
Abstract
Objectives
According to the Common Sense Model of self-regulation, cancer survivors construct perceptions of their illness as a (mal)adaptive mechanism. These perceptions might impact on health care use. We aimed to explore the association between illness perceptions and health care use in stage I–II endometrial cancer (EC) survivors, and whether these associations differed by time since diagnosis.
Methods
A survey was conducted in 2008 by the population-based PROFILES registry among EC survivors diagnosed between 1999 and 2007. Survivors (n = 742, 77% response) completed the Brief Illness Perception Questionnaire (BIPQ) and questions on health care use in the past 12 months. Clinical data were accessed from the Netherlands Cancer Registry. Multiple logistic regression was used to evaluate the relationship between illness perceptions and health care use.
Results
Between 15 and 22% of the survivors had negative illness perceptions. Survivors with more negative perceptions on consequences, timeline, treatment control, identity, cognitive representation, concern, emotion, and emotional representation were more likely to make ≥ 1 visit to their family physician/general practitioner in relation to their cancer when compared with survivors with more positive illness perceptions. More negative perceptions on consequences, timeline, identity, and concern were associated with ≥ 2 general or cancer-related visits to the medical specialists. The association between negative illness perceptions and health care use was more prominent among long-term (>5 years post-diagnosis) EC survivors.
Conclusions
Negative illness perceptions among EC survivors were associated with higher health care use. For individuals with maladaptive illness perceptions, visits to their health care provider may reduce worry about their illness. Future research might address the effects of intervening in maladaptive illness perceptions on use of health care in this category of survivors.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
According to the Common Sense Model (CSM) of self-regulation, individuals construct personal models or representations of illness as a (mal)adaptive mechanism when confronted with an illness [1]. These representations, cognitive and emotional, can be informed by personality, previous experience and observations, or received information of the illness and related symptoms [2]. In turn, these representations or illness perceptions could motivate subsequent self-management behaviors such as health care use [3]. Previous research in a primary care setting found that individuals with more self-reported symptoms, illness worry, emotional distress, a long timeline perspective of their illness, and a belief that experienced symptoms have a serious consequence, made more visits to their family physician/general practitioner [3]. Individuals with perceptions of poorer health were found to have higher primary health care use regardless of actual physical health as assessed by their attending physician [4]. Perceived illness susceptibility and severity, knowledge about illness, and belief in the effectiveness of self-care have been shown to be associated with health-seeking behavior [5].
Our research group has previously reported on the health care use of endometrial cancer (EC) survivors. We found that EC survivors reported more health care use in comparison with women in the general population [6]. Furthermore, survivors with shorter time since diagnosis had greater health care use related to their cancer when compared to longer-term survivors, reflecting the follow-up care according to Dutch guidelines. For a significant proportion of survivors (19%), the frequency of follow-up care exceeded recommended Dutch guidelines [7]. When stratified by time since diagnosis, overconsumption of health care was lowest in EC survivors with 1-year follow-up (13%) and highest in survivors in the 6–10 years follow-up category (27%). EC survivors who experienced more worry had greater consumption of health care use [7]. Previous study has shown that cancer survivors with higher fear of recurrence were more likely to have more outpatient visits [8]. In our recent cluster randomized controlled trial, EC survivors who were given a survivorship care plan experienced more symptoms, had more concerns about their illness, were more emotionally affected, and made more cancer-related visits to their primary care physician than survivors who were treated with usual care [9]. In contrast, a study found that cancer survivors who were provided verbal explanations of their written treatment summary and follow-up care plans reported higher levels of self-efficacy, and fewer emergency room visits and hospitalizations than those who received only written information [10]. Taken together, these results suggest that individuals’ appraisal of their health threat could play a role in help-seeking behavior.
We have not found published results on the association between illness perceptions and health care use among population-based cancer survivors. With an annual incidence of 19–25 per 100,000 women, EC is the most common gynecological cancer in the Western world [11, 12]. The incidence of EC is increasing due to an aging population and increasing obesity [13]. Also, EC is often detected early and has high 5-year survival rate of 86%, contributing to the increasing numbers of EC survivors [12, 14]. This growing number of survivors can have considerable economic impact through increased health care use [15], leading to discussions about follow-up care regimens.
Our study aims were twofold: (1) to explore the association of illness perceptions with health care use in (long-term) stage I–II EC survivors treated with curative intent, and (2) whether these associations differed by time since diagnosis. We hypothesized that (1) EC survivors with more negative illness perceptions will have higher health care use compared with survivors with more positive illness perceptions. Based on our previous study which reported that worry about health was associated with higher health care use among longer-term EC survivors [7], our second hypothesis is that the association between negative illness perceptions and health care use will be more evident among longer-term EC survivors than in shorter-term survivors.
Methods
Setting and participants
In 2008, we included women diagnosed with stage I–II EC between 1999 and 2007 in 10 hospitals in the south of the Netherlands as registered in the Netherlands Cancer Registry (NCR). The NCR records data on all individuals who are newly diagnosed with cancer in the Netherlands. Exclusion criteria included cognitive impairment, those who died prior to start of the study (according to the Central Bureau for Genealogy which collects information on all deceased Dutch citizens via the civil municipal registries, and hospital records), or had unverifiable addresses. Details of this study are reported elsewhere [6].
Ethical approval for the study was obtained from Maxima Medical Center Medical Ethics Committee in the Netherlands (reference number: 0733).
Data collection
Data collection was completed within the PROFILES registry as previously described [16]. In short, survivors were invited to participate in the study by their attending gynecologist. Eligible survivors were sent information of the study and a questionnaire. By returning a completed questionnaire in a pre-paid envelope, survivors indicated their consent to study participation and for the linkage of their questionnaire data with their clinical data registered by the NCR. Non-respondents were sent a reminder letter and questionnaire within 2 months. Survivors were reassured that non-participation had no consequences on their follow-up care or treatment. Data from PROFILES is linked directly to clinical data from the NCR and is available for non-commercial scientific research purposes (www.profilesregistry.nl), subject to study question, privacy, and confidentiality restrictions, and registration [16].
Study measures
Health care use
Four items were used to assess health care use: (1) How often did you contact a general practitioner (GP) in the past 12 months? (2) How many of these visits were related to cancer or the consequences of your cancer? (3) How often did you visit a medical specialist (MS) in the past 12 months? (4) How many of these visits were related to cancer or the consequences of your cancer? These 4 questions could be answered by filling in the number of visits. These questions were asked in a similar way as by Statistics Netherlands (http://statline.cbs.nl/Statweb/).
Illness perceptions
Respondents completed the Dutch version of the Brief Illness Perception Questionnaire (BIPQ). [17] The BIPQ has sound psychometric properties and has been used with cancer populations (www.uib.no/ipq) [18]. The BIPQ consists of 8 items: 5 items assess cognitive representations (consequences, timeline, personal control, treatment control, identity), 2 items assess emotional representations (concern, emotion), and 1 item assesses illness comprehensibility (coherence). It uses a single-item scale approach to assess perceptions on a linear 1–10 point scale. The responses of three items (personal control, treatment control, coherence) were recoded to be in the same direction as the other items for statistical analyses. Higher scores indicated more negative perceptions.
Psychological distress
Psychological distress was measured with the Hospital Anxiety and Depression Scale (HADS). It comprises 14 items, 7 each assessing anxiety and depression [19]. Items were scored on a 4-point scale, ranging from 0 to 3. Total score for each subscale was 21 and a cutoff score ≥ 8 indicated clinical levels of anxiety or depression [19, 20].
Demographics and clinical data
Self-reported demographic data included marital status and education level. Comorbid status at the time of survey was categorized according to the adapted Self-administered Comorbidity Questionnaire (SCQ) [21].
Survivors’ demographics and clinical information including date of birth, date of diagnosis, tumor grade and stage, and treatment were accessed from the NCR.
Statistical analyses
As health care use was not normally distributed, we dichotomized the four variables using median split as previously done [6]: visits to GP and visits to the MS, zero to 1 versus 2 or more; visit to GP related to cancer, zero versus 1 or more; and visit to the MS related to cancer, zero to 1 versus 2 or more.
To facilitate interpretation of results in daily clinical practice and to identify the survivors with the most negative illness perception, we dichotomized the BIPQ scores using the 75th percentile of the interquartile range (IQR) score as cutoff, as described previously [3]. BIPQ scores above the cutoff were defined as “negative.”
We derived 2 scale scores from the dichotomized BIPQ scores: cognitive and emotional representation, in line with suggestion of Broadbent et al. [17]. To determine the prevalence of survivors who scored negatively on multiple BIPQ dimensions, we summed the BIPQ dimensions categorized as negative for each subscale: cognitive representation (consequences, timeline, personal control, treatment control, identity) and emotional representation (concern, emotion) [17]. Negative cognitive representation was defined as scoring negatively on at least 3 out of 5 dichotomized cognitive dimensions, and negative emotional representation was defined as scoring negatively on 2 out of 2 of the dichotomized emotional dimensions [22]. Survivors whose scores on all items of the cognitive and emotional representation scales were below the 75% IQR cutoff, were defined as having “positive cognitive and emotional representation.”
Analysis of variance or chi-square tests, where appropriate, was used to determine differences in sociodemographic and clinical factors of the 4 groups stratified by cognitive and emotional representations (positive cognitive and emotional, negative cognitive, negative emotional, negative cognitive and emotional).
We conducted multiple logistic regression analyses to evaluate the relationship between health care use as the dependent variable and illness perceptions as the independent variable. Time since diagnosis was dichotomized as ≤ 5 years (“short-term”) and > 5 years (“long-term”). For all analyses, individual BIPQ dimensions were entered into the regression models on a continuous scale. Other independent variables included in the logistic regression models were selected a priori: age at survey, years since diagnosis, education status, number of comorbid conditions, and psychological distress. Psychological distress variables were entered into the regression models on a continuous scale.
All tests were two-sided and significant if p < 0.05. Analyses were performed using SPSS (Statistical Package for Social Sciences, Chicago, IL, USA) version 23 for Windows.
Results
Survivors’ characteristics
In all, 742 (77%) survivors completed the questionnaire. Sociodemographic and clinical details of respondents, non-respondents, and survivors with unverifiable addresses have been reported elsewhere. [6] Briefly, respondents were younger and had a higher socioeconomic status than non-respondents. No significant differences were found for the clinical factors.
Illness perceptions
The mean, median, and 75th percentile IQR of the BIPQ scores for the sample are shown in Table 1. The percentage of survivors who scored negatively on the cognitive and emotional BIPQ dimensions ranged between 15 and 22%. Twenty percent of survivors scored negatively on the coherence dimension.
The majority of survivors (83%) were classified as having positive cognitive and emotional representations (Table 2). On the prevalence of survivors with negative perceptions on multiple BIPQ items, 3% were classified as having negative cognitive representation, 8% as having negative emotional representation, and 6% had both negative cognitive and emotional representations. Survivors classified as having negative emotional representation were younger and more often had a diagnosis of depression in the past 12 months when compared with survivors who had positive illness representations. Survivors who were classified as having both negative cognitive and emotional representations were more likely to have been diagnosed with EC more recently, and had higher self-reported symptoms of anxiety and depression.
Health care use
The annual median number of visits to the GP or to the MS for general consultation was 2. For cancer-specific visits, the median was 0 to the GP and 2 for visits to the MS.
Illness perceptions and health care use
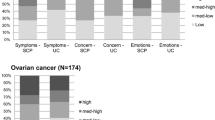
More negative illness perceptions, except for personal and treatment control, were associated with higher number of mean visits to the GP and the MS, in general or for cancer-related consultations (Fig. 1).

Mean number of visits to general practitioner (GP) and medical specialist (MS) in general (GP general, MS general) and in relation to cancer (GP cancer, MS cancer) by illness perception dimensions within the cognitive and emotional representation subscales of the Brief Illness Perception Questionnaire [17, 22]
The adjusted logistic regression models showed that survivors who made 2 or more visits to their GP in the past 12 months were more likely to have more negative perceptions of consequences and emotional representation. More negative perceptions of consequences, timeline, treatment control, identity, cognitive representation, concern, emotion, and emotional representation were associated with 1 or more cancer-related GP visits. As for general or cancer-related MS visits, more negative perceptions on consequences, timeline, identity, and concern were associated with 2 or more visits in the past 12 months (Table 3).
As the BIPQ emotional representation items assess concern and negative emotions, we reran the adjusted logistic regression models excluding psychological distress (anxiety and depression) for adjustment in the models (results not shown). Results were similar to those reported in Table 3, except that negative emotions were significantly associated with more MS visits for either general or cancer-related matters, and that the associations between personal control and cognitive representation with cancer-related MS visits became significant.
Illness perceptions and health care use, stratified by time since diagnosis
In analyses stratified by time since diagnosis, illness perceptions were not associated with general visits to the GP among EC survivors with ≤ 5 years follow-up (Table 4). Among survivors with > 5 years follow-up, only emotional representation was associated with more visits to the GP for general matters. As for visits to GP for cancer-related matters, negative illness perceptions on cognitive representation, consequences, timeline, identity, concern, and emotion were associated with more visits in both short- and long-term EC survivors. In addition, long-term EC survivors with more negative perceptions on treatment control and emotional representation were more likely to visit the GP for cancer-related matters.
With regard to MS visits, illness perceptions were, in general, not related to more visits to the MS for either general or cancer-related matters among short-term EC survivors (Table 5). In contrast, short-term EC survivors with negative emotional representation were less likely to visit the MS for cancer-related matters. Among long-term EC survivors, negative perceptions on consequences, identity, concern, and emotion were associated with more visits to the MS for general and cancer-related matters. More negative perception on coherence with lower odds of MS visits for cancer-related matter, while negative cognitive representation, timeline, and emotional representation were associated with higher odds for MS cancer-related visits among long-term EC survivors.
Sensitivity analyses were conducted excluding psychological distress in the logistic models, In general, similar patterns were noted in the association between illness perceptions and health care use among short- and long-term EC survivors as in the full models (Supplementary Tables 1 and 2).
Discussion
This study explored the association between illness perceptions and health care use stage I–II EC survivors, and whether the association varied by time since diagnosis. As hypothesized, we observed that EC survivors who had more negative illness perceptions were more likely to have higher health care use when compared with survivors with more positive perceptions. EC survivors who were younger, had a more recent cancer diagnosis, and higher levels of self-reported anxiety and depressive symptoms were more likely to have negative illness perceptions. When stratified by time since diagnosis, the association between negative illness perceptions and visits to either the GP or MS for cancer-related matters were stronger among long-term EC survivors.
Our results showed that EC survivors who were more concerned, perceived that their illness has affected their lives, perceived that their illness will have a long duration, and those with higher symptom burden were more likely to visit either the GP or MS for cancer-related matters. These results are comparable to a Danish study of primary health care use among the general population [3]. In that study, a strong illness identity, a long timeline perspective, and a belief in serious consequences of the illness were associated with higher health care use.
EC survivors who perceived that their illness has an emotional impact were more likely to visit the GP for cancer-related matters. EC survivors who had negative emotional and cognitive representations also reported higher levels of anxiety and depressive symptoms. These results are in line with previous research which suggests that for individuals with maladaptive illness perceptions, visits to their health care providers may help to reduce worry about their illness. Cancer survivors with more psychological distress incurred higher health care costs when compared with cancer survivors without psychological distress or non-cancer individuals with psychological distress [23]. Cancer survivors with higher fear of recurrence were more likely to have more outpatient visits [8]. We found that the association between illness perceptions and health care use differed by time since diagnosis, in which the association was more prominent among long-term EC survivors when compared with short-term survivors. This finding is logical as short-term survivors can expect regular follow-ups with their health care provider, thereby reducing the role of illness perceptions in seeking help. However, for long-term EC survivors who might no longer have a regular surveillance protocol according to the Dutch guidelines, negative illness perceptions could increase visits to either the GP or MS to assuage their fears about possible recurrence. Previously, our research group reported that 27% of long-term EC survivors had consumption of follow-up care above Dutch guideline, due to worry about their cancer [7]. Taken together, this implies that exploring the illness perceptions in distressed EC survivors may avoid possible somatization and also to encourage more adaptive problem solving and self-management.
In our study, 20% of survivors scored above the cutoff on the coherence item, suggesting that a significant proportion of EC survivors might not have a good understanding of their illness. Providing inadequate or insufficient information by the health care system could explain the poorer knowledge of disease. [24] Previously, we have found that EC survivors were not satisfied with information provided on treatment side effects, follow-up care, and supportive care [25]. Although we did not find an association between more negative perceptions of coherence with health care use, other studies suggest that poorer understanding of one’s illness was associated with higher health care use [26]. Providing written information regarding cancer treatment and follow-up care can improve self-efficacy [10]. In addition, cancer survivors who were provided verbal explanations of the written information reported higher levels of self-efficacy, and had fewer emergency room visits and hospitalizations than those who received only written information.
Clinical implication
The CSM is a relevant model for cancer survivorship as it considers individuals as problem solvers actively involved in the management of their own health and illness. It implies that maladaptive cognitions of cancer survivors can be addressed, through interventions, to achieve better health outcomes when they have a more adaptive understanding of their condition and are able to evaluate the effects of acting on this understanding [27]. Maladaptive illness perceptions have been shown to be amenable to intervention in other chronically ill populations. Individuals with myocardial infarction who received an illness perception intervention had significantly less worry about a future myocardial infarction and made fewer telephone calls to their GP about their heart condition at follow-up when compared with individuals without the illness perception intervention [28]. Positive changes in illness perceptions improved emotional well-being among breast cancer survivors who attended a psychosocial aftercare program [29]. Breast cancer patients who received a cognitive-behavioral stress-management intervention, designed to improve coping and psychosocial adaptation and to reduce stress and negative mood, had lower depressive symptoms and higher health-related quality life up to 15 years follow-up [30].
Study limitations
Our study is the first to assess the association of illness perceptions with health care use in a large population-based EC survivors that had a high response rate. However, there are limitations. Health care use was self-reported which raises the possibility of recall bias. We did not ask EC survivors about visits to the gynecologist in specific, but used a more general term of visit to the MS. The cross-sectional design limits possible conclusions on the causal relationship between illness perceptions and health care use. As our survey data were collected up to 9 years after diagnosis, there could have been changes in illness perceptions and health-seeking behavior which could have an influence on our results [31, 32]. Furthermore, we have no information on possible recurrence of the disease or new malignancy which could influence illness perceptions and health care use. Therefore our results, namely those reporting on difference between short- and long-term survivors, should be interpreted with caution.
In conclusion, we found that EC survivors with more negative illness perceptions were more likely to have higher health care use. Furthermore, these associations varied by time since diagnosis. Survivors classified as having negative emotional representation were younger and more often had a diagnosis of depression in the past 12 months when compared with survivors who had positive illness representations. Future research might address the effects of intervening in maladaptive illness perceptions on use of health care in this group of survivors.
References
Leventhal H, Brissette I, Leventhal EA (2003) The common-sense model of self-regulation of health and illness. In: Cameron LD, Leventhal H (eds) The self-regulation of health and illness behaviour. Routledge, London, pp 42–65
Scott SE (2010) Symptom perception and help seeking. In: French D, Vedhara K, Kaptein AA et al (eds) Health Psychology, 2nd edn. BPS Blackwell Publishing, Chichester, pp 162–174
Frostholm L, Fink P, Christensen KS, Toft T, Oernboel E, Olesen F, Weinman J (2005) The patients’ illness perceptions and the use of primary health care. Psychosom Med 67:997–1005
Connelly JE, Philbrick JT, Smith GR Jr, Kaiser DL, Wymer A (1989) Health perceptions of primary care patients and the influence on health care utilization. Med Care 27:S99–S109
Campbell SM, Roland MO (1996) Why do people consult the doctor? Fam Pract 13:75–83
Ezendam NP, Nicolaije KA, Boll D et al (2013) Health care use among endometrial cancer survivors: a study from PROFILES, a population-based survivorship registry. Int J Gynecol Cancer 23:1258–1265
Nicolaije KAH, Ezendam NPM, Vos MC, Boll D, Pijnenborg JMA, Kruitwagen RFPM, Lybeert MLM, van de Poll-Franse LV (2013) Follow-up practice in endometrial cancer and the association with patient and hospital characteristics: a study from the population-based PROFILES registry. Gynecol Oncol 129:324–331
Lebel S, Tomei C, Feldstain A, Beattie S, McCallum M (2013) Does fear of cancer recurrence predict cancer survivors’ health care use? Support Care Cancer 21:901–906
Nicolaije KAH, Ezendam NPM, Vos MC, Pijnenborg JMA, Boll D, Boss EA, Hermans RHM, Engelhart KCM, Haartsen JE, Pijlman BM, van Loon-Baelemans IEAM, Mertens HJMM, Nolting WE, van Beek JJ, Roukema JA, Zijlstra WP, Kruitwagen RFPM, van de Poll-Franse LV (2015) Impact of an automatically generated cancer survivorship care plan on patient-reported outcomes in routine clinical practice: longitudinal outcomes of a pragmatic, cluster randomized trial. J Clin Oncol 33:3550–3559
Kenzik KM, Kvale EA, Rocque GB, Demark-Wahnefried W, Martin MY, Jackson BE, Meneses K, Partridge EE, Pisu M (2016) Treatment summaries and follow-up care instructions for cancer survivors: improving survivor self-efficacy and health care utilization. Oncologist 21:817–824
(2016) http://seer.cancer.gov/statfacts/html/corp.html. Accessed on 08.04.2018
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JWW, Comber H, Forman D, Bray F (2013) Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer 49:1374–1403
Renehan AG, Tyson M, Egger M et al (2008) Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371:569–578
Siegel RL, Miller KD, Jemal A (2015) Cancer statistics, 2015. CA Cancer J Clin 65:5–29
Hayata E, Seto K, Kitazawa T, Matsumoto K, Morita M, Hasegawa T (2016) Informing health policy in Japan: a mixed-model estimation to compare the cost of illness of cervical cancer and endometrial cancer. J Obstet Gynaecol Res 42:446–456
van de Poll-Franse LV, Horevoorts N, Van Eenbergen MC et al (2011) The patient reported outcomes following initial treatment and long term evaluation of survivorship registry: scope, rationale and design of an infrastructure for the study of physical and psychosocial outcomes in cancer survivorship cohorts. Eur J Cancer 47:2188–2194
Broadbent E, Petrie KJ, Main J, Weinman J (2006) The brief illness perception questionnaire. J Psychosom Res 60:631–637
Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ (2015) A systematic review and meta-analysis of the Brief Illness Perception Questionnaire. Psychol Health 30:1361–1385
Zigmond AS, Snaith RP (1983) The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 67:361–370
Olsson I, Mykletun A, Dahl AA (2005) The Hospital Anxiety and Depression Rating Scale: a cross-sectional study of psychometrics and case finding abilities in general practice. BMC Psychiatry 5:46
Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN (2003) The Self-administered Comorbidity Questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Rheum 49:156–163
Thong MS, Kaptein AA, Vissers PA et al (2016) Illness perceptions are associated with mortality among 1552 colorectal cancer survivors: a study from the population-based PROFILES registry. J Cancer Surviv 10:898–905
Han X, Lin CC, Li C, de Moor JS, Rodriguez JL, Kent EE, Forsythe LP (2015) Association between serious psychological distress and health care use and expenditures by cancer history. Cancer 121:614–622
Husson O, Thong MSY, Mols F, Oerlemans S, Kaptein AA, van de Poll-Franse LV (2013) Illness perceptions in cancer survivors: what is the role of information provision? Psychooncology 22:490–498
Nicolaije KA, Husson O, Ezendam NP et al (2012) Endometrial cancer survivors are unsatisfied with received information about diagnosis, treatment and follow-up: a study from the population-based PROFILES registry. Patient Educ Couns 88:427–435
Ninou A, Guthrie E, Paika V, Ntountoulaki E, Tomenson B, Tatsioni A, Karagiannopoulou E, Carvalho AF, Hyphantis T, ARISTEIA-ABREVIATE Study Group members (2016) Illness perceptions of people with long-term conditions are associated with frequent use of the emergency department independent of mental illness and somatic symptom burden. J Psychosom Res 81:38–45
Wearden A, Peters S (2008) Therapeutic techniques for interventions based on Leventhal’s common sense model. Br J Health Psychol 13:189–193
Broadbent E, Ellis CJ, Thomas J, Gamble G, Petrie KJ (2009) Further development of an illness perception intervention for myocardial infarction patients: a randomized controlled trial. J Psychosom Res 67:17–23
Fischer MJ, Wiesenhaan ME, Does-den Heijer A et al (2013) From despair to hope: a longitudinal study of illness perceptions and coping in a psycho-educational group intervention for women with breast cancer. Br J Health Psychol 18:526–545
Stagl JM, Bouchard LC, Lechner SC, Blomberg BB, Gudenkauf LM, Jutagir DR, Glück S, Derhagopian RP, Carver CS, Antoni MH (2015) Long-term psychological benefits of cognitive-behavioral stress management for women with breast cancer: 11-year follow-up of a randomized controlled trial. Cancer 121:1873–1881
Lawson VL, Bundy C, Belcher J et al (2013) Changes in coping behavior and the relationship to personality, health threat communication and illness perceptions from the diagnosis of diabetes: a 2-year prospective longitudinal study. Health Psychol Res 1:e20
Dempster M, Howell D, McCorry NK (2015) Illness perceptions and coping in physical health conditions: a meta-analysis. J Psychosom Res 79:506–513
Acknowledgements
We thank all survivors and their doctors for their participation in the study.
Disclaimer
The funding sources were neither involved in the collection, interpretation, and analysis of the data, nor in the decision for the writing and submission of this report for publication.
Funding
The present research is financially supported in part by a Social Psychology Fellowship from the Dutch Cancer Society to Dr. Nicole Ezendam (UVT 2014-6632). Data collection for this study was funded by the Netherlands Comprehensive Cancer Organisation, Eindhoven, The Netherlands; the Center of Research on Psychology in Somatic diseases (CoRPS), Tilburg University, The Netherlands; and an investment subsidy (#480-08-009) of the Netherlands Organization for Scientific Research (The Hague, The Netherlands).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
ESM 1
(DOCX 18 kb)
Rights and permissions
About this article

Cite this article
Thong, M.S.Y., Mols, F., Kaptein, A.A. et al. Illness perceptions are associated with higher health care use in survivors of endometrial cancer—a study from the population-based PROFILES registry. Support Care Cancer 27, 1935–1944 (2019). https://doi.org/10.1007/s00520-018-4451-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-018-4451-3