-B following intervention. Physical (P = 0.04) and functional well-being (P = 0.05) subscale scores of the FACT-B and total FACT-B score (P = 0.01) significantly reduced following eight weeks in the CON group. However, no additional changes in PROs were observed in the CON group (P > 0.05).
Physical function (Table 2)
Post-intervention, significant improvements in the Margaria-Kalamen stair climb test (− 3.39%; P = 0.013) and 6MWT (+ 11.6%; P = 0.008) were observed in the HIIT group compared to the CON group. No significant changes were observed in the other functional measures following the 8-week intervention in the HIIT group (P > 0.05). Physical function did not change in the CON group (p > 0.05). There were no differences between groups for the baseline Maragaria-Kalamen stair climb test.
Discussion
A supervised 8-week HIIT intervention led to significant improvements in the Margaria-Kalamen stair climb test and 6MWT among breast cancer patients receiving anthracycline-based chemotherapy while maintaining QOL scores. This is the first study to our knowledge to report significant improvements in measures of physical function with HIIT in breast cancer patients receiving anthracycline-based chemotherapy.
To date, only one study has reported the effects of a HIIT intervention on PROs and physical function in breast cancer patients receiving chemotherapy. Mijwel et al. (2018) compared the effects of resistance and high-intensity interval training (RT-HIIT), and moderate-intensity aerobic and high-intensity interval training (AT-HIIT) to a usual care (UC) group in women with breast cancer (n = 240) undergoing chemotherapy. In brief, participants in both exercise groups experienced improvements in QOL, measured through the European Organization for Research and Treatment for Cancer Quality of Life Questionnaire (EORTC-QLQ-C30), maintenance of cancer-related fatigue (CRF), assessed through multidimensional Piper Fatigue Scale [26], and an increase in physical function measured by hand grip strength [27]. RT-HIIT counteracted several dimensions of CRF and was significantly superior compared to UC in total CRF, behavior/daily life CRF, and sensory/physical CRF. Both RT-HIIT and AT-HIIT exhibited beneficial effects for certain aspects of QOL. Role functioning significantly improved for RT-HIIT and AT-HIIT compared to UC. AT-HIIT significantly improved in emotional functioning versus UC [26], while grip strength only improved significantly in the RT-HIIT group for those receiving taxane treatment [27].
However, when compared to our study, the aforementioned study incorporated a longer duration of HIIT bouts, a longer intervention, different chemotherapy regimens, and different exercise modalities. These findings may suggest that longer exercise interventions may be necessary to observe significant changes in PROs. The effect of RT-HIIT on fatigue reported by Mijwel et al. may also suggest that higher intensity/load combined exercise training is needed to combat increases in fatigue and exercise intensity may offset QOL. Both HIIT interventions resulted in improvements in physical function; however, it should be noted the difference in testing, stair climb and 6MWT vs grip strength, and the difference in exercise prescription, HIIT vs RT-HIIT.
Similar findings were also reported by Courneya et al. (2007) who did not utilize HIIT training but compared aerobic exercise, resistance exercise, and usual care in breast cancer patients undergoing adjuvant chemotherapy. Courneya et al. found no significant improvements in cancer-specific QOL, assessed through FACT-anemia, in a multi-site, three-armed, supervised exercise intervention [28]. Secondary outcomes, however, such as physical fitness and chemotherapy completion rates improved [28]. A similar trend was seen with improvements in physical outcomes and only non-significant improvements in QOL, despite the longer study duration compared to our study (18 weeks vs 8 weeks, respectively). Though QOL did not significantly improve in this study, these results may emphasize findings by Mijwel et al. (2018) that to improve psychosocial outcomes in breast cancer patients undergoing chemotherapy, the use of combination resistance exercise and a high-intensity aerobic component should be considered.
Conversely, a recent meta-analysis of exercise during adjuvant radiotherapy in breast cancer patients reported positive improvements in fatigue and QOL from exercise [29]. Nine studies were examined, each study with varying modes of exercise (aerobic, resistance, combination) [29]. The main findings suggest that exercise during adjuvant radiotherapy can be beneficial to fatigue and QOL, with supervised, combined aerobic-resistance exercise showing the most promise when alleviating fatigue [29]. This could potentially explain why we did not see significant improvements in PROs, as both our research and previously mentioned studies did not include combination exercise modalities.
Although our study is a pilot study of a short duration, our findings are promising given that PROs did not worsen in the HIIT group as opposed to the CON group. Participants in the CON group experienced worsened PROs such as total FACT-B score (− 27.8%). Our results align with previous studies which reported that chemotherapy significantly reduced QOL (− 10 points) measured by EORTC within six months up to two years after chemotherapy [30, 31]. Further, our study adds evidence that reductions in QOL can be observed in as few as eight weeks from the initiation of chemotherapy.
Though research on HIIT in cancer populations is limited, there is promising evidence of beneficial impact on physical function and PROs. Our study of eight weeks of lower body interval training seemed to be long enough to elicit changes in cardiorespiratory fitness and functional power, reflected in the 6MWT and Margaria-Kalamen stair climb. We suspect that these two outcomes saw significant changes because these two activities mirror activities of daily living and the muscle groups associated with these outcome measures are more often used. Failure to see improvements in all physical testing measures and lack of significant improvements in PROs could be reflective of duration, intensity, and exercise type as evidence reflects superior benefit with the use of longer duration, longer training intensity, and combined resistance and/or aerobic exercise with HIIT on psychosocial and functional measures [26]. Another consideration for unchanging PROs with exercise could be a result of chemotherapy and/or anti-emetics causing drowsiness or steroids and other medicines causing poor sleep or pain. There is a possibility that exercise is not enough, even with varying intensities, to combat issues during active treatment.
Also of note, fatigue may be mitigated through HIIT or lower intensity exercises, and our findings do not conclude whether or not HIIT is better than lower intensity exercises in ameliorating chronic post-treatment fatigue. Incorporation of resistance exercise may have additional benefits specific to physical functioning and PROs when compared to HIIT or used in conjunction with HIIT [29]. This could be indicative of a need for higher load/intensity exercise in future study design to influence psychosocial outcomes to combat deleterious effects of chemotherapy.
Strengths of our study include a focus on a single chemotherapy regimen, utilization of an objective HIIT prescription using peak power output rather than a subjective measure such as ratings of perceived exertion, and inclusion of a diverse (mainly Hispanic) sample.
Study limitations
Limitations include a shorter study design, reflecting the duration of anthracycline, 8 weeks vs 12–16 weeks, and consisted of a smaller sample size (n = 30) with no follow-up. Our intervention utilized short HIIT bouts which may influence the outcome measures, although preferred duration of HIIT bouts are not currently defined. Data collection of physical activity in the CON was gathered through patient-reported logs, a potentially less efficient method of activity tracking. Future studies should extend the intervention period, allowing for training to overlap with consecutive chemotherapy regimens.
Clinical implications
Given the psychosocial and physical detriment on breast cancer patients caused by anthracycline-based chemotherapy, prescription of exercise offers a safe, feasible, non-pharmaceutical option for patients to participate in while undergoing treatment. Our results of improvements in physical functioning and maintenance of QOL provide clinicians with promising alternative ways to decrease the burden on their patients.
In summary, the results of the current study demonstrate that HIIT improves some aspects of physical function and maintains QOL in breast cancer patients undergoing anthracycline-based chemotherapy. This finding highlights the benefit of HIIT on physical function and PROs, which provides evidence to support the adoption of exercise during chemotherapy. Future studies are needed to elucidate the HIIT prescription parameters needed to globally improve physical function and PROs against negative anthracycline-related side effects.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
Giordano SH et al (2012) Decline in the use of anthracyclines for breast cancer. J Clin Oncol 30(18):2232
Gilliam LA, St DK (2011) Clair, Chemotherapy-induced weakness and fatigue in skeletal muscle: the role of oxidative stress. Antioxid Redox Signal 15(9):2543–2563
Mills PJ et al (2005) The relationship between fatigue and quality of life and inflammation during anthracycline-based chemotherapy in breast cancer. Biol Psychol 69(1):85–96
Wong ML et al (2018) Characteristics associated with physical function trajectories in older adults with cancer during chemotherapy. J Pain Symptom Manage 56(5):678-688.e1
Hofman M et al (2007) Cancer-related fatigue: the scale of the problem. Oncologist 12(1):4
Manir KS et al (2012) Fatigue in breast cancer patients on adjuvant treatment: course and prevalence. Indian J Palliat Care 18(2):109
Sehl M et al (2013) Decline in physical functioning in first 2 years after breast cancer diagnosis predicts 10-year survival in older women. J Cancer Surviv 7(1):20–31
Patel AV et al (2019) American College of Sports Medicine roundtable report on physical activity, sedentary behavior, and cancer prevention and control. Med Sci Sports Exerc 51(11):2391–2402
Campbell KL et al (2019) Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci Sports Exerc 51(11):2375–2390
Troeschel AN, Leach CR, Shuval K, Stein KD, Patel AV (2018) Peer reviewed: physical activity in cancer survivors during “Re-entry” following cancer treatment. Prev Chronic Dis 15:E65
Mugele H et al (2019) High-intensity interval training in the therapy and aftercare of cancer patients: a systematic review with meta-analysis. J Cancer Surviv 13(2):205–223
Choi H-Y et al (2018) Superior effects of high-intensity interval training compared to conventional therapy on cardiovascular and psychological aspects in myocardial infarction. Ann Rehabil Med 42(1):145
Coetsee C, Terblanche E (2017) The effect of three different exercise training modalities on cognitive and physical function in a healthy older population. Eur Rev Aging Phys Act 14(1):13
Thum JS et al (2017) High-intensity interval training elicits higher enjoyment than moderate intensity continuous exercise. PLoS ONE 12(1):e0166299
Lee K et al (2018) Effects of high-intensity interval training on vascular function in breast cancer survivors undergoing anthracycline chemotherapy: design of a pilot study. BMJ Open 8(6):e022622
Lee K et al (2019) Feasibility of high intensity interval training in patients with breast cancer undergoing anthracycline chemotherapy: a randomized pilot trial. BMC Cancer 19(1):653
Nguyen J et al (2015) EORTC QLQ-BR23 and FACT-B for the assessment of quality of life in patients with breast cancer: a literature review. J Comp Eff Res 4(2):157–166
Krohe M et al (2019) Content validity of the National Comprehensive Cancer Network-Functional Assessment of Cancer Therapy-Breast Cancer Symptom Index (NFBSI-16) and Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function Short Form with advanced breast cancer patients. Health Qual Life Outcomes 17(1):92
Wintermann G-B et al (2018) Fatigue in chronically critically ill patients following intensive care-reliability and validity of the multidimensional fatigue inventory (MFI-20). Health Qual Life Outcomes 16(1):37
Gu J et al (2016) Examining the factor structure of the 39-item and 15-item versions of the five facet mindfulness questionnaire before and after mindfulness-based cognitive therapy for people with recurrent depression. Psychol Assess 28(7):791
Morishita S et al (2019) Assessment of the mini-balance evaluation systems test, timed up and go test, and body sway test between cancer survivors and healthy participants. Clin Biomech 69:28–33
Eden MM, Tompkins J, Verheijde JL (2018) Reliability and a correlational analysis of the 6MWT, ten-meter walk test, thirty second sit to stand, and the linear analog scale of function in patients with head and neck cancer. Physiother Theory Pract 34(3):202–211
Schmidt K et al (2013) Validity of the six-minute walk test in cancer patients. Int J Sports Med 34(07):631–636
Hetzler RK et al (2010) Development of a modified Margaria-Kalamen anaerobic power test for American football athletes. J Strength Cond Res 24(4):978–984
Nedeljkovic A et al (2007) Evaluation of Margaria staircase test: the effect of body size. Eur J Appl Physiol 100(1):115–120
Mijwel S et al (2018) Adding high-intensity interval training to conventional training modalities: optimizing health-related outcomes during chemotherapy for breast cancer: the OptiTrain randomized controlled trial. Breast Cancer Res Treat 168(1):79–93
Mijwel S et al (2018) Highly favorable physiological responses to concurrent resistance and high-intensity interval training during chemotherapy: the OptiTrain breast cancer trial. Breast Cancer Res Treat 169(1):93–103
Courneya KS et al (2007) Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: a multicenter randomized controlled trial. J Clin Oncol 25(28):4396–4404
Lipsett A et al (2017) The impact of exercise during adjuvant radiotherapy for breast cancer on fatigue and quality of life: a systematic review and meta-analysis. The breast 32:144–155
Farthmann J et al (2016) The impact of chemotherapy for breast cancer on sexual function and health-related quality of life. Support Care Cancer 24(6):2603–2609
Cámara RJ et al (2019) Quality of life during and after adjuvant anthracycline-taxane-based chemotherapy with or without Gemcitabine in high-risk early breast cancer: results of the SUCCESS A trial. Breast Cancer Res Treat 175(3):627–635
Acknowledgements
We acknowledge the Clinical Investigations Support Office of the Norris Comprehensive Cancer Center for their regulatory support of this investigation and the extraordinary generosity of our study participants.
Funding
This work was supported by grant UL1TR001855 from the National Center for Advancing Translational Science (NCATS) of the U.S. National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
Conceptualization (all authors); methodology (Kyuwan Lee and Christina Dieli-Conwright); writing original draft (all authors); review & editing (all authors); resources (Christina Dieli-Conwright), and supervision (Christina Dieli-Conwright). All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval
The protocol was approved by the University of Southern California Institutional Review Board (HS-1500227); ClinicalTrials.gov: NCT02454777; date of registration: May 27th, 2015.
Consent to participate
The informed consent was approved by the University of Southern California Institutional Review Board (HS-1500227); ClinicalTrials.gov: NCT02454777; date of registration: May 27th, 2015.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Kyuwan Lee and Mary K. Norris are co-first authors
Rights and permissions
About this article

Cite this article
Lee, K., Norris, M.K., Wang, E. et al. Effect of high-intensity interval training on patient-reported outcomes and physical function in women with breast cancer receiving anthracycline-based chemotherapy. Support Care Cancer 29, 6863–6870 (2021). https://doi.org/10.1007/s00520-021-06294-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-021-06294-7