
Abstract
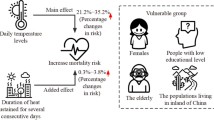
Few studies have examined the attributable fraction (AF) of temperature to mortality and Years of Life Lost (YLL), especially in developing countries. This study aims to explore the short-term effect of the cold and hot temperatures on the cause-specific YLL and mortality, discover the attributable contributions from the temperature variations, and identify the vulnerable populations in Weifang, China. Daily registered death information and meteorological data over the period 2010–2016 were obtained in Weifang, a northern Chinese city. Generalized additive Poisson and Gaussian regression models were used to assess the impacts of temperatures on both mortality and YLL, explore the AF of the temperature variations on mortality, after adjusting for other covariates. Both hot and cold temperatures have had significant negative impacts on cause-specific mortality counts and YLL, with heat presented an acute and short effect and the cold temperatures had delayed effects and lasted for several days. In terms of the attributable fraction calculations, the contributions from cold effects was higher than that of hot effects on non-accidental, cardiovascular, and respiratory deaths (YLL 10.88 vs. 1.23%, 19.58 vs. 1.71%, and 14.47 vs. 3.05%; mortality 13.97 vs. 1.65%, 19.20 vs. 1.59%, and 14.89 vs. 3.09%), respectively. The elderly and women and people with low education level were the most vulnerable. The findings will provide important scientific evidences and policy implications for developing adaptation strategies to reduce the adverse effect of cold and hot exposure in Weifang, in terms of resource allocation, healthcare workforce capacity building, and community health education, especially for the vulnerable groups.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Climate change has been regarded as one of the biggest threats on population health in the twenty-first century (Intergovernmental Panel on Climate Change. 2015). The increased frequency, intensity, and duration of extreme weather events such as heat waves and cold spells (Li et al. 2016a) have been recognized as important hazards on population health (Shaposhnikov et al. 2014; Yang et al. 2016). Up to now, many studies have found significant associations between ambient temperature and a series of health outcomes in the past years, using time series study design (Basu 2009; Gasparrini et al. 2015), including cardiovascular, renal diseases and mental health illnesses (Hanna et al. 2011), as well as work-related injuries in the past years (Xiang et al. 2018).
Among these studies, mortality and morbidity, the most common indicators in public health research, have been utilized to assess the associations between temperature and population health. However, as each death weighs equally in the calculation of mortality and morbidity, the influence of premature death is generally ignored in assessing the relationships between two variables in different age groups. For example, a person who died at 35 years old has been assumed to pose the same disease burden when compared to another who died at 75, although the disease burden should be different in different age groups. Years of life lost (YLL), including incorporating both premature death and people’s life expectancy, could be a more precise indicator of disease burden because it takes into account the weight of death at younger age (McKenna et al. 2005; Steenland and Armstrong 2006). To date, there have been very few studies assessing the relationship between climate variability and YLL, especially in developing countries including China.
In addition to quantitative assessing the relationship between climate variability and population health, using RR or OR, it is also crucial and even more important to understand the attributable contributions from the climate variation so more precise actions could be implemented. The Attributable Fraction (AF) refers to the proportion of incidents in the population that are attributable to a specific risk factor, that is, the proportion reduced in the absence of the exposure (Gasparrini and Leone 2014; McKenna et al. 2005). AF has been used by the World Health Organization (WHO) to calculate the disability-adjusted-life-years (DALYs) attributable to the major known risk factors for many diseases (Ezzati et al. 2003). However, there are few studies exploring temperature attributable fraction to health outcomes including China.
To provide robust evidence for the attributable risk of temperature-health associations in China, we conducted a time series study in a typical continental monsoon climate region of China to assess the short-term effect of the hot and cold temperature on the cause-specific YLL and mortality, to explore the attributable contributions from temperature variations and to identify the vulnerable populations for intervention.
Methods
Study area and population
The study is based in Weifang, a northern Chinese city covering an area of 15,895 km2 and with a population of about 9.27 million in 2015 (male vs. female, 1.02:1). Located in the center of Shandong Province (geographical coordinates, 35°41′-37°26′North, 108°10′-120°01′ East) (Fig. 1), it has sub-humid and warm climate, with continental monsoon weather and four distinct seasons. The annual average temperature is 12.3 °C, and the annual precipitation is about 650 mm.

The location of the study area in Shandong province, China
Data collection
Mortality data
The daily mortality data from 1 January 2010 to 31 December 2016 were collected from the Weifang Center for Disease Control and Prevention, an official health outcome data custodian for the city. The causes of death were coded according to the International Classification of Diseases, the tenth revision (ICD-10), as follows: total non-accidental deaths (ICD-10: A00-A99), cardiovascular disease (ICD-10: I00-I99), and respiratory disease (ICD-10: J00-J99). The data were stratified by sex, age (0–65 years, and over 65 years), and education level (low: ≤ 9 years, and high: > 9 years).
Meteorological data
Daily meteorological data over the same period were retrieved from the China Meteorological Data Sharing Service System (http://data.cma.cn/), including daily minimum temperature, average temperature, maximum temperature, relative humidity, and barometric pressure. To estimate the effects of temperature on different death causes, the average temperature was used as the exposure factor in this study as it indicates the average exposure throughout the 24-h period (Yang et al. 2015b).
YLL data
Chinese national life tables from 2000 to 2016 were obtained from the WHO website (http://www.who.int/gho/countries/chn/en). Life expectancy in 2015 was used to estimate the age-specific life expectancies for both sexes over the 2010–2016 period because of the little variations over this period (Table A.1). For the death of each individual, YLL was calculated by matching the sex and age in the life tables, and the daily total YLL were calculated as the YLL for the death of all causes on the same day. Like the mortality data, daily YLLs were also stratified with sex, age (0–65 years and over 65 years), and education level (low, ≤ 9 years school education, and high, > 9 years school education).
Statistical analysis
We used DLNM to assess the nonlinear temperature-YLL/mortality relationship according to the following equations (Gasparrini et al. 2015; Li et al. 2017b):
In these equations, YLL and Yt are the daily YLLs and death counts at calendar day t (t = 1, 2, 3 … 2557), respectively; α is the intercept; Tempt, l is a cross-basis matrix used to interpret the potentially lagged and nonlinear associations between temperature and mortality produced by DLNM. For the matrix, we combined the exposure-response function with a natural cubic spline which has three internal knots placed at the 10th, 75th, and 90th percentiles of temperature distribution, and also the lag-response function with a natural cubic spline with three internal knots placed at equally spaced values in the log scale, the maximum lag being 21 days. To control the potential confounders, we incorporated several covariates in the Generalized Additive Model (GAM): (1) we adopted a natural cubic spline with seven degree of freedom (df) per year to control the long-term trend and seasonality (Yang et al. 2016), (2) we used a smooth function of natural cubic spline with three df for relative humidity (Hum) and atmosphere pressure (Press) (Gasparrini et al. 2012), and (3) we used the day of week (Dow) and public holiday (Holiday) as indicator variables, as covered in the model.
Attributable risk measure by a forward perspective within the DLNM framework was used to calculate the attributable fraction (AF) of temperature for YLL and mortality. The forward AF was calculated according to the following Formula:
βx is the risk association with the exposure. The definition of the βx here is the effect value of association of temperature and YLL/mortality, compared to a reference value called minimum-mortality temperature (MMT). MMT, being the lowest point of the overall temperature-mortality curve, is referred to as the optimal temperature related to the lowest risk of non-accidental mortality. The total attributable number of deaths is the sum of the death contributions during the study period. Meanwhile, its ratio with the total number of deaths is the total attributable fraction (AF).
Attributable risks due to cold and heat were calculated as the sum of the subsets corresponding to days with temperatures lower or higher than MMT. These risks were further separated into death causes from moderate and extreme temperatures. The extreme cold and heat temperatures are defined as the temperatures below 2.5th and above 97.5th percentile and the moderate temperature as the temperature range between the cut-off points and MMT (Gasparrini et al. 2015; Li et al. 2018; Yang et al. 2016). Empirical confidence intervals (eCI) were calculated from Monte Carlo simulations assuming a multivariate normal distribution of the BLUPs of the reduced coefficients (McKenna et al. 2005). To identify the vulnerable populations to different temperature variables, we repeated the above analysis according to sex, age, and educational levels.
Sensitivity analysis
To check the stability of our main results, we have conducted the following sensitivity analyses: (1) changing the location of knots for temperature-mortality and using the maximum lag of 14–28 days; (2) varying the df (8–10) for time trend; (3) using df (2–6) for relative humidity and atmosphere pressure, respectively; and (4) testing the residual distribution and autocorrelation.
For all the statistical tests, effects of P < 0.05 (two-tailed) were considered statistically significant. All models were fitted with the R software (V.3.3.1, R Development Core Team 2016), with the “dlnm” package for DLNMs and the “mgcv” for GAMs.
Results
Description of daily death counts, YLL, and meteorological data
Descriptive results of death counts, YLL, and weather variables from 2010 to 2016 in Weifang are displayed in Table 1. The dataset includes 363,933 deaths and 5,047,038.8 YLL for non-accidental deaths over the 7-year study period. The average death counts of daily cases due to non-accidental, cardiovascular, and respiratory diseases were 142.3, 76.1, and 16.4, which is consistent with the average YLL of 1973.8, 908.8, and 174.3, respectively. For non-accidental mortality, males and the people with low education level showed higher death counts and YLL. Although the younger population (age ≤ 65) showed fewer deaths, they have much higher YLLs when compared with the older people.
As is shown in Fig. 2, YLL and death counts had a clear seasonal pattern, with a peak in both cold and hot seasons. Inconsistent with the seasonal fluctuation in YLL and death counts, the mean temperature represented a reverse distribution trend.

Line chart of death counts and daily years of life lost in Weifang, China, during 2010–2016. Plot a shows the time trend of death counts for non-accidental death, cardiovascular death, respiratory death, and mean temperature from top to down. Plot b shows the time trend of YLL for non-accidental death, cardiovascular death, and respiratory death from top to down
Association between temperature and YLL/mortality
All the plots showed acute effects of extreme heat exposure, with about 3-day lagged effects, while the lagged effects for cold exposure were longer up to 7 days (see Fig. 3).

3-D graphs of bi-dimensional exposure lag-response surfaces of the temperature on YLL (top) and death counts (bottom)
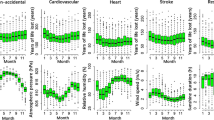
Figure 4 illustrates the overall cumulative association between temperature and YLL/mortality, explaining the effect cumulated over the whole lag period. The corresponding MMT and cut-off points defining the moderate and extreme temperature differs in different cause of death. The minimum YLL-related temperatures in the lag of the first 21 days were 25.9, 19.3, and 14.8 °C for non-accidental, cardiovascular, and respiratory mortality, respectively.

Overall cumulative exposure-response associations between temperature and YLL (top) and death counts (bottom) with mean temperature distributions
In general, the temperature-YLL/mortality curves are U shaped, with higher risks of mortality below and above the MMT. The histogram plots show that most of the temperatures were distributed near the MMT. Increasing trends are obvious for the cumulative effects when the temperature was below or above the cut-off points. Meanwhile, cold effect has a higher impact on mortality than that on YLL.
Estimation of AF for YLL and mortality under cold and heat effect
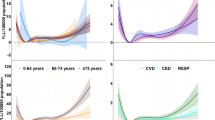
The attributable fractions of heat and cold effects to the YLL and mortality death with different causes have been presented in Table 2. Overall, coldness was responsible for almost up to 20% of YLLs and mortality for non-accidental death (10.88 and 13.97%), cardiovascular death (19.58 and 19.20%), and respiratory death (14.47 and 14.89%), respectively, while the AF from heat was limited, with the effects of 1.23 and 1.65%, 1.71 and 1.59%, and 3.05 and 3.09%, respectively.
The effects of heat on YLL and mortality are statistically significant in all the three causes of disease categories. Although the effect of cold showed statistical significance only in cardiovascular diseases, the AF increase was several times higher than that of heat. The total effect of the extreme temperature (cold effect and heat effect) was most evident in the mortality caused by cardiovascular disease than by non-accidental and respiratory causes.
Table 2 also reveals the modifying effects of gender, age, and education level on YLL and mortality. For cause-specific diseases, the AF of the effects of heat and cold on non-accidental death is statistically significant to the YLL and mortality of the females and the elderly. For older people, the negative impact from low temperature on the mortality is greater than that on the YLL; in contrast, the AF of YLL in respiratory diseases was lower than that on the mortality for the young people.
Stratified analyses according to the levels of education demonstrated that high temperature was related to greater increase in YLL in lower educated population. Detailed information on the components of AF in the moderate and extreme temperature of the subgroups is shown in Table A.2.
Sensitivity analysis
Sensitivity analyses were performed to examine the robustness of the model. The effect of low and high temperature on YLL and mortality were roughly similar when we changed the locations of knots for temperature-mortality relation and used 14–28 days of maximum lag days for temperature, 8–10 df for time trend and 4–6 df for relative humidity and air pressure, respectively (Table A.3), suggesting our models are robust.
Discussion
We examined the associations between temperature variations (both heat and cold) and three different health outcomes (non-accidental death, cardiovascular death, and respiratory death and relevant YLLs), explored the attributive contributions from temperature variables in this northern Chinese city with sub-humid and warm climate. To our best knowledge, this is one of the first such studies in China and the results will provide important policy implications to health and social service authorities for relevant actions.
Further to the RR calculation in other time series studies, the exploration of AF in this study provided one step further information about the exact contributions from the temperature variations to both mortality and YLLs in Weifang. The results provide comprehensive scientific evidences to relevant government organizations and local health network in their policy-making, resource allocation, and health workforce capacity building. In this study, we found that the hot temperature had significant influence on the YLL and mortality caused by non-accidental, cardiovascular, and respiratory conditions, while the effect of cold on the YLL and mortality was only significant in non-accidental death and cardiovascular death. Meanwhile, the AF of cold effects was higher than that of hot effects in non-accidental, cardiovascular, and respiratory death, with the contribution up to 20%. Cold days were much more than hot days in Weifang which may be the reason for higher effects of cold-attributable mortality/AF than that of hot effects (Zhang et al. 2019). So we further compared the effect between extremely hot days and extremely cold days that the numbers of days were almost same. The results in Table A.2 also showed that the extreme cold effects were stronger than extreme hot effects. Like other regions (Gasparrini et al. 2017), cold weather should be as an important public health threat in Weifang.
To develop a better early temperature-response plan, it is important to understand the lagged effects. Our results demonstrated that for YLL and mortality, the high temperature had an acute effect while the low temperature had a delayed effect. Hence, timely preventative measures are important to prevent the risk from extremely high temperature, and lasting protections after the cold days are needed to reduce the harmful effects especially for the vulnerable populations.
The effects of temperatures on YLL/mortality also differ in different sex, age, and educational levels. In this study, we found that the ambient temperature has strong impact on people with cardiovascular diseases, especially the low temperature in Weifang. This is in line with some European studies which had higher cardiovascular mortality in the cold spell (Kysely et al. 2009) and other similar studies in China and Australia (Huang et al. 2012a, Yang et al. 2015a; Zhang et al. 2018b). The significant increase of cardiovascular mortality and YLL could be explained by the biological pathways under the direct and indirect influence of the ambient temperature, including the changes of hemodynamic effects, hydration, the sympathetic and renin-angiotensin system, and the inflammatory mechanism (Giorgini et al. 2017). Low temperature could increase the catecholamine level, which causes vasoconstriction, tachycardia, and rising blood pressure. Exposure to heat can lead to the increase in vasodilation and perspiration to reduce the core temperature in human body, and therefore may change heart rate, blood pressure, blood viscosity, electrolyte, and acid base balance. These changes may have a vital role in exacerbating risks of cardiovascular diseases (Hajat et al. 2007; Liu et al. 2015; Madaniyazi et al. 2016; Yang et al. 2015a).
Moreover, respiratory mortality was significantly influenced by the effects of temperatures. The result of temperature-related respiratory mortality in a national investigation covering 107 US communities showed that a 4.64 and 1.60% increase in risk, compared with the reference temperature for cold and hot effects, respectively (Ma et al. 2014). A national research in China found that 0.98% of increase in the mortality of the population could contribute to 1 °C of increase in the temperature variation for respiratory death (Yang et al. 2018). However, we did not find a positive relationship between low temperature and respiratory mortality in our study. We have also found that the ranges of temperature other than the optimal temperature range have negative influence on people’s respiratory mortality; and the low temperature especially the moderately low temperature accounts for most of the AF. Yang et al. (2015a) found that the cold weather is one of the main causes of death for the population in subtropical regions. As the city of Weifang belongs to the relative cold region, the residents are likely to have adapted to the mildly cold weather and developed proper measures to cope with such weather in a long run. For the extreme cold temperatures, the higher AF for respiratory disease could be explained by the following reasons. On the one hand, when the peripheral temperature suddenly drops, people are likely to reduce outdoor activities or use the air conditioner, which might influence air quality inside and further have impacts on people’s respiratory health. On the other hand, the human body will activate a range of regulation and adaptation mechanisms in extreme temperature (Li et al. 2016b; Mourtzoukou and Falagas 2007). As a result, people with adaptation problems will trigger the potential respiratory diseases.
In line with previous epidemiology studies, our study found more severe negative health impacts from extreme temperatures on the elderly when compared to the younger age groups (Chen et al. 2016; Donaldson et al. 2003; Phung et al. 2016). For the causes other than respiratory diseases, the AF value of YLL in people under age 65 is higher than that of mortality. Although the AF value of mortality among the elderly was about three times higher than that of the younger population, the AF value of YLL of the two populations were very similar, which was consistent with a study regarding PM10-YLL relationship in Nanjing (Chen et al. 2018). This could be because the YLL included not only the death counts, but also the premature death indicating the preventable years of life lost (Li et al. 2017a; Zhu et al. 2017). Taking the YLL into consideration in public health policy-making should be more beneficial in resource distribution in public health and medical services. Further epidemiological research should use YLL as an indispensable indicator to examine the burden of disease due to climate factors.
Prior studies have found that gender might be an effect modifier when evaluating temperature-YLL/mortality relationship (Huang et al. 2013; Liang et al. 2018; Yang et al. 2015a). Females in Brisbane and England were identified as vulnerable groups to the impact of both high and low temperature on YLLs (Huang et al. 2012b; Zhang et al. 2018a), which is consistent with our study. A study conducted in Ningbo and 14 other Chinese cities had an opposite conclusion, suggesting that males were the vulnerable population. More studies in different geographic locations with different climatic characteristics are needed in the future.
The study results from Hubei and England suggested that overall socioeconomic status (SES) may also modify the association between ambient temperature and YLL/mortality (Zhang et al. 2018a; Zhang et al. 2018b). Our results indicate that the high temperatures have more impact on people with lower education level, a surrogate of SES, which was in line with the study conducted on 11 cities of the eastern USA (Curriero et al. 2002). People with lower education level might be more sensitive to high temperature, because of poor nutritional support, bad living conditions, limited medical service, short of preventive knowledge, and daily behavior patterns such as smoking and drinking (Chen et al. 2016; Chen et al. 2018; Yang et al. 2015a).
The limitations of our study should also be acknowledged. First, the study was not able to control the effects of air pollution because of data availability. Second, our research is only conducted in one city, and the results cannot be generalized to other regions. Third, like other epidemiological studies, we explored the effect of the exposure to different ambient temperatures, but this may lead to some unavoidable measurement errors. Beyond that, the omission of monitoring and collection of death data may cause some slight effects on the result of the research. Lastly, we noticed that children under 5 years old are more vulnerable to extreme temperatures (Scovronick et al. 2018). However, the data were not available for this analysis.
Conclusion
The effect of high temperature presented a more acute effect than that of cold temperature on YLL and mortality. A substantial amount of AF was resulted from moderate lower temperature. Hence, public health intervention should not only pay attention to the extreme temperature, but also focus on the moderate temperature. Lastly, demographic characteristics and socioeconomic status could influence the impacts of temperature, which may be an important reference to the decision-making and resource allocation to reduce attributable risk on temperature-related YLL/mortality.
Abbreviations
- AF:
-
Attributable fraction
- YLL:
-
Years of life lost
- RR:
-
Relative risk
- OR:
-
Odds ratio
- AN:
-
Attributable number
- DALYs:
-
Disability-adjusted-life-years
- CDC:
-
Center for Disease Control and Prevention
- ICD:
-
International Classification of Diseases
- WHO:
-
World Health Organization
- GAM:
-
Generalized Additive Model
- DLNM:
-
Distributed lag nonlinear model
- MMT:
-
Minimum-mortality temperature
- CI:
-
Confidence interval
- TV:
-
Temperature variability
References
Basu R (2009) High ambient temperature and mortality: a review of epidemiologic studies from 2001 to 2008. Environ Health 8:40
Chen K et al (2016) Urbanization level and vulnerability to heat-related mortality in Jiangsu Province, China. Environ Health Perspect 124:1863–1869
Chen R et al (2018) Association between ambient temperature and mortality risk and burden: time series study in 272 main Chinese cities. BMJ 363:k4306
Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA (2002) Temperature and mortality in 11 cities of the eastern United States American. J Epidemiol 155:80–87
Donaldson GC, Keatinge WR, Saunders RD (2003) Cardiovascular responses to heat stress and their adverse consequences in healthy and vulnerable human populations. Int J Hyperth 19:225–235
Ezzati M, Hoorn SV, Rodgers A, Lopez AD, Mathers CD, Murray CJ (2003) Estimates of global and regional potential health gains from reducing multiple major risk factors. Lancet 362:271–280
Gasparrini A, Leone M (2014) Attributable risk from distributed lag models. BMC Med Res Methodol 14:55
Gasparrini A, Armstrong B, Kenward MG (2012) Multivariate meta-analysis for non-linear and other multi-parameter associations. Stat Med 31:3821–3839
Gasparrini A, Guo Y, Hashizume M, Lavigne E, Zanobetti A, Schwartz J, Tobias A, Tong S, Rocklöv J, Forsberg B, Leone M, de Sario M, Bell ML, Guo YLL, Wu CF, Kan H, Yi SM, de Sousa Zanotti Stagliorio Coelho M, Saldiva PHN, Honda Y, Kim H, Armstrong B (2015) Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet 386:369–375
Gasparrini A, Guo Y, Sera F, Vicedo-Cabrera AM, Huber V, Tong S, de Sousa Zanotti Stagliorio Coelho M, Nascimento Saldiva PH, Lavigne E, Matus Correa P, Valdes Ortega N, Kan H, Osorio S, Kyselý J, Urban A, Jaakkola JJK, Ryti NRI, Pascal M, Goodman PG, Zeka A, Michelozzi P, Scortichini M, Hashizume M, Honda Y, Hurtado-Diaz M, Cesar Cruz J, Seposo X, Kim H, Tobias A, Iñiguez C, Forsberg B, Åström DO, Ragettli MS, Guo YL, Wu CF, Zanobetti A, Schwartz J, Bell ML, Dang TN, van DD, Heaviside C, Vardoulakis S, Hajat S, Haines A, Armstrong B (2017) Projections of temperature-related excess mortality under climate change scenarios. Lancet Planet Health 1:e360–e367
Giorgini P, Di Giosia P, Petrarca M, Lattanzio F, Stamerra CA, Ferri C (2017) Climate changes and human health: a review of the effect of environmental stressors on cardiovascular diseases across epidemiology and biological mechanisms. Curr Pharm Des 23:3247–3261
Hajat S, Kovats RS, Lachowycz K (2007) Heat-related and cold-related deaths in England and Wales: who is at risk? Occup Environ Med 64:93–100
Hanna EG, Kjellstrom T, Bennett C, Dear K (2011) Climate change and rising heat: population health implications for working people in Australia. Asia-Pac J Public He 23:14S–126S
Huang C, Barnett AG, Wang X, Tong S (2012a) Effects of extreme temperatures on years of life lost for cardiovascular deaths: a time series study in Brisbane, Australia. Circ Cardiovasc Qual Outcomes 5:609–614
Huang C, Barnett AG, Wang X, Tong S (2012b) The impact of temperature on years of life lost in Brisbane, Australia. Nat Clim Chang 2:265–270
Huang C, Barnett AG, Xu Z, Chu C, Wang X, Turner LR, Tong S (2013) Managing the health effects of temperature in response to climate change: challenges ahead. Environ Health Perspect 121:415–419
Intergovernmental Panel on Climate Change, (2015) Climate change 2014: mitigation of climate change. Cambridge University, England
Kysely J, Pokorna L, Kyncl J, Kriz B (2009) Excess cardiovascular mortality associated with cold spells in the Czech Republic. BMC Public Health 9:19
Li J, Xu X, Wang J, Zhao Y, Song XP, Liu ZD, Cao LN, Jiang BF, Liu QY (2016a) Analysis of a community-based intervention to reduce heat-related illness during heat waves in Licheng, China: a quasi-experimental study. Biomed Environ Sci 29:802–813
Li Q, Wang HJ, Song Y, Ma J, Song JY, Guo Y (2016b) Association between children's forced vital capacity and long-term exposure to local ambient temperature in China: a national cross-sectional survey. Sci Total Environ 557-558:880–887
Li G, Huang J, Xu G, Pan X, Qian X, Xu J, Zhao Y, Zhang T, Liu Q, Guo X, He T (2017a) Temporal variation in associations between temperature and years of life lost in a southern China city with typical subtropical climate. Sci Rep-UK 7:4650
Li J, Xu X, Yang J, Liu Z, Xu L, Gao J, Liu X, Wu H, Wang J, Yu J, Jiang B, Liu Q (2017b) Ambient high temperature and mortality in Jinan, China: a study of heat thresholds and vulnerable populations. Environ Res 156:657–664
Li J et al (2018) Impact of ambient temperature on chronic non-communicable disease mortality in Jinan, China during 2007-2013: an attributable risk study. J Shandong University (Health Sci) 56(8):76–87
Liang H, Qiu H, Tian L (2018) Short-term effects of fine particulate matter on acute myocardial infarction mortality and years of life lost: a time series study in Hong Kong. Sci Total Environ 615:558–563
Liu C, Yavar Z, Sun Q (2015) Cardiovascular response to thermoregulatory challenges. Am J Physiol Heart Circ Physiol 309:H1793–H1812
Ma W, Chen R, Kan H (2014) Temperature-related mortality in 17 large Chinese cities: how heat and cold affect mortality in China. Environ Res 134:127–133
Madaniyazi L, Zhou Y, Li S, Williams G, Jaakkola JJK, Liang X, Liu Y, Wu S, Guo Y (2016) Outdoor temperature, heart rate and blood pressure in Chinese adults: effect modification by individual characteristics. Sci Rep-UK 6:21003
McKenna MT, Michaud CM, Murray CJ, Marks JS (2005) Assessing the burden of disease in the United States using disability-adjusted life years. Am J Prev Med 28:415–423
Mourtzoukou EG, Falagas ME (2007) Exposure to cold and respiratory tract infections. Int J Tuberc Lung Dis 11:938–943
Phung D, Guo Y, Nguyen HT, Rutherford S, Baum S, Chu C (2016) High temperature and risk of hospitalizations, and effect modifying potential of socio-economic conditions: a multi-province study in the tropical Mekong Delta region. Environ Int 92-93:77–86
Scovronick N, Sera F, Acquaotta F, Garzena D, Fratianni S, Wright CY, Gasparrini A (2018) The association between ambient temperature and mortality in South Africa: a time-series analysis. Environ Res 161:229–235
Shaposhnikov D, Revich B, Gurfinkel Y, Naumova E (2014) The influence of meteorological and geomagnetic factors on acute myocardial infarction and brain stroke in Moscow, Russia. Int J Biometeorol 58:799–808
Steenland K, Armstrong B (2006) An overview of methods for calculating the burden of disease due to specific risk factors. Epidemiology 17:512–519
Xiang et al. (2018) Correlates of occupational heat-induced illness costs: case study of South Australia 2000 to 2014. J Occup Environ Med 60(9):e463–e469
Yang J, Ou CQ, Guo Y, Li L, Guo C, Chen PY, Lin HL, Liu QY (2015a) The burden of ambient temperature on years of life lost in Guangzhou, China. Sci Rep-UK 5:12250
Yang J, Yin P, Zhou M, Ou CQ, Guo Y, Gasparrini A, Liu Y, Yue Y, Gu S, Sang S, Luan G, Sun Q, Liu Q (2015b) Cardiovascular mortality risk attributable to ambient temperature in China. Heart 101:1966–1972
Yang J et al (2016) The burden of stroke mortality attributable to cold and hot ambient temperatures: Epidemiological evidence from China. Environ Int 92-93:232-238
Yang J, Zhou M, Li M, Liu X, Yin P, Sun Q, Wang J, Wu H, Wang B, Liu Q (2018) Vulnerability to the impact of temperature variability on mortality in 31 major Chinese cities. Environ Pollut 239:631–637
Zhang Y, Peng M, Wang L, Yu C (2018a) Association of diurnal temperature range with daily mortality in England and Wales: a nationwide time-series study. Sci Total Environ 619-620:291–300
Zhang Y, Yu C, Peng M, Zhang L (2018b) The burden of ambient temperature on years of life lost: a multi-community analysis in Hubei. China Sci Total Environ 621:1491–1498
Zhang Y, Xiang Q, Yu Y, Zhan Z, Hu K, Ding Z (2019) Socio-geographic disparity in cardiorespiratory mortality burden attributable to ambient temperature in the United States. Environ Sci Pollut Res Int 26(1):694–705
Zhu J, Zhang X, Zhang X, Dong M, Wu J, Dong Y, Chen R, Ding X, Huang C, Zhang Q, Zhou W (2017) The burden of ambient air pollution on years of life lost in Wuxi, China, 2012-2015: a time-series study using a distributed lag non-linear model. Environ Pollut 224:689–697
Acknowledgements
This study was supported by the Social Science Planning Research Project of Shandong Province (18CQXJ18), Medicine and Health of Shandong Province for Science and Technology Development Program (2017WS703, 2016WS0664), Science and Technology Project of Shandong Health Science and Technology Association, and State Key Laboratory of Infectious Disease Prevention and Control Program of China (2018SKLID306). The authors are grateful to the Weifang Center for Disease Control and Prevention sharing with us the information needed for this study.
Funding
This study was supported by the Science and Technology Development Program for Medicine and Health of Shandong Province (2017WS703, 2016WS0664), Social Science Planning Research Project of Shandong Province (18CQXJ18), and State Key Laboratory of Infectious Disease Prevention and Control Program of China (2018SKLID306).
Author information
Authors and Affiliations
Contributions
JL and XX conceived and designed the study; ZC, XH, NL, and XM collected the data; ZC, XH, CW, and QW performed the data analysis; JL and XX drafted the manuscript; QL and PB provided significant intellectual advice. PB helped revise the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Xin Xu, Zuosen Chen, and Xiyuan Huo are co-first authors
Highlights
• To our knowledge, the first few studies to explore the attributable fraction of ambient temperature on both mortality and YLL in China.
• Cold rather than heat contributed substantially to cause-specific YLLs and mortality.
• AF vulnerability on YLL and mortality to ambient temperature varied not only by classification of diseases, but also by demographic characteristics.
• Findings are important for public health decision-making and resource allocation due to extreme temperature in China.
Electronic supplementary material
ESM 1
(DOCX 39 kb).
Rights and permissions
About this article

Cite this article
Xu, X., Chen, Z., Huo, X. et al. The effects of temperature on human mortality in a Chinese city: burden of disease calculation, attributable risk exploration, and vulnerability identification. Int J Biometeorol 63, 1319–1329 (2019). https://doi.org/10.1007/s00484-019-01746-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-019-01746-6