
Abstract
This paper presents a novel approach for evaluating the smart medical device selection process in a group decision-making setting in an uncertain decision environment. Intuitionistic fuzzy Choquet integral (IFCI) approach is applied to treat the uncertainty and vagueness in the decision-making process. IFCI also considers the interactions among the decision criteria in the data provided by the decision makers. In this paper, the emphasis is placed upon the selection of wearable monitoring devices for cardiac patients. The goal is to present the complexity of the problem, raise interest among specialists in the healthcare industry and assess smart medical devices under different evaluation criteria. The problem is formulated as a multi-criteria decision model with ten criteria and eight alternatives. The results of the IFCI model are analyzed using 9 sensitivity analysis scenarios, which prove the adequacy of the obtained results. The result of the proposed method is also compared with the IF extensions of the VIKOR, TOPSIS, COPRAS, MOORA and MULTIMOORA models in order to validate and verify the obtained outcome. The Spearman coefficient of correlation is applied to check the stability of the variations in the rankings. The results indicate that the model and the rankings it generates are sufficiently stable.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
A rapid growth is observed in the number of medical devices in the light of emerging digital technologies and their applications in medical systems. The first driving factor in this progress is primarily based on the developments in the sensor and actuator technology, which are becoming more capable in integrating with chemical and electrical elements. Developments in the fields of micro-/nanotechnology make it easier for better data gathering, communication with external systems, and more and more substances to be detected that can be injected directly into human body. Minimally invasive or noninvasive small-scale medical tools present important challenges to creating new smart and robust devices. Portable and wearable devices today can monitor and measure the heart or brain signals. Medical robots are gaining new abilities to perform different medical tasks. Digitalization is revolutionizing the delivery of healthcare services both at homes and in hospitals by using surgical robots for assistance during complex procedures or for simpler routine tasks, such as administration of medicines to patients. In the future, more advanced medical devices can perhaps even enable patients to access healthcare services without the need of physically being present in hospitals. In this picture, smartphone apps can support patients to not only remotely access these services, but also interact with medical devices attached to the patient. New smart devices can potentially be fixed to the human body in the form of, e.g., skin patches, smart woven textiles or small implants. Current trends in the medical industry focus on collecting data from patients with such technologies in order to support medical staff in better understanding patients’ vital information. Thanks to these technologies, traditional ward rounds can soon become a thing of the past. Instead of medical staff visiting patients to take notes of their vital information, biosensors can overtake these tedious tasks in the form of a wearable patch with their electrocardiography electrodes with axis accelerometer to detect and record the breathing rate, temperature and heart rate, etc. These smart, wearable and connected devices can also be linked to external smartphones or tablets for analyzing the results.
As a response to this market growth in novel wearable medical devices and a wide availability of different devices, the healthcare industry is actively pursuing new ways on how to select those devices that best address the needs of patients. These needs can sometimes be uncertain and vague, as they are associated with the demands and expectations of human beings. Therefore, medical devices can be selected on the basis of properly selected decision criteria, such as their reliability, accuracy and precision. One of the purposes of this study is to propose a set of evaluation criteria for the healthcare industry in relation to the selection and evaluation of smart wearable devices and their outcome measures for real-life situations. These evaluation criteria are collected from the current literature, available regulations to date and the judgments of industrial and academic experts.
Decision making is mostly about selecting the best option among the set of available alternatives by considering the impact of many criteria at the same time. Since the early 1970s, the multi-criteria decision-making (MCDM) methodology is evolving and has been one of the key research areas in solving complex decision problems in the presence of multiple objectives or criteria (Lertprapai 2013). In the wake of this progress, several different types of MCDM methods are proposed to successfully solve many types of decision-making problems. The MCDM theory can be used to solve many ranking and evaluation problems that integrate a number of conflicting criteria. For decision makers (DMs), this powerful theory often entails quantitative and qualitative data which are used in the measurement of available alternatives’ performance per relevant decision criteria. In many MCDM problems, interactivity or interdependency features among decision criteria are mutual and many concepts are of an uncertain nature, which obscures the assignment of a membership function (Joshi and Kumar 2016). Most of the ordinary MCDM approaches, however, rely on crisp numerical values, which is why such methods mostly prove inadequate in solving real-life problems. To overcome this difficulty, many MCDM approaches have been extended to make use of the fuzzy set theory. Nevertheless, fuzzy numbers are also not always sufficient.
The fuzzy logic, known as type-1 ordinary fuzzy sets, can be extended to type-2 fuzzy sets, in which the membership degree itself in ordinary fuzzy sets is measured as a fuzzy number. Type-2 fuzzy sets have proven to be successful in some applications. Nevertheless, it is our view that it is a compromise and that intuitionistic fuzzy (IF) sets offer great potential (Büyüközkan and Göçer 2017). In cases where the given information is not adequate to define its inexactness and in situations where there is lack of precision due to the limitations imposed by the conventional fuzzy or crisp sets, the concept of IF sets provides a substitute approach. Characterized by a membership degree, a nonmembership degree and a hesitancy degree, IF sets are very strong and successful in handling situations under vagueness, uncertainty and imprecision. Thus, IF sets offer a capable tool for expressing DMs’ preferences and properly defining the membership function in cases where DM opinions are subject to hesitation or lack of expertise.
Many decision problems faced in regular life necessitate the contribution of more than one DM in the decision-making processes. Therefore, most of the MCDM approaches are also extended to group decision making (GDM). The key advantage of IF sets over the crisp or classical fuzzy sets is their ability to distinguish the positive and the negative indications of an element’s values on membership and nonmembership in the sets. When DMs express their opinions, they mostly rely on information about completely nonindependent criteria. To overcome these complications, a widely accepted MCDM approach is the Choquet integral (CI) method with a major advantage over multiple conflicting and often interacting criteria (Büyüközkan and Ruan 2010; Büyüközkan et al. 2009, 2018a, c). Aggregation operators are quite useful in information summarizing and have been widely used. In this context, the CI has taken a leading role (Belles-Sampera et al. 2014). Many other IF set aggregation operators are proposed in cases where almost all of them only consider independent decision-making problems. In contrast, the components of IF sets usually have interaction properties. Hence, using CI is very efficient in finding the expected utility of an uncertain situation. Based on these interaction properties, the IFCI operator is proposed by Xu (2010), Tan and Chen (2010) in chronologic order. Due to its multi-criteria nature, this paper proposes an MCDM approach to evaluate the smart medical device selection process with a GDM approach in an uncertain environment. A significant feature of this analysis is the interactions among the decision criteria that are applied to the smart medical device evaluation. These interactions are handled with a method based on IFCI. To the best of authors’ knowledge, the approach in this study has not yet been applied for any types of medical device selection in the literature to this extent. The proposed approach makes use of IF set properties and integrated CI method under GDM to consider a wide range of different scenarios and attitudes and to select the most suitable alternative in accordance with desired interest for the assessment of smart medical devices. The main contribution of this paper is the characterization and elaboration of an effective evaluation framework to guide the medical industry for the suitable smart medical device selection. This research also contributes to the literature by providing a novel IFCI method under GDM setting by considering the interactions among medical device selection criteria.
Structure of this paper is summarized as follows. In Sect. 2, review of related publications is given. Then, Sect. 3 provides a simple introduction to IF sets and explains the detailed steps of the proposed method structure. Section 4 gives a detailed explanation of the alternatives and evaluation criteria in a case study, in which wearable cardiac monitoring devices are selected to present the performance of the applied method. Managerial implications are discussed in Sect. 5 with a comparison of different MCDM techniques and a sensitivity analysis. Finally, the last section discusses the results and limitations of this study.
2 Related literature
The following review about the smart medical devices literature indicates a research gap between the practice and theory. Presently, there are a limited number of studies exploring the field of smart medical devices. As far as we know, there is no academic study so far that explicitly deals with the concept of smart medical devices in connection with MCDM. Those studies discuss related technologies or their specific applications. The following review assents this proposition.
Stoppa and Chiolerio (2014) review the recent advances in the field of smart textiles and pay particular attention to the materials and their manufacturing process. Vashist et al. (2014) provide a critical review of widely used personalized healthcare monitoring, smartphone-based devices and their applications. Walsh et al. (2014) give a comprehensive overview of novel wireless cardiac monitoring devices that are available as well as the technologies that are currently under development and poised to revolutionize the way cardiology is practiced. Khan et al. (2016) review the latest development in flexible and wearable human vital sensors. Gómez-Mascaraque et al. (2014) have a book chapter about the types of smart polymers, the technologies used for their production and their applications in the field of medical devices. In another recent book chapter presented by Sliwa (2016), smart medical device data reuse for quality control and evidence-based medicine is explored.
This shows that the literature in the context of smart medical devices is quite limited. There are, however, recent studies focusing on the employed technique, which can give us an understanding of the proposed method’s utilization areas and features. As readers go through the review, they will notice that the proposed method is different from the existing ones and its originality comes from its ability to present a distinctively different approach which applies CI operator using GDM settings under IF set theory for selecting wearable cardiac monitoring devices.
On the methodology side of the review, decision making in real-world situations is the means of choosing the best candidate among several. It is imperative to DMs to simultaneously consider multiple criteria in order to select the best candidate. MCDM methods are widely developed and used by scholars since the early 1970s. In case of multiple objectives or criteria, MCDM methods embody a fundamental area of research to deal with complex problems. Several MCDM methods with distinguishing features have been proposed in the literature, such as Višekriterijumsko Kompromisno Rangiranje (VIKOR) (Opricovic 1998), Technique for Order of Preference by Similarity to Ideal Solution (TOPSIS) (Hwang and Yoon 1981), Complex Proportional Assessment (COPRAS) (Zavadskas et al. 1994), Multi-Objective Optimization on the basis of Ratio Analysis (MOORA) (Brauers and Zavadskas 2006), MOORA plus the Full Multiplicative Form (MULTIMOORA) (Brauers and Zavadskas 2010), Weighted Aggregated Sum Product Assessment (WASPAS) (Zavadskas et al. 2012), Evaluation based on Distance from Average Solution (EDAS) (Keshavarz Ghorabaee et al. 2015), Multi-Attributive Border Approximation area Comparison (MABAC) (Pamučar and Ćirović 2015), Multi-Attributive Ideal-Real Comparative Analysis (MAIRCA) (Gigović et al. 2016; Pamučar et al. 2017) and Best–Worst Method (BWM) (Rezaei 2015; Rezaei et al. 2015), among others.
Many types of MCDM methods have been successfully applied to different types of decision-making problems. Since these methods mostly run with crisp sets, they have been seen insufficient to deal with many decision problems. As decision making gets more complicated, the task of identifying the best candidate also becomes more challenging for a DM. Thus, many such techniques are successfully extended to other world environments. Zadeh (1965) has been the most influential author by far in fuzzy research (Merigó et al. 2015; Blanco-Mesa et al. 2017), introduced the concept of ordinary fuzzy sets in which each element of a set is given a membership value. Most of the studies in the literature apply the classical fuzzy set theory due to its similarity to human reasoning. Following that, Atanassov (1986) introduced the concept of IF sets, which is the generalized concept of Zadeh’s ordinary fuzzy sets, where each element of the set is given a nonmembership value in addition to its membership value. Many different types of MCDM approaches are integrated by IF sets. When compared to the classical fuzzy set, IF sets have many advantages in the sense that they are more adequate and capable of identifying DMs’ judgments. Consequently, it is widely studied in the last decades by numerous researchers (Büyüközkan and Güleryüz 2016a; Büyüközkan and Göçer 2017, 2018; Büyüközkan et al. 2017, 2018a, b, c).
The mutual relationship among decision criteria is ignored in almost all of these traditional methods. The CI method, on the other hand, allows criteria to be dependent on each other, which is represented by a fuzzy measure with a weight given to each criteria combination (Büyüközkan et al. 2018a). In this section, studies about CI integrated with IF sets are reviewed with an emphasis on the employed technique. Tan and Chen (2010) presented one of the first studies about IFCI, in which the interactions among the decision-making criteria are considered. They discussed the special t-norms and t-conorms properties to show that the IFCI operator can be utilized. Xu (2010) also uses the CI approach to offer an aggregation operator on IF sets. They consider not only the importance of the elements or their ordered positions, but also the correlations among the elements or their ordered positions. In another study, Tan (2011) examines the extension of TOPSIS, an MCDM technique, under IF settings for a GDM environment, where interdependent characteristics among decision criteria are taken into account. Ashayeri et al. (2012) present an operator for IFCI-based approach for the configuration and partner selection. Considering IFCI literature, Tuzkaya (2013) suggests an MCDM approach utilizing the decision environment’s vagueness and interactions among decision criteria and combines supplier evaluation processes in terms of IFCI operator. Wu et al. (2013) present the integration properties of the IFCI using the improper applications of CI. Similar versions of the proposed method are successfully applied to urban transportation and Web site evaluation in earlier studies (Büyüközkan et al. 2018a, c). Table 1 provides a more detailed review of these publications within the scope of IFCI. The given method in this study is presented in detail in the next section.
3 Proposed methodology
The aim of the proposed method is to develop a conceptual framework for evaluation and to prioritize smart medical devices with regard to predefined objectives. The next subsection gives the preliminary explanations about IF and CI, respectively. After that, the proposed method is introduced.
3.1 Preliminaries
Basics of IF sets are briefly introduced in this subsection. Atanassov (1986) defines a fixed crisp set E and A ⊂ E, also a fixed set. An IFS, \( A^{*} \), in E is an object of the following form;
Here the degree of the membership is defined by the functions: \( \mu_{A} : E \to [0, 1] \) and \( v_{A} : E \to [0, 1] \), as well as the degree of nonmembership of the element \( x \in E \) to the set A, respectively, and for all \( x \in E \);
then \( \pi_{A} (x) \) is defined as the degree of uncertainty of the membership of element \( x \in E \) to set A. In the ordinary fuzzy sets case, \( \pi_{A} (x) = 0 \) for all \( x \in E \).
The CI technique is proposed by Gustave Choquet in (1954) as a scientific method to aggregate criteria which allow the selection of alternatives by considering interactions between criteria. Its use in the MCDM domain starts in the 1990s in different contexts for similar classification problems (Feyzioğlu and Büyüközkan 2008). Since its introduction by Sugeno in (1974), the concept of the fuzzy measure has also been often used in MCDM settings. After this date, CI is revalued in terms of fuzzy measure. These fuzzy integrals have been applied to various MCDM evaluation and prediction problems. IFCI operator in Eq. (9) is offered by Xu (2010) and also by Tan and Chen (2010) almost at the same time.
3.2 IFCI method
This section presents the proposed IFCI method. The steps of the method are as follows:
Step 1
Construct a committee of DMs and define the objective, evaluation criteria and alternatives.
Assume that K DMs want to evaluate the set of n criteria and m alternatives. DMs are represented by \( D_{k} = \{ D_{1} , D_{2} , \ldots , D_{K} \} \), where \( k = 1, 2, \ldots , K \), and alternatives are represented by \( A_{i} = \{ A_{1} , A_{2} , \ldots , A_{m} \} \), where \( i = 1, 2, \ldots , m \), each assessed on n criteria \( C_{j} = \{ C_{1} , C_{2} , \ldots , C_{n} \} \), \( j = 1, 2, \ldots , n \).
Step 2
Design and identify the linguistic scales to weight DMs and to assess the alternatives.
Step 3
Obtain DMs’ judgments on each factor.
DMs are asked to deliver their judgments based on their prior knowledge and expertise on the topics. Each DM provides his/her judgment on each of these factors linguistically.
-
(a)
Gather the judgments of DMs about each other. DMs are asked to express their opinions about their qualification from the viewpoint of the kth DM.
-
(b)
Obtain the judgments on the available alternatives for each criterion. DMs are asked to express their opinions on the alternative \( A_{i} \) over criterion \( C_{j} \) from the viewpoint of the kth DM.
Step 4
Obtain the transformation of IF values.
When all DMs give their evaluations on each factor, the IF value preference scale in Table 2 is used.
-
(a)
Convert DMs’ linguistic evaluations into IF values. For each DMλk\( (1 < k < K) \), DM “k” gives his/her judgment about the other DMs with the help of the linguistic weighting terms shown in Table 2.
-
(b)
Establish the preference relation matrix with the help of IF values. DMs use the linguistic terms shown in Table 2 to evaluate the ratings of alternatives with respect to each criterion. Let \( (R_{ij}^{k} ) \) be an IF decision matrix of the kth DM for the alternatives.
$$ \left( {R_{ij}^{k} } \right) = \left[ {\begin{array}{*{20}l} {r_{11}^{k} } \hfill & \cdots \hfill & {r_{1n}^{k} } \hfill \\ \vdots \hfill & \ddots \hfill & \vdots \hfill \\ {r_{m1}^{k} } \hfill & \cdots \hfill & {r_{mn}^{k} } \hfill \\ \end{array} } \right], \quad k \in K $$(3)where \( r_{ij}^{k} = (\mu_{ij}^{k} , v_{ij}^{k} , \pi_{ij}^{k} ) \), \( k = 1, 2, \ldots , K \), \( i = 1, 2, \ldots , m \) and \( j = 1, 2, \ldots , n \).
Step 5
Obtain the weights of DMs.
DMs’ judgments are aggregated by the IF weighted average (IFWA) (Xu and Cai 2012) operator, given in Eq. (4). Then, the priority of the kth DM is acquired by means of Eq. (5). Here, \( D_{k} = (\mu_{k} ,v_{k} ,\pi_{k} ) \) is an IF value and the priority degree of DM \( D_{k} \) is \( \lambda_{k} = \{ \lambda_{1} , \lambda_{2} , \ldots \lambda_{K} \} \), where \( \sum\nolimits_{k = 1}^{K} {\lambda_{k} } = 1 \).
Step 6
Aggregate the individual IF values into group IF values.
The aggregation of IF preference relation matrix based on all DMs is constructed. Individual opinions of the DMs are aggregated into an IF decision matrix using the IFWA aggregation operator given in Eq. (6).
Equation (6) is applied to aggregate \( R_{ij}^{k} \). The \( \tilde{A}_{ij} \) matrix as illustrated in Eq. (7) is obtained with an aggregation of each DM’s opinions.
Step 7
Obtain score values and accuracy values.
Let \( \tilde{a}_{ij} = (\mu_{ij} ,v_{ij} ,\pi_{ij} ) \) be IF values for alternative \( A_{i} \) with respect to \( C_{j} \). The score function \( S(\tilde{a}_{ij} ) \) and the accuracy function \( H(\tilde{a}_{ij} ) \) are calculated using Eq. (8).
Step 8
Obtain the ordered list of evaluation criteria.
Rank partial evaluation \( \tilde{a}_{ij} \) of alternative \( A_{i} \). \( i = 1, 2, \ldots , m \), \( j = 1, 2, \ldots , n \) and \( l = 1, 2, \ldots , n \) (Xu and Yager 2006).
List the rank of score and accuracy values.
Step 9
Obtain the reordered list of evaluation criteria.
Reorder the partial evaluation of alternative Ai so that \( \tilde{a}_{i(j)} \le \tilde{a}_{i(j + 1)} \) for each alternative in ascending order by their listed ranks of score and accuracy values in Step 8.
Step 10
Obtain the fuzzy measure using the pairwise comparison.
There are different ways to determine the fuzzy measure (\( m(A_{(j)} ) \)) (Tan and Chen 2010). In this paper, the common gateway interface (CGI) system (Takahagi 2000) is applied. The individual weight of each criterion \( w_{j} = \{ w_{1} , w_{2} , \ldots , w_{n} \} \), \( \sum\nolimits_{j = 1}^{n} {w_{j} = 1} \), is also acquired in this step.
Step 11
Obtain the results of the IFCI operator.
Use the IFCI operator in Eq. (9) to obtain the results.
Step 12
Find the ranking of alternatives.
The ranks are obtained with the following Eq. (10). Let \( \tilde{A}_{i} = (\mu_{i} ,v_{i} ,\pi_{i} ) \) be in the form of IF values, where \( i = 1, 2, \ldots , m \).
Sort \( S_{i} \) in an ascending order, the rank of \( i \) being the ranking order of the associated alternative. If there are any equal \( S_{i} \) values, then sort \( H_{i} \) in ascending order. If there are any equal \( H_{i} \) values, then related \( A_{i} \) values are represented as equal.
Figure 1 gives the illustration of the proposed method in a schematic diagram to illustrate the flow of steps. The next section presents the application of the proposed method in a real case study from the healthcare industry.

The schematic diagram of the proposed IFCI method
4 Case study
The way we live is hugely altered by the digital revolution and the rapid development of social networking, mobile connectivity and smartphones. An average person in a developed country is constantly connected to a vast network of information. This revolution era on digitalization has not only conspicuously transformed every industry, but also every facet of people’s personal lives. The healthcare industry is no different. This industry has been quick in adopting smart, digital ubiquitous devices. Recently, another novel device has emerged for monitoring cardiac patients. The authors believe that the evolution of these smart cardiac monitoring devices marks a new era for cardiac patients and the medical industry. Currently, there are numerous companies competing on the development of wearable cardiac monitoring devices for cardiac patients.
Step 1
A committee consisting of four DMs, \( \{ {\text{DM}}_{1} ,{\text{DM}}_{2} , {\text{DM}}_{3} , \;{\text{and}}\;{\text{DM}}_{4} \} \), is constructed to evaluate eight different wearable cardiac monitoring alternatives \( A_{i} \); \( \{ A_{1} , A_{2} , \ldots , A_{8} \} \) manufactured by medical device producers. DMs’ committee is constructed with two industrial experts and two scholars dealing explicitly with smart medical devices. The proposed smart medical device evaluation approach is tested for eight smart cardiac monitoring devices. Company names are undisclosed due to privacy, whereas brief explanations for each product are presented in Table 3 to validate the evaluation criteria and usability of the proposed method. These alternatives are assessed based on ten comprehensive evaluation criteria \( C_{j} \), \( \{ C_{1} , C_{2} , \ldots , C_{10} \} \), which are gathered from an extensive examination of literature and DMs’ opinions. Detailed explanations of the evaluation criteria are given in Table 4.
Step 2
A nine-point IF preference scale in Table 2 is used to weight DMs and to assess the alternatives.
Step 3
Judgments of DMs about each other are given in Table 5. The judgments on alternatives based on each criterion are given in Table 6.
Step 4
DMs’ linguistic evaluations gathered in the previous step are converted into IF values. The whole preference relation matrix is omitted for contextual focus and space limitations. A sample is given on Alternative \( A_{2} \) in Table 7. The transformed IF values for DMs’ evaluations are also given in Table 8.
Step 5
IF values taken individually for each DM are aggregated with Eq. (4). Their respective priorities are calculated with Eq. (5). The aggregation matrix and weights of DMs are given in Table 8. A sample for the \( {\text{DM}}_{2} \) is given below.
Step 6
Individual opinions of DMs are aggregated into an IF decision matrix with the IFWA aggregation operator, as shown in Eq. (6). The aggregated matrices are given in Table 9. A sample aggregation is illustrated below.
Step 7
Score values and accuracy values are calculated with Eq. (8).
A sample calculation is given below. All score and accuracy values are given in Table 10.
Step 8
Orders of the evaluation criteria are sorted according to the calculated score and accuracy values, as given in Table 10.
Step 9
Reordered list of the evaluation criteria is given in Table 11 in ascending order.
Step 10
CGI is used to obtain the fuzzy measure.
The relevant fuzzy measures are displayed in Table 12. For example, for \( A_{2} \) some of the fuzzy measures are:
Step 11
IFCI operator in Eq. (9) is applied to get the results in Table 13. An illustration is given below for the second alternative.
Step 12
Ranking of alternatives is calculated by Eq. (10) according to the defined procedure. Table 13 gives the calculated rankings.
As the above evaluations suggest, the third alternative is selected as the best one, while the seventh alternative is the worst in the analysis.
5 Managerial implications
The growth of wearable, software-based and networked medical devices is opening a new era for extending human life and enhancing its quality. The emergence of these smart devices is becoming a major disruptive trend for the medical industry, which is evolving to create better tools in aiding patients and medical staff to manage health conditions outside healthcare facilities. Many of these technological wearable medical devices and applications are categorized as noninvasive sensors, invasive or implantable and programmable sensors, robots, home health devices, hospital equipment and smartphone apps. More recently, novel smart medical devices have emerged in monitoring the status of cardiac patients. This study offers a novel approach that focuses on the evaluation and ranking of smart medical devices. The decisions on the selection of wearable cardiac monitoring devices are difficult. Such decisions need to be taken carefully by considering different perspectives. Due to the problem’s MCDM nature, the proposed method employs the CI technique under GDM with IF sets. A practical study is presented for eight wearable cardiac monitoring devices to prove the proposed method’s viability and validity. According to the analysis, the proposed method ranks the alternative A5 as the best smart medical device, while \( A_{8} \) is ranked last. This IFCI method is relevant not only in evaluating and ranking the DMs’ importance, but also in aggregating individual decisions into a GDM judgment. Subjective and objective preferences are considered in measuring DMs’ priority and criteria weights. Since a GDM process is incorporated into the ranking procedure, the calculated weights are more comprehensive.
Many MCDM problems deal with uncertainty or imprecision using several types of distinctive objective world environments. Therefore, the terminology may differ, such as the probability theory, ordinary fuzzy set theory, rough set theory or IF set theory, besides others. The rough set theory, for example, is a quite suitable technique in order to address imprecise and uncertain conditions without the impact of subjectivity (Pamučar et al. 2018a, b). The extension of ordinary fuzzy sets to type-2 fuzzy sets is proven successful in some applications. However, it is our view that it is a compromise and that IF sets have great potential (Büyüközkan et al. 2018b). Following the previous objective world environments, the IF set theory is a new mathematical tool to deal with uncertain, imprecise, vague and inconsistent knowledge. The concept of IF sets can be seen as a relevant approach in cases where the ordinary fuzzy sets, crisp sets or other objective world environments are insufficient in defining the vagueness or when there is a lack of accuracy of collected information. The fundamental key advantage of IF sets over the classical fuzzy or crisp sets is its differentiation of the positive and the negative indication for the membership and nonmembership of an element in the set (Büyüközkan and Göçer 2017).
IFCI does not only consider the interaction among criteria. It also processes multiple criteria that are used by IF sets. MCDM techniques can effectively be utilized in real case problems so that the interaction phenomena can be modeled and the independence of criteria can be taken into account. In the CI method, selected evaluation criteria can be dependent on each other, where the priority of each combination of criteria is defined with a fuzzy measure, ensuring that the interactions among criteria are well modeled (Fodor et al. 2000). The proposed method demonstrates its strength by seeing DMs’ judgment preferences as personal opinions and real needs, while many other methods assume that DMs are fully rational and objective, ignoring subjective personal thoughts, prejudices and wishes.
Table 15 shows that the most important criteria are cost and safety, respectively. This is quite understandable, as smart medical devices are still in their baby steps. In situations like these, CI’s property becomes particularly useful for expressing decision behaviors involving interactions among criteria (e.g., if \( C_{2} \) is satisfied, then \( C_{5} \) is not important; otherwise, \( C_{5} \) is important). The principal reason why the proposed method returns superior results than existing methods is that it considers DMs’ opinions more precisely and produces more appropriate and precise outcomes according to the DMs’ actual needs and preferences by utilizing the IF sets. Hence, the outcome obtained by the IFCI method is more precise and realistic compared to alternative methods in the literature. In order to validate the confirmation of this strong claim, the following sections are presented.
5.1 Comparative analysis
The proposed IFCI approach is compared with the results of IF VIKOR (Büyüközkan et al. 2016), IF TOPSIS (Büyüközkan and Güleryüz 2016b; Büyüközkan and Gocer 2017), IF COPRAS, IF MOORA and IF MULTIMOORA (Büyüközkan et al. 2018b) as given in Table 14. These comparisons with different MCDM methodologies illustrate a distinctive difference among rankings. The lowest ranking alternative is the same in all methodologies; however, the rest of the rankings are aligned differently. The authors conclude that the property of IFCI in considering interactions among criteria lead to more accurate and realistic results for IFCI than other MCDM techniques.
It is obvious that a straightforward comparison can be misleading. In order to discuss the usefulness of the ranking found by the IFCI approach, a sensitivity analysis is applied to evaluate the performance of alternatives in which the importance of criteria weights is varied. Therefore, the next subsection presents a sensitivity analysis to demonstrate the validity and viability of the proposed method compared to other MCDM methodologies. Similar types of comparisons are presented by some researchers (Ashtiani and Azgomi 2016; Wang et al. 2016; Büyüközkan and Göçer 2017), however, usually with one method.
5.2 Sensitivity analysis
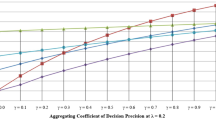
The sensitivity analysis is performed by changing the criteria weights, which is common in both IFCI and other MCDM techniques under IF environment to check whether the ranking changes. The IFCI fuzzy measure and related IF MCDM criteria weights are encompassed within sensitivity analysis. Case 0 displays the actual criteria weights calculated by the CGI system as presented in Table 3. Nine different cases, in which the criteria weights are altered as displayed in Table 15, are applied in the sample. Figure 2 presents the outcome of the obtained rankings.

The ranking outcome of sensitivity analysis
In Fig. 2, the first cases of IFCI and other MCDM methodologies show the current situation and ranking. The next cases indicate the results when the criteria weights are varied. In other words, the ranking of the alternatives changes utterly and the problem is not dynamic, where the alternatives are evaluated with respect to their current performance. The sensitivity analysis in ranking the results of both the IFCI method and MCDM methods shows that similar pattern occurs as the weights of criteria are altered.
In the light of this analysis, the alternatives \( A_{3} \) and \( A_{6} \) share the first position in most cases. Since the DMs have assumed monotonically altering weights, the readers should consider cases 1, 5, 6 and 8. Consequently, the alternative \( A_{3} \) emerges as the best one according to these cases. Nevertheless, since the proposed method uses both the IF sets concept and CI approach, it experimentally outperforms other approaches. The advantages and distinguishing characteristics of the proposed method are detailed in the earlier subsections.
5.3 Spearman’s ratio correlation
Our extensive literature review on how to find the relationship among rankings of different approaches shows that the Spearman coefficient of correlations seems to be a good approach. This approach has already been successfully applied in various publications (Ghorabaee et al. 2016; Pamučar et al. 2018a, b; Chatterjee et al. 2018; Stojić et al. 2018). Its properties as a nonparametric rank or statistical dependence correlation make it a useful tool for this study. This study uses it to find the relationship among rankings obtained by the proposed approach and other MCDM methodologies. It is also used to check the rankings obtained by altering the weights in the sensitivity analysis section. Spearman’s correlation coefficient shows an effect size, in which the strength of the correlation can be verbally described by using the following values of the obtained values: The values “0.00–0.19,” “0.20–0.39,” “0.40–059,” “0.60–0.79” and “0.80–1.00” indicate “Very Weak,” “Weak,” “Moderate,” “Strong” and “Very Strong” statistical significance, respectively. Table 16 displays the correlations among various MCDM methods under IF environment. As also indicated in (Pamučar et al. 2018a), if the Spearman coefficient value is greater than 0.8, it shows extremely high correlation and thus the association between the two rankings would be considered statistically significant. In the cases of MCDM comparisons, very strong correlations exist between the proposed IFCI approach and two other methods, i.e., IF TOPSIS and IF COPRAS. Also, strong correlations exist in between IFCI and IF MOORA, while only moderately strong correlations exist between the proposed IFCI approach and two other methods, i.e., IF VIKOR and IF MULTIMOORA.
Spearman’s correlation is also used to check the correlations among different weight combinations using nine different cases. Coefficient values are displayed in Table 17 for the nine cases of weights, which shows that there is a positive monotonic correlation between the rankings obtained. Since in all of the cases coefficient values vary from case to case, we can come to a verdict that the correlation between the proposed IFCI approach under altered weights generates different statistical significance. This analysis also confirms that the ranking of the alternatives changes utterly and the problem is not dynamic. Based on these analyses of obtained rankings, the Spearman ratio correlation validates the results of the comparisons and the sensitivity analysis.
6 Concluding remarks
Better health care can be possible by continuously tracking the vitals of patients and their medical needs. Medical devices are getting smarter and being integrated into many devices such as smart watches, wearable and connected cardiac monitors and even smartphones. This paper introduces an IFCI method for an MCDM problem, which is the selection of wearable cardiac monitoring devices for cardiac patients. This method is then applied to a case study to compare eight smart medical devices using ten evaluation criteria to validate the proposed approach. Smart medical device evaluation criteria are compiled through an extensive literature review and experts’ opinions. Since CI can successfully capture and model the interactions among selection criteria, the proposed method generates more accurate and realistic results than other MCDM techniques. In order to reduce the bias and partiality of individual opinions, a group of DMs is often more advantageous than a single one. The selection process is enhanced by the use of IF values. The IF theory can hinder the loss of data and assist with the incorporation of nonnumerical, linguistic statements into analytical models. The information gathered this way is then evaluated by means of the IFCI method, a prominent technique for acquiring complete or partial rankings. The verification and validation of the proposed method are accomplished by comparison and sensitivity analyses. In order to determine the link between the results obtained in comparison and sensitivity analyses, Spearman’s coefficient of correlation is applied. Even though the introduced MCDM technique is applied for the sake of wearable cardiac monitoring device evaluation, it can also be utilized for other smart medical device evaluations.
This study is limited to the case of smart medical devices. Nevertheless, it can be adapted to other decision-making problems as well. In addition, the authors have begun researching the possibility of using the proposed methods in other wearable device selection problems. Besides, other objective world environments could be used to validate and verify the given outcome.
References
Ashayeri J, Tuzkaya G, Tuzkaya UR (2012) Supply chain partners and configuration selection: an intuitionistic fuzzy Choquet integral operator based approach. Expert Syst Appl 39:3642–3649
Ashtiani M, Abdollahi Azgomi M (2016) Trust modeling based on a combination of fuzzy analytic hierarchy process and fuzzy VIKOR. Soft Comput 20:399–421
Atanassov K (1986) Intuitionistic fuzzy sets. Fuzzy Sets Syst 20:87–96
Beg I, Rashid T (2014) Multi-criteria trapezoidal valued intuitionistic fuzzy decision making with Choquet integral based TOPSIS. Opsearch 51:98–129
Belles-Sampera J, Merigó JM, Guillén M, Santolino M (2014) Indicators for the characterization of discrete Choquet integrals. Inf Sci 267:201–216
Blanco-Mesa F, Merigó JM, Gil-Lafuente AM (2017) Fuzzy decision making: a bibliometric-based review. J Intell Fuzzy Syst 32:2033–2050
Brauers WKM, Zavadskas EK (2006) The MOORA method and its application to privatization in a transition economy. Control Cybern 35:445–469
Brauers WKM, Zavadskas EK (2010) Project management by multimoora as an instrument for transition economies. Technol Econ Dev Econ 16:5–24
Büyüközkan G, Gocer F (2017) An intuitionistic fuzzy MCDM approach for effective hazardous waste management. In: Intelligence systems in environmental management: theory and applications. Springer, Berlin, pp 21–40
Büyüközkan G, Göçer F (2017) Application of a new combined intuitionistic fuzzy MCDM approach based on axiomatic design methodology for the supplier selection problem. Appl Soft Comput 52:1222–1238
Büyüközkan G, Göçer F (2018) An extension of ARAS methodology under interval valued intuitionistic fuzzy environment for digital supply chain. Appl Soft Comput 69:634–654
Büyüközkan G, Güleryüz S (2016a) A new integrated intuitionistic fuzzy group decision making approach for product development partner selection. Comput Ind Eng 102:383–395
Büyüközkan G, Güleryüz S (2016b) Multi criteria group decision making approach for smart phone selection using intuitionistic fuzzy TOPSIS. Int J Comput Intell Syst 9:709–725
Büyüközkan G, Ruan D (2010) Choquet integral based aggregation approach to software development risk assessment. Inf Sci 180:441–451
Büyüközkan G, Feyzioǧlu O, Şakir Ersoy M (2009) Evaluation of 4PL operating models: a decision making approach based on 2-additive Choquet integral. Int J Prod Econ 121:112–120
Büyüközkan G, Arsenyan J, Ruan D (2012) Logistics tool selection with two-phase fuzzy multi criteria decision making: a case study for personal digital assistant selection. Expert Syst Appl 39:142–153
Büyüközkan G, Feyzioğlu O, Göçer F (2016) Evaluation of hospital web services using intuitionistic fuzzy AHP and intuitionistic fuzzy VIKOR. In: 2016 IEEE international conference on industrial engineering and engineering management (IEEM). IEEE, pp 607–611
Büyüközkan G, Güleryüz S, Karpak B (2017) A new combined IF-DEMATEL and IF-ANP approach for CRM partner evaluation. Int J Prod Econ 191:194–206
Büyüközkan G, Feyzioğlu O, Göçer F (2018a) Selection of sustainable urban transportation alternatives using an integrated intuitionistic fuzzy Choquet integral approach. Transp Res Part D Transp Environ 58:186–207
Büyüközkan G, Göçer F, Feyzioğlu O (2018b) Cloud computing technology selection based on interval-valued intuitionistic fuzzy MCDM methods. Soft Comput 22:5091–5114
Büyüközkan G, Göçer F, Feyzioǧlu O (2018c) Healthcare website evaluation using intuitionistic fuzzy Choquet approach. J Multiple-Valued Log Soft Comput 30:215–237
Chatterjee K, Pamucar D, Zavadskas EK (2018) Evaluating the performance of suppliers based on using the ŔAMATEL–MAIRCA method for green supply chain implementation in electronics industry. J Clean Prod 184:101–129
Cheng H, Tang J (2015) Interval-valued intuitionistic fuzzy multi-criteria decision making based on the generalized Shapley geometric Choquet integral. J Ind Prod Eng 1015:1–16
Choquet G (1954) Theory of capacities. Ann Inst Fourier 5:131–295
De Miguel L, Bustince H, Pekala B et al (2016) Interval-valued Atanassov intuitionistic OWA aggregations using admissible linear orders and their application to decision making. IEEE Trans Fuzzy Syst 24:1586–1597
Feyzioğlu O, Büyüközkan G (2008) An integrated group decision-making approach for new product development. Int J Comput Integr Manuf 21:366–375
Fodor J, De Baets B, Perny P (eds) (2000) Preferences and decisions under incomplete knowledge. Physica, Heidelberg
Ghorabaee MK, Zavadskas EK, Turskis ZZ, Antucheviciene J (2016) A new combinative distance-based assessment (CODAS) method for multi-criteria decision-making. Econ Comput Econ Cybern Stud Res 50:25–44
Gigović L, Pamučar D, Bajić Z, Milićević M (2016) The combination of expert judgment and GIS-MAIRCA Analysis for the selection of sites for ammunition depots. Sustainability 8:372
Gómez-Mascaraque LG, Palao-Suay R, Vázquez B (2014) The use of smart polymers in medical devices for minimally invasive surgery, diagnosis and other applications. In: Aguilar MR, San Román J (eds) Smart polymers and their applications. Elsevier, Amsterdam, pp 359–407. https://doi.org/10.1533/9780857097026.2.359
Hwang CL, Yoon K (1981) Multiple attribute decision making-methods and application. Springer, New York
Joshi D, Kumar S (2016) Interval-valued intuitionistic hesitant fuzzy Choquet integral based TOPSIS method for multi-criteria group decision making. Eur J Oper Res 248:183–191
Keshavarz Ghorabaee M, Zavadskas EK, Olfat L, Turskis Z (2015) Multi-criteria inventory classification using a new method of evaluation based on distance from average solution (EDAS). Informatica 26:435–451
Khan Y, Ostfeld AE, Lochner CM et al (2016) Monitoring of vital signs with flexible and wearable medical devices. Adv Mater 28:4373–4395
Lertprapai S (2013) Review: multiple criteria decision making method with applications. Int Math Forum 8:347–355
Liu Y, Wu J, Liang C (2015) Attitudinal ranking and correlated aggregating methods for multiple attribute group decision making with triangular intuitionistic fuzzy Choquet integral. Kybernetes 44:1437–1454
Meng F, Chen X (2015) Interval-valued intuitionistic fuzzy multi-criteria group decision making based on cross entropy and 2-additive measures. Soft Comput 19:2071–2082
Meng F, Tan C (2017) A method for multi-attribute group decision making based on generalized interval-valued intuitionistic fuzzy Choquet integral operators. Int J Uncertain Fuzziness Knowl Based Syst 25:821–849
Meng F, Zhang Q, Cheng H (2013) Approaches to multiple-criteria group decision making based on interval-valued intuitionistic fuzzy Choquet integral with respect to the generalized λ-shapley index. Knowl Based Syst 37:237–249
Meng F, Chen X, Zhang Q (2014a) Some interval-valued intuitionistic uncertain linguistic Choquet operators and their application to multi-attribute group decision making. Appl Math Model 38:2543–2557
Meng F, Cheng H, Zhang Q (2014b) Induced Atanassov’s interval-valued intuitionistic fuzzy hybrid Choquet integral operators and their application in decision making. Int J Comput Intell Syst 7:524–542
Meng F, Zhang Q, Zhan J (2015) The interval-valued intuitionistic fuzzy geometric choquet aggregation operator based on the generalized banzhaf index and 2-additive measure. Technol Econ Dev Econ 21:186–215
Merigó JM, Gil-Lafuente AM, Yager RR (2015) An overview of fuzzy research with bibliometric indicators. Appl Soft Comput 27:420–433
Opricovic S (1998) Multicriteria optimization of civil engineering systems. Faculty of Civil Engineering, Belgrade
Pamučar D, Ćirović G (2015) The selection of transport and handling resources in logistics centers using multi-attributive border approximation area comparison (MABAC). Expert Syst Appl 42:3016–3028
Pamučar D, Mihajlović M, Obradović R, Atanasković P (2017) Novel approach to group multi-criteria decision making based on interval rough numbers: hybrid DEMATEL-ANP-MAIRCA model. Expert Syst Appl 88:58–80
Pamučar D, Petrović I, Ćirović G (2018a) Modification of the Best-Worst and MABAC methods: a novel approach based on interval-valued fuzzy-rough numbers. Expert Syst Appl 91:89–106
Pamučar D, Stević Ž, Zavadskas EK (2018b) Integration of interval rough AHP and interval rough MABAC methods for evaluating university web pages. Appl Soft Comput 67:141–163
Qin J, Liu X (2013) Study on interval intuitionistic fuzzy multi-attribute group decision making method based on Choquet integral. Proc Comput Sci 17:465–472
Qin J, Liu X, Pedrycz W (2016) Multi-attribute group decision making based on Choquet integral under interval-valued intuitionistic fuzzy environment. Int J Comput Intell Syst 9:133–152
Qu G, Qu W, Zhang Z, Wang J (2017) Choquet integral correlation coefficient of intuitionistic fuzzy sets and its applications. J Intell Fuzzy Syst 33:543–553
Rezaei J (2015) Best-worst multi-criteria decision-making method. Omega 53:49–57
Rezaei J, Wang J, Tavasszy L (2015) Linking supplier development to supplier segmentation using Best Worst Method. Expert Syst Appl 42:9152–9164
Sliwa J (2016) Reuse of data from smart medical devices for quality control and evidence-based medicine. In: Dobre C, Xhafa F (eds) Pervasive Computing. Elsevier, Amsterdam, pp 255–297. https://doi.org/10.1016/B978-0-12-803663-1.00009-7
Stojić G, Stević Ž, Antuchevičienė J et al (2018) A novel rough WASPAS approach for supplier selection in a company manufacturing PVC carpentry products. Information 9:121
Stoppa M, Chiolerio A (2014) Wearable electronics and smart textiles: a critical review. Sensors 14:11957–11992
Sugeno M (1974) Theory of fuzzy integral and its application (Doctoral dissertation). Tokyo Institute of Technology, Tokyo
Takahagi E (2000) On Identification methods of λ-fuzzy measures using weights and λ. Jpn J Fuzzy Sets Syst 12:665–676
Tan C (2011) A multi-criteria interval-valued intuitionistic fuzzy group decision making with Choquet integral-based TOPSIS. Expert Syst Appl 38:3023–3033
Tan C, Chen X (2010) Induced intuitionistic fuzzy Choquet integral operator for multicriteria decision making. Expert Syst Appl 37:149–157
Tan C, Chen X (2011) Induced intuitionistic fuzzy Choquet integral operator for multicriteria decision making. Int J Intell Syst 26:659–686
Tuzkaya G (2013) An intuitionistic fuzzy Choquet integral operator based methodology for environmental criteria integrated supplier evaluation process. Int J Environ Sci Technol 10:423–432
Vashist S, Schneider E, Luong J (2014) Commercial smartphone-based devices and smart applications for personalized healthcare monitoring and management. Diagnostics 4:104–128
Walsh JA, Topol EJ, Steinhubl SR (2014) Novel wireless devices for cardiac monitoring. Circulation 130:573–581
Wang Q, Sun H (2018) Interval-valued intuitionistic fuzzy Einstein geometric Choquet integral operator and its application to multiattribute group decision-making. Math Probl Eng 2018:1–11
Wang J, Wu J, Wang J et al (2016) Multi-criteria decision-making methods based on the Hausdorff distance of hesitant fuzzy linguistic numbers. Soft Comput 20:1621–1633
Wei G, Lin R, Zhao X, Wang H (2014) An approach to multiple attribute decision making based on the induced Choquet integral with fuzzy number intuitionistic fuzzy information. J Bus Econ Manag 15:277–298
Wu J, Chen F, Nie C, Zhang Q (2013) Intuitionistic fuzzy-valued Choquet integral and its application in multicriteria decision making. Inf Sci 222:509–527
Xia M, Xu Z (2013) Group decision making based on intuitionistic multiplicative aggregation operators. Appl Math Model 37:5120–5133
Xu Z (2010) Choquet integrals of weighted intuitionistic fuzzy information. Inf Sci 180:726–736
Xu Z, Cai X (2012) Intuitionistic fuzzy information aggregation. Springer, Berlin, pp 1–102
Xu Z, Yager RR (2006) Some geometric aggregation operators based on intuitionistic fuzzy sets. Int J Gen Syst 35:417–433
Xu Y, Wang H, Merigó JM (2014) Intuitionistic fuzzy Einstein Choquet integral operators for multiple attribute decision making. Technol Econ Dev Econ 20:227–253
Yu L, Wang L, Bao Y (2018) Technical attributes ratings in fuzzy QFD by integrating interval-valued intuitionistic fuzzy sets and Choquet integral. Soft Comput 22:2015–2024
Zadeh LA (1965) Fuzzy sets. Inf Control 8:338–353
Zavadskas EK, Kaklauskas A, Sarka V (1994) The new method of multicriteria complex proportional assessment of projects. Technol Econ Dev Econ 1:131–139
Zavadskas EK, Turskis Z, Antucheviciene J (2012) Optimization of weighted aggregated sum product assessment. Electron Electr Eng 122:1–4
Acknowledgements
The authors kindly express their appreciation for the support of industrial experts. The authors would like to thank the editor and anonymous reviewers for their valuable comments and suggestions which improved the quality of the paper. This research has received financial support of Galatasaray University Research Fund (Projects Nos. 17.402.004 and 18.402.001).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Communicated by V. Loia.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Büyüközkan, G., Göçer, F. Smart medical device selection based on intuitionistic fuzzy Choquet integral. Soft Comput 23, 10085–10103 (2019). https://doi.org/10.1007/s00500-018-3563-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00500-018-3563-5