
Abstract
Compared to previous decade, impact of heat waves (HWs) on mortality in recent years needs to be discussed in Iran. We investigated temporal change in added impact of summer HWs on mortality in eight cities of Iran. The pooled length of HWs was compared between 2015–2022 and 2008–2014 using random and fixed-effects of meta-analysis regression model. The temporal change in impact of HWs was evaluated through interaction effect between crossbasis function of HW and year in a two-stage time varying model. In order to pool the reduced coefficients of each period, multivariate meta-regression model, including city-specific temperature and temperature range as heterogenicity factors, was used. In addition to relative risk (RR), attributable fraction (AF) of HW in the two periods was also estimated in each city. In the last years, the frequency of all HWs was higher and the weak HWs were significantly longer. The only significant RR was related to the lowest and low severe HWs which was observed in the second period. In terms of AF, compared to the strong HWs, all weak HWs caused a considerable excess mortality in all cities and second period. The subgroup analysis revealed that the significant impact in the second period was mainly related to females and elderlies. The increased risk and AF due to more frequent and longer HWs (weak HWs) in the last years highlights the need for mitigation strategies in the region. Because of uncertainty in the results of severe HWs, further elaborately investigation of the HWs is need.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The increase in global air temperature has resulted in a big concern for human health. Because of climate change and some sociodemographic changes such as ageing, it is necessary to understand the impact of extreme temperatures on human health. Heat-related excess mortality is also projected to increase in future because of the climate change (Allen and Sheridan 2018). The increase in mortality is one of the most important health effects of both long term and short term of heat and extreme temperatures (Basara et al. 2010; Campbell et al. 2018). The climate change seems to increase number and length of heat waves (HWs) in addition to extreme temperatures. For example, Kuglitsch et al. (2010) revealed that from the 1960s to 2006, the number as well as the length of HWs in the eastern Mediterranean region have increased by 6.2 (± 1.1) and 7.5 (± 1.3), respectively. Also, in the 1960s, the average temperature during days with heat wave across 50 cities in USA was 2 °F above the local threshold (85th percentile). While, in 2020s, the average temperature in the days with heat wave was 2.3 °F above the threshold (Agency 2022). Consequently, higher HW-related excess mortality might be seen because there are many evidences showing higher cause-specific mortality including cardiovascular, respiratory, and trauma during the days with HWs (Dadbakhsh et al. 2017; Venturini et al. 2022). Previous studies found that the HWs in August 2003 in Europe (Basara et al. 2010; Robine et al. 2008), July 1995 in Chicago (Whitman et al. 1997), and the summer of 2010 in Russia (Barriopedro et al. 2011) caused 70,000, 696, and 55,000 excess deaths, respectively. In addition, three HWs occurred in Brisbane, Australia, in January 2000, December 2001, and February 2004 resulted in 51,233 excess deaths during the entire study period (Tong et al. 2012). Therefore, given the increase in HWs as well as their adverse impact on human health, it is important to show the temporal change in HWs and their impact on human health in regions where there is no evidence. It is also important to assess the impact in different regions because the development of preventive plans such as heat-health warning systems is dependent on available evidence (Luan et al. 2017). Furthermore, these evidences help health policy makers knowing how much effort they need to tackle HW-related mortality. In addition, and even more importantly, the study of temporal change in impact of HW can bring evidence of adaptation or maladaptation to heat.
There is no unit and standard definition of HW. They are determined using four key aspects namely intensity, duration, frequency, and spatial extent (Raei et al. 2018). Totally, they describe a period of time (days) with unusual hot and dry or hot and wet condition which last for at least two or three days (McGregor et al. 2015). To define unusual hot days, relative (percentile) or absolute thresholds (a value of temperature (are usually used as the cut of point (Guo et al. 2017). Also, the impact of defined HW on human health is investigated through comparing the risk in days with HW relative to the risk in days with no HW which is called added effect of heat wave. Although the added impact of heat waves has been widely investigated, especially in developed countries (Serdeczny et al. 2017), there are few evidence on the temporal change in the impact, especially in the Middle East (Campbell et al. 2018). In this study, temporal change (2015–2022 vs 2008–2014) in added impact of HW on mortality was investigated in eight cities of Kurdistan, Iran.
Methods
Study area and data
This study was conducted in eight cities of Kurdistan which is located to the west of Iran with the land area of 29,600 km2. The geographic location of the regions has been provided in Fig. 1. The climate in the regions is variable from cold to semi-arid based on Köppen climate classification (Fatehi and Shahoei 2021). The area’s elevation is also variable from 710 m in the southwest and northwest to 3220 m in middle parts of the region. In addition, the long-term mean annual precipitation ranges from minimum of 260 mm in the east (Bijar) to maximum of 860 mm in the west (Marivan). The long-term mean annual temperature varies between 9.6 °C in the north (Saqez) and 13.5 °C in the southwest (Kamyaran). The weather data including daily mean temperature(°C), humidity (%), and wind speed (m/s) were obtained from national weather organization (Iran Meteorological Organization). The data are measured by one monitoring station in each city which have been placed based on international and national guidelines (Organization 2023) considering climate generalizability, stability, topographic standards, etc. The mortality data due to all causes (i.e., all ICD 10 codes) were collected by the health deputy of Kurdistan University of Medical Sciences. The mortality data were categorized to sex and age groups in order to perform subgroup analysis.

Location of the Kurdistan region, Iran, including eight cities
Heat wave definition
We detect the HWs occurred in hot season (June–September) during 2008–2022. So, the data were strict to the hot months. Mean temperature was used for definition of HWs because it has been mostly used for HW definition in literature (Chen et al. 2015; Gasparrini and Armstrong 2011; Guo et al. 2017; Son et al. 2012). It has also been more frequently used as predictor of mortality compared to maximum and minimum temperature (Ahmadi et al. 2015; Guo et al. 2011; Yu et al. 2012). The heat waves were defined based on either percentiles or duration. Due to lack of no standard definition of HW, different percentiles (threshold) and durations (length) were considered in definitions to address weak and strong HWs. To do so, the daily mean temperatures above 95th and 98th percentiles for at least 2, 3, and 4 days were considered as HW. Therefore, we had 6 definitions of HWs from lowest to the highest severity, namely HW1, HW2, HW3, HW4, HW5, and HW6 (Table 1). We used mean temperature for the definition because many studies have revealed that it is better predictor of mortality than maximum or minimum temperature (Guo et al. 2011; Hajat et al. 2006; Zhang et al. 2016).
Temporal change in HWs
In addition to frequency of HWs, their mean duration (days) was compared between 2015–2022 and 2008–2014 in each city. We split the time to the two half periods because we had 14-year data that would have probably confronted with under or over estimation, if we had selected entire period. The mean difference of HWs duration in each city as well as pooled mean difference in the entire region (i.e., weighted average of the differences among the cities) was estimated using meta-analysis in which both fixed- and random-effects model were used. The analysis was done by each HW definition.
HW-related mortality risk (first-stage analysis)
The HW-related mortality relative risk (i.e., risk of mortality in days with HW relative to the days with no HWs; added effect of HWs) was estimated using distributed lag non-linear model. The cumulative impact of HWs during 21 days was estimated using the model through crossbasis function in which exposure–response and lag-response dimensions were defined. Twenty-one days were used as the maximum lag in the model because harvesting effect is more likely to happen in few days after heat waves (Kouis et al. 2019; Toulemon and Barbieri 2008). In the model, HW was main exposure which was a categorical variable. Therefore, there was no need for non-linear function in exposure–response dimension. In the lag-response dimension, linear association was defined based on sensitivity analysis. The model was as follows:
where \({Y}_{t}\) is the number of all-cause mortality in each day t which follows Poisson distribution. However, because of over-dispersion, quasi-Poisson family was applied in the model. Cb (HW) is the crossbasis (Cb) function of heat wave (HW) derived from DLNM (distributed lag non-linear model) which is composed of two dimensional associations: one in lag dimension and the second one in exposure dimension. HW is a dummy variable (i.e., 0 = no HW, 1 = HW). Thus, the relative risk (RR) was estimated through risk estimation in days with heat waves relative to not heat wave days (i.e., added effect).
Natural cubic B-spline function (Ns) with 4 degrees of freedom (df) was applied on day of the year (\({Day}_{y})\) to address seasonal variation in mortality (i.e., seasonality in mortality). The knots were placed at equal distance of the fitted function. Because the seasonal variation can potentially be different among years, the interaction effect between the non-linear function and year was therefore included in the model. Long trend was also addressed using the same spline function of time (Date) with equally distanced knots and 1 degree of freedom per 5 years. In the model, we adjusted for impact of humidity, wind speed, days of week (Dow), and public Holidays on mortality. Natural spline with df equal to 4 was fitted on humidity and wind speed. The days of week and public holidays were dummy variables which needed no non-linear function. The weekend and non-holidays were reference category of the Dow and Holidays, respectively. We chose the functions as well as their parameters (df) using literature and quasi-Akaike Information Criterion (Q-AIC).
Temporal change in risk
Overall impact of heat wave during entire study period (2008–2022) was estimated by the model in Eq. 1. Temporal change in impact of HWs was evaluated by comparison of HW-related mortality risk between 2008–2014 and 2015–2022. To do so, interaction effect between crossbasis function of HW and year was included to the model in Eq. 1. Therefore, a time-varying distributed lag non-linear model was developed as follows:
The model is composed of interaction term as well as main term named crossbasis (Cb) function of heat wave (HW). Because there is a variable named Date (i.e., time: days) in the model, there was no need for main term of year (Gasparrini et al. 2015). The time periods 2008–2014 and 2015–2022 were centered around 2011 and 2018, respectively, to ease interpretation of the interaction effect. Similar to Eq. 1, seasonality in each year and entire periods were taken into account for using interaction term between natural cubic B-spline function (Ns) of days of year (\({Day}_{y}\)) and year in the model which relaxes the hypothesis of a constant seasonal trend. Also, similar to Eq. 1, days of week (DOW) and public holidays were dummy variables.
In stage 1, two coefficients were estimated by the Cb function: one for exposure–response dimension and one for lag-response dimension. The coefficients were then decreased to one dimension to estimate overall cumulative exposure–response associations. This decrease in dimensions decreased the number of parameters which were pooled in the second-stage analysis while taking account for intricacy of Cb (Lee et al. 2018).
Second-stage analysis
In this stage, multivariate meta-regression model was utilized to pool the reduced coefficients of entire study periods, period 1 (2008–2014) and period 2 (2015–2022), by which some city-specific measures were adjusted for. Specifically, the heterogenicity among cities derived from different temperature distribution in the cities was controlled for through two proxy variables named mean temperature and temperature range in the cities. They were used as meta predictors in the meta-regression model. To assess statistical difference in the added effect of HWs between period 1 and period 2, Wald test was utilized in which no difference between the periods was the null hypothesis.
Attributable fraction/number
Besides relative risk (RR) of HWs, the attributable fraction (AF) of HW in the two periods was also estimated in each city that seems to be more helpful for health policy makers than RR because it gives information about the fraction of mortality in an exposed population that is attributable to the exposure (Mansournia and Altman 2018). It is primarily estimated by the RR (\(\frac{RR-1}{RR}\)) which is derived from the two-stage regression model. The details of AF estimation in DLNM (distributed lag non-linear model) can be found elsewhere (Gasparrini and Leone 2014). Totally, the AF is estimated in each day with HW. The overall AF (AF of all days with HW) is also estimated through summation of the AF for each day with HW. In order to facilitate the interpretation, attributable number (AN), in addition to AF, was estimated through multiplication of AF by number of deaths in each day with HW. The uncertainty (i.e., empirical confidence interval) of AF was estimated by Monte Carlo simulation.
Sensitivity analysis
We tested different functions and parameters for lag dimension of main exposure and covariates. They were selected based on the lowest Q-AIC. In addition, we accounted for the seasonality as well as trend by different df per year. The interaction effect was also assessed using time stratification method.
Results
The overall weather and mortality status in the two periods have been provided in Table 2. Totally, in the first period, daily mean air temperature and total mortality across all the cities were 13.43 °C and 2.38 deaths per day, respectively. In the second period, they were 13.25 °C and 2.68 deaths, respectively.
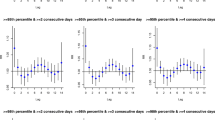
The feature of weak HWs (defined based on the 95th percentile) by two periods and cities has been presented in Fig. 2. Also, the feature of HW4, HW5, and HW6 has been provided in Figure S1. As seen in Fig. 2, except for Kamyaran, the number of heat waves increased in all cities in the second period; in Baneh, Bijar, Divandarreh, Marivan, Qorveh, Sanandaj, and Saqez, the number increased as 15, 14, 11, 11, 12, 2, and 5 days for the weakest HW, for example. The HWs’ duration (days) in the second period in most of the cities increased, as well. For example, for the weakest HW, it was on averaged increased as 1.59, 1.40, 0.04, 0.67, 1.51, 1.18, and 1.38 days in Bijar, Divandarreh, Marivan, Qorveh, Sanandaj, and Saqez, respectively. The mean difference (MD) of HW’s duration between two periods in each city as well as pooled MD has been shown in the figure. As seen, the pooled MD for HW1 (0.87 days) and HW2 (1.18 days) was significantly higher than zero, showing higher overall HW’s duration in the second period for the definitions. Based on other definitions (HW3 in Fig. 2 and HW4, HW5, HW6 in Figure S1) and based on both random- and fixed-effects models, there was no significant difference in pooled mean duration of HWs between the two periods. However, in the second period, the pooled mean duration was non-significantly higher (Fig. 3b).

Meta-analysis of mean difference (MD) of heat wave’s duration (days) between 2008–2014 and 2015–2022 by three definitions of HW; HW1, HW2, and HW3 represent the HW definition based on the 95th percentile and 2, 3, and 3 consequent days, respectively. The solid and dashed vertical lines represent the reference and observed mean difference, respectively. MD is mean difference between the two periods, and it was reported based on both random- and fixed-effects models. The weight of each city has been provided on the left side, and the heterogenicity indices (I2 and τ2) between the cities as well as definitions have been provided in the bottom sides

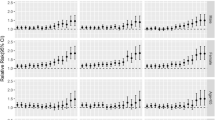
Heat wave properties and their impact on mortality over 2008–2014 and 2015–2022 by all heat wave definitions in the Kurdistan region; a: Number of heat waves, b: The pooled (weighted average) duration (days) of heat waves across all cities, c: Pooled relative risk of mortality across all cities associated to each heat wave definition
Figure 3 panel a shows the overall number of HWs (i.e., number of HWs in all cities based on different definition) in the two periods. It was evident that the overall number was higher in the second period based on all definitions. Panel b in the figure summarizes the pooled duration in each period, separately (single pooled mean in each period). As mentioned, in the second period, the pooled duration was higher, though the difference was significant for HW1 and HW2, only. The pooled relative risk (RR) of mortality due to HW by different definitions and two periods has been presented in Fig. 3 panel c. Based on the 95th percentile, there was small difference in RR between the periods. Based on the 98th percentile, the impact of HWs was higher in the first period; though, they were not significant neither in the first nor second period. The only significant impact was observed for HW1 and HW2 in the second period. The subgroup analysis revealed that the statistically significant impacts in the second period were mainly related to females and elderlies. For example, the impact (i.e., the relative risk) of the weakest HW on female and elderlies was 1.6 (1.16, 2.21) and 1.48 (1.16,1.87), respectively (Table 3). Table 3 shows that there was no significant impact of HW on male and young people neither in the first nor second period.
Table 4 represents fraction and number of deaths that are attributable to HWs based on the 95th percentile. Also, Table S1 shows the fraction and number of deaths that are attributable to HW4, HW5, and HW6 (i.e., based on the 98th percentile). As seen in Table 4, it was second period in which the HWs caused positive excess mortality in all cities while they were protective in the first period (negative excess mortality). However, the negative or positive excess mortality was not significant based on 95% confidence interval. The same pattern was observed for the HWs defined using the 98th percentile (Table S1). The age and sex group death number attributed to HW in each city has been provided in Table S2 and Table S3 by different definitions of HWs. Elderlies, especially those who lived in Sanandaj, were the most people who were vulnerable to HWs.
Discussion
In this study, temporal change in HWs as well as their impact on mortality were investigated. We found that the number of HWs in 2015–2022 was more than 2008–2014. In addition, the results of meta-analysis revealed that the weak HWs defined based on 95th percentile significantly lasted longer in the second period (the mean difference was 0.87, 1.18, and 0.74 days for HW1, HW2, and HW3, respectively). That we confronted with more dangerous HWs and warmer summers in recent years in Kurdistan might be mainly explained by the climate change. Also, due to recent increasing air pollution in the region which is probably derived from the Arabic dust phenomenon entering to the region through the deserts of neighboring countries in the West of Iran (Ahmadi et al. 2015) might potentially be the second reason for the result. In addition, the increase in number of industries and energy sources as well as number of nonstandard vehicles and accordingly high level of pollution in the region might be other reasons for the severe HWs in the last years. Indeed, nonstandard motor vehicles and other traffic-related sources of air pollution play an important role in the increase of poor air quality in Iran. For instance, more than 90% of the CO gas is produced by motor vehicles in Tehran (Saeb et al. 2012). This finding probably highlights confronting with more severe HWs, if no mitigation strategy is implemented.
An important finding of this study was significantly higher risk of total mortality in the second period based on the weakest (RR 1.29; CI 95% 1.7–1.59) and weak HWs (RR 1.25; CI 95% 1.04–1.51). There was no significant impact of stronger HWs neither in the first nor second period. In the second period, the stronger HWs had even caused lower risk of mortality which is in accord with previous studies. For example, a study conducted in Korea and Japan found that the number of heat waves increased in the last years compared to the 2000s in the countries (in Japan, North, 503 days in 2010s vs 247 days in 2000s and 97.8 days vs 64.8 days in the same decades in Korea); though, they found a temporal decreases in the risk of mortality due to HWs for all intensities (definitions) of HWs (Lee et al. 2018). A multi-country study also revealed that, except in Australia, Ireland, and the UK, the heat-related mortality was reduced in all countries (Vicedo-Cabrera et al. 2018). In Spain, Díaz et al. (2018) showed that there was a sharp reduction in heat-related mortality over the past 10 years (RR 1.14; CI 95% 1.09–1.19 in the first period vs RR 1.01; CI 95% 1.00–1.01 in the third period). As the authors mentioned, the lower risk due to severe HWs in the mentioned studies probably shows that there has been steeper decrease in vulnerability to severe HW compared to the observed severe HWs, which shows scope for adaptation to additional warming summers due to climate change. Indeed, because of preventive strategies in the countries (e.g., heat-health warning system)(Kovats and Kristie 2006), it is expected to see the faster reduction of heat-related mortality. In our study, the risk due to severe HWs was lower in the last years (second period), though the severity (duration) of the HWs was not significantly higher in the period (Figure S1). In other words, the decrease in severe HW-related risk in the second period was probably related to less severe HWs in the period. More specifically, as mentioned above, previous evidence revealed that the severity of HWs increased in recent years in many countries while the risk of heat-related mortality decreased (Boeckmann and Rohn 2014; Kinney 2018; Sheridan and Allen 2018). This might be due to high prevalence of air conditioning, for example (Kinney 2018). So, given previous evidence, it is apparent in our study that the decrease in risk was related to less severe HWs in the last years. Accordingly, the steeper decrease in vulnerability to severe HW was less likely to occur in the region, and there needs more attention to properly determine risk factors and adaptation strategies, for example, either at individual and population levels to decrease the HW-related mortality (Vicedo-Cabrera et al. 2018). This hypothesis is supported by the significant impact of weaker HWs in the second period. Indeed, all HWs based on all definition had adverse impact on mortality in some cases, though the weaker ones with higher risk increased in the second period which means the need for the preventive strategies.
Besides the risk, the AF of HW1, HW2, and HW3 in the second period was significantly high compared to first period; the number of deaths attributed to the HWs was variable between a minimum of 21 deaths in Divandarreh and a maximum of 175 in Sanandaj based on HW3 and HW1, respectively. In the first period, we even observed protective AFs. The mortality attributed to severe HWs in the second period was not as the same as the weaker HWs, though the Afs were positive in the second period compared to first period. Again, this finding highlights that the severe HWs (HW4, HW5, and HW6) should be more carefully discussed in the next studies. In addition, there was uncertainty in the AFs either in the first or second period. It can probably be due to short periods compared with each other or the small size of the cities in this study.
In this study, given that the number of deaths in males was higher than females, even the small risk in this group made higher number of deaths related to some of the heat waves definitions in some cities. However, the higher and significant risk in the second period was mostly observed in females and elderlies. The change in demographic characteristics over time in terms of vulnerability factors might explain why we observed the significant impact of weak HWs on the subgroup in the last years (De’Donato et al. 2018). Similar results have been found by some studies. For example, Wan et al. (2022) showed that the elderly had the highest relative risk related to both cold and heat events, and females experienced higher heat effects than males. Physiological aspects such as lower sweating ability and menopausal effects like elevated body temperature and sweating might be related to the impact (Mehnert et al. 2002). In Iran, the increasing trend in the proportion of elderly is obvious (i.e., growth rate of 3.9% in 2007 vs 8.26% in 2012) (Afshar et al. 2016; Zeinalhajlou et al. 2015), suggesting a greater fraction of individuals at risk and a greater HW-related burden for public health. Furthermore, lack of high-quality air conditioners, physiological acclimatization of elderlies, and not using climate-related standards in housing (i.e., housing with low carbon features such as using solar panels and thermodynamic elements) are suspected as the reason of vulnerability of elderlies in the region. Also, because of Hijab rules, the Iranian females follow the dress code in public areas. Probably, it makes them more vulnerable to heat stress and might have contributed to the significant impact of HWs on the people in the second period because the black Hijab creates a barrier for heat exchange, especially in hot climates.
A previously mentioned, most of the previous studies conducted in different countries found a decrease in heat-related mortality (Bobb et al. 2014; Kim et al. 2019; Lee et al. 2018; Petkova et al. 2014). This decrease can probably be explained by adaptation or preventive strategies. For instance, Martínez-Solanas and Basagaña (2019) found that the impact of extreme heat on mortality was totally lower after implementation of the preventive plan in Spain. Bobb et al. (Bobb et al. 2014) showed that the temporal decrease in heat-related mortality risk could be due to the increasing use of central air conditioners over time. Air conditioners have been widely hypothesized as a main contributor of adaptation and reduction in the adverse effect of heat (Barnett 2007; Davis et al. 2003). However, due to lack of central air conditioners (i.e., public cooling centers) or a comprehensive adaptation strategy, it is hard to judge about the adaptation to the heat in the region under study. Also, this was a 14-year study, and it is not easy to see adaptation or maladaptation during the short time. Meanwhile, given our result, preventive interventions should be introduced in the region in order to minimize the impact of HWs on mortality of the subgroups.
Conclusion
Weak HW-related deaths and risk have substantially increased in the last years in Kurdistan. Number of deaths related to severe HWs were negligible during the years, though the uncertainty in results of severe HWs indicates the need for more elaborately investigation of the HWs in the region. The increased risk as well as AF of mortality related to weak HWs in the last years reveals that a population or individual-based mitigation strategies should be implemented in the region in future. In addition to the increased risk, the increased number and severity of HWs in the second period points out the need for more researches on climate change patterns in the region, which is in particular influenced by human activities, burning of fossil fuels, and urbanization in Iran.
Data availability
The data is not publicly available due to ethical concerns but are available from the corresponding author on reasonable request.
Code availability
The R codes are available under request from corresponding author.
References
Afshar PF, Asgari P, Shiri M, Bahramnezhad F (2016) A review of the Iran’s elderly status according to the census records. Galen Med J 5:1–6
Agency USEP (2022) Climate change indicators: heat waves. https://www.epa.gov/climate-indicators/climate-change-indicators-heat-waves. Accessed 24 April 2022 2022
Ahmadi H, Ahmadi T, Shahmoradi B, Mohammadi S, Kohzadi S (2015) The effect of climatic parameters on air pollution in Sanandaj. Iran J Adv Environ Health Res 3:49–61
Allen MJ, Sheridan SC (2018) Mortality risks during extreme temperature events (ETEs) using a distributed lag non-linear model. Int J Biometeorol 62:57–67
Barnett AG (2007) Temperature and cardiovascular deaths in the US elderly: changes over time. Epidemiology 18:369–372
Barriopedro D, Fischer EM, Luterbacher J, Trigo RM, García-Herrera R (2011) The hot summer of 2010: redrawing the temperature record map of Europe. Science 332:220–224
Basara J, Basara H, Illston B, Crawford K (2010) The impact of the urban heat island during an intense heat wave in Oklahoma City. Adv Meteor 2010:230365
Bobb JF, Peng RD, Bell ML, Dominici F (2014) Heat-related mortality and adaptation to heat in the United States. Environ Health Perspect 122:811–816
Boeckmann M, Rohn I (2014) Is planned adaptation to heat reducing heat-related mortality and illness? A systematic review. BMC Public Health 14:1–13
Campbell S, Remenyi TA, White CJ, Johnston FH (2018) Heatwave and health impact research: a global review. Health Place 53:210–218
Chen K, Bi J, Chen J, Chen X, Huang L, Zhou L (2015) Influence of heat wave definitions to the added effect of heat waves on daily mortality in Nanjing, China. Sci Total Environ 506:18–25
Dadbakhsh M, Khanjani N, Bahrampour A, Haghighi PS (2017) Death from respiratory diseases and temperature in Shiraz, Iran (2006–2011). Int J biometeorol 61:239–246
Davis RE, Knappenberger PC, Novicoff WM, Michaels PJ (2003) Decadal changes in summer mortality in US cities. Int J Biometeorol 47:166–175
De’Donato F, Scortichini M, De Sario M, De Martino A, Michelozzi P (2018) Temporal variation in the effect of heat and the role of the Italian heat prevention plan. Public Health 161:154–162
Díaz J, Carmona R, Mirón I, Luna M, Linares C (2018) Time trend in the impact of heat waves on daily mortality in Spain for a period of over thirty years (1983–2013). Environ Int 116:10–17
Fatehi Z, Shahoei SV (2021) Predicting the impact of climate change on temperature in Sanandaj City Environment and Water. Engineering 7:170–182
Gasparrini A, Armstrong B (2011) The impact of heat waves on mortality. Epidemiology (Cambridge, Mass) 22:68
Gasparrini A, Leone M (2014) Attributable risk from distributed lag models. BMC Med Res Methodol 14:1–8
Gasparrini A et al (2015) Temporal variation in heat–mortality associations: a multicountry study. Environ Health Perspect 123:1200–1207
Guo Y, Barnett AG, Pan X, Yu W, Tong S (2011) The impact of temperature on mortality in Tianjin, China: a case-crossover design with a distributed lag nonlinear model. Environ Health Perspect 119:1719–1725
Guo Y et al (2017) Heat wave and mortality: a multicountry, multicommunity study. Environ Health Perspect 125:087006
Hajat S, Armstrong B, Baccini M, Biggeri A, Bisanti L, Russo A, Paldy A, Menne B, Kosatsky T (2006) Impact of High Temperatures on Mortality. Epidemiology. 17(6):632–8
Kim H, Kim H, Byun G, Choi Y, Song H, Lee J-T (2019) Difference in temporal variation of temperature-related mortality risk in seven major South Korean cities spanning 1998–2013. Sci Total Environ 656:986–996
Kinney PL (2018) Temporal trends in heat-related mortality: implications for future projections. Atmosphere 9:409
Kouis P, Kakkoura M, Ziogas K, Paschalidou AΚ, Papatheodorou SI (2019) The effect of ambient air temperature on cardiovascular and respiratory mortality in Thessaloniki, Greece. Sci Total Environ 647:1351–1358
Kovats RS, Kristie LE (2006) Heatwaves and public health in Europe. Eur J Pub Health 16:592–599
Kuglitsch FG, Toreti A, Xoplaki E, Della-Marta PM, Zerefos CS, Türkeş M, Luterbacher J (2010) Heat wave changes in the eastern Mediterranean since 1960. Geophysical Research Letters 37(4):L04802
Lee W, Choi HM, Lee JY, Kim DH, Honda Y, Kim H (2018) Temporal changes in mortality impacts of heat wave and cold spell in Korea and Japan. Environ Int 116:136–146
Luan G, Yin P, Li T, Wang L, Zhou M (2017) The years of life lost on cardiovascular disease attributable to ambient temperature in China. Sci Rep 7:13531
Mansournia MA, Altman DG (2018) Population attributable fraction. BMJ (Clinical research ed.) 22(360)
Martínez-Solanas È, Basagaña X (2019) Temporal changes in temperature-related mortality in Spain and effect of the implementation of a Heat Health Prevention Plan. Environ Res 169:102–113
McGregor G, Bessemoulin P, Ebi K, Menne B (2015) Heat waves and health: guidance on 7 warning system development 8. World meteorological organization 14:15
Mehnert P, Bröde P, Griefahn B (2002) Gender-related difference in sweat loss and its impact on exposure limits to heat stress. Int J Ind Ergon 29:343–351
Organization SW (2023) Standards for the construction of various meteorological stations. http://www.semnanweather.ir/index.php. Accessed August 24 2023
Petkova EP, Gasparrini A, Kinney PL (2014) Heat and mortality in New York City since the beginning of the 20th century. Epidemiology (Cambridge, Mass) 25:554
Raei E, Nikoo MR, AghaKouchak A, Mazdiyasni O, Sadegh M (2018) GHWR, a multi-method global heatwave and warm-spell record and toolbox. Sci Data 5:1–15
Robine J-M, Cheung SLK, Le Roy S, Van Oyen H, Griffiths C, Michel J-P, Herrmann FR (2008) Death toll exceeded 70,000 in Europe during the summer of 2003. C R Biol 331:171–178
Saeb K, Malekzadeh M, Kardar S (2012) Air pollution estimation from traffic flows in Tehran highways Current World. Environment 7:1
Serdeczny O et al (2017) Climate change impacts in sub-Saharan Africa: from physical changes to their social repercussions. Reg Environ Change 17:1585–1600
Sheridan SC, Allen MJ (2018) Temporal trends in human vulnerability to excessive heat. Environ Res lett 13:043001
Son J-Y, Lee J-T, Anderson GB, Bell ML (2012) The impact of heat waves on mortality in seven major cities in Korea. Environ Health Perspect 120:566–571
Tong S, Wang XY, Guo Y (2012) Assessing the short-term effects of heatwaves on mortality and morbidity in Brisbane, Australia: comparison of case-crossover and time series analyses. PloS one 7:e37500
Toulemon L, Barbieri M (2008) The mortality impact of the August 2003 heat wave in France: investigating the ‘harvesting’effect and other long-term consequences. Popul stud 62:39–53
Venturini T, De Pryck K, Ackland R (2022) Bridging in network organisations. The case of the Intergovernmental Panel on Climate Change (IPCC). Soc Netw 75:137–147
Vicedo-Cabrera AM et al (2018) A multi-country analysis on potential adaptive mechanisms to cold and heat in a changing climate. Environ Int 111:239–246
Wan K, Feng Z, Hajat S, Doherty RM (2022) Temperature-related mortality and associated vulnerabilities: evidence from Scotland using extended time-series datasets. Environ Health 21:99. https://doi.org/10.1186/s12940-022-00912-5
Whitman S, Good G, Donoghue ER, Benbow N, Shou W, Mou S (1997) Mortality in Chicago attributed to the July 1995 heat wave. Am J Public Health 87:1515–1518
Yu W, Mengersen K, Wang X, Ye X, Guo Y, Pan X, Tong S (2012) Daily average temperature and mortality among the elderly: a meta-analysis and systematic review of epidemiological evidence. Int J Biometeorol 56:569–581
Zeinalhajlou AA, Amini A, Tabrizi JS (2015) Consequences of population aging in Iran with emphasis on its increasing challenges on the health system (literature review). Depiction Health 6:54–64
Zhang Y, Li C, Feng R, Zhu Y, Wu K, Tan X, Ma L (2016) The short-term effect of ambient temperature on mortality in Wuhan, China: a time-series study using a distributed lag non-linear model. Int J Environ Res Public Health 13:722
Acknowledgements
We thank the National Department of Environment and Iran Meteorological Organization for providing us the data.
Funding
This work was supported by Deputy of Research and Technology at Kurdistan University of Medical Sciences with grant number of 1401.302.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This study was approved by ethic committee of Kurdistan University of Medical Sciences.
Consent to participate
The study did not involve human subjects and the data with no personal identity was obtained from health deputy.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Rezaee, R., Fathi, S., Maleki, A. et al. Summer heat waves and their mortality risk over a 14-year period in a western region of Iran. Int J Biometeorol 67, 2081–2091 (2023). https://doi.org/10.1007/s00484-023-02564-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-023-02564-7