
Abstract
Purpose
Our aim was to determine the efficacy and quality of life outcomes of head and neck (HN) stereotactic body radiotherapy (SBRT) in a palliative population with significant proportions of de novo HN tumors not amenable to surgery or protracted course of curative radiotherapy (RT).
Methods
A retrospective review of a prospective database identified 21 patients with 24 sites that were treated. Patients were treated with intensity modulated RT (IMRT), usually 7–9 static fields with a 2–3-mm margin from gross tumor volume to planning target volume only with no microscopic margin added. Electronic patient records and treatment plans were reviewed. Basic demographic information was collected. The EORTC QLQ-H&N35 questionnaire was the tool used to collect QOL data both pre- and on-treatment fraction 5. Univariate analysis was performed for predictors of local control (LC) and prognostic factors for overall survival (OS).
Results
A total of 21 patients had 24 sites that were treated. The median age was 87 (range 25–103) and median KPS was 70. The most common histology was squamous cell carcinoma (SCC) 19/24 (79 %), basal cell carcinoma (BCC) 3/24 (16 %), and melanoma (4 %). The median maximal diameter was 3.7 cm (range 1–10 cm). The most commonly treated site was lymph nodes in the neck 13/24 (54 %), skin 8/24 (33 %), 4/24 (16 %) other HN mucosal primary sites. Of the 24 lesions, 17 (71 %) were de novo, without prior treatment and 7/24 (29 %) were recurrent. The most commonly used dose/fraction (fx) was 40 Gy/5 (fx) (range 35/5fx−48/6fx). Of the 24 lesions, 6 (25 %) had complete response, 16/24 (67 %) had partial response, and 2/24 (8 %) had no response. Control was defined as no further progression after treatment. For the entire cohort, LC at 3, 6, and 9 months were 66, 50, and 33 %, respectively. In the de novo group, 2/16 (12.5 %) had local failures with the LC rate of 94, 94, and 87 % at 3 months, 6 months, and 1 year, respectively. In the recurrent group, 4/8 (50 %) had failure with LC rates of 87. 5, 62.5, and 50 % at 3 months, 6 months, and 1 year, respectively. Of the 21 patients, 10 died during follow up, with the OS rate at 3 months, 6 months, and 1 year of 90, 70, and 60 %, respectively. Being defined “de novo” showed a trend toward statistical significance p = 0.046 for local failure. Overall survival did not show significant difference between de novo and recurrent with a p value of 0.267. No significant prognostic variables for OS were found. Pre-treatment QOL scores for the entire cohort were 53/130 versus 38/130 (lower scores indicating better QOL) scores with a trend toward statistical significance p = 0.05.
Conclusions
SBRT is efficacious with improved quality of life within this elderly frail population in the treatment of de novo and recurrent tumors of the head and neck with promising quality of life scores.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The treatment of head and neck cancers has typically involved a protracted course of chemoradiation with significant acute toxicity. Patients who were medically unfit or frail were treated with palliative radiotherapy. However palliative doses were associated with poor local control which resulted in significant symptom burden with tumor progression. Barnes et al. [1] utilized a palliative radiotherapy (RT) regimen of 2,400 cGy in three fractions on days 0, 7, and 21, which was associated with a response rate of 58.1 % and alleviation of symptoms in 61.3 % of patients for non-melanoma skin cancer. The rationale behind stereotactic body radiotherapy (SBRT) is that it has the potential to limit toxicity and complications to normal tissues through precise dose delivery utilizing real-time conformal imaging [2]. With the advent of SBRT, high precision delivery of 2–6 times more the biologically equivalent dose is possible resulting in greater local control. The capacity to deliver radiation in larger doses over a shorter time course renders benefits in terms of reduced treatment burden through fewer hospital visits, which is critical for patients of significant old age or ill health [3–6]. In the palliative setting, when compared to the standard conventional treatment, SBRT may be more effective in tumor control [7, 8] and with fewer side effects.
SBRT is increasingly becoming a common treatment option for patients with head and neck cancers although predominantly in the salvage (previously radiated) setting [8–16] where conventional radiotherapy regimens for re-irradiation are often protracted fractionation schedules (sometimes twice a day) that are not desirable in the palliative setting and still can result in unacceptably high complication rates of up to 40 % [17]. Thus, SBRT has gained popularity as a treatment for this cohort of patients [14, 18]. There are relatively few studies investigating the use of SBRT in the de novo setting where patients are unable to tolerate toxicities associated with standard curative fractionation schemes, but could receive a short SBRT course with more durable local control over standard palliative fractionations but with lesser toxicities [1]. Most series published to date are comprised of mostly recurrent patients, with only small proportions of de novo patients. Our series has the largest number of de novo patients of any published series. Kodani et al. [19] published a study evaluating the efficacy and safety of SBRT for 34 patients with head and neck tumors where 21 had prior radiotherapy and the remaining 13 received SBRT as primary treatment. The prescribed dose ranged from 19.5 to 42 Gy (median, 30 Gy) in 3–8 fractions for consecutive days. For those patients receiving SBRT as primary treatment, the complete response rate was 38 % with no high grade acute or long term toxicities. However, six patients, all of whom received previous RT, suffered severe late complications including normal tissue necrosis and incidences of carotid blowout. Siddiqui et al. [13] also included a small group of patients whom were treated with SBRT. In this study, their 44 patients were divided into three groups: those with primary (n = 10), recurrent (n = 21), and metastatic tumors (n = 13). Radiation doses were either single fraction 13–18 Gy or 36–48 Gy in five to eight fractions. Overall, a 77 % response rate was noted. Tumor control rates at 1 year were 83.3 and 60.6 % in the primary and recurrent groups, respectively.
Taken together, it would seem these results of small patient cohorts show promise for SBRT as a treatment modality. However, further quality of life (QOL) data is needed. QOL is of paramount importance in a group of patients where the goal is palliation of symptoms. The objective of this study was to determine the efficacy of head and neck stereotactic body radiotherapy in a palliative population not amenable to surgery or protracted course of curative radiotherapy (RT) and to explore quality of life parameters pre- and post-treatment.
Methods
A retrospective study was conducted over a prospective database. In order to be included in the study, patients were required to have undergone intensity modulated radiation therapy (IMRT), using 7–9 static fields with a 2–3-mm margin from gross tumor volume to planning target volume only with no microscopic margin added. Patients were also required to have completed the European Organization of Research and Treatment of Cancer Quality of Life-Head and Neck module (EORTC QLQ-H&N35) on the first day of treatment and at treatment fraction 5.
Electronic patient records and treatment plans were reviewed to collect data on patient demographic factors, and treatment factors, including toxicity from treatment, local control rates, and overall survival. Univariate analysis was performed for predictors of local control (LC) and prognostic factors for overall survival (OS). We were unable to assess local control and survival rates using the Kaplan-Meier method; therefore, we compared overall survival and local control means for each group.
The EORTC QLQ-H&N35 is a validated quality of life tool to be used alongside the EORTC QLQ-C30 general cancer quality of life questionnaire to assess quality of life in patients with head and neck cancer [20]. The QLQ-H&N35 is comprised of questions specifically for head and neck cancer patients, with seven multi-item scales that assess pain, swallowing, senses, speech, social eating, social contact and sexuality, and eleven single items. A higher score indicates worse quality of life and greater symptom severity.
Results
A total of 21 patients with 24 treated sites were included in this study. The median age of the patients was 87 years old (range 25–103) and the median KPS was 70. The most common histologies were squamous cell carcinoma (SCC) (79 %), basal cell carcinoma (BCC) (17 %), and melanoma (4 %). The median maximal diameter of the lesion was 3.7 cm (range 1–10 cm). Most commonly treated sites were neck lymph nodes (54 %), skin (33 %), and other head and neck (HN) mucosal primary sites (16 %). Of the 24 sites, 17 (71 %) were de novo without prior treatment and 7 (29 %) were recurrent. The most commonly used dose/fraction (fx) was 40 Gy/5fx (range 35/5fx–48/6fx). Complete response was seen in 25 % of the lesions, while 67 % of lesions had a partial response and 8 % had no response (Table 1).
Control was defined as no further progression after treatment. For the entire cohort, local control at 3, 6, and 9 months was 66, 50, and 33 %, respectively. The median time to local failure was 2.7 months. In the de novo group, local control rates were 94, 94, and 87 % at 3 months, 6 months, and 1 year, respectively. In this group, 12.5 % of lesions experienced local failures. In the recurrent group, half of the lesions had local failure at 1 year. Local control rates for the recurrent group were 87.5, 62.5, and 50 % at 3 months, 6 months, and 1 year, respectively.
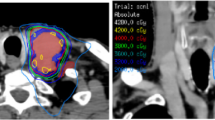
During the follow-up period of 8 months, 10 of the 21 patients died, with a median time to death of 8 months. The actuarial overall survival rates at 3 months, 6 months, and 1 year were 90, 70, and 60 %, respectively. Being defined de novo (p = 0.046) had a trend toward statistical significance. No significant prognostic variables for overall survival were found. 6/21 (25 %) patients had distant relapse. Figures 1 and 2 show pre- and post-SBRT treatment effectiveness.

Ninety-year-old patient with new SCC, pre-SBRT

First follow up 2 months post-SBRT with dose of 40/5
Quality of life was assessed prior to and after radiation treatment. Pre-treatment quality of life scores for the entire cohort were 53/130, while at follow-up these scores were 38/130. For the EORTC QLQ-H&N35, lower scores indicate better quality of life, thus demonstrating that radiation was able to improve quality of life in this patient cohort. This demonstrated a trend toward statistical significance (p = 0.05). The QLQ-H&N35 questionnaire is comprised mostly of symptom-related items, such as pain, swallowing, taste, and coughing. As quality of life improved from baseline to follow-up, it is likely that patient symptom burden decreased. This again demonstrates the efficacy of SBRT in this patient group.
Discussion
This study demonstrates the effectiveness of SBRT in the palliative setting in patients with head and neck cancers where a lack of local control can have devastating effects on quality of life. While we included both de novo and recurrent patients, our series has the largest number of de novo patients of any series published to date. It is evident that the de novo patients had better outcomes, although SBRT was able to adequately control a significant portion of tumors in the recurrent setting as well. A recent review article on locally ablative treatment for patients with oligometastases from head and neck cancer has demonstrated that SBRT can be effective; however, further research is needed to determine the ideal candidates [7]. Overall efficacy exceeding 85 % has been cited, which is similar to the local control rates in this study. Comet et al. [8] quoted overall response rates (CR/PR) of 79.4 % in their cohort of patients with locally recurrent head and neck cancers. Interestingly, SBRT was delivered with cetuximab in some cases. There were a few cases of grade 3 toxicity, while we did not observe any cases of grade 3 toxicity. These two cited response rates [7, 8] are lower than the rate of 92 % achieved in this study without the addition of a biologic agent.
Another study by Siddiqui et al. [13] included patients treated with de novo SBRT, and patients treated for recurrent head and neck cancer and metastatic tumors. Tumor control rates at 1 year were determined to be 83.3 and 60.6 % in primary and recurrent groups, respectively. Similarly, tumor control rates at the 1 year point were found in our study: 87 % for the primary group and 60 % for the recurrent group.
In our study as well, not surprisingly, patients with de novo cancers, in admittedly a short follow up seemed to maintain a high level of locoregional control with a short course of SBRT that is relatively easy to tolerate even for an elderly (median age—87) and frail population.
Head and neck SBRT appears to improve quality of life, with a trend toward statistical significance. Indeed, the ability to deliver SBRT-like doses without excessive morbidity to the head and neck is possible because of technological improvements within radiation oncology, in particular intensity modulated RT (IMRT) which has been shown to improve quality of life when compared to conventional radiation therapy [21]. In a study by Vargo et al. [22] with recurrent, previously radiated head and neck cancer patients, they prospectively analyzed patient-reported quality of life outcomes in patients treated with SBRT. In this study, the University of Washington Quality-of-Life Revised was utilized, and it was determined that improved tumor control associated with SBRT is able to improve quality of life in this patient cohort. Improvements were seen on all domains of this questionnaire, regardless of patient age, chemotherapy, tumor volume, and time since previous radiation. Our study supports these previous findings as we have demonstrated that SBRT could be able to improve quality of life and symptom burden of head and neck cancer patients.
Elderly patients oftentimes find it difficult to undergo treatment and to travel numerous times to the cancer center for treatments such as conventional radiation. In addition, this patient population often has a number of comorbidities that make surgery a poor treatment option. For these patients, SBRT can be feasible and efficacious, as its local control rates and quality of life have been acceptable.
This study demonstrates the effectiveness of SBRT in the de novo and recurrent settings for elderly patients with head and neck cancer for whom surgery is not an option. Overall survival rates and local control rates were better than those seen with conventional radiation treatment.
Conclusions
SBRT is efficacious in the treatment of de novo and recurrent tumors of the head and neck with promising quality of life scores. In these head and neck patients not amendable to surgery or protracted curative radiotherapy, short course SBRT achieved good local control and showed a trend to better quality of life on treatment fraction 5 compared to baseline. SBRT is also associated with fewer hospital visits and is a desirable treatment option. Further studies are currently underway, but at our institution we routinely employ SBRT in the de novo and recurrent setting in the elderly and patients with poor performance status. A limitation to our study is the fact that only one time point was used for quality of life assessment compared to baseline; therefore, we were not able to make any conclusions on whether or not improvement in QOL is durable. Another limitation of our study is the small number of patients; however, our study still represents one of the largest series in the setting of SBRT for HN in the literature.
References
Barnes EA, Breen D, Culleton S, Zhang L, Kamra J, Tsao M et al (2010) Palliative radiotherapy for non-melanoma skin cancer. Clin Oncol (R Coll Radiol) 22(10):844–849
Simpson J, Drzymala R, Rich K (2006) Stereotactic radiosurgery and radiotherapy. Technical basis of radiation therapy. Springer, Berlin, pp 233–253
Ch'ng S, Maitra A, Lea R, Brasch H, Tan ST (2006) Parotid metastasis—an independent prognostic factor for head and neck cutaneous squamous cell carcinoma. J Plast Reconstr Aesthet Surg 59(12):1288–1293
delCharco JO, Mendenhall WM, Parsons JT, Stringer SP, Cassisi NJ, Mendenhall NP (1998) Carcinoma of the skin metastatic to the parotid area lymph nodes. Head Neck 20(5):369–373
Hinerman RW, Indelicato DJ, Amdur RJ, Morris CG, Werning JW, Vaysberg M et al (2008) Cutaneous squamous cell carcinoma metastatic to parotid-area lymph nodes. Laryngoscope 118(11):1989–1996
Veness MJ, Palme CE, Smith M, Cakir B, Morgan GJ, Kalnins I (2003) Cutaneous head and neck squamous cell carcinoma metastatic to cervical lymph nodes (nonparotid): a better outcome with surgery and adjuvant radiotherapy. Laryngoscope 113(10):1827–1833
Florescu C, Thariat J (2014) Local ablative treatments of oligometastases from head and neck carcinomas. Crit Rev Oncol Hematol Jan 23
Comet B, Kramar A, Faivre-Pierret M, Dewas S, Coche-Dequeant B, Degardin M et al (2012) Salvage stereotactic reirradiation with or without cetuximab for locally recurrent head-and-neck cancer: a feasibility study. Int J Radiat Oncol Biol Phys 84(1):203–209
Heron DE, Ferris RL, Karamouzis M, Andrade RS, Deeb EL, Burton S et al (2009) Stereotactic body radiotherapy for recurrent squamous cell carcinoma of the head and neck: results of a phase I dose-escalation trial. Int J Radiat Oncol Biol Phys 75(5):1493–1500
Kawaguchi K, Sato K, Horie A, Iketani S, Yamada H, Nakatani Y et al (2010) Stereotactic radiosurgery may contribute to overall survival for patients with recurrent head and neck carcinoma. Radiat Oncol 5:51
Roh KW, Jang JS, Kim MS, Sun DI, Kim BS, Jung SL et al (2009) Fractionated stereotactic radiotherapy as reirradiation for locally recurrent head and neck cancer. Int J Radiat Oncol Biol Phys 74(5):1348–1355
Rwigema JC, Heron DE, Ferris RL, Gibson M, Quinn A, Yang Y et al (2010) Fractionated stereotactic body radiation therapy in the treatment of previously-irradiated recurrent head and neck carcinoma: updated report of the University of Pittsburgh experience. Am J Clin Oncol 33(3):286–293
Siddiqui F, Patel M, Khan M, McLean S, Dragovic J, Jin JY et al (2009) Stereotactic body radiation therapy for primary, recurrent, and metastatic tumors in the head-and-neck region. Int J Radiat Oncol Biol Phys 74(4):1047–1053
Stevens KR Jr, Britsch A, Moss WT (1994) High-dose reirradiation of head and neck cancer with curative intent. Int J Radiat Oncol Biol Phys 29(4):687–698
Unger KR, Lominska CE, Deeken JF, Davidson BJ, Newkirk KA, Gagnon GJ et al (2010) Fractionated stereotactic radiosurgery for reirradiation of head-and-neck cancer. Int J Radiat Oncol Biol Phys 77(5):1411–1419
Voynov G, Heron DE, Burton S, Grandis J, Quinn A, Ferris R et al (2006) Frameless stereotactic radiosurgery for recurrent head and neck carcinoma. Technol Cancer Res Treat 5(5):529–535
De Crevoisier R, Bourhis J, Domenge C, Wibault P, Koscielny S, Lusinchi A et al (1998) Full-dose reirradiation for unresectable head and neck carcinoma: experience at the Gustave-Roussy Institute in a series of 169 patients. J Clin Oncol 16(11):3556–3562
Pomp J, Levendag PC, van Putten WL (1988) Reirradiation of recurrent tumors in the head and neck. Am J Clin Oncol 11(5):543–549
Kodani N, Yamazaki H, Tsubokura T, Shiomi H, Kobayashi K, Nishimura T et al (2011) Stereotactic body radiation therapy for head and neck tumor: disease control and morbidity outcomes. J Radiat Res 52(1):24–31
Bjordal K, de Graeff A, Fayers PM, Hammerlid E, van Pottelsberghe C, Curran D et al (2000) A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur J Cancer 36(14):1796–1807
Graff P, Lapeyre M, Desandes E, Ortholan C, Bensadoun RJ, Alfonsi M et al (2007) Impact of intensity-modulated radiotherapy on health-related quality of life for head and neck cancer patients: matched-pair comparison with conventional radiotherapy. Int J Radiat Oncol Biol Phys 67(5):1309–1317
Vargo JA, Heron DE, Ferris RL, Rwigema JC, Wegner RE, Kalash R et al (2012) Prospective evaluation of patient-reported quality-of-life outcomes following SBRT +/− cetuximab for locally-recurrent, previously-irradiated head and neck cancer. Radiother Oncol 104(1):91–95
Conflict of interests
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Khan, L., Tjong, M., Raziee, H. et al. Role of stereotactic body radiotherapy for symptom control in head and neck cancer patients. Support Care Cancer 23, 1099–1103 (2015). https://doi.org/10.1007/s00520-014-2421-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-014-2421-y