
Abstract
The principal source of the fetal electrocardiogram (FECG) signal valuation is noted for scientific examination and also related to biomedical applications. A great requirement in fetal monitoring is the extraction or diagnosis of the FECG signal from the highly developed methodologies of composite abdominal impulses. The efficiency of an access procedure is exposed using the methodological evaluation which supports the deep facts of fetal ECG which gives useful data. In this survey, research-revealed methods to extract the FECG signals are reviewed. The use of an adaptive filter in the abdominal ECG signal provides an efficient and effective mode of FECG signal extraction. Similarly, the effectiveness of the FECG extraction can be improved through different methodologies. In this document, the most modern investigations related to the FECG extraction are effectively analyzed and briefed on so as to effectively furnish the traits and classifications. The performance of each FECG extraction technique is confirmed quantitatively by working out SNR and PRD. From the effects, we can make out that the proposed algorithm can be efficiently employed for extracting fetal ECG from abdominal signals.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The fetal electrocardiogram (ECG) waveform investigation is carried out with the help of estimating the electrical activity from the fetal heart. This has been in vogue for the past 30 years, thereby witnessing gradual growth during the period. It is effectively determined by inserting the electrodes into the abdomen of the mother. It tends to have inferior power, and hence it is to be blended by various sources of noise and interference. The electrocardiogram (ECG) has, over the years, established itself as the easiest and most efficient noninvasive investigative method for a host of diverse heart ailments. The Fetal ECG (FECG) signal, in turn, mirrors the electrical function of the fetal heart and accurately offers beneficial data on its physiological condition. The noninvasive FECG is effectively utilized to realize fruitful clinical data on the fetus. This is used to obtain valuable clinical information about the fetal state in the course of the pregnancy by effectively using the skin electrodes. It is inserted into the maternal abdomen.
1.1 FECG extraction
The extraction of the hygienic fetal electrocardiogram (ECG) signals has emerged in Wu et al. (2013) to be a highly critical factor in fetal monitoring. The salient features of the LMS adaptive filtering techniques are shown below.
-
1.
The LMS invariably achieved higher levels of perfection in the case of superposition of the R-peaks of fetal ECG and maternal ECG.
-
2.
It effectively steered clear of the noise interruption using the integration of the SSNF technique, which resulted in the extraction of further robust waveforms.
-
3.
The efficiency in the accomplishment of the technique was well established quantitatively with the help of SNR estimation.
Further, it exemplified the deployment of the reconfigurable system for the fetal electrocardiogram (FECG) evaluation.
An innovative system was proposed by Morales et al. (2013) by employing a reconfigurable system for the fetal electrocardiogram (FECG) evaluation from the ECG estimations of the abdomen of the mother. The novel technique invariably depended on two divergent reconfigurable devices. At the outset, a field-programmable analog array (FPAA) tool was entrusted with the task of performing the analog reconfigurable preprocessing for the ECG signal attainment. The signal processing chain was extended into a field-programmable gate array (FPGA) gadget, which functioned as a base to the entire set of the transmission and interfacing protocols. This together with the exact digital signal processing blocks was needed for the basic period extraction after the FECG waveforms in the sequence of the acquirement function of achieving a superior outcome. The synergy between these contrivances was empowered with the necessary skills to adapt to any crucial constraint. The effective employment of the FPGA was farfetched in performing various techniques intended for the FECG signal extraction, like the adaptive signal filtering.
Two novel techniques are introduced in Jagannath and Immanuel Selvakumar (2014) such as the fetal scalp electrode (invasive), and maternal abdomen skin electrode (noninvasive) has been devoted to the achievement of the ECG. Out of the two, the former approach, viz. the fetal scalp electrode technique, proved to be hazardous to the fetus. Inserting the scalp electrodes on the head of the fetus after passing through the womb of the mother was really a dangerous process. The relative technique was injurious to the mother as it was likely to rip the womb and trigger contagion in the interior of the womb or bloodshed. In addition to being detrimental, it was perilous to the fetus as well, as it caused undue pressure on the head of the fetus, infection and cast gloom on the security of the fetus safety, and so on. Striking a different note, the maternal abdomen skin–electrode emerged as an ideal candidate with several merits such as easiness, noninvasiveness and the feasibility for use in the course of labor.
Cardiotocography (CTG) derived that fetal heart rate time series does not qualify for the beat-to-beat examination in Karmakar et al. (2015), which is clinically more important than the long-term measure. The fetal magnetocardiogram (fMCG) effectively overpowers the drawbacks of the CTG and offers a noninvasive technique for examining the fetal cardiac function with adequate accuracy. Nevertheless, the fMCG invariably needed magnetically shielded rooms (MSR), which restricts the normal deployment of the device on account of the elevated expenditure of the MSR materials. On a similar note with the fMCG, the fetal electrocardiogram (FECG) represented a noninvasive technique for analyzing the beat–beat fetal cardiac function with enough accuracy. Even though the extraction of the FECG was very hard, the blind source separation with reference signals (BSSR) approach was envisaged for the steady and consistent extraction of the FECG. Hence, FECG was considered as an easy and expedient technique for the noninvasive scrutiny of the fetal cardiac function. So, in this survey, we review some previous literature which focused research on FECG extraction.
2 Literature review
In this section, some previous FECG extraction techniques based on artificial intelligence, wavelet transform, singular value decomposition (SVD), independent component analysis (ICA), computational intelligence, blind source separation (BSS), adaptive noise cancelation (ANC) algorithms and Bayesian methodologies are reviewed.
2.1 Artificial intelligence techniques in FECG extraction
The noninvasive FECG signal is to be extracted in Jagannath and Immanuel Selvakumar (2015) with the maximum possible efficiency. With a view of helping the physicians, they envisioned an innovative intrapartum monitoring method known as the STAN (ST analysis) for effectively predicting the intrapartum fetal hypoxia. Nevertheless, the vital dilemma was that the noninvasive FECG signals verified after the maternal abdomen were adversely affected by various interferences such as
-
Power-line interference
-
Baseline drift interference
-
Electrode movement interference
-
Muscle motion interference
-
The MECG dominant interference.
Further, this flagged off a ground-breaking approach known as the BANFIS (Bayesian adaptive neurofuzzy inference system). The novel BANFIS technique was the base of a Bayesian filter and an adaptive neurofuzzy filter for the eradication of the MECG and nonlinear artifacts to bring in a superior-quality FECG signal.
Numerous methods are used to verify the characteristics of fetal heart and situation other than using the FECG signal. The wellness of the fetal heart is being observed by a variety of other methods besides electrocardiography like echocardiography which is dependent on the ultrasound method also known as sonography. Cardiotocography (CTG) is the synchronized capacity of the fetal heart rate with the help of an ultrasound transducer, and the uterine reduction by a pressure-sensitive transducer called the tocodynamometer, to calculate the frequency and the strength of uterine contractions. Phonocardiography is a graphic illustration of the heart sounds and murmurs produced by the contracting heart. They are picked up as vibrations and distorted using a piezoelectric crystal microphone into an unreliable electrical number according to the pressure imparted by the sound waves.
Magnetocardiography calculates the magnetic fields of cardiac signals with very sensitive devices such as the superconducting quantum interference device. To establish oxygen saturation of fetal blood as an accessory to fetal heart monitoring, pulse oximetry is used. A large amount of redirected infrared light is cast off to confirm the qualifying amount of oxygen in the fetus’s blood under the skin. During these methods, echocardiography can be taken as the general means of fetal cardiac monitoring. Though the ECG and the magnetocardiography have more sources of information due to the morphologic resemblance of the magnetocardiography and ECG, magnetocardiography processing techniques are alike to that of ECG. The SNR of the fetal magnetocardiography is much eminent than the normal ECG. Yet, ECG recording machinery is straightforward and more reasonable as compared with the magnetocardiography arrangement (Jagannath and Immanuel Selvakumar 2015).
An adaptive method was launched in Amin et al. (2011) to extract FECG by employing an innovative adaptive linear neural network (ADALINE) for trouble-free fetal scrutiny in which the suitable learning rate, momentum and initial weights were employed. This was done to harmonize the network error until it became equivalent to the fetal ECG. This novel technique achieved superlative precision when the constraints such as the learning rate (LR), momentum(M) and initial weights (IW) were estimated using specified values such as high LR, low M and small IW
An adaptive neurofuzzy inference system (ANFIS) was launched in Nasiri et al. (2011) to examine and locate the nonlinear high-frequency components of maternal electrocardiogram (MECG). The particle swarm optimization (PSO) was treated as a highly sophisticated device meant for training the ANFIS structure which recognized the nonlinear components of MECG (transformation). This was done while training the input AECG data and subsequently effectively eradicated the associated edition of the MECG signal from the noise-free abdominal ECG (AECG) signal extorted by the FECG (Table 1).
2.2 Wavelet transform-based FECG extraction approaches
An innovative pattern for the fetal heart rate (FHR) examination from single-lead mother’s abdomen ECG (AECG) measurements is enlightened in Castillo et al. (2013). The proposed technique was passed through the following two phases.
-
In the former phase, a single-step wavelet-based preprocessing was performed for instantaneous baseline and high-frequency noise repression.
-
In the latter phase, effective identification of the fetal QRS complexes was accomplished, thereby facilitating the FHR scrutiny.
The offered framework was further simplified to a feasible extent, with the intention of significantly scaling down the computational expenses. This facilitated the potential custom hardware accomplishments. Further, the innovative technique of fixed-point modeling was extensively investigated with the deployment of the genuine abdominal ECG signals. This enabled the authentication of the novel technique, thereby giving precision.
A concurrent fetal electrocardiogram (FECG) feature extraction technique was dependent on multiscale discrete wavelet transform (DWT) which was flagged off in Desai and Sankhe (2012). The wavelet-based peak recognition was employed to identify the QRS complex. This was used for detecting the ups and downs of the noise-polluted FECG signal. Further, the two-channel perfect reconstruction (PR) filter banks were employed to perform the discrete wavelet transform effectively. The expanded fetal maternal ECG monitor machine was investigated in a local hospital on a sample group of 35 pregnant women at various intervals in the course of the gestation period. This consistent system was able to identify the entire FECG beats with incredible accuracy to the tune of 99.5%. This was done by taking into account the restraints in the measuring system parameters in the five-minute recording of each subject (Table 2).
2.3 SVD–ICA-based approaches for FECG extraction
The blind source separation has the capacity to successfully divide the mixed signals, without the guidelines of any previous facts concerning the source signals. The factorization of actual or composite matrix is called the singular value decomposition (SVD). This is mainly developed in the signal separation. The independent component analysis represents a novel approach which is processed for the segregation of a multivariate signal into additive subcomponents.
For the extortion of FECG, the independent component analysis (ICA) depends on blind source separation (BSS) technique which was developed in Wen and Luo (2012), in which ICA can be used as the superior-order statistics resulting in the computational complexity. ICA-related technique for the FECG extraction and MECG annulment was processed efficiently in the nonexistence of signal-to-noise ratio equal to -200 db. Without quantification of the noise and likewise, the efficiency of the system went down with quantification.
For a fetus with a gestational age between 32 and 41 weeks, the heart rate is in the array of 80–240 BPM (beats per minute) with an anticipated heart rate around 140 BPM and a peak-to-peak amplitude fluctuating any place in the middle of 3–25 μV, with an expected amplitude at 20 μV2. For the finest separation of FECG, second-order blind identification (SOBI), fast ICA and joint approximation diagonalization (JADE) chosen algorithm were tested. Among ICA systems, fast ICA, π-CA, JADE and Pearson ICA were compared based on the correlation coefficient parameter. Both prefer fast ICA over all other methods to extract fetal ECG. Another comparison of PCA and ICA was made for the accuracy check of extracted fetal ECG; both gave almost the same accuracy. However, ICA gave unsorted independent constituents and thus was required to form for the obligatory signal individually. Another method which was well scored in the PhysioNet 2013 challenge is a combination of template subtraction (TS) and ICA. This is termed the FUSE method. FUSE was defined as the mixture of a subsection of the evaluated approaches; the methods are ICA-TS, ICA-TS-ICA, TS-ICA, ICA and TS. The unsurpassed technique was determined to be FUSE-SMOOTH (FUSE with a smoothening block introduced). ICA is the favored technique in most of the current methods for fetal ECG extraction with adequate results. This work also has castoff ICA together with preprocessing and postprocessing approaches (Raja et al. 2015).
Luo (2012) discussed the nonlinear blind mixed ECG signals separation technology, introducing the model of the ICA algorithm and the employment methods. The experimental results showed that, with the simulated dataset, this technique can efficiently progress the operational effectiveness and achieve a good result for segregating the signals, and the monitoring time episode error was less than 0.5%.
An innovative mechanized technique was introduced in Dhage and Madhe (2014) for the extortion of the fetal electrocardiogram (FECG) from the abdominal electrocardiogram (AECG) recording. The FECG represented a feeble signal from the maternal ECG. This was indirectly evaluated by the surface electrode inserted in the abdomen of the mother. The fetal signals were buried in the other interference signal. This extraction of the FECG from strong background interference was a very valuable factor in the clinical application.
However, a number of investigation works have been carried out in this domain, a few of which include the following.
-
Threshold and filtering technique
-
Neural network technique
-
Wavelet transform and others.
The innovative technique includes the independent analysis technique for FECG extraction. The ICA functions in diverse constraints such as the kurtosis and negentropy. In the current investigation, the focus is on the negentropy. Subsequent to the extraction of FECG signal, the fetal R-peak is identified by means of the threshold-free identification technique involving the R–R moving interval, estimated as per the normal maximum and minimum heart rate (Table 3).
2.4 Computational intelligence for FECG extraction
Ahmed et al. (2011) proposed a technique for FECG extraction. This was based on a genetic algorithm (GA) by working with an adaptive filter. GA is a practical technique optimization problem-solving method which is based on natural genetics. GA is a powerful method and appropriate for stochastic investigation systems. It is the utmost extensively recognized type of evolutionary computational methodology. GA twitches primarily with a populace of arbitrarily produced vectors. It then tests the fitness of those vectors and lastly picks the finest ones and recombines the parameter values of those finest ones. In this method, GA was used whenever the adaptive filter is alleged of accomplishing local iotas. Further, an independent GA search was performed without the adaptive filter. The algorithm was verified with the help of the database widely used by the signal processing community, the SISTA/DAISY dataset. The compensations of the projected way are simple and not complex.
An adaptive neurofuzzy interference system (ANFIS) trained with particle swarm optimization (PSO) methodology was developed in Sargolzaei et al. (2011) using four different techniques for the elicitation of FECG signal. That was completed with the help of abandoning the MECG signal after the AECG signal. The PSO algorithms are population-based search algorithms quite similar to the social behavior of birds within a flock. Each individual bird in the search space is with a velocity that is enthusiastically accustomed according to its self-flying experience and its companion’s flying experience. Background noise is barred by adaptive noise cancelation. PSO has helped faster convergence. The complexity of the algorithm was also admirable. The replicated dataset was used for experimentations. The percentage root-mean-square difference (PRD) was 0.4734. The drawback was that real-time processing was not executed.
An ANFIS trained with PSO method for FECG signal elicitation was proposed in Nasiri et al. (2011, 2012). Two signals were used, one recorded at the thoracic part and the other at the abdominal area of the mother. Simulated dataset and also the Daisy database and PhysioNet catalogue were used for experiments. The resulted signal had a considerable enhancement along with 0.4734 percent root-mean-square difference (PRD). The only difference between the proposed technique and the method of Sargolzaei was that a different database was used for the former, whereas in Sargolzaei method used only simulated data (Table 4).
2.5 Blind source separation (BSS) methodologies
A three-stage methodology adopting BSS technique was proposed in Karvounis et al. (2010). At the primary phase, the fetal heart rate (fHR) was removed after the AECG signals along with the help of nonlinear analysis. In the second phase, blind source departure method was smeared to the eradicated ECG signals and the FECG signal was accomplished. Finally, fetal monitoring was performed using the extracted features. The extracted FECG was compared with the actual FECG signal and was known to be connected with the true FECG. The methodology was evaluated using a dataset of replicated multichannel AECG signals which displayed 94.79% accuracy for fHR elicitation, 92.49% accuracy in T/QRS ratio computation and 79.87% in ST waveform organization. Replicated signals only have been engaged; evaluation with actual records was not achieved.
Romero (2010) investigated the performance of principal component analysis (PCA) for denoising ECG signals recorded in ambulatory circumstances. An imitation database was organized by the collection of clean ECG signals. Here, noise measured to various levels of energy was improved for assessment. It attained development of 0.95 dB at 10 dB of SNR and 1.92 dB at − 10 dB of SNR. The process of shorter noise was not studied. Decomposition of single- or multichannel recording is another popular method. Hereby, using particular basis function, the signals are collapsed into different components. These functions are chosen from the classes that are in one way or the other inconsistency with frequency, time or degree of fetal components features. Spatial filtering methods are indicated as decomposition techniques such as singular value decomposition (SVD), blind and semiblind source separation that is determined by data, which creates the necessary basic functions from the data itself, by maximizing many statistical quantities of signal separation (Table 5).
2.6 ANC algorithms and methodologies
Rahman et al. (2011) developed an adaptive filtering technique for noise exclusion. Introduced signed-based normalized adaptive filtering techniques such as normalized signed regressor LMS (NSRLMS) algorithm, normalized sign LMS (NSLMS) algorithm and also normalized sign–sign LMS (NSSLMS) algorithm and block-based NLMS (BB-NLMS) are used for the removal of noise from ECG signals. In conditions of SNR improvement and computational complexity, the signed regressor LMS algorithm processes better than LMS. MIT-BIH database is mainly used for various noises which contain double-channel ECG recordings. This was accessed from 47 subjects including 25 men aged 32–89 years and women aged 23–89 years. The recordings were at 360 samples per second and per channel with an 11-bit resolution above 10 mV range digitized. The advantages of the NLMS algorithm were that the step size was chosen from the input signals and the number of tap weights and the convergence rate of an algorithm and steady-state error are better than LMS algorithm. The need for extra computations is its drawback.
2.7 Bayesian methodologies
FECG signal was derived in Yin et al. (2010) by using Bayesian inference with neural networks. The ECG signal was formed by generalized Gaussian distribution, and backpropagation neural network was used to estimate the nonlinear purpose within two signals such as MECG and AECG. These two experiments were done; one uses real ECG signal data, while the other uses artificially mixing ECG signal data. The first one was Bayesian inference related to neural networks approximation. The second one was by using polynomial networks. The technique has been proved to be effective and simple.
An adaptive Kalman filter was developed in Vullings et al. (2011) for improving the SNR of the ECG signal. The ECG signal characteristics change because it is subjected to long-term monitoring tasks. The adaptive Kalman filter is capable of quickly adapting itself to the noise calculation. This is done to compare the filter’s output to the new input. On the other hand, the fixed Kalman filter required 10 s to manage the output because of the nonflexible calculation of the Kalman gain. A sequential averaging filter was improved adaptively that differed from the number of critical consisting in the averaging depend on the features of the ECG signal. The filter has the model of an adaptive Kalman filter. The estimation of the improved Kalman filter was completed by a diversity of ECG signal which includes ECG signal of adult patients that was affected with T-wave alternans (TWA). FECG signals were recorded from the maternal abdomen, and this documented neonatal ECG signals. The capable methods for MECG deletion and FECG enrichment are the Kalman filtering frameworks. This framework creates the base for extensions on more highly improved filters such as the particle filter. The drawbacks of Bayesian modeling and Kalman filtering are involved with mathematical complexity. Here, computational time is not fast and needs brief information on the ECG signal dynamics.
Gupta et al. (2016) proposed a methodology to extract FHR (fetal RR time series) from the abdominal electrocardiogram (AECG) recordings using the recently introduced multivariate empirical mode decomposition (MEMD) method. MEMD breakdowns a signal into a limited set of intrinsic mode functions (IMFs). Initially, it is dependent on the differentiation of equivalent indexed IMFs. This removes the noisier AECG channels that were acquired through the MEMD-conducted method. After that, denoising of the remaining AECG channels is processed by removing certain similar indexed IMFs. The unwanted mother QRS complexes are eliminated from noise-free AECG channels, and the candidate fetal R-peaks are recognized by a wavelet-based method. The projected methodology is corrected by using open-source real-life clinical database. The projected method is concluded in high value (0.983) of cross-correlation between the detected and true FHR signals (Table 6).
3 Adaptive filtering-based FECG extraction approaches
An adaptive filter consists of an effective filter which self-adapts its transfer function on the basis of an optimization technique motivated by an error signal. In this regard, diverse categories of the adaptive filters have been extensively employed for the purpose of the fetal and maternal signal separation. The corresponding techniques invariably employ one or more reference maternal signals for either training an adaptive or harmonized filter or directly training the filter devoid of the reference signal for the extortion of the fetal QRS waves. The Kalman filter symbolizes a universal class of adaptive filters extensively employed. It utilizes only a random MECG as a reference for the MECG annulment and FECG extortion. The temporal dynamics of AECG signals are modeled or AECG signals. They are synthesized depending on the compilation of the state-space equations and Bayesian filter which has been employed for the purpose of the ECG denoising. However, the filter miserably fails to distinguish between the maternal and a fetal component when there is overlapping in time. When the waves of varied signals completely overlap in time, it is a complex task filtering out the preferred ECG employing the relative filter.
3.1 Multistage adaptive filter for FECG extraction
An enhanced technique was launched in Swarnalatha and Prasad (2010) by effectively employing the multistage adaptive filtering for the FECG extraction. Here, MECG annulment is performed taking into account thoracic ECG as the reference signal. Further, the denoising techniques have been elegantly employed to augment the quality of an extracted signal. Usually, the adaptive filter is in need of two input signals as shown below.
-
AECG signal
-
Thoracic ECG
Here, thoracic ECG is adapted by means of the scaling and squaring. Scaling factors are selected in such a way so as to attune the adaptive filters to accomplish the extraction. An important quality of the novel technique is that the input thoracic signal need not necessarily be original which is gathered from the pregnant woman whose AECG has been furnished as the primary input. Along with this, an even intimately identical signal may also be taken into account. In this regard, three diverse techniques are employed for the self-adapting filter such as the LMS, RLS and NLMS for the purpose of augmenting the SNR ratio by suitably adapting the filter coefficients.
3.2 Adaptive noise canceler for FECG extraction
The elimination of background noise and artifacts from the FECG signals employing the adaptive filters is discussed in Prasanth et al. (2013) which involves the application of two input signals as detailed below.
-
The primary signal represents the FECG signal combined with the MECG signal
-
The secondary signal characterizes the reference signal which is the noise to be annulled such as the MECG signal.
The secondary noise signal has to be effectively associated with the noise in the primary signal. The adaptive filters are effectively utilized in the fetal electrocardiography, wherein a maternal heartbeat signal is adaptively detached from a fetal heartbeat signal. In an adaptive filter functioning in a motionless scenario, the error performance surface possesses a fixed form and orientation. When the adaptive filter is functioning in a moving scenario, the bottom of the error performance surface moves frequently, whereas the orientation and curvature of the surface also undergo certain changes. Hence, when the inputs are moving, the adaptive filter performs the function of looking for the bottom of the error performance surface, thereby incessantly tracking it.
3.3 Kalman filters for FECG extraction
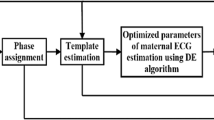
The Kalman filtering (KF) framework was started in Niknazar et al. (2012) which are deemed as a member of the universal class of adaptive filters. This was done in addition to this being a prospective technique for the annulment of the MECG and the enrichment of the FECG. To devise a Bayesian filter for the purpose of ECG denoising, a set of state-space equations is effectively employed to fashion the temporal dynamics of ECG signals. The captioned Bayesian filter structure is then effectively utilized to extract the FECG from a single-channel blend of the MECG and FECG. Thus, we find that the filter has miserably failed to distinguish between the maternal and fetal components when the MECG and FECG waves completely overlay in time. It is because of the fact that if MECG is evaluated, the FECG and the parallel components are deemed to be the Gaussian noises. Yet, the presumption turns out to be false, particularly if the MECG and FECG waves completely overlay in time. Thus, it is very hard for the filter to pursue the preferred ECG. The algorithm for FECG extraction is given below (Fig. 1).

Algorithm for FECG extraction
3.4 Transabdominal fetal electrocardiogram
The ta-FECG recording with the assist of the AN24 fetal ECG monitor in the serene scenarios in the utero was performed in Stampalija et al. (2015). The electrophysiological signal invariably includes the following elements.
-
Maternal ECG
-
Fetal ECG
-
Electrohysterogram
In a homogeneous way, it is recorded with a sample frequency of 900 Hz utilizing five disposable electrodes located on the maternal abdomen. The method that works for the extraction of the fetal ECG signal and assessment is richly elucidated. The fetal ECG complexes are efficiently utilized to estimate the R–R pulse intervals with an accuracy of about 1 ms. The STV (in ms) is expected from the found R–R intervals in accordance with the investigation recordings with signal loss > 50% which are eradicated from additional examination.
3.5 RMI extraction
It is practically easy to visually place the RMI as a noise superposition on top of the ECG. A simple technique for its extraction is the abandonment of the ECG. Recently, a novel cancelation method was planned in the backdrop of the noninvasive fetal ECG extraction in Maier and Dickhaus (2014) which may prove effective for the working of the extraction of the RMI. The associated process commences right from the baseline- and power-line-filtered raw ECG signals. At the outset, a template (average cardiac cycle) is produced and incessantly reduced from the ECG. The residual inconsistency associated with the ECG waves is additionally triggered by the abolition of the foremost principal components from several epochs encompassing the QRS complex ([R − 100 ms; R + 100 ms]), P-wave ([R − 300 ms; R − 100 ms]) and T-wave ([R + 100 ms; R + 500 ms]) of the vector ensembles that are attained. With an eye on enumerating the vigor of RMI, a time-variant measure of variability has to be executed on this signal. The unrefined RMI signal envelope characterizes an instant index of RMI strength with the time resolution of the ECG. The raw RMI signal standard deviation (SD) is calculated in a sliding windows of 100 ms width, the reasons for which will be elucidated later (Table 7).
3.6 FHR estimation
A new algorithm was proposed in Ruffo et al. (2010) to detect fetal heart rate calculation from fetal phonocardiographic recordings. A filtering emerges as the first step of the algorithm to minimize the background noise. A block for first heart sounds enhancing is used to an additional decrease of extra components of fetal heart sound signals. A complex logic block is led by a number of rules relating to fetal heart beat reliability. This is projected as a successive block, for the recognition of most possible first heart sounds from several candidates. A final block is used to extract first heart sound timing and fetal heart rate evaluation. Filtering and enhancing blocks are essentially executed by various methods, so that various processing paths are introduced.
Moreover, a reliability index is initiated to measure the reliability of the predictable fetal heart rate and depends on statistic strictures; a software eminence index is intended to point out the most reliable analysis procedure (that is, merge the best processing path and the most exact time mark of the first heart sound, and supply the lowest inference errors). The algorithm presentations have been verified on phonocardiographic signals recorded in a local gynecology confidential practice from a sample group of about 50 pregnant women. Phonocardiographic signals have been recorded concurrently to ultrasonic cardiotocographic signals in order to contrast the two fetal heart rate series (the one predictable by our algorithm and the other offer by cardiotocographic device). The results demonstrate that the projected algorithm, in particular some analysis procedures, supplies reliable fetal heart rate signals, very close to the suggested cardiotocographic recordings.
3.7 ST analysis
Computerized ST evaluation of fetal electrocardiography (ECG) is linked with cardiotocography (CTG) which is proposed in Salmelin et al. (2013) for intrapartum monitoring and is the existing technique where ST analysis (STAN) is used. To review the confirmation that computerized ST analysis through labor diminishes the presence of fetal metabolic acidosis, cesarean section, hypoxic ischemic encephalopathy, instrumental vaginal delivery or the amount of instances where fetal scalp blood sampling is used as contrast with CTG only. To search PubMed, Cochrane Library, EMBASE, Web of Science, CINAHL and CRD databases. CTG was only differentiated with CTG + computerized ST analysis. Studies were reviewed by using predesigned patterns.
Meta-analyses of integrated randomized controlled trials were performed using a random effects design. Risk ratio for cord metabolic acidosis with STANR was 0.96 [95% confidence interval (CI) 0.49–1.88]. Risk ratio of cesarean sections or instrumental vaginal deliveries for fetal distress was 0.93 (95% CI 0.80–1.08), and for fetal scalp blood sampling, it was 0.55 (95% CI 0.40–0.76). Due to their low incidence, encephalopathy cases were not evaluated. There is no complete scientific proof to state that computerized ST analysis minimizes the states of metabolic acidosis. Cesarean sections and also instrumental vaginal deliveries are the causes for fetal distress or other indications. At the same time, regardless of technique, STANR minimizes the number of instances which requires scalp blood sampling.
3.8 Performance index of fetal ECG extraction
The fetal ECG extraction technique is used in Vijila et al. (2005) to analyze by both observation and quantitative process. The removal of maternal ECG was displayed by extracted waveforms, and R-peaks of fetal ECG are restricted. R-peaks are recognized by the various algorithms. Let \( f(n) \) be the original signal and \( D(n) \) be the second-order difference of \( f(n) \)
If the adjacent elements \( D(i)\,\,\,{\text{to}}\, \) \( D(k) \), \( (i < k) \) are all positive ones, the threshold \( {\text{Thr}} \) is defined as
All the \( n \) fundamentals in \( D(n) \) were differentiated with the threshold \( {\text{Thr}} . \) If any element \( n_{i} \,(1 \le n_{i} \le n) \) satisfies \( D(n_{i} ) > {\text{Thr}}\,\,{\text{or}}\,\,D(n_{i} ) < - {\text{Thr}} \), then the particular elements \( x(n_{i} ) \) will be recognized as an R-peak.
Quantitative process can be analyzed by the signal-to-noise ratio (SNR) by the eigenvalue analysis and the cross-correlation estimation.
The SNR based on eigenvalues can be obtained by
where \( \lambda_{\hbox{max} } \) is the maximal eigenvalue of the M pieces of signal.
The SNR based on correlation coefficient can be obtained by
where \( \eta = \frac{2}{M(M - 1)}\sum\nolimits_{i = 0}^{M - 2} {\sum\nolimits_{k = i + 1}^{M - 1} {P(i)^{T} P(k)} } \) is the average power estimation of fetal ECG and \( p(.) \) is the signal piece.
4 Result and analysis of FECG extraction methods
In Wu et al. (2013), the simulation experimental result with the heart rate of 80 and 140 beats per minute is shown in the following figures. The three waveforms from top to bottom are replicated by abdominal signal, the replicated maternal ECG and the fetal ECG removed. It can be detected that the projected method could eliminate maternal ECG and extract fetal ECG resourcefully.
The comparison of signal-to-noise ratio is based on eigenvalue and cross-correlation of LMS algorithm and adaptive filtering algorithm as depicted in Figs. 2 and 3. Though it is illustrated that the first waveform of fetal ECG is not whole, the adaptive filter has to regulate the coefficients by the stable state. Other replicated data with dissimilar heart rates were used to extract fetal ECG, and all of them can extract fetal ECG from the simulated abdominal signals.

Comparison of signal-to-noise ratio based on eigenvalue of the least mean square algorithm and adaptive filtering algorithm (Wu et al. 2013)

Comparison of signal-to-noise ratio based on cross-correlation coefficient of the LMS algorithm and adaptive filtering algorithm (Wu et al. 2013)
4.1 FECG extraction using BANFIS
In Wen and Luo (2012), the BANFIS consists of a Bayesian filter and an adaptive neurofuzzy filter for MECG eradication and nonlinear artifacts elimination to yield high-quality FECG signal. The improved SNRs of the extorted FECG signals by the projected BANFIS are designed in Fig. 4 . The red plots indicate BANFIS using EKF, and the blue plots indicate BANFIS using EKS for different experimented signals. The input signal SNRs packed in our complete experiments were from − 30 to 15 dB. For greatly advanced SNRs, there is no notable dissimilarity between noisy and noise-free signals. Therefore, there is no use in denoising a noise-free signal, and also assessment of SNR development has no consequence.

Fetal SNR enhancement (Wen and Luo 2012)
For the complete series of the input SNRs, BANFIS was established to be very useful in improving the SNR. When the unique signal’s noise power is − 30 dB, where there is less intrusion, the standard SNR improved for FECG signal extract is 40.1 dB. Throughout the predominant noisy phase of the original input signal at 15 dB, the standard SNR improvement accomplished for the extorted fECG signal is 35.69 dB.
4.2 FECG extraction using ANFIS and PSO
In Sargolzaei et al. (2011) for both synthetic and real signals, each one of thoracic and abdominal signals has been structured in Ali and Zeng (2011). This overlaps the first for assembling the training data. The algorithm is not responsive to the frame size. We can use a better frame size if the established signals are motionless over numerous frames. Five of these signals were acquired from the mother’s abdomen, whereas the other three signals were recorded from the mother’s thoracic part. We have used one thoracic signal and one abdominal signal as the projected algorithm. There is just a requirement for one thoracic and one abdominal recorded signal. For estimating the process of the projected algorithm, we also replicate the thoracic and abdominal ECG signals using MATLAB software. Here, we will explain the transmission path, where the mother’s ECG movements from the thoracic area to the mother’s abdomen are used as a FIR filter.
Also we have explained a parameter for differentiating the outcomes of algorithms. Our prejudiced principle is percent root-mean-square difference (PRD). The declared criterion is frequently used for presentation estimation of signal compression algorithms and is explained in the below equation:
where \( x_{\text{ori}} (i) \) and \( x_{\text{rec}} (i) \) denote the original signal and reconstructed signal, respectively.
Table 8 displays the outcomes of implementing ANFIS algorithm depending on gradient descent (GD) training algorithm and our projected algorithm. This parameter displays the equivalence between the original signal and the outcome signal (Fig. 5).

Extraction from a real signal using proposed techniques a Thorax ECG, b abdominal ECG, c extracted FECG signal (Sargolzaei et al. 2011)
4.3 FECG enhancement using internal power-line reference adaptive canceler (IPRAC)
In Gupta et al. (2016), the internal power-line reference adaptive canceler (IPRAC) illustrates very good presentation in PLI cancelation devoid of disturbing the FECG morphology. The IPRAC recital is estimated on both real and fake signals with also the worst-case situation when the PLI signal does not have an absolutely constant primary frequency.
The IPRAC algorithm also legalized on actual abdominal signals where Fig. 6 exposes the PLI obstruction including the 150 Hz harmonic that is entirely detached. It permits the study of the FECG morphology. The found results support the use of noninvasive abdominal recordings in fetal monitoring, where the FECG obtained by electrodes located on maternal wall is a more attractive substitute as compared to the invasively recorded FECG, using an electrode located on the fetus scalp only after the burst of the membrane. The noninvasive feature is just one major advantage of the abdominal fetal monitoring. The technique is also quite appropriate for long-term FECG monitoring.

Performance of the IPRAC algorithm: the signal after applying the IPRAC algorithm, and the FECG obtained after removing the MECG from the signal (Gupta et al. 2016)
5 Conclusion
The fetal electrocardiogram (FECG) had its humble origin way back in the year 1901, when the preliminary growth of investigation in the related domain was considerably restricted. With the onset of enhanced amplifiers and filters, the identification of the waveform was significantly simplified. Though the surveillance of the waveform morphology was a complicated issue due to the then-prevalent background noise subsequent to the filtering of the tainted signal, the signal-to-noise ratio of the original FECG was incredibly enhanced by means of the effective signal processing and computer technologies. This was albeit the noninvasive attainment of the signals. The document exhibits the assessment of a host of approaches extensively employed for the extraction of fetal ECG extraction used until now such as artificial intelligence, wavelet transform, singular value decomposition (SVD), independent component analysis (ICA), computational intelligence, blind source separation (BSS), adaptive noise cancelation (ANC) algorithms and Bayesian methodologies. By analyzing these previous studies, we suggest to increase the performance of FECG extraction by enhancing adaptive filtering using an optimization algorithm.
References
Ahmed S, Ali X (2011) A novel technique for extraction foetal electrocardiogram using adaptive filtering and simple genetic algorithm, pp 75–81
Amin MS, Mamun M, Hashim FH, Husain H (2011) Separation of fetal electrocardiography (ECG) from composite ECG using adaptive linear neural network for fetal monitoring. Int J Phys Sci 6(24):5871–5876
Castillo E, Morales DP, Botella G, García A, Parrilla L, Palma AJ (2013) Efficient wavelet-based ECG processing for single-lead FHR extraction. Digit Signal Proc 23:1897–1909
Desai KD, Sankhe MS (2012) A real-time fetal ECG feature extraction using multiscale discrete wavelet transform. In: 5th International conference on bio medical engineering and informatics
Dhage N, Madhe S (2014) An automated methodology for FECG extraction and fetal heart rate monitoring using independent component analysis. In: IEEE international conference on advanced communication control and computing technologies
Gupta P, Sharma KK, Joshi SD (2016) Fetal heart rate extraction from abdominal electrocardiograms through multivariate empirical mode decomposition. Comput Biol Med 68:121–136
Jagannath DJ, Immanuel Selvakumar A (2015) Superior foetal electrocardiogram signal elicitation using a novel artificial intelligent bayesian methodology. Appl Soft Comput 37:1002–1017
Jagannatha DJ, Immanuel Selvakumar A (2014) Issues and research on foetal electrocardiogram signal elicitation. Biomed Signal Process Control 10:224–244
Karmakar C, Kimura Y, Palaniswami M, Khandoker A (2015) Analysis of fetal heart rate asymmetry before and after 35 weeks of gestation. Biomed Signal Process Control 21:43–48
Karvounis EC, Tsipouras MG, Papaloukas C, Tsalikakis DG, Naka KK, Fotiadis DI (2010) A non-invasive methodology for fetal monitoring during pregnancy. Methods Inform Med 49:238–253
Luo D (2012) Research and application of fetal electrocardiogram blind signal separation technology. Res J Appl Sci Eng Technol 4(14):231–2235
Maier C, Dickhaus H (2014) Extraction of respiratory myogram interference from the ECG and its application to characterize sleep-related breathing disorders in atrial fibrillation. J Electrocardiol 47:826–830
Morales DP, García A, Castillo E, Carvajal MA, Parrilla L, Palma AJ (2013) An application of reconfigurable technologies for non-invasive fetal heart rate extraction. Med Eng Phys 35:1005–1014
Nasiri M, Faez K, Nasrabadi AM (2011) A new method for extraction of fetal electrocardiogram signal based on adaptive nero-fuzzy inference system. In: IEEE international conference on signal and image processing applications
Nasiri M, Faez K, Nasrabadi AM (2011) A new method for elicitation of fetal electrocardiogram signal based on adaptive nero-fuzzy inference system. In: IEEE international conference on signal and image processing applications ICSIPA, pp 456–461
Nasiri M, Faez K, Motie A (2012) Fetal electrocardiogram signal elicitation by ANFIS trained with PSO method. Int J Electric Comput Eng 2:247–260
Niknazar M, Rivet B, Jutten C (2012) Fetal ECG extraction by extended state Kalman filtering based on single-channel recordings. IEEE Trans Biomed Eng 60(5):1345–1352
Prasanth K, Paul B, Balakrishnan AA (2013) Fetal ECG extraction using adaptive filters. Int J Adv Res Electric Electron Instrument Eng 2(4):1483–1487
Rahman MZU, Shaik RA, Rama Koti Reddy DV (2011) Efficient sign based normalized adaptive filtering techniques for cancelation of artifacts in ECG signals: application to wireless biotelemetry. Signal Process 91:225–239
Raja CG, Harsha VS, Gowthami BS, Sunitha R (2015) Virtual instrumentation based fetal ECG extraction. In: 4th International conference on eco-friendly computing and communication systems, procedia computer science, vol 70, pp 289–295
Romero I (2010) PCA-based noise reduction in ambulatory ECGs. Comput Cardiol 37:677–680
Ruffo M, Cesarelli M, Romano M, Bifulco P, Fratini A (2010) An algorithm for FHR estimation from foetal phonocardiographic signals. Biomed Signal Process Control 5:131–141
Salmelin A, Wiklund I, Bottinga R, Brorsson B, Ekman-Ordeberg G, Grimfors EE, Persson E (2013) Fetal monitoring with computerized ST analysis during labor: a systematic review and meta-analysis. Acta Obstet Gynecol Scand 92:28–39
Sargolzaei A, Faez K, Sargolzaei S (2011) A new method for foetal electrocardiogram elicitation using adaptive nero-fuzzy interference system trained with PSO algorithm. In: IEEE international conference on signal and image processing applications ICSIPA, pp 1–5
Stampalija T, Casati D, Montico M, Sassi R, Rivolta MW, Maggi V, Ferrazzi E (2015) Parameters influence on acceleration and deceleration capacity based on trans-abdominal ECG in early fetal growth restriction at different gestational age epochs. Eur J Obstet Gynecol Reprod Biol 188:104–112
Swarnalatha R, Prasad DV (2010) A novel technique for extraction of FECG using multistage adaptive filtering. J Appl Sci 10(4):319–324
Vijila CKS, Kanagasabapathy P, Johnson S (2005) Adaptive neuro fuzzy inference system for extraction of FECG. In: Proceedings of IEEE India annual conference, pp 224–227
Vullings R, De Vries B, Bergmans JWM (2011) An adaptive kalman filter for ECG signal enhancement. IEEE Trans Biomed Eng 58:1094–1103
Wen X, Luo D (2012) Performance comparison research of the FECG signal separation based on the BSS algorithm. Res J Appl Sci Eng Technol 4(16):2800–2804
Wu S, Shen Y, Zhou Z, Lin L, Zeng Y, Gao X (2013) Research of fetal ECG extraction using wavelet analysis and adaptive filtering. Comput Biol Med 43(10):1622–1627
Yin Y, Ye M, Ren D, Zhu Y, Yang C (2010) FECG extraction using Bayesian inference and neural networks approximation. J. Comput Inform Syst 6:1769–1778
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Communicated by V. Loia.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mohammed Kaleem, A., Kokate, R.D. A survey on FECG extraction using neural network and adaptive filter. Soft Comput 25, 4379–4392 (2021). https://doi.org/10.1007/s00500-020-05447-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00500-020-05447-w