
Abstract
Purpose
Return to work (RTW) is an important component of cancer survivorship for individual rehabilitation and economic development. The focus of prior research on cancer survivor RTW has generally been on Western and general cancer populations. There is a need to examine the existing research on RTW decisions and experiences in Korean breast cancer survivors (BCS).
Methods
This scoping review followed the framework of Arksey and O’Malley, which consisted of identifying the research question, discovering and selecting studies, charting data, analyzing results, and incorporating expert consultations. Quality assessments and a thematic map were included.
Results
Out of 863 original articles found in the literature search, 8 articles met the inclusion criteria. Majority were published in the past 5 years. The scope of the field, socio-demographic and clinical associations, and factors associated with RTW decision-making and experiences were reported. In the thematic analysis, 4 main categories were derived.
Conclusions
Future research needs to be conducted on effective RTW interventions targeting various educational backgrounds, socioeconomic levels, and job types. More institutional and social support would encourage more successful RTW through educational awareness, financial assistance, and workplace accommodations. Future studies should focus on interdisciplinary RTW efforts with multiple stakeholders.
Implication for cancer survivors
BCS need programs that include social support, individual coping strategies, reliable RTW information, physical rehabilitation, vocational counseling, workplace allowances, and psychological support. More support should be provided through extending the work law and engaging employers. If they desire to resume working, BCS should be fully supported with RTW specific resources.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
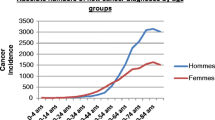
Breast cancer is the second most common cancer in South Korean women and its incidence rate has been increasing annually by 4.5% between 2007 and 2015 [1]. Whereas the incidence rate of breast cancer in the USA is highest for 55–64 year olds, the highest proportion in Korea is among those aged 40–49 years old [1]. With positive survival outcomes accompanying more diagnoses at younger ages, there have been increasingly more breast cancer survivors (BCS) in Korea. Korean women have been seen retiring in their 60s and later [2]. Not only are there high levels of working among older Koreans [1, 3] but there also are higher rates of self-employed workers who often retire later than their wage-and-salary counterparts [2]. Yet, Korean BCS have been found to lag behind Western patients in rejoining or continuing to participate in the workforce after diagnosis and treatment, with significant costs from lost productivity and difficulty with return to work (RTW) [3, 4].
Prior research emphasizes the importance of conducting RTW-focused studies as there is substantial evidence that cancer survivors are more likely to be unemployed than the general population [5]. As found in studies primarily focused on Western populations, RTW can be an important part of survivorship, in terms of economic contributions, sense of purpose and normality, increase in quality of life (QoL), and benefits to physical and mental health [3, 6, 7]. According to a Western review study, as BCS readjust to work, social, and family roles after their diagnosis, they might struggle with a wide variety of difficulties that significantly impact their QoL and ability or desire to RTW [6].
There are a number of existing reviews that examine factors associated with RTW of cancer survivors [5,6,7,8,9,10,11]. However, the majority is focused on white populations in Western countries, and usually has limited focus on breast cancer specific studies [5,6,7,8,9, 12]. A handful of studies have noted key cultural differences and challenges (such as high levels of self-stigma, importance of social relationships, and concern over cancer diagnosis disclosure) that define RTW experiences for Asian cancer survivors [13,14,15]. In certain Asian populations, Confucianism influences gender and familial roles which might affect priorities, support, and expectations of BCS [15]. RTW is a recent research field of interest in South Korea and is quickly growing [3]. As BCS’ experiences in Korea are closely intertwined with cultural traditions and the healthcare system, it is important to understand the differing aspects of Korean cultural and socioeconomic context in order to design and implement effective interventions targeting RTW [16]. This scoping review sought to contribute to the existing gap by extensively identifying and charting RTW information specific to a breast cancer and a non-Western population.
This scoping review aims to provide a comprehensive overview on and to increase our collective understanding of the RTW experiences of BCS in South Korea. Scoping reviews are increasingly used to map and analyze the existing research evidence in a particular complex or relatively unexamined field of interest [17]. A scoping review has a broad conceptual range and allows for a wide variety of relevant literature and studies to be included [17].
Methods
This scoping review followed the 6 stages outlined in the Joanna Briggs Institute manual [18], based on Arksey and O’Malley’s classical framework [17].
Stage 1: Identification of research question
We aimed to identify: (1) What is the current research progress regarding RTW of BCS in Korea, with a focus on scope and quality of research? (2) What are the RTW experiences of BCS in Korea, especially related to RTW decision-making?
Stage 2: Identification of relevant studies
A preliminary search for existing reviews was conducted in January 2019. CINAHL Plus, Cochrane Library, Medline, and KoreaMed were searched to identify relevant keywords. After finalizing keywords (e.g., breast cancer, and RTW), a formal search was conducted in February and March 2019, for articles published in Korean or English from January 2000 to March 2019. We searched the following electronic databases: Medline, Embase, Cochrane Library, CINAHL Plus, JSTOR, and PsycINFO; including five Korean databases, ProQuest Dissertations & Theses Global, and Open Grey Database. Finally, a search was run on the reference lists of identified full-text articles. Full-text publications and unpublished research were considered for this review. The full search strategy can be found in Table 1 of the Appendix.
Stage 3: Selection of studies
Studies that met the following inclusion criteria were selected: (1) Korean BCS; (2) women aged 20–70 years old; and (3) reported work experience, RTW decision-making, or a RTW-focused intervention. Exclusion criteria were selected: (1) did not report work experience or RTW decision-making and (2) included other cancer types.
Titles and abstracts were independently assessed by two reviewers (A, B) for fit and relevance, followed by evaluation of full-text versions to determine inclusion and exclusion. A third reviewer (C) was present to settle any disagreements.
Stage 4: Charting the data
Data from each study was extracted, including author information, publication year, study type and design, study population, RTW definition, study aims, methodology, outcome variables, key findings, limitations, and future directions.
Stage 5: Collating, summarizing, and reporting the results
We conducted thematic mapping (Table 2, Table 2 in the Appendix) utilizing the Braun and Clarke framework [17, 19,20,21]. Using Microsoft Excel as an organizational and conceptual tool, we extracted variables found in the main findings of the included studies and re-arranged these results into larger thematic clusters in order to identify key trends across the studies [18, 19]. To guide the write up and serve as a visual aid, a thematic map was constructed [19].
Methodological quality appraisal was an important component for this scoping review [20]. The Critical Appraisal Skills Programme (CASP) checklist for qualitative studies [22, 23] and the Risk of Bias for Non-Randomized Study (RoBANS) tool [24, 25] were utilized to assess the quality of the studies. Two researchers (A, B) conducted the quality appraisal in order to reduce bias and maintain consistency. We adhered to the PRISMA checklist in writing this manuscript [21].
Stage 6: Consultation
Consultations were held with several experts in cancer survivorship, e.g., academics and clinicians. They reviewed and offered revisions for the thematic map and pointed out gaps in the literature.
Results
Eight articles were included for analysis [26,27,28,29,30,31,32,33]. The PRISMA flow diagram [21] presenting the selection process is found in Fig. 1.

PRISMA flow diagram for selection of studies regarding return to work decision-making and experiences of breast cancer survivors in Korea
Characteristics of selected studies
Scope of articles
The characteristics of these studies are shown in Tables 1 and 2, and Table 2 in the Appendix. Seventy-five percent were published 2015–2017, indicating research in this field being relatively new. The majority of studies produced descriptive results [27, 28, 30, 31]. Most were based on surveys and interviews, with only 1 preliminary clinical intervention study identified [32]. As only 1 study was prospective in nature [33], this limited causality of variables and examining change over time. Another common limitation was a lack of generalizability of results related to skewed population characteristics (higher income, more education, lack of personal information) and use of particular recruitment methods (convenience sampling, single institution, selection bias, low response rate) [26, 28,29,30,31, 33]. Examined RTW topics included employment status [26, 28, 30, 33], balancing work and treatment [27, 29, 31, 32], workload [31], sick leave [27, 31], disclosure of cancer diagnosis [31], and labor welfare programs in the workplace [27, 31].
Quality assessment
Quality assessments are presented in Tables 3 and 4 in the Appendix. The majority of included studies appeared to be well designed and ethically conducted, with visible efforts to reduce bias. The greatest concerns were that selection of participants wasn’t sufficiently reported in 4 studies [27, 29, 32, 33] and blinding of outcome assessments [26, 28,29,30, 32, 33] had unclear or high risk of bias for 6 studies.
Relationships among socio-demographic and clinical characteristics
While women in their 40s might be more likely to keep their jobs than younger women, there was a high prevalence of depression and anxiety in these Korean BCS [26, 28, 31]. More education was positively associated with RTW [32]. Correlates of higher QoL for Korean BCS in their 40s included being self-employed or in a professional/ managerial position and having a monthly income greater than 4 million (in comparison to the average 2.9 million) Korean Won [30, 34]. Unemployment was associated with more than 2 comorbidities and advanced or extensive surgery in the case-control study [26], whereas a prospective cohort study found clinical characteristics to have no association with RTW [33] (Table 2).
Factors associated with decision to RTW
Found in both qualitative and observational research, support is an important factor in determining BCS RTW in Korea [27, 33]. Negative associations with RTW included appetite loss, fatigue, and childbirth at 12–24 months post-diagnosis [33]. Positive associations with successful RTW included more educational materials, regular exercise, better personal body image and physical function post-treatment, and healthy existential well-being [33]. According to a qualitative grounded theory study, single mothers were more likely to resume employment in order to support their children [31].
Factors associated with RTW experiences
Fatigue and exhaustion were perceived to be the most frequent physical difficulties [26]. Yet, overall low levels of pain were reported in mostly qualitative research [27, 28, 31]. According to interviews and surveys, cancer survivorship is also a time of increased emotional sensitivity and distress, particularly depression and anxiety [26,27,28, 31, 32]. Cancer diagnoses appear to change people’s perception of the meaning of their work and roles in life, with patients experiencing varied struggles with helplessness, body image negativity, and other emotions [27,28,29, 31,32,33]. In addition, survivors struggled with balancing simultaneous treatment and work as reported by interviews and semantic network analysis [27, 29], while also voicing concerns about potential disadvantages as a cancer patient in their workplace [26, 31]. One case-control study highlighted how BCS might face reduced wages, working hours, and promotional opportunities after their diagnosis [26]. From two qualitative studies, other concerns are negatively received diagnosis disclosures and discrimination [27, 31].
According to both qualitative and observational research, positive high-quality support is imperative [27,28,29, 31, 32]. Throughout several different study designs, participants made various personal efforts towards adopting effective coping mechanisms including self-care, positive thinking, consistent exercise, healthy eating habits, working strategically, and reducing extra responsibilities [27, 31,32,33]. The intervention study [32] stressed the importance of counseling and peer support groups to facilitate post-traumatic growth and of considering personality traits. Furthermore, lack of labor welfare programs offered by the workplace and specific RTW informational resources for Korean BCS was highlighted in the qualitative grounded theory study [31] (Table 2).
Thematic mapping
A total of 407 concepts were created by extensively examining the key findings of each included study. These concepts were classified into 24 subcategories based upon shared themes, and 4 final categories were derived. For example, one study found that women living with a spouse were more likely to stop working. This data was categorized as “family relationships and effect on RTW” as opposed to peer support. However, since family relationships and peer support are all related to support for BCS, these subcategories were combined into a larger theme of “Impact of Support and Relationships” which is directly related to the main theme of “Employment Status/RTW Experience of BCS” (Fig. 2).

Thematic map of employment status/RTW experience of breast cancer survivors in Korea. RTW, return to work
“Identifying the struggles of individuals” pointed to the physical, psychological, and financial burdens of cancer and how these challenges related to the general work ability and daily work activity of survivors. Primary concerns were psychological difficulties adjusting to physical and body image changes, general psychological difficulties, and difficulty balancing daily work responsibilities and schedule changes. Financial burden was not noted as a high priority by the experts consulted in Stage 6.
“Coming to terms with breast cancer and working again” focused on coping strategies and mindsets, lifestyle changes and priority shifts, and decision-making in disclosing breast cancer diagnoses. Mindset and personality were important, with individual BCS pursuing thankfulness, positivity, and open mindsets. Personal measures for healthier living included improving fitness, diet, hygiene, and sleep.
“Impact of support and relationships” included the influence of workplace, family, and social relationships on well-being and RTW. Supervisors and colleagues played an important role. Family support was also significant, with contributions such as emotional support and housework help being desired by Korean BCS from their spouse and children. High-quality social support was necessary to avoid additional psychological burden. Stigma is acknowledged to be a concern when attempting to RTW, resulting in reduced wages, less promotional opportunities, tensions in the workplace, and loss of employment. Expert consultations pointed to the importance of implementing effective RTW interventions, providing more support within the workplace, and the need for more institutional support. There was a strong desire from BCS for more reliable and specific resources, such as professional education and counseling.
Finally, “associated factors” consisted of clinical factors and socio-demographics. Lower educational level, lower household income, two or more comorbid diseases, more advanced stage cancer, and extensive surgery were found to be associated with unemployment.
Discussion
Overview of studies
Research on RTW in BCS in Korea primarily utilized an observational or qualitative study design. International interventions may be applicable, as long as considerations for Korean cultural, legal, and healthcare system differences are taken into account. Comparing Korean and Western reviews covering RTW, limitations were similar, including bias in population characteristics, unreliable recruitment methods, difficulty comparing studies due to variable study measures, and lack of long-term follow-up [6, 9, 26, 28,29,30,31, 33].
International research covered physical/sexual/cognitive function, psychological distress, support, and financial burden as related to RTW [6, 8, 11]. However, for Korean BCS, we only found 1 study on cognitive and sexual function [33], and only 2 studies examining social bias and discrimination [27, 31]. Western reviews have covered individual meaning of work, employment types, RTW interventions, vocational guidance, rehabilitation programs [11] employment status, sick leave duration, and working hours [8]. In contrast, our review had limited coverage of RTW interventions [32], post-traumatic growth promotion [32], disclosure of diagnosis [31], labor welfare programs [27, 31], and reduced working hours [26, 27]. In fact, the studies in this review explicitly highlighted lack of data on changing priorities [33], work problems occurring pre-cancer diagnosis [33], job type or physical workload [26, 33], flexibility of jobs [33], and assistance from colleagues/employers [33]. More research is needed to expand the current understanding of RTW of Korean BCS.
Factors influencing RTW
This review identified conflicting data about clinical characteristics and RTW. In agreement with international research [7, 8, 10], 1 study noted disease stage and type of treatment to have a significant impact on RTW outcomes [26]. Yet, another study found no such association [33]. As a prospective cohort study, the latter study suggested that clinical characteristics might have less of an impact on RTW farther out from the initial breast cancer diagnosis [33]. It would be beneficial to provide RTW interventions during or immediately after treatment for BCS with more advanced stages and extensive surgery to counteract the challenges of RTW that present early on for these BCS.
For Korean BCS, marriage [3, 30] and low-paying jobs [3] meant a lower likelihood of RTW, whereas education was positively associated with RTW [30, 33]. This appears parallel to a Western study that found less education and low income to be negatively associated with RTW [9]. These combined results suggest that it would be beneficial to develop more RTW interventions for Korean BCS with lower education and income.
Fatigue was generally perceived to be the most common physical barrier to RTW of BCS [26, 33], whereas better physical function is positively associated with better RTW outcomes, in agreement with international reports [7, 10]. Overall low levels of pain were reported in Korean BCS [27, 28, 31], contrasting with chronic pain found in Western populations [6]. Individual fatigue management strategies, as well as consistent nutrition and physical activity, should be incorporated into RTW programs as means of improving physical function and surgery outcomes post-treatment [28, 29, 31,32,33].
Findings from this scoping review noted that Korean BCS significantly struggle in terms of psychological difficulties. Whereas these articles largely focused on personal body image and existential well-being [27, 29, 31,32,33], Korean research is expanding quickly to include cognitive impairments and frustrations with role fulfillment [29, 31, 33]. There is some evidence in BCS that cognitive dysfunction negatively impacts QoL and work-related outcomes, but the impact appears to diminish in severity over time [5, 7]. With limited results reporting on cognitive and emotional function, we should further explore their impact on RTW of Korean BCS.
Although financial burden was examined in many of our articles [26, 27, 30, 31, 33], it was not noted as a major factor in RTW. The lesser priority may be because Korea has universal healthcare coverage that supports breast cancer treatments. However, it appears that with a rapidly increasing incidence rate of breast cancer, overall socioeconomic cost and individual financial burden for Korean BCS are becoming more burdensome [1]. More research is needed to better understand financial situations of Korean BCS.
Work-related concerns and interventions
Korean BCS struggle with balancing simultaneous treatment and work [27, 29], and also might experience disadvantages in their workplace [26, 31]. In agreement with Western research, Korean BCS may also face reduced wages, working hours, promotional opportunities, and work ability [10, 26].
In order to combat RTW difficulties, positive high-quality social support is imperative. In agreement with international research [7, 8, 12], the importance of social support appears to be emphasized heavily in the RTW of Korean BCS [27, 29, 31] and comes from peers, religious groups, family, and the workplace [27,28,29, 31, 32]. Support has been found to be positively associated with QoL, survivor well-being [6], and successful RTW [27, 31]. Difficulties in relationships with coworkers and superiors, internal struggles regarding identity and ability, and balancing responsibilities are all important target areas requiring intervention for Korean BCS. More RTW support resources need to be easily accessible to BCS and could be provided in the workplace such as through a company-based cancer survivor support group.
International research has found that RTW is positively associated with the availability of counseling, rehabilitation services, career training, and job search systems [10]. However, those programs catering to BCS are limited in Korea [3] and BCS may be reluctant to reveal their diagnosis to potential employers [31]. Furthermore, the existing employment law offers little legal protection for BCS, with limited right to little paid sick leave, and even less protection for self-employed workers on short-term contracts (or employed by firms with less than 5 employees) [4]. More institutional and workplace resources should be provided for Korean BCS [31]. Government support could include incentives like tax benefits for companies to employ cancer survivors, expanded insurance coverage for lower socioeconomic BCS, and laws to ensure adequate paid sick leave and flexible work hours for cancer survivors [27]. Employers should provide more resources about BCS rights at work, vocational counseling and rehabilitative services, and address discrimination in the workplace [31]. Workplaces could help adjust workload and working hours to make RTW more manageable.
Survivors worldwide continue to face stigma in the workplace [27, 31, 35, 36]. Particularly in Asia and in Asian American populations, stigma, self-stigma, and misinformation regarding the RTW of cancer survivors is prevalent [3, 13, 14, 35, 37]. Over 30% of Korean cancer survivors had negative stereotypical views of cancer patients, about with about 10% experiencing discrimination [38]. Stigma related to cancer diagnosis is critical to address due to potential negative outcomes of hiring discrimination, harassment and hostile work environments, denial of necessary workplace accommodations, reduced wages, and demotion or loss of employment [35]. Others’ negative reactions and discriminatory workplace behaviors can also be driving forces in BCS being unwilling to reveal their diagnosis or access support [35,36,37]. Furthermore, it has been found that individual perception of limited ability at work can play a significant role in the RTW decision-making process [12]. More work needs to be done to increase awareness in the general Korean public, and provide support for BCS experiencing self-stigma outcomes.
RTW interventional programs can include easily accessible RTW information, instructions for structured RTW plans, and support groups [9]. The preliminary intervention study addressed the need for professional educational materials and stressed the importance of counseling and peer support [32]. Adjusting mindsets and lifestyle habits can be useful tools of RTW intervention, perhaps addressed during support group meetings and with online educational materials verified by healthcare providers. More educational resources and peer support (cooking, typing, rehabilitation), along with a focus on strengthening coping skills, is needed to better cope with physical and body image changes for Korean BCS [12].
Moderate evidence over the years has found multidisciplinary interventions that combine physical, psycho-behavioral, educational, and vocational components help increase RTW rates for BCS [6, 7]. There must be interdisciplinary teamwork (including healthcare providers and employers) to bind together these multidisciplinary interventions to begin at the start of sick leave [9]. In Western literature, a review on RTW interventions for BCS found that only 38% were work directed and offered services beyond basic RTW information, 80% were provided by healthcare professionals, and 75% took place after completion of treatment [9]. Although strides are being made to acknowledge RTW as an essential component of cancer survivorship, more stakeholders need to get involved, providing more consistent and reliable resources. We should focus on helping survivors plan structured RTW for individual-specific challenges, evaluating the impact and severity of illness on RTW abilities, and encouraging employers to make flexible and informed workplace accommodations [9]. Not only do more RTW interventions need to be designed and implemented but the efficacy of such programs also should be rigorously evaluated [5]. In Korea, more clinicians and researchers are getting involved in developing RTW interventions to meet this need [3], such as a multi-center randomized control trial [32].
Strengths and limitations
This study’s strength is that it offers understanding of Korean BCS and BCS in other Asian regions as well, as public perceptions of cancer stigma and Confucian influences may be shared [37]. It also employed rigorous and transparent methods including systematic efforts to review the literature and thorough quality assessments. A limitation of this study is that with focus on BCS, perspectives of other stakeholders in the RTW of Korean BCS were not included. Finally, some relevant studies might have been missed and unintentionally excluded from review due to database selection, search strategy errors, and time constraints.
Directions for future research
Future Korean BCS research examining RTW should expand its scope to include more studies examining fatigue assessment, cognitive/emotional function, stigma and discrimination, and financial burden. It would be beneficial for further studies to examine perceptions of workplace stigma from a variety of perspectives, across a variety of occupations, and to compare across different Asian cancer populations. Additionally, more RTW support studies are needed that target survivors with lower educational and socioeconomic levels, especially single mothers. Finally, it is important that more longitudinal and RCT intervention studies are conducted.
This scoping review identified many recommendations for future clinical interventions and policy change to encourage effective RTW in Korean BCS. Strategies to combat fatigue, address appetite loss, manage emotional distress, and tackle body image issues should be incorporated into a unified care plan to increase RTW success rates [33]. Development of effective multidisciplinary RTW intervention models, addressing psychological difficulties (particularly physical and body image changes), work ability, and handling work schedules, would benefit BCS. A successful RTW intervention might include social support, self-care management and coping tools, reliable information about healthy diet and exercise, physical rehabilitation, vocational counseling, workplace coordination to increase schedule flexibility/ accommodations, and financial support. Beyond clinicians and researchers, more stakeholders need to become involved in improving the survivorship care of Korean BCS. The employment law needs to be expanded to offer more legal protection, insurance coverage, and adequate sick leave payment. Employers can provide more support with flexible working hours, systems to pinpoint and address stigma and discrimination in the workplace, and vocational counseling and rehabilitative services.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Kang SY, Kim YS, Kim Z, Kim H-Y, Lee SK, Jung KW, Youn HJ, Korean Breast Cancer Society (2018) Basic findings regarding breast cancer in Korea in 2015: data from a breast cancer registry. J Breast Cancer 21(1):1–10. https://doi.org/10.4048/jbc.2018.21.1.1
Lee C, Lee J (2013) Employment status, quality of matching, and retirement in Korea: evidence from Korean longitudinal study of aging. J Popul Ageing 6(1–2):59–83. https://doi.org/10.1007/s12062-012-9080-x
Kielstra P (2018) Breast cancer patients and survivors in the Asia-Pacific workforce. South Korea: an incipient response to the ballooning problem The Economist Website https://eiuperspectives.economist.com/healthcare/breast-cancer-patients-and-survivors-asia-pacific-workforce/white-paper/breast-cancer-patients-and-survivors-asia-pacific-workforce-south-korea-incipient-response. Accessed 13 July 2020
Park JH, Lee SK, Lee JE, Kim SW, Nam SJ, Kim JY, Ahn JS, Park W, Yu JH, Park YH (2018) Breast cancer epidemiology of the working-age female population reveals significant implications for the South Korean economy. J Breast Cancer 21(1):91–95. https://doi.org/10.4048/jbc.2018.21.1.91
Richardson A, Addington-Hall J, Amir Z, Foster C, Stark D, Armes J, Brearley SG, Hodges L, Hook J, Jarrett N, Stamataki Z, Scott I, Walker J, Ziegler L, Sharpe M (2011) Knowledge, ignorance and priorities for research in key areas of cancer survivorship: findings from a scoping review. Br J Cancer 105(1):S82–S94. https://doi.org/10.1038/bjc.2011.425
de Boer AG, Taskila TK, Tamminga SJ, Feuerstein M, Frings-Dresen MH, Verbeek JH (2015) Interventions to enhance return-to-work for cancer patients. Cochrane Database Syst Rev 9:CD007569. https://doi.org/10.1002/14651858.CD007569.pub3
Bijker R, Duijts SF, Smith SN, de Wildt-Liesveld R, Anema JR, Regeer BJ (2018) Functional impairments and work-related outcomes in breast cancer survivors: a systematic review. J Occup Rehabil 28(3):429–451. https://doi.org/10.1007/s10926-017-9736-8
Van Muijen P, Weevers N, Snels IA, Duijts S, Bruinvels DJ, Schellart AJ, Van Der Beek AJ (2013) Predictors of return to work and employment in cancer survivors: a systematic review. Eur J Cancer Care 22(2):144–160. https://doi.org/10.1111/ecc.12033
Bilodeau K, Tremblay D, Durand MJ (2017) Exploration of return-to-work interventions for breast cancer patients: a scoping review. Support Care Cancer 25(6):1993–2007. https://doi.org/10.1007/s00520-016-3526-2
Mehnert A (2011) Employment and work-related issues in cancer survivors. Crit Rev Oncol Hematol 77(2):109–130. https://doi.org/10.1016/j.critrevonc.2010.01.004
Stergiou-Kita M, Grigorovich A, Tseung V, Milosevic E, Hebert D, Phan S, Jones J (2014) Qualitative meta-synthesis of survivors’ work experiences and the development of strategies to facilitate return to work. J Cancer Surviv 8(4):657–670. https://doi.org/10.1007/s11764-014-0377-z
Sun Y, Shigaki CL, Armer JM (2017) Return to work among breast cancer survivors: a literature review. Support Care Cancer 25(3):709–718. https://doi.org/10.1007/s00520-016-3446-1
Tang PL, Mayer DK, Chou F-H, Hsiao KY (2016) The experience of cancer stigma in Taiwan: a qualitative study of female cancer patients. Arch Psychiatr Nurs 30(2):204–209. https://doi.org/10.1016/j.apnu.2015.08.015
Tsai W, Lu Q (2019) Ambivalence over emotional expression and intrusive thoughts as moderators of the link between self-stigma and depressive symptoms among Chinese American breast cancer survivors. J Behav Med 42(3):452–460. https://doi.org/10.1007/s10865-018-9996-6
Yoon H, Chatters L, Kao T-SA, Saint-Arnault D, Northouse L (2016) Factors affecting quality of life for Korean American cancer survivors: an integrative review. Oncol Nurs Forum 43(3):132–142. https://doi.org/10.1188/16.ONF.E132-E142
Suh EE (2013) Cultural models of female breasts and breast cancer among Korean women. Open J Nurs 3(05):404–413. https://doi.org/10.4236/ojn.2013.35055
Arksey H, O'Malley L (2005) Scoping studies: towards a methodological framework. Int J Sci Res 8(1):19–32. https://doi.org/10.1080/1364557032000119616
Peters MDJ, Godfrey CM, McInerney P, Soares CB, Khalil H, Parker D (2015) Methodology for JBI scoping reviews. The Joanna Briggs Institute Reviewers’ Manual 2015. The Joanna Briggs Institute, Adelaide
Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3(2):77–101. https://doi.org/10.1191/1478088706qp063oa
Daudt HM, van Mossel C, Scott SJ (2013) Enhancing the scoping study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res Methodol 13(1):48. https://doi.org/10.1186/1471-2288-13-48
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151(4):264–269. https://doi.org/10.7326/0003-4819-151-4-200908180-00135
Critical Appraisal Skills Programme (2017) CASP qualitative checklists. https://casp-uk.net/casp-tools-checklists/. Accessed 13 July 2020
Hannes K, Lockwood C, Pearson A (2010) A comparative analysis of three online appraisal instruments’ ability to assess validity in qualitative research. Qual Health Res 20(12):1736–1743. https://doi.org/10.1177/1049732310378656
Dixon-Woods M, Sutton A, Shaw R, Miller T, Smith J, Young B, Bonas S, Booth A, Jones D (2007) Appraising qualitative research for inclusion in systematic reviews: a quantitative and qualitative comparison of three methods. J Health Serv Res Pol 12(1):42–47. https://doi.org/10.1258/135581907779497486
Kim SY, Park JE, Lee YJ, Seo H-J, Sheen S-S, Hahn S, Sheen SS, Hahn SK, Jang BH, Son HJ (2013) Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J Clin Epidemiol 66(4):408–414. https://doi.org/10.1016/j.jclinepi.2012.09.016
Ahn E, Cho J, Shin DW, Park BW, Ahn SH, Noh DY, Nam SJ, Lee ES, Yun YH (2009) Impact of breast cancer diagnosis and treatment on work-related life and factors affecting them. Breast Cancer Res Treat 116(3):609–616. https://doi.org/10.1007/s10549-008-0209-9
Heo E, Kang H, Kim K, Hong Y (2011) Return-to-work experiences among breast cancer survivors. J Korean Soc Matern Child Health 15(1):92–102
Hwang SY (2015) Risk factors for depression and anxiety among breast cancer survivors in their 40s. J Korea Cont 15(2):313–323. https://doi.org/10.5392/JKCA.2015.15.02.313
Bae KR, Kwon SY (2016) The workplace experiences of breast cancer survivors: a survey of an online community. Asia Oncol Nurs 16(4):208–216. https://doi.org/10.5388/aon.2016.16.4.208
Hwang SY (2016) The impact of socioeconomic status on quality of life among breast cancer survivors: focusing on breast cancer survivors in their 40s. J Korea Cont 16(2):503–512. https://doi.org/10.5392/JKCA.2016.16.02.503
Kim J (2016) Return-to-work experience of breast cancer survivors: a qualitative study based on grounded theory approach. Dissertation, Seoul, Yonsei University
Bae K (2017) Development of a posttraumatic growth promoting program for working breast cancer patients. Dissertation, Seoul, Yonsei University
Lee MK, Kang HS, Lee KS, Lee ES (2017) Three-year prospective cohort study of factors associated with return to work after breast cancer diagnosis. J Occup Rehabil 27(4):547–558. https://doi.org/10.1007/s10926-016-9685-7
Choi HJ (2019) Average monthly income for labor workers, and corporate and small company employees. Chosun Biz Website. https://biz.chosun.com/site/data/html_dir/2020/01/22/2020012202374.html. Accessed 13 July 2020
Stergiou-Kita M, Pritlove C, Kirsh B (2016) The “Big C”-stigma, cancer, and workplace discrimination. J Cancer Surviv 10(6):1035–1050. https://doi.org/10.1007/s11764-016-0547-2
Knapp S, Marziliano A, Moyer A (2014) Identity threat and stigma in cancer patients. Health Psychol Open 1(1):1–10. https://doi.org/10.1177/2055102914552281
Wang JW, Shen Q, Ding N, Zhang TR, Yang ZQ, Liu C, Chen SJ, Berry HL, Yuan ZP, Yu JM (2016) A qualitative exploration of the unmet psychosocial rehabilitation needs of cancer survivors in China. Psycho-Oncology 25(8):905–912. https://doi.org/10.1002/pon.4023
Cho J, Ek C, Kim SY, Shin DW, Cho BL, Kim CH, Koh DH, Guallar E, Bardwell WA, Park JH (2013) Association between cancer stigma and depression among cancer survivors: a nationwide survey in Korea. Psycho-Oncology 22(10):2372–2378. https://doi.org/10.1002/pon.3302
Acknowledgments
The Fulbright Research Scholarship allowed Kate Sohn to initiate and complete this analysis of the existing literature. Neither the Government of the USA nor any agency representing it has endorsed the conclusions nor approved the contents of this manuscript. We thank Dr. Eun Joo Yang, Dr. Ka Ryeong Bae, and Ms. Jae Yoon Yi, for sharing their insights in the consultations for stage 6.
Author information
Authors and Affiliations
Contributions
All authors contributed substantially to this scoping review. Kim S and Sohn K conceived, designed, and outlined the study. Park S and Sohn K undertook the article selection process, identified/ retrieved data from the articles, and independently conducted quality assessments. All authors participated in the analysis, and wrote and approved manuscript drafts.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sohn, K.J., Park, SY. & Kim, S. A scoping review of return to work decision-making and experiences of breast cancer survivors in Korea. Support Care Cancer 29, 1741–1751 (2021). https://doi.org/10.1007/s00520-020-05817-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-020-05817-y