
Abstract
Objective
The present study was designed to validate the Hindi version of the Multidimensional Fatigue Inventory-20 (MFI-20) in Indian oncology population.
Methods
The original English version of the MFI-20 was translated into Hindi (hMFI-20) using the translation and back translation processes. The hMFI-20 was administered to 200 cancer patients. The item analysis for hMFI-20 was carried out using the corrected item-total correlation. The confirmatory factor analysis (CFA) was employed to test whether the original factor structure of MFI-20 is confirmed for the hMFI-20. Further, convergent and discriminant validities were also tested. The reliability of the hMFI-20 was evaluated by computing composite reliability and Cronbach’s α coefficient.
Results
Corrected item-total correlation value for each of the items of hMFI-20 was greater than 0.6. Results of the CFA (comparative fit indices (CFI) = 0.91, root mean squared residual (RMR) = 0.04, root mean square error of approximation (RMSEA) = 0.028, and χ 2 = 45.68, p > 0.05) indicated that the five-factor model provided a good fit to the data. The findings indicated that hMFI-20 has a good convergent (composite reliability (CR) >0.7; average variance extracted value (AVE) >0.5) and discriminant (maximum shared variance (MSV) < AVE; average shared variance (ASV) < AVE; square root of AVE > inter-factor correlations) validities. The Cronbach’s α coefficient for the total hMFI-20 was 0.8 and was more than 0.7 for each of the five factors.
Conclusions
We conclude that the hMFI-20 has a high internal consistency and reasonable construct validity. Therefore, the hMFI-20 is a reliable and valid tool to assess the multidimensional fatigue in Indian oncology population. However, we recommend further validation of hMFI-20 in population of cancer patients of different linguistic settings and regions of India.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Measuring fatigue is important as it is usually associated with the diagnosis, stage, and treatment modalities of the disease [1–10] and can be adequately performed with a self-report scale. The magnitude of fatigue varies among cancer patients between 17 and 95 % depending upon the types of methods used for its measurement [8]. It has been reported that the higher the level of fatigue, the lower are the health-related quality of life (HrQoL) and general well being of cancer patients [1, 11–13]. Fatigue can be used as an indicator of a health problem as has been reported in the case of myocardial infarction [14]. Furthermore, it can also be considered as an indicator of treatment outcome [15]. It has been unequivocally accepted that fatigue evaluation is an interesting and promising area of research [16]. Omitting its measurement may lead to incomplete evaluation of treatment outcomes.
Numerous one-dimensional and multi-dimensional inventories have been developed for the assessment of fatigue [17–19]. Among those, the Multidimensional Fatigue Inventory-20 (MFI-20), developed by a Dutch research group [18], is widely used to measure fatigue in cancer patients [20]. The MFI-20 is a self-report assessment tool capable of measuring several dimensions of fatigue, such as general fatigue (GF), physical fatigue (PF), mental fatigue (MF), reduced motivation (RM), and reduced activity (RA). A higher score obtained using MFI-20 always reflects an elevated level of fatigue. The psychometric properties of this inventory have been tested at the time of its development in human subjects as diverse as cancer patients receiving radiotherapy, patients with the chronic fatigue syndrome, psychology students, medical students, army recruits, and junior physicians [18]. The MFI-20 has also been translated into other languages by the native investigators and tested for its robustness across cross-cultural settings [21–24].
In India, neither an independently developed construct nor a translated version of any existing constructs to measure fatigue of cancer patients is available. Therefore, in the present study, we thought it worthwhile to translate the original English version of the MFI-20 [18] into one of the Indian vernaculars, i.e., Hindi, the most of the Indians speak. We hypothesized that the translated version (Hindi MFI-20, hereafter hMFI-20) will be equally effective in measuring fatigue through testing its reliability and validity in a sample of cancer patients mainly drawn from the southeastern region of India.
Methods
Patient sample
Newly diagnosed 200 cancer patients of southeastern region of India, visiting the outdoor patient department (OPD) of the Regional Cancer Center (RCC), Pt. J.N.M. Medical College, Dr. B.R. Ambedkar Memorial Hospital, Raipur, Chhattisgarh, were selected. Firstly, the patient selection was based on inclusion criteria. Thereafter, the final selection was undertaken on the basis of the written consent given by the eligible patients. This strategy falls in the category of probability sampling especially because occurrence of a consenting patient in a group is a random phenomenon [25]. Detailed information on socio-demographics, anthropometrics and clinical characteristics were obtained for each patient.
The study obtained ethics approval of the Institutional Ethics Committee for Human Research of the Pt. Ravishankar Shukla University, Raipur, India.
Study design
The study was carried out using a cross-sectional study design. Each cancer patient completed the questionnaire once only.
Inclusion criteria
The inclusion criteria were (i) patients with good communication skill in Hindi, (ii) age range 25–50 years, (iii) diagnosis not more than 1 year, (iv) recipients of ≤ one cycle of chemotherapy, and (v) in good general conditions with Karnofsky performance status (KPS) ranging between 100 and 80 [26]. The 100 % KPS score implies that the patient is in normal condition without any complaints; whereas, 0 % means death of the patient [27].
Procedure
Inventory (MFI-20)
A prior permission (through email) for translation and validation of the original English version of MFI-20 was obtained from the author [18]. The MFI consists of 20 items. The inventory is divided in to five dimensions, such as GF (item numbers 1, 5, 12, 16), PF (item numbers 2, 8, 14, 20), MF (item numbers 7, 11, 13, 19), RA (item numbers 3, 6, 10, 17), and RM (item numbers 4, 9, 15, 18). Response to each item is measured on a scale of 1–5; thus, a maximum score of 20 could be obtained for each dimension.
Translation procedure
The original English version of MFI-20 was validated in Hindi using translation and back translation processes adopted by Tian and Hong [21]. In the first step, the original English version of the MFI-20 was translated into Hindi by two bilingual university teachers. In the second step, translated version of MFI-20 was back translated in English by two other bilingual university teachers. In the third step, the back-translated English version of MFI-20 was compared with its original English version to test the consistency. The final version of hMFI-20 was obtained following removal of the discrepancies between the translated and back-translated versions. This was achieved through unequivocal consensus.
Administration of Hindi version of MFI-20
The hMFI-20 was administered to the cancer patients (N = 200), when they visited the outdoor patient department (OPD) of the RCC for consultation. Data collection was carried out between February–April 2014. The patients were assured that their responses will be kept confidential and will never be shared with others. They were advised to give their honest response on each item.
Data analyses
Item analysis
Item analysis for hMFI-20 was carried out using the item-total correlation test. In compliance with the cutoff value reported by Hair et al. [28], we retained an item in the instrument with the corrected item-total correlation equal to or greater than 0.6.
Confirmatory factor analysis
Confirmatory factor analysis (CFA) was used to test whether the original factor structure of MFI-20 is confirmed for the translated version. Further, the fitness of model with the data was evaluated by computing the absolute and comparative fit indices (CFI). Absolute fit indices include chi-square goodness-of-fit, root mean squared residual (RMR), and root mean square error of approximation (RMSEA). A good model fit was ascertained with a lower chi-square value at p > 0.05 [29]. It was further substantiated by RMR and RMSEA values less that 0.05 [30] and 0.08 [31], respectively. In addition, a value greater than 0.9 for CFI was considered to be the good fit [32].
Construct validity
A valid and reliable construct is expected to have the following characteristics: (a) it should represent all associated observations and alternative measures and (b) it should also be relevant to other constructs of interest [33]. Of the three types of validity, namely content, construct, and criterion, in this study, we chose construct validity that includes both convergent and discriminant validity, and it was assessed using CFA.
Convergent validity
It is always important to gauge relationship among measures of the same construct. We measured this using convergent validity and tested the magnitude of relationship between the items and their latent factor [34].
Convergent validity of the hMFI-20 was evaluated and considered to be confirmed on the basis of (a) standardized regression coefficient (β) of each item (>0.5), (b) composite reliability (CR > 0.7), and (c) average variance extracted value (AVE > 0.5) of each factor [28, 35, 36]. These tests therefore complement results of the convergent validity. With reference to regression coefficient, items of the scale are independent predictors of the outcome variables, such as GF, PF, MF, RA, and RM.
Discriminant validity
Discriminant validity indicates the degree of correlation between paired factors in the same scale [37]. We tested and confirmed the discriminant validity on the basis of (a) maximum shared variance (MSV < AVE), (b) average shared variance (ASV < AVE), and (c) square root of AVE greater than inter-factor correlations [28].
Construct reliability
Construct reliability of the hMFI-20 was considered to be confirmed on the basis of composite reliability (CR >0.7) [36].
Internal consistencies
The internal consistencies of the hMFI-20 were evaluated by computing Cronbach’s α coefficient [38]; a value greater than 0.7 was considered fairly reliable.
Descriptive statistics, corrected item-total correlation, and internal consistency were computed using SPSS (version 16). CFA was carried out with the help of SPSS AMOS (version 22). CR, AVE, MSV, ASV, and square root of AVE were calculated using stats tool package. In this study, we rejected all statistical hypotheses at p ≤ 0.05.
Results
Socio-demographic, anthropometric, and clinical characteristics of 200 cancer patients, consisting of 100 males and 100 females, are summarized in Table 1. The mean age of the sample was 42.1 years with the averages for male and female patients, respectively, were 42.7 and 41.5 years. While all male patients were suffering from cancer in head and neck region, 50 % female patients were suffering from cervical cancer and the remaining from breast cancer. Educational background of the most of the patients (96 %) was below the graduation level. Of the total patients, 146 (73 %) were inhabitants of rural areas and 54 (27 %) were from urban areas of Chhattisgarh. The evaluation of Karnofsky performance status of all patients indicated that all of them were in good condition. Of the 200 patients, 49.5 % received one cycle of chemotherapy; whereas, the remaining 50.5 % did not receive any cycle of chemotherapy at the time of the study (Table 1).
Item analysis
Corrected item-total correlation
The corrected item-total correlation coefficient for each of the items of hMFI-20 was greater than 0.6 (Table 2). Therefore, all 20 items were retained in the instrument for further analysis.
Confirmatory factor analysis
Prior to conducting CFA, it is a prerequisite to test the multivariate normality for the data by computing z-statistic [39]. According to Bentler [40], normality is confirmed when z-statistic is less than 5. We proceeded with the testing of the hypothesized model especially since we obtained z-statistic less than 5.0 in our case.
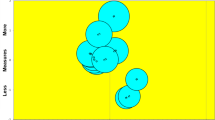
Results of CFA indicated that there is a significant standardized estimate (β) of all the items on their respective factors and specifically, the values of β ranged from 0.75 to 0.85 for GF, from 0.7 to 0.81 for PF, from 0.7 to 0.87 for MF, from 0.76 to 0.92 for RA, and from 0.77 to 0.95 for RM. However, relationships among the factors were insignificant, confirming that all the five factors are empirically distinct from each other (Fig. 1).

Factorial validity of the translated Hindi version of the Multidimensional Fatigue Inventory-20
We found that the hypothesized model has a good fitting for our data. The validity of this statement was based on the following indicators: the chi-square was not significant (χ 2 = 45.68, p > 0.05), the comparative fit index was higher than 90 % (CFI = 0.91), root mean square residual was less than 0.05 (RMR = 0.04), and root mean square error of approximation was less than 0.08 (RMSEA = 0.028) (Table 3).
Construct validity
Convergent validity
In the present study, β ranged from 0.70 to 0.95 for all five factors of hMFI-20 (Fig. 1). Further, CR and AVE values were greater than 0.7 and 0.5, respectively, for each of the five factors (Table 4). These findings indicated that hMFI-20 has a good convergent validity.
Discriminant validity
The values of MSV (range 0.03–0.04) and ASV (range 0.01–0.03) of each of the five factors of hMFI-20 were less than the AVE (Table 4). Further, square root of AVE value was greater than the correlations involving the factors of hMFI-20 (Table 4). These results indicated that the hMFI-20 has good discriminant validity.
Construct reliability
The composite reliability (CR) for each factor was higher than 0.6 (ranged between 0.84 and 0.91).
Internal consistency
The Cronbach’s α coefficient for the entire hMFI-20 scale was 0.8. The coefficients for all factors were also computed, and the values were found to be greater than 0.7 (0.81 for GF, 0.82 for PF, 0.81 for MF, 0.75 for RA, and 0.8 for RM). All coefficients were statistically significant at p < 0.001.
Discussion
In this study, we examined the validity and reliability of the Hindi version of the MFI-20. Reasons for our endeavor are justified because of the following: (1) in India, not a single construct equivalent to MFI-20 is available, in any vernacular languages, to measure the magnitude of fatigue in cancer patients; and (2) the MFI-20 is one of the most reliable and globally accepted and validated construct for the purpose. It is indeed difficult to imagine how the oncologists are measuring the magnitude of fatigue in the large population of cancer patients in India without the availability of a comparable construct.
Fatigue is a common consequence of cancer and many other chronic and acute diseases. The measurement of fatigue is not simple, and no such objective approach has yet been developed to accomplish measurement of fatigue among Indian cancer patients. The current approach to measure fatigue in the population of cancer patients is based on subjective paradigm. To the best of our knowledge and belief, the English version of the MFI-20 is the most ideal subjective tool to measure fatigue among cancer patients and survivors of cancer. The MFI-20 is multidimensional in nature with social, psychological, and physiological aspects. It has been translated into many different languages for the assessment of fatigue in diverse group of subjects [21–23, 41]. The hMFI-20 was constructed following the established procedures of the scale development [21, 33]. The reliability and validity were checked by administering the hMFI-20 inventory in a large sample of cancer patients (n = 200). The subjects responded to all the items of the hMFI-20, and there was no missing data. This indicates that they fully comprehended all items of the inventory.
The corrected item-total correlations for all items of hMFI-20 ranged between 0.62 and 0.80. This indicates that all items of the five factors were in an acceptable range as reported by Hair et al. [28] and therefore, retained in the instrument.
Subsequently, the five-factor model was tested by CFA through a structural equation modeling approach to check whether the assumptions of the dimensions of the model fit our data of cancer patients. The results confirmed the assumptions of the dimensionality and corroborate with the observations reported earlier [21, 22, 42]. The findings of CFA emanated from our study also complemented multidimensionality of the original five-factor model related to MFI-20. In addition, values of the absolute and comparative fit indices indicated and supported a good model fit to the data. In the present study, the cutoff point for these indices related to the model was comparable with those reported by Hair et al. [28], Barrett [29], Byrne [30], MacCallum et al. [31], Hu and Bentler [32]. Numerous researchers have also confirmed the criteria of model fit for all these indices for other constructs [43–45].
Further, our results indicate that hMFI-20 has good convergent and discriminant validities. Resultant higher values of AVE of each factor with regard to its correlation with other factors confirmed the convergent validity of hMFI-20. Similarly, discriminant validity was established on the basis of maximum shared variance (MSV < AVE), average shared variance (ASV < AVE), and square root of AVE greater than inter-factor correlations. Our results on discriminant validity are in agreement with the criteria laid down by Hair et al. [28].
Furthermore, the estimated values for construct reliability computed as composite reliability of each of the factors of hMFI-20 were more (range 0.84–0.91) than 0.7 [36]. This implied that the inventory has good reliability. Cronbach’s α coefficients were in the good range, and the values of inter-correlations for all factors ranged between 0.75 and 0.82. Our observations are comparable with the findings reported earlier [18, 20, 22, 42, 46]. These findings strengthen our assumption that the hMFI-20 is a reliable inventory and could be used to assess fatigue level in Indian cancer patients. Furthermore, the hMFI-20 also does not suffer from any item redundancy, and the factors are capable of measuring assumptions of the multidimensional fatigue in cancer patients independently and fairly accurately.
Strengths and limitations
The strength of the study includes the following: (1) adequate sample size was selected randomly from cross-sectional oncology population, (2) the responses on the inventory were complete, (3) there were no instances of missing data either on the inventory or in the biographical information input, and (4) each of the factors was adequate with their respective items. The hMFI-20 was well accepted by our sample of oncology population.
However, the limitations of the present study are the following: (1) “criterion-related validity” was not performed through determining correlation between the hMFI-20 and other available measures, (2) criterion validity was not determined using groups with different levels of fatigue, (3) test-retest reliability of the hMFI- 20 was not conducted, (4) differences in responsiveness to multiple treatments along a longitudinal time scale was not examined, and (5) lack of universality. The responses and acceptability might differ when the study design will be implemented to oncology population of India in different regions with diverse cultures and different native languages.
Conclusion
In conclusion, the Hindi version of MFI-20 (hMFI-20) has a high internal consistency and reasonable construct validity. Thus, the hMFI-20 with valid factor structure is a reliable and convincing tool to assess the multidimensional fatigue in Indian oncology population. We have a hunch that the hMFI-20 may yield inconsistent results when it is used on cancer patients of other regions of India. Therefore, we recommend that testing of MFI-20 should be carried out on cancer patients along different linguistic settings and regions of the Indian subcontinent with about 20 different officially recognized languages and diverse culture. It is also desirable to conduct further extensive study to test the validity of the hMFI-20 obtaining responses, along a longitudinal time scale, from patients receiving multiple treatments. Such an endeavor will certainly substantiate the strengths and merits of the hMFI-20 along with its parent English version. On the basis of our results, we suggest that hMFI-20 may be used as one of the tools to assess the cancer-related fatigue in clinics. The hMFI-20 will enable the clinicians to plan the treatment strategy for fatigue management, in addition to cancer treatment.
References
Smets EMA, Garssen B, Schuster-Oitterhoeve ALJ, De Haes JCJM (1993) Fatigue in cancer patients. Br J Cancer 68:220–224
Smets EMA, Garssen B, Cull A, de-Haesl JCJM (1996) Application of the multidimensional fatigue inventory (MFI-20) in cancer patients receiving radiotherapy. Br J Cancer 73:241–245. doi:10.1038/bjc.1996.42
Richardson A, Ream E, Wilson-Barnett J (1998) Fatigue in patients receiving chemotherapy: patterns of change. Cancer Nurs 21:17–30. doi:10.1097/00002820-199802000-00003
Richardson A (1998) Measuring fatigue in patients with cancer. Support Care Cancer 6(2):94–100. doi:10.1007/s005200050141
Schwartz AL, Nail LM, Chen S, Meek P, Barsevick AM, King ME, Jones LS (2000) Fatigue patterns observed in patients receiving chemotherapy and radiotherapy. Cancer Invest 18(1):11–19. doi:10.3109/07357900009023057
Lin CC, Chang AP, Chen ML, Cleeland CS, Mendoza TR, Wang XS (2006) Validation of the Taiwanese version of the brief fatigue inventory. J Pain Symptom Manag 32(1):52–59. doi:10.1016/j.jpainsymman.2005.12.019
Butt Z, Rosenbloom SK, Abernethy AP, Beaumont JL, Paul D, Hampton D, Jacobsen PB, Syrjala KL, Von Roenn JH, Cella D (2008) Fatigue is the most important symptom for advanced cancer patients who have had chemotherapy. J Natl Compr Canc Netw 6(5):448–455
Giacalone A, Polesel J, De Paoli A, Colussi AM, Sartor I, Talamini R, Tirelli U (2010) Assessing cancer-related fatigue: the psychometric properties of the revised piper fatigue scale in Italian cancer inpatients. Support Care Cancer 18:1191–1197. doi:10.1007/s00520-009-0741-0
Ryan JL, Carroll JK, Ryan EP, Mustian KM, Fiscella K, Morrow GR (2007) Mechanisms of cancer-related fatigue. Oncologist 12(1):22–34. doi:10.1634/theoncologist.12-S1-22
Stone P, Richards M, A’Hern R, Hardy J (2000) A study to investigate the prevalence, severity and correlates of fatigue among patients with cancer in comparison with a control group of volunteers without cancer. Ann Oncol 11(5):561–567. doi:10.1023/A:1008331230608
Annunziata MA, Muzzatti B, Mella S, Bidoli E (2013) Fatigue, quality of life, and mood states during chemotherapy in Italian cancer patients. Tumori 99(1):e28–e33. doi:10.1700/1248.13808
Curt GA, Breitbart W, Cella D, Groopman JE, Horning SJ, Itri LM, Johnson DH, Miaskowski C, Scherr SL, Portenoy RK, Vogelzang NJ (2007) Impact of cancer-related fatigue on the lives of patients: new findings from the fatigue coalition. Oncologist 5(5):353–360. doi:10.1634/theoncologist.5-5-353
Gupta D, Lis CG, Grutsch JF (2007) The relationship between cancer-related fatigue and patient satisfaction with quality of life in cancer. J Pain Symptom Manag 34(1):40–47. doi:10.1016/j.jpainsymman.2006.10.012
Appels A, Mulder P (1998) Excess fatigue as a precursor of myocardial infarction. Eur Heart J 9:758–764. doi:10.1093/eurheartj/9.7.758
Fawzy FI, Cousins N, Fawzy NW, Kemeny ME, Elashoff R, Morton D (1990) A structured psychiatric intervention for cancer patients. Arch Gen Psychiatry 47:720–725. doi:10.1001/archpsyc.1990.01810200037005
Lis CG, Rodeghier M, Grutsch JF, Gupta D (2009) Distribution and determinants of patient satisfaction in oncology with a focus on health related quality of life. BMC Health Serv Res 9:190. doi:10.1186/1472-6963-9-190
Pearson PG, Byars GE (1956) The development and validation of a checklist measuring subjective fatigue. Report: 56–115, Randolph Air Force Base, Tex.: Air University, School of Aviation Medicine, USAF
Smets EM, Garssen B, Bonke B, De Haes JC (1995) The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res 39:315–325. doi:10.1016/0022-3999(94)00125-O
Chang YJ, Lee JS, Lee CG, Lee WS, Lee KS, Bang SM, Wang XS, Mendoza TR, Cleeland CS, Yun YH (2007) Assessment of clinical relevant fatigue level in cancer. Support Care Cancer 15(7):891–896. doi:10.1007/s00520-007-0219-x
Hagelin CL, Wengström Y, Runesdotter S, Fürst CJ (2007) The psychometric properties of the Swedish Multidimensional Fatigue Inventory MFI-20 in four different population. Acta Oncol 46:97–104. doi:10.1080/02841860601009430
Tian J, Hong JS (2012) Validation of the Chinese version of Multidimensional Fatigue Inventory-20 in Chinese patients with cancer. Support Care Cancer 20:2379–2383. doi:10.1007/s00520-011-1357-8
Lin JS, Brimmer DJ, Maloney EM, Nyarko E, Belue R, Reeves WC (2009) Further validation of the Multidimensional Fatigue Inventory in a US adult population sample. Popul Health Metr 15(7):18. doi:10.1186/1478-7954-7-18
Gentile S, Delaroziere JC, Favre F, Sambuc R, San Marco JL (2003) Validation of the French Multidimensional Fatigue inventory (MFI 20). Eur J Cancer Care 12:58–64. doi:10.1046/j.1365-2354.2003.00295.x
Munguía-Izquierdo D, Segura-Jiménez V, Camiletti-Moirón D, Pulido-Martos M, Alvarez-Gallardo IC, Romero A, Aparicio VA, Carbonell-Baeza A, Delgado-Fernández M (2012) Multidimensional Fatigue Inventory: Spanish adaptation and psychometric properties for fibromyalgia patients. The Al-Andalus study. Clin Exp Rheumatol 30:94–102
Hsia J (2014) Probability sampling. Wiley StatsRef: Statistics Reference Online
Karnofsky DA, Burchenal JH (1949) The clinical evaluation of chemotherapeutic agents in cancer. In: MacLeod CM (ed) Evaluation of chemotherapeutic agents. Columbia University Press, New York, p 196
Mor V, Laliberte L, Morris JN, Wiemann M (1994) The Karnofsky performance status scale. An examination of its reliability and validity in a research setting. Cancer 53:2002–2007. doi:10.1002/1097-0142(19840501)53:93.0.CO;2-W
Hair J, Black W, Babin B, Anderson R (2010) Multivariate data analysis, 7th edn. Prentice-Hall, Inc, Upper Saddle River
Barrett P (2007) Structural equation modelling: adjudging model fit. Personal Individ Differ 42:815–824. doi:10.1016/j.paid.2006.09.018
Byrne BM (1998) Structural equation modeling with LISREL, PRELIS and SIMPLIS: basic concepts, applications and programming. Lawrence Erlbaum Associates, Mahwah
MacCallum RC, Browne MW, Sugawara HM (1996) Power analysis and determination of sample size for covariance structure modeling. Psychol Methods 1:130–149. doi:10.1037/1082-989X.1.2.130
Hu LT, Bentler PM (1995) Evaluating model fit. In: Hoyle R (ed) Structural equation modeling: concepts, issues, and applications. Thousand Oaks, Sage, pp 76–99
Nunnally JC, Bernstein IH (1994) Psychometric theory, 3rd edn. McGraw-Hill, New York
Holmes-Smith P, Cunningham E, Coote L (2006) Structural equation modelling: from the fundamentals to advanced topics. Sream and Statsline, Melbourne
Ghadi I, Alwi NH, Abu Bakar K, Talib O (2012) Construct validity examination of critical thinking dispositions for undergraduate students in university Putra Malaysia. High Educ Stud 2:138–145. doi:10.5539/hes.v2n2p138
Fornell C, Larcker DF (1981) Evaluating structural model with unobserved variables and measurement errors. J Mark Res 18:39–50. doi:10.2307/3151312
Kline RB (2005) Principles and practice of structural equation modeling, 2nd edn. The Guilford Press, New York
Cronbach LJ (1990) Essentials of psychological testing, 5th edn. Harper and Row, New York
Byrne BM (2010) Structural equation modeling with AMOS: basic concepts, applications, and programming. Routledge, New York
Bentler PM (2005) EQS 6 structural equations program manual. Multivariate Software, Encino
Lundh HC, Wengstrom Y, Runesdotter S, Furst CJ (2007) The psychometric properties of the Swedish Multidimensional Fatigue Inventory MFI-20 in four different populations. Acta Oncol 46:97–104. doi:10.1080/02841860601009430
Stein KD, Jacobsen PB, Blanchard CM, Thors C (2004) Further validation of the Multidimensional Fatigue Symptom Inventory-Short Form. J Pain Symptom Manag 27:14–23. doi:10.1016/j.jpainsymman.2003.06.003
Yusoff MSB (2011) Psychometric properties of the learning approach inventory: a confirmatory factor analysis. Educ Med J 3:e24–e31. doi:10.5959/eimj.3.2.2011.or3
Hafiz B, Shaari JAN (2013) Confirmatory factor analysis (CFA) of first order factor measurement model-ICT empowerment in Nigeria. Int J Busi Manag Adm 2:081–088
Bonham VL, Sellers SL, Woolford S (2014) Physicians’ knowledge, beliefs, and use of race and human genetic variation: new measures and insights. BMC Health Serv Res 14:456. doi:10.1186/1472-6963-14-456
Schwarz R, Krauss O, Hinz A (2003) Fatigue in the general population. Onkologie 26:140–144. doi:10.1159/000069834
Acknowledgments
This study was supported by the University Grants Commission, New Delhi, through its DRS-Special Assistance Program sanctioned to the School of Life Sciences, Pt. Ravishankar Shukla University, Raipur, in the thrust area “Chronobiology.” We are grateful to Prof. A.K. Pati, School of Life Sciences, Pt. Ravishankar Shukla University, Raipur, for the valuable suggestions and for reviewing the manuscript. We thank two anonymous reviewers for offering numerous constructive suggestions. We are thankful to all cancer patients for their voluntary participation in the present study.
Conflicts of interest
None of the funding source influenced the study design, collection, analysis, interpretation of data, and decision to submit the manuscript. We state that we have had full access to all the data in the study and that we agree to allow the journal to review our data if requested.
Disclosures
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chandel, P., Sultan, A., Khan, K.A. et al. Validation of the Hindi version of the Multidimensional Fatigue Inventory-20 (MFI-20) in Indian cancer patients. Support Care Cancer 23, 2957–2964 (2015). https://doi.org/10.1007/s00520-015-2661-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-015-2661-5