
Abstract
The use of diuretics is extremely frequent in sick neonates, the more so in very premature newborn infants. The use of diuretics in patients whose kidney function is immature necessitates a thorough knowledge of renal developmental physiology and pathophysiology. This review presents the basic aspects of body fluid homeostasis in the neonate, discusses the development of kidney function, and describes the mechanisms involved in electrolyte and water reabsorption along the nephron. Diuretics are then classified according to the site of their action on sodium reabsorption. The use of diuretics in sodium-retaining states, in oliguric states, in electrolyte disorders, and in arterial hypertension, as well as in a few specific disorders, is presented. Common and specific adverse effects are discussed. Recommended dosages for the main diuretics used in the neonatal period are given. New developments in diuretic therapy are briefly mentioned.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diuretics are pharmacologic agents that promote the excretion of water and electrolytes. They represent one of the most common classes of drugs administered to sick neonates, for whom they are primarily used in the treatment of illnesses associated with inappropriate water and sodium retention, such as congestive heart failure, kidney disorders, and liver disease. The use of diuretics is extended to various clinical conditions not evidently related to salt retention (i.e., respiratory diseases, unwanted fluid excess or oliguric states, electrolyte disorders). According to a recent study, furosemide is one of the 20 medications most prescribed during the neonatal period, with an overall exposure rate of 6.9% in infants cared for in neonatal wards and up to 44.2% in preterm infants of gestational age less than 27 weeks [1]. It is evident that expectations for diuretic therapy by neonatologists caring for very low birth weight (VLBW) infants may exceed evidence of efficacy [2].
This article reviews the actions of the diuretic agents commonly used in neonates, the rationale for the use of diuretics in preterm and term infants, and the adverse effects of diuretic therapy.
Body fluid homeostasis in neonates
The kidney is the main organ responsible for maintaining the extracellular fluid (ECF) volume and osmolality within narrow limits. In neonates, the functional capacity of the kidney is clearly influenced by the infant’s gestational and postnatal ages. Thus, a precise knowledge of both the physiology of the fluid balance and the pathophysiology of the immature kidney provides an adequate basis for the rational prescription of diuretics in newborn infants.
Body fluid homeostasis
NaCl is the major osmotically active solute in the ECF and determines its volume. The overall balance between the intake and the renal excretion of Na+ regulates the ECF volume, and as a consequence the cardiac output and pressure. Pressure receptors within the vasculature and flow receptors within the kidney trigger a coordinated response for maintaining the “effective arterial circulating volume,” a term that describes the critical blood flow for an adequate organ perfusion.
Aldosterone is the main hormone regulating long-term changes in sodium excretion, though renal sodium handling is also modulated by other factors, such as changes in glomerular filtration rate (GFR) and various intrarenal hormones and paracrine factors. The plasma renin activity generated by the fetal kidney is elevated and is essential for the maintenance of blood pressure in the fetus. It slowly decreases after birth. While sodium is the main solute regulating ECF volume, the antidiuretic hormone (ADH, or vasopressin) plays a central role in the defense of the plasma osmolality.
The reabsorption of Na along the nephron
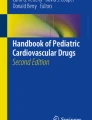
Up to 99% of the filtered sodium is reabsorbed by the kidney tubule. To achieve this, 65% is reabsorbed in the proximal tubule, 25% in the ascending limb of Henle’s loop, and ~ 10% in the distal tubule and collecting duct. The key sites of sodium transport along the nephron are shown in Fig. 1.

Sites of sodium reabsorption and diuretic site of action along the nephron. (1) sodium hydrogen exchanger (NHE); (2) sodium glucose cotransporter (SGLT2); (3) sodium potassium chloride cotransporter (furosemide receptor)(NKCC2); (4) sodium chloride cotransporter (thiazide receptor)(NCC); (5) proton ATPase and epithelial sodium channel (ENaC) (amiloride receptor). V2R = arginine vasopressin receptor. ADH = antidiuretic hormone
Throughout the nephron, the driving force for Na+ reabsorption is the Na+, K+- ATPase in the basolateral membrane of tubular epithelial cells. In the early portion of the proximal tubule, the luminal reabsorption of Na+ is primarily coupled to that of the filtered load of bicarbonate, with the help of the Na+/H+ exchanger (NHE). In the late proximal tubule, sodium is mostly reabsorbed with chloride. In the loop of Henle, the majority of the sodium is reabsorbed by the Na+, K+, 2Cl− cotransporter (NKCC). This is the transporter that is inhibited by furosemide and bumetanide. Sodium, but not water, is reabsorbed in the ascending limb, thus allowing the generation of a hyperosmolar medullary interstitium necessary for urinary concentration. In the distal convoluted tubule, sodium reabsorption primarily occurs with chloride, via the Na+Cl− cotransporter (NCC), which is inhibited by thiazides. The collecting duct has two types of cells. The principal cells reabsorb Na+ and water and secrete K+, under the control of aldosterone. Neighboring type A intercalated cells reabsorb K+ and secrete H+ in the tubular lumen, playing an important role in acid-base balance. They are also affected by aldosterone. The active sodium transport that occurs in the collecting duct is mediated by the amiloride-sensitive ENaC channel. The principal cells of the collecting duct also express the vasopressin-sensitive water channel aquaporin-2 (AQP2) which represents the chief target of the ADH for the regulation of water permeability. AQP2 is translocated from intracellular vesicles to the apical membrane of collecting duct cells after ADH stimulation. Under physiological conditions, urinary AQP-2 excretion is a marker of the kidney concentrating ability.
Body fluid homeostasis and kidney function after birth
The amount of total body water and its distribution between the body fluid compartments is very different in the fetus and in the neonate as compared to the adult. The transition from fetal to neonatal life is associated with major changes in water and sodium homeostasis. The ECF volume in the neonate is affected by antenatal factors, gestational age, birth weight, adaptation to extra-uterine environment, and postnatal age. The ECF amount per body weight is greater at lower gestational ages. A physiologic contraction of ECF volume occurs after birth, and, under normal conditions, a net water and sodium loss occur appropriately in the first week of life, especially in the most preterm infants. From a value of 60% of body weight in neonates of 24 weeks of gestational age, the ECF volume decreases to 44% of body weight near term. The ECF volume decreases to 30% in the infant and stabilizes at a value of 20% in the grown-up child. At birth GFR is low, both in term and preterm infants, and this limits the newborn infant’s ability to excrete a water and sodium load. After birth, renal blood flow (RBF) and GFR mature rapidly according to gestational and postnatal ages [3]. The abrupt increase of GFR largely contributes to contract the ECF volume and increases the filtered load of sodium and the diuresis. Postnatal variations in ECF volume and GFR are paralleled by maturational changes in tubular transport and marked changes in tubular sodium handling occur with and following birth (the reader is referred to [4, 5] for a more detailed description). These developmental changes are mostly dependent upon gestational age more than upon postnatal age, thus inducing a certain degree of glomerulotubular imbalance, especially in VLBW infants. Briefly, several factors are responsible for the reduced sodium renal handling: (i) the activity of the basolateral Na+, K+- ATPase presents with a rapid increase during the first 24 h of life, but is completely mature at 35 weeks of gestational age; (ii) the NHE activity in the proximal tubular increases immediately after birth, but this is not paralleled by corresponding mRNA abundance and protein activity; (iii) plasma aldosterone levels at birth increase significantly with gestational age but, despite levels higher than adults, preterm infants are less responsive to aldosterone; and (iv) there is a paucity of conducting ENaC channels in principal cells of the collecting duct.
Concerning the newborn’s ability to regulate urine concentration, noteworthy is the fact that the immature kidney can produce urine as diluted as 50 mOsm/kg H2O, after prolonged decrease of serum osmolality. Conversely, the ability to concentrate urine is deeply impaired by the limited concentration of urea in the medullary interstitium. Despite the huge increase of ADH in response to augmented serum osmolality or reduced effective arterial circulating volume, and even though urinary AQP2 excretion increases under these circumstances [6], the immature neonatal kidney can only concentrate urine up to 600 mOsm/kg H2O. This places neonates at risk of volume depletion. Furthermore, urinary water losses may also be augmented by other conditions in sick or preterm infants, such as caffeine or theophylline therapy, glycosuria, and, of course, diuretic therapy.
Classification of diuretics
All diuretics are natriuretic agents. Diuretics can variably modify electrolyte excretion. Diuretic drugs can be classified according to their site of action on Na+ transport along the nephron, as shown in Fig. 1.
From a clinical point of view, diuretics can be classified according to their mode of action (Table 1). Table 1 also describes the most commonly used diuretic agents in neonates.
Indications of diuretics
Diuretics are used in sodium-retaining states with or without the formation of edema, in oliguric kidney failure, in situations of electrolyte imbalances or arterial hypertension, and in nephrogenic diabetes insipidus. Diuretics can be used to test the integrity of distal tubular function (Table 1).
Sodium-retaining states
Sodium retention is the primary indication of diuretics. Salt and water retention may result either from primary excessive volume or pressure overload, or from a reduced effective circulating volume. This latter triggers a secondary hyperaldosteronism, with the result of restoring perfusion of the vital organs.
The most common sodium-retaining state in neonates is congestive heart failure (CHF). In CHF systemic and pulmonary congestion arises from the inability of the heart to pump as much blood as required for an adequate organ metabolism. The decrease of effective circulating volume is sensed by the kidney which retains sodium and water. A newborn infant with CHF carries the risk of rapid deterioration, and even if the chief treatment of CHF consists in restoring an adequate cardiac output, the use of diuretics can be life-saving in reducing pulmonary edema and congestion. The loop diuretic furosemide is the most used diuretic in neonates worldwide, and CHF is its main therapeutic indication [1, 11, 12]. Several studies provide strong evidence that, in case of volume overload after cardiac surgery and in critically ill patients, continuous intravenous furosemide is effective, well tolerated, and safe [13, 14]. In the postoperative management of hemodynamically stable infants following open heart surgery, intermittent infusion should be preferred [15]. Furosemide increases the peripheral venous capacitance and can thus be useful independently from its diuretic effect. In infants with severe CHF, the diuretic effect of furosemide is inversely related to serum aldosterone levels. The concomitant administration of a K+- sparing diuretic improves the response to loop diuretics [16], and oral spironolactone is often associated with furosemide in the mid-long-term treatment of neonatal CHF.
Few pharmacokinetic studies provide evidence that intermittent administration of bumetanide is effective and tolerated in volume overloaded, critically ill newborn infants, with no data available, to date, on its continuous infusion [17]. It is interesting to note that in neonates undergoing extra-corporeal membrane oxygenation (ECMO), substantial pharmacokinetic alterations in loop diuretics occur [18]. These alterations, along with the variable kidney function, make the dosing schedule for furosemide and bumetanide in newborn infants under ECMO very empirical (see dosage drug table here below).
Nephrotic and liver failure edemas are less frequent in neonatal life. In these conditions, sodium retention occurs in order to defend the circulating volume which can be very low, and the use of diuretics (loop diuretics, thiazides, and K+-sparing diuretics) requires a careful assessment of the infant intravascular volume. In severe forms of congenital nephrotic syndrome (CNS) generalized edema, urine protein concentration > 20 g/L, and serum albumin level < 10 g/L can be detected since the neonatal period [19]. Intravenous furosemide can be used to promote sodium and water excretion and should be given together with the expansion of the extracellular space with intravenous albumin [20]. In the management of edema associated with CNS, amiloride has been studied in conjunction with loop diuretics and has been shown to have an additive effect [21]. Broadly, refractory edema secondary to CHF, cirrhosis of the liver or nephrotic syndrome, represents a common indication for the use of K+-sparing diuretics. In all conditions associated with secondary hyperaldosteronism, spironolactone is the first-choice agent, provided kidney function is not impaired. Because they induce K+ retention, K+-sparing diuretics should not be used in patients with impaired kidney function or in those receiving potassium supplementation. They should also be avoided in patients prone to develop metabolic acidosis.
Oliguric states
There are no specific guidelines regarding the use of diuretics in newborn infants with acute kidney injury (AKI), and there is no evidence that this treatment can ameliorate kidney function or improve the outcome of infants with AKI. Among diuretics, the osmotic diuretic mannitol is presently not recommended in neonates with the indication of improving diuresis in oliguric states, due to several reported adverse effects (see paragraph 6). With a lack of consensus from human adult studies [22], and based on animal models of the immature kidney [23], there is no evidence that loop diuretics can prevent the evolution from prerenal to intrinsic kidney failure or that they can improve the outcome of patients with established kidney failure.
Nevertheless, in neonates with oliguric AKI, standard practice includes a trial with loop diuretic therapy (often furosemide) to improve diuresis and avoid fluid overload [24,25,26,27]. Moreover, in neonates undergoing cardiopulmonary bypass surgery, it has been proven that urine output response to furosemide administered intraoperatively predicts cardiac surgery-induced AKI development and other important morbidities [28].
Very few studies have reported results on the use of bumetanide in preterm or LBW infants, and they do not allow a definite conclusion on the usefulness of bumetanide in AKI [29,30,31].
Finally, since the late 80s, experimental studies have explored the role of adenosine in the immature kidney and in functional kidney insufficiency and the protective effects of theophylline, a xanthine derivative with strong adenosine antagonistic properties [32, 33]. They provided evidence of natriuretic and diuretic properties of theophylline when used in oliguric acute hypoxemic vasomotor nephropathy in rabbits [34]. In recent years, aminophylline and theophylline have been tested in several randomized controlled trials for their prophylactic and curative use in kidney impairment in critically ill neonates. Systematic reviews and meta-analyses conclude that prophylactic theophylline helps in prevention of AKI/severe kidney dysfunction in term neonates with severe birth asphyxia [35, 36]. Asphyxia is the most frequent cause of severe oligo-anuric kidney failure. Inhibition of intrarenal adenosine seems promising for improving kidney outcome of asphyxiated neonates undergoing therapeutic hypothermia and deserves further investigation [37].
Electrolyte disorders
Diuretics are used in clinical situations associated with electrolyte disorders.
In hyperkalemic states, loop diuretics and thiazides can increase potassium excretion; in hypercalcemia, loop diuretics can be used to increase calcium excretion; in hypercalciuric states, thiazides decrease the rate of calcium excretion. Increased bicarbonate excretion can be achieved by acetazolamide, and increased excretion of hydrogen ions can be stimulated by loop diuretics.
Arterial hypertension
Loop diuretics, thiazides, and aldosterone antagonists can be used in treatment of slow onset neonatal hypertension (NH), especially if arterial hypertension is a consequence of, or is aggravated by, sodium and water retention. This type of hypertension responds to diuretic-induced natriuresis. Furosemide and hydrochlorothiazide have modest effects on blood pressure, but they can be used in association with K+- sparing diuretics in NH related to bronchopulmonary dysplasia (BPD). Diuretics do not represent the first-line treatment for NH, and they should not be used as antihypertensive drugs in the treatment of malignant, fast onset crisis [38].
Specific indications
Acetazolamide, furosemide, and hydrochlorothiazide have been used in the past to test distal tubular acidification or distal sodium reabsorption defects in neonatal onset kidney tubulopathies [39]. In the newborn infant with congenital Bartter syndrome, amiloride (or triamterene) and spironolactone can be added for the treatment of hypokalemia as they will also improve the metabolic alkalosis [40]. Potassium-sparing diuretics should however be administered with caution because they carry the risk of inducing hypovolemia. Thiazides can be used to create mild hypovolemia which encourages salt and water uptake in the proximal tubule and thus improve polyuria in nephrogenic diabetes insipidus [41].
Dosages of diuretics in newborn infants
While not the object of this review, it is important to remember that the age-related establishment and maturation of RBF and GFR, and the kidney tubular secretory capacity, affect the delivery of diuretics to their sites of action and, as a consequence, condition the pharmacodynamics and neonatal response.
With the exception of furosemide, pharmacokinetic and pharmacodynamic of diuretics have been poorly studied in human newborn infants [17, 42,43,44]. Most of the available data on dosages of diuretics in neonates are derived from studies conducted in pediatric or adult patients, without logical or justified extrapolation [45].
Table 2 reports the dose of the diuretics most often used during the neonatal period according to pharmacokinetic and pharmacodynamic data or clinical pharmacology studies.
The use of diuretics in neonatal intensive care—where is the evidence?
Diuretic drugs, especially loop diuretics, are often used in the neonatal intensive care unit as off-label treatments for several clinical conditions. This occurs despite significant side effects and also despite that, to date, studies have not demonstrated a positive impact of diuretic therapy upon important clinical outcomes. These conditions are discussed below.
Diuretics for respiratory distress syndrome of the newborn infant
As it can produce an acute diuresis, furosemide may induce a transient improvement in pulmonary function. However, the most recent critical review of the literature [46] failed to support the routine administration of furosemide (or any diuretic) in preterm infants with RDS and concluded that elective administration of diuretics should be weighed against the risk of inducing cardiovascular complications. Recent results from the PROP (prematurity and respiratory outcomes program) cohort did not support the ability of diuretics to substantially improve the extremely premature infant’s respiratory status [47]. Diuretics cannot even be recommended for the treatment of transient tachypnea of the newborn at term [48].
Diuretics for preterm infants with evolving or established BPD
Diuretics are used as symptomatic therapy in the management of BPD. Loop diuretics increase re-absorption of the interstitial fluid and pulmonary vasodilation, decrease filtration of transpulmonary fluid, and systemic vasodilation [49]. So, enteral and aerosolized administration of furosemide have been studied, but Cochrane meta-analyses [50, 51] conclude that they are not recommended for routine management of the early or late phases of BPD. Noteworthy is however the recent observation demonstrating that more days on furosemide between postnatal day 7 and 36 weeks were associated with decreased risk of BPD and of combined outcome of BPD or death [52].
Acute and chronic administration of thiazides improve pulmonary mechanics. However, their positive effects should be interpreted with caution as the numbers of patients studied are small in surprisingly few randomized controlled trials [53]. To date, there is no evidence to support that combined diuretic treatments (i.e., adding spironolactone to thiazide or adding metolazone to furosemide) improve the outcome of preterm infants with BPD.
It is important to note that caffeine has unequivocal beneficial effects in prevention of BPD due to several mechanisms, among which is its diuretic effects [54].
Furosemide in preterm infants with patent ductus arteriosus
Oliguria occurs frequently after administration of indomethacin or ibuprofen to close a PDA, and AKI is also a complication of these drugs. On the one side, there is no evidence that furosemide can prevent the incidence of AKI in infants treated by non-steroidal anti-inflammatory drugs for PDA closure [55]. On the other side, the suggestion that by stimulating prostaglandin synthesis furosemide could promote PDA has not been confirmed. On the contrary, in a large cohort of VLBW infants, furosemide exposure was recently associated with decreased odds of PDA treatment [56]. According to a recent study in preterm infants born before 32 weeks of gestation and treated for PDA [57], furosemide exposure reaches about 25% and increases with decreasing gestational age, and individual cumulative doses can reach as much as 10 mg per kg bodyweight, which is considered an independent risk factor for nephrocalcinosis in VLBW infants.
Despite all the above conclusions, diuretics administration remains recommended in severe chronically ill patients for the management of accumulation of interstitial lung fluid, such as in cases of pulmonary edema which may occur in respiratory and cardiac acute and chronic morbidities. Repeated doses of the diuretic are often needed to restore the fluid balance.
Common side effects of diuretics
Electrolyte disturbances and frequent side effects of diuretics commonly used in neonates are shown in Table 3.
New developments in diuretic therapy
Among the three categories of diuretics under development (natriuretic peptides, adenosine A1 receptor antagonists, and ADH antagonists), only adenosine receptor antagonists have been studied in newborn infants. The diuretic effects of the methylxanthines theophylline and caffeine, two nonselective antagonists of adenosine receptors, have been briefly discussed in this article.
Key summary points
-
1.
Diuretics promote the excretion of electrolytes and water. They are primarily used in states of inappropriate salt and water retention.
-
2.
Diuretics can also be used in a variety of conditions where an increase in sodium excretion is not the primary goal of treatment, as for instance electrolyte disturbances and nephrogenic diabetes insipidus.
-
3.
Loop diuretics are the used in acute states of sodium retention. Their prolonged use in neonates and infants can impair growth, induce nephrocalcinosis, and lead to deleterious hypokalemic states.
-
4.
Among the new diuretics under development, adenosine A1 receptor antagonists appear the most promising agents.
Multiple choice questions (answers are given after the references)
-
1.
Which of the following is not a therapeutic indication of loop diuretics?
-
a)
Sodium-retaining states
-
b)
Hyperkalemic states
-
c)
Hypercalcemic states
-
d)
Nephrogenic diabetes insipidus
-
e)
Assessment of distal acidification
-
a)
-
2.
Which of the following is not a side effect of loop diuretics?
-
a)
Ototoxicity
-
b)
Hyperglycemia
-
c)
Hyperuricemia
-
d)
Gynecomastia
-
e)
Nephrocalcinosis
-
a)
-
3.
Which of the following is a possible side effect of inhibitors of carbonic anhydrase?
-
a)
Metabolic alkalosis
-
b)
Hyperkalemia
-
c)
Hypercalcemia
-
d)
Hypokalemia
-
e)
Hirsutism
-
a)
-
4.
Which diuretic among the following inhibits the sodium-potassium-chloride cotransporter NKCC?
-
a)
Acetazolamide
-
b)
Spironolactone
-
c)
Amiloride
-
d)
Hydrochlorothiazide
-
e)
Furosemide
-
a)
References
Gouyon B, Martin-Mons S, Iacobelli S, Razafimahefa H, Kermorvant-Duchemin E, Brat R, Caeymaex L, Couringa Y, Alexandre C, Lafon C, Ramful D, Bonsante F, Binson G, Flamein F, Moussy-Durandy A, Di Maio M, Mazeiras G, Girard O, Desbruyeres C, Mourdie J, Escourrou G, Flechelles O, Abasse S, Rosenthal JM, Pages AS, Dorsi M, Karaoui L, ElGellab A, Le Bail Dantec F, Yangui MA, Norbert K, Kugbe Y, Lorrain S, Pignolet A, Garnier EM, Lapillonne A, Mitanchez D, Jacqz-Aigrain E, Gouyon JB (2019) Characteristics of prescription in 29 Level 3 Neonatal Wards over a 2-year period (2017-2018). An inventory for future research. PLoS One 14:e0222667. https://doi.org/10.1371/journal.pone.0222667
Hagadorn JI, Sanders MR, Staves C, Herson VC, Daigle K (2011) Diuretics for very low birth weight infants in the first 28 days: a survey of the U.S. neonatologists. J Perinatol 31:677–681. https://doi.org/10.1038/jp.2011.11
Iacobelli S, Guignard JP (2020) Maturation of glomerular filtration rate in neonates and infants: an overview. Pediatr Nephrol. https://doi.org/10.1007/s00467-020-04632-1
Gattineni J, Baum M (2015) Developmental changes in renal tubular transport—an overview. Pediatr Nephrol 30:2085–2098. https://doi.org/10.1007/s00467-013-2666-6
Segar JL (2017) Renal adaptive changes and sodium handling in the fetal-to-newborn transition. Semin Fetal Neonatal Med 22:76–82. https://doi.org/10.1016/j.siny.2016.11.002
Iacobelli S, Gouyon JB, Bonsante F, Mastrofrancesco L, Svelto M, Valenti G (2010) Aquaporin-2 urinary excretion in preterm infants: relationship to diuresis and vasopressin. Acta Physiol (Oxf) 200:339–345. https://doi.org/10.1111/j.1748-1716.2010.02164.x
Adhikari M, Moodley M, Desai PK (1990) Mannitol in neonatal cerebral oedema. Brain Dev 12:349–351. https://doi.org/10.1016/s0387-7604(12)80320-2
Tam B, Chhay A, Yen L, Tesoriero L, Ramanathan R, Seri I, Friedlich PS (2014) Acetazolamide for the management of chronic metabolic alkalosis in neonates and infants. Am J Ther 21:477–481. https://doi.org/10.1097/MJT.0b013e31825e792c
Andrews MG, Johnson PN, Lammers EM, Harrison DL, Miller JL (2015) Acetazolamide in critically ill neonates and children with metabolic alkalosis. Ann Pharmacother 47:1130–1135. https://doi.org/10.1177/1060028013500468
Seikaly MG, Baum M (2011) Thiazide diuretics arrest the progression of nephrocalcinosis in children with X-linked hypophosphatemia. Pediatrics 108:E6. https://doi.org/10.1542/peds.108.1.e6
Krzyżaniak N, Pawłowska I, Bajorek B (2016) Review of drug utilization patterns in NICUs worldwide. J Clin Pharm Ther 41:612–620. https://doi.org/10.1111/jcpt.12440
Manfredini VA, Cerini C, Clavenna A, Dotta A, Caccamo ML, Staffler A, Massenzi L, Rezzonico RM, Study Group of Neonatal Pharmacotherapy of the Italian Society of Neonatology (2020) Furosemide use in Italian neonatal intensive care units: a national survey. Ital J Pediatr 46:86. https://doi.org/10.1186/s13052-020-00851-2
van der Vorst MM, Ruys-Dudok van Heel I, Kist-van Holthe JE, den Hartigh J, Schoemaker RC, Cohen AF, Burggraaf J (2001) Continuous intravenous furosemide in haemodynamically unstable children after cardiac surgery. Intensive Care Med 27:711–715. https://doi.org/10.1007/s001340000819
van der Vorst MMG, Kist-van Holthe JE, den Hartigh J, van der Heijden AJ, Cohen AF, Burggraaf J (2007) Absence of tolerance and toxicity to high-dose continuous intravenous furosemide in haemodynamically unstable infants after cardiac surgery. Br J Clin Pharmacol 64:796–803. https://doi.org/10.1111/j.1365-2125.2007.02913.x
Klinge JM, Scharf J, Hofbeck M, Gerling S, Bonakdar S, Singer H (1997) Intermittent administration of furosemide versus continuous infusion in the postoperative management of children following open heart surgery. Intensive Care Med 23:693–697. https://doi.org/10.1007/s001340050395
Baylen BG, Johnson G, Tsang R, Srivastava L, Kaplan S (1980) The occurrence of hyperaldosteronism in infants with congestive heart failure. Am J Cardiol 45:305–310. https://doi.org/10.1016/0002-9149(80)90650-5
Pacifici G (2012) Clinical pharmacology of the loop diuretics furosemide and bumetanide in neonates and infants. Pediatr Drugs 14:233–246. https://doi.org/10.2165/11596620-000000000-00000
Sutiman N, Koh JC, Watt K, Hornik C, Murphy B, Chan YH, Lee JH (2020) Pharmacokinetics alterations in critically ill pediatric patients on extracorporeal membrane oxygenation: a systematic review. Front Pediatr 8:260. https://doi.org/10.3389/fped.2020.00260
Jalanko H (2009) Congenital nephrotic syndrome. Pediatr Nephrol 24:2121–2128. https://doi.org/10.1007/s00467-007-0633-9
Hölttä T, Jalanko H (2020) Congenital nephrotic syndrome: is early aggressive treatment needed? Yes. Pediatr Nephrol. https://doi.org/10.1007/s00467-020-04578-4
Reynolds BC, Oswald RJA (2019) Diagnostic and management challenges in congenital nephrotic syndrome. Pediatric Health Med Ther 10:157–167. https://doi.org/10.2147/PHMT.S193684
Bagshaw SM, Delaney A, Haase M, Ghali WA, Bellomo R (2007) Loop diuretics in the management of acute renal failure: a systematic review and meta-analysis. Crit Care Resusc 9:60–68
Dubourg L, Drukker A, Guignard JP (2000) Failure of torasemide to improve renal function of hypoxemic vasomotor nephropathy in the newborn rabbit. Pediatr Res 47:504–508. https://doi.org/10.1203/00006450-200004000-00015
Gouyon JB, Guignard JP (2000) Management of acute renal failure in newborns. Pediatr Nephrol 14:1037–1044. https://doi.org/10.1007/s004670050068
Guignard JP, Ali US (2016) Acute renal failure in the neonate. J Pediatr Intensive Care 5:42–49. https://doi.org/10.1055/s-0035-1564735
Nada A, Bonachea EM, Askenazi DJ (2017) Acute kidney injury in the fetus and neonate. Semin Fetal Neonatal Med 22:90–97. https://doi.org/10.1016/j.siny.2016.12.001
Pandey V, Kumar D, Vijayaraghavan P, Chaturvedi T, Raina R (2016) Non-dialytic management of acute kidney injury in newborns. J Renal Inj Prev 6:1–11. https://doi.org/10.15171/jrip.2017.01
Borasino S, Wall KM, Crawford JH, Hock KM, Cleveland DC, Rahman F, Martin KD, Alten JA (2018) Furosemide response predicts acute kidney injury after cardiac surgery in infants and neonates. Pediatr Crit Care Med 19:310–317. https://doi.org/10.1097/PCC.0000000000001478
Oliveros M, Pham JT, John E, Resheidat A, Bhat R (2011) The use of bumetanide for oliguric acute renal failure in preterm infants. Pediatr Crit Care Med 12:210–214. https://doi.org/10.1097/PCC.0b013e3181e912a7
Merheb RC, Kruzer KA, Mhanna MJ (2014) The effect of bumetanide in extremely low birth weight infants with acute kidney injury during their first weeks of life. J Clin Pediatr Nephrol 2:53–63. https://doi.org/10.15401/jcpn/2014/v2i1/50526
Pandey V, Dummula K, Go M, Parimi P (2015) Bumetanide use in the management of oliguric preterm infants with acute kidney injury–a single center experience. J Clin Pediatr Nephrol 2:33–38. https://doi.org/10.15401/jcpn/2014/v2i2/66346
Gouyon JB, Guignard JP (1988) Functional renal insufficiency: role of adenosine. Biol Neonate 53:237–242. https://doi.org/10.1159/000242796
Gouyon JB, Guignard JP (1989) Adenosine in the immature kidney. Dev Pharmacol Ther 13:113–119. https://doi.org/10.1159/000457592
Gouyon JB, Guignard JP (1988) Theophylline prevents the hypoxemia-induced renal hemodynamic changes in rabbits. Kidney Int 33:1078–1083. https://doi.org/10.1038/ki.1988.114
Bhatt GC, Gogia P, Bitzan M, Das RR (2019) Theophylline and aminophylline for prevention of acute kidney injury in neonates and children: a systematic review. Arch Dis Child 104:670–679. https://doi.org/10.1136/archdischild-2018-315805
Bellos I, Pandita A, Yachha M (2019) Effectiveness of theophylline administration in neonates with perinatal asphyxia: a meta-analysis. J Matern Fetal Neonatal Med. https://doi.org/10.1080/14767058.2019.1673722
Chock VY, Cho SH, Frymoyer A (2020) Aminophylline for renal protection in neonatal hypoxic-ischemic encephalopathy in the era of therapeutic hypothermia. Pediatr Res. https://doi.org/10.1038/s41390-020-0999-y
Sharma D (2019) Hypertension in neonates: need for future research. J Neonatal Biol 06:3. https://doi.org/10.4172/2167-0897.1000261
Alon U, Hellerstein S, Warady BA (1991) Oral acetazolamide in the assessment of (urine-blood) PCO2. Pediatr Nephrol 5:307–311. https://doi.org/10.1007/BF00867488
Plumb LA, Van't Hoff W, Kleta R, Reid C, Ashton E, Samuels M, Bockenhauer D (2016) Renal apnoea: extreme disturbance of homoeostasis in a child with Bartter syndrome type IV. Lancet 388:631–632. https://doi.org/10.1016/S0140-6736(16)00087-8
Kirchlechner V, Koller D, Seidl, Waldhauser F (1999) Treatment of nephrogenic diabetes insipidus with hydrochlorothiazide and amiloride. Arch Dis Child 80:548–552. https://doi.org/10.1136/ade.80.6.548
Pacifici GM (2013) Clinical pharmacology of furosemide in neonates: a review. Pharmaceuticals (Basel) 6:1094–1129. https://doi.org/10.3390/ph6091094
Suyagh M, Hawwa AF, Collier PS, Millership JS, Kole P, Millar M, Shields MD, Halliday HL, McElnay JC (2012) Population pharmacokinetic model of canrenone after intravenous administration of potassium canrenoate to paediatric patients. Br J Clin Pharmacol 74:864–872. https://doi.org/10.1111/j.1365-2125.2012.04257.x
Bestic M, Reed MD (2012) Common diuretics used in the preterm and term infant. NeoReviews 13:e410–e419. https://doi.org/10.1542/neo.13-7-e410
Segar JL (2012) Neonatal diuretic therapy: furosemide, thiazides, and spironolactone. Clin Perinatol 39:209–220. https://doi.org/10.1016/j.clp.2011.12.007
Stewart A, Brion LP, Soll RF (2011) Diuretics for respiratory distress syndrome in preterm infants. Cochrane Database Syst Rev 1:CD001454. https://doi.org/10.1002/14651858.CD001454.pub3
Blaisdell CJ, Troendle J, Zajicek A (2018) Prematurity and respiratory outcomes program. Acute Responses to Diuretic Therapy in Extremely Low Gestational Age Newborns: Results from the Prematurity and Respiratory Outcomes Program Cohort Study. J Pediatr 197:42–47. https://doi.org/10.1016/j.jpeds.2018.01.066
Kassab M, Khriesat WM, Anabrees J (2015) Diuretics for transient tachypnoea of the newborn. Cochrane Database Syst Rev 11:CD003064. https://doi.org/10.1002/14651858.CD003064.pub3
Michael Z, Spyropoulos F, Ghanta S, Christou H (2018) Bronchopulmonary dysplasia: an update of current pharmacologic therapies and new approaches. Clin Med Insights Pediatr 12:1179556518817322. https://doi.org/10.1177/1179556518817322
Stewart A, Brion LP (2011) Intravenous or enteral loop diuretics for preterm infants with (or developing) chronic lung disease. Cochrane Database Syst Rev 9:CD001453
Brion LP, Primhak RA, Yong W (2006) Aerosolized diuretics for preterm infants with (or developing) chronic lung disease. Cochrane Database Syst Rev 2:CD001694
Greenberg RG, Gayam S, Savage D, Tong A, Gorham D, Sholomon A, Clark RH, Benjamin DK, Laughon M, Smith PB, Best Pharmaceuticals for Children Act—Pediatric Trials Network Steering Committee (2019) Furosemide exposure and prevention of bronchopulmonary dysplasia in premature infants. J Pediatr 208:134–140.e2. https://doi.org/10.1016/j.jpeds.2018.11.043
Stewart A, Brion LP, Ambrosio-Perez I (2011) Diuretics acting on the distal renal tubule for preterm infants with (or developing) chronic lung disease. Cochrane Database Syst Rev 9:CD001817
Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A, Solimano A, Tin W, Caffeine for Apnea of Prematurity Trial Group (2006) Caffeine therapy for apnea of prematurity. N Engl J Med 354:2112–2121. https://doi.org/10.1056/NEJMoa054065
Lee BS, Byun SY, Chung ML, Chang JY, Kim HY, Kim EA, Kim KS, Pi SY (2010) Effect of furosemide on ductal closure and renal function in indomethacin-treated preterm infants during the early neonatal period. Neonatology 98:191–199. https://doi.org/10.1159/000289206
Thompson EJ, Greenberg RG, Kumar K (2018) Association between furosemide exposure and patent ductus arteriosus in hospitalized infants of very low birth weight. J Pediatr 199:231–236. https://doi.org/10.1016/j.jpeds.2018.03.067
Iacobelli S, Lorrain S, Gouyon B, Gambacorta S, Laforgia N, Gouyon JB, Bonsante F (2020) Drug exposure for PDA closure in France: a prospective, cohort-based, analysis. Eur J Clin Pharmacol. https://doi.org/10.1007/s00228-020-02974-1
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Answers: 1: d, 2: d, 3: d, 4: e
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Guignard, JP., Iacobelli, S. Use of diuretics in the neonatal period. Pediatr Nephrol 36, 2687–2695 (2021). https://doi.org/10.1007/s00467-021-04921-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-021-04921-3